Poxvirus Infections
25
AT-A-GLANCE
■ Poxviruses are the largest animal viruses; they can cause disease of varying severity in humans.
■ Smallpox is the only poxvirus whose sole reservoir is humans, which allowed its eradication.
■ The virus used in smallpox vaccines, vaccinia, has its own adverse effects.
■ Monkeypox is a zoonotic infection endemic in Africa.
■ Milker’s nodule and orf mainly cause localized cutaneous infections.
■ Molluscum contagiosum is generally a benign cutaneous disease most frequently seen in children and immunocompromised individuals.
■ Histopathologic features of poxviral cutaneous lesions include the presence of intracytoplasmic eosinophilic inclusion bodies.
Poxviruses are a family of double-stranded DNA viruses that replicate in the cytoplasm of host cells (Table 166-1). They are the largest known animal viruses and can be seen with light microscopy.1 The poxvirus family is divided into multiple genera. Four genera affect humans: Orthopoxvirus, Parapoxvirus, Molluscipoxvirus, and Yatapoxvirus. The poxviruses that cause significant disease in humans are reviewed here. Their effects on humans range from systemic disease to localized infection to epithelial cell proliferation without other findings.
ORTHOPOXVIRUS INFECTIONS
Members of the Orthopoxvirus genus that cause disease in humans include variola (smallpox), vaccinia, cowpox, and monkeypox. Variola, vaccinia, and monkeypox are discussed in detail below. Cowpox, whose major reservoir is thought to be cats and small rodents rather than cows, rarely infects humans.
SMALLPOX (VARIOLA)
SMALLPOX (VARIOLA)
AT-A-GLANCE
■ Mortality from the major form of smallpox is approximately 30%.
■ Smallpox is transmitted mainly by the respiratory route; viremia leads to cutaneous and visceral involvement.
■ The eruption consists of multiple papules in a centrifugal distribution that progress en masse through vesicular and pustular stages.
■ The disease has not been seen since 1978, but concern exists about the potential use of variola virus for bioterrorism.
■ Smallpox vaccination has been reinstituted on a selective basis for response in the case of an outbreak.
Variola virus is the pathogen responsible for smallpox, a disease that devastated humankind in catastrophic epidemics for more than 3000 years. This poxvirus scarred and killed millions of people in both the Old and New Worlds, affecting entire populations on every continent. It is estimated to have killed approximately 500 million people in the 20th century alone.2 The practice of variolation, the intentional introduction of smallpox virus from a pustule of an infected person into a healthy nonimmune person to induce a mild form of the disease as prophylaxis against a full-scale infection, gained popularity in the 18th century.3 This practice reduced mortality significantly but caused full-scale disease in a subset of individuals, resulting in 1% to 2% mortality.3
Edward Jenner altered the course of history in 1796 when he created the first vaccine by inoculating patients with cowpox virus to protect them against the related smallpox virus. Later, vaccinia virus was used for vaccination, and smallpox was eradicated in the United States in 1949. The World Health Organization (WHO) launched a global campaign to eradicate smallpox in 1959,3 and an intensive effort culminated in global eradication by 1980.3,4
25
GENUS SPECIES HOSTS MAIN PORTAL OF ENTRY CLINICAL FEATURES TREATMENT
Orthopoxvirus Variola virus (smallpox) Humans Respiratory tract High fever and myalgia precede oropharyngeal enanthem and centrifugal exanthem. Simultaneous progression of skin lesions from macules to papulovesicles, pustules, and crusts, resulting in significant scars. Last reported case in 1978; concern for use in bioterrorism.
Postexposure vaccination to reduce severity and disease occurrence (prior to onset of clinical symptoms) Tecovirimat (SIGA Technologies) Brincidofovir (CMX001, Chimerix)
Vaccinia virus Humans Skin Used as vaccine for smallpox. Also protects against monkeypox. Vaccination site progresses from papule to vesicle, pustule, and crust, leaving scar. Adverse events occur when virus spreads locally or in a generalized manner, more severe in individuals with disruption of the skin barrier or immune compromise.
Monkeypox virus Rodents, humans, monkeys, anteaters
Symptomatic treatment for minor local reactions, or for typical systemic symptoms Vaccinia immune globulin or cidofovir for extensive lesions distant from vaccination site Skin care Fluid and electrolyte repletion
Skin Clinical presentation similar to that of smallpox but with more prominent lymphadenopathy and lower mortality.
Postexposure prophylaxis with vaccinia virus (4-14 days after exposure) Tecovirimat Cidofovir Brincidofovir
Cowpox virus Rodents, cats, humans, cattle Skin Contact with infected animal host gives rise to papule that becomes vesicular, hemorrhagic, pustular, and ulcerative; resulting eschar heals over 3-4 weeks with scarring. Constitutional symptoms and lymphangitis common. Can be extensive or severe if skin barrier is disrupted.
No known treatment
Parapoxvirus Orf virus Sheep, goats, humans Skin Contact with infected animal or fomite leads to 1 or more papules, usually on hand. Papule progresses into pustule or nodule with central umbilication and surrounding gray-white or violaceous ring and outer zone of erythema. Becomes weepy, then dries and crusts. Healing occurs over 4-8 weeks, usually without scarring. Constitutional symptoms are uncommon.
Pseudocowpox virus (paravaccinia virus)
Resolves within 4-6 weeks Debridement, topical cidofovir, or topical imiquimod may speed resolution
Cattle, humans Skin Transmission by contact with infected teats/mouths of cattle. Causes milker’s nodule. Clinical findings and course similar to orf; differentiated by animal hosts.
Bovine papular stomatitis virus
Disease is self-limited; symptomatic treatment only Curettage of large lesions may speed resolution
Cattle, humans Skin Transmitted by contact with infected mouths of cattle. Clinical findings and course similar to orf and paravaccinia.
3066
Similar to above
(Continued)
(Continued)
25
GENUS SPECIES HOSTS MAIN PORTAL OF ENTRY CLINICAL FEATURES TREATMENT
Molluscipoxvirus Molluscum contagiosum virus
Humans Skin Discrete firm, dome-shaped papules; may have central umbilication. Can be extensive in individuals with atopic dermatitis or immune compromise. Most cases resolve spontaneously in months to years, but lesions often are treated to reduce symptoms and minimize autoinoculation. Can be persistent/refractory in immunocompromised individuals.
Yatapoxvirus Tanapox
Cantharidin 0.7% topically for 2-6 hours, before rinsing Imiquimod cream Intralesional candida antigen Oral cimetidine Podophyllotoxin Cidofovir Physically destructive therapies (curettage, cryotherapy, CO2 laser, pulsed-dye laser, electrodessication)
Yatapoxvirus Tanapox virus Humans, monkeys Possibly skin Uncertain mode of transmission; possible mosquito vector from infected monkeys to humans. Short fever precedes eruption of 1 or more pruritic, indurated papules with surrounding edema. Become necrotic and/or ulcerative, then heal within 6 weeks with scarring.
Humans,
Possibly skin Uncertain mode of transmission; pos-
virus
monkeys
After eradication, the WHO directed all laboratories other than the Centers for Disease Control and Prevention (CDC) in the United States and the Vector laboratory in Russia to destroy their smallpox samples. However, a misplaced vial of variola virus was discovered at the National Institutes of Health facility in Bethesda, Maryland in 2014,5 raising the theoretical possibility that other unreported stocks of virus may exist and could be used as a biologic weapon. Concerns about bioterrorism have renewed the need for knowledge about smallpox and the development of improved vaccines and treatments in case the disease reemerges.
EPIDEMIOLOGY
Unlike other members of the poxvirus family, smallpox only affects humans and cannot be acquired from other species. Transmission is generally via respiratory droplets and requires close contact but aerosol spread also has been reported. Outbreaks occur in the winter and early spring seasons when conditions of low humidity and low temperature favor survival of the aerosolized virus.6 Smallpox is less infectious than other diseases spread by the respiratory route, including measles, varicella, and influenza. The estimated rate of secondary infection of unvaccinated contacts is 37% to 88%.7 Secondary cases are often limited to family members or health care workers. Spread of smallpox is facilitated by the large quantity of virus in the aerosolized droplets, high population density, and extensive contact between the infected individual and others. The very young, the elderly, and pregnant women are more susceptible to infection.8 Individuals with more-severe clinical disease are reported to be
Self-resolving within
Self-resolving within 6 weeks, with resulting lifelong immunity
sible mosquito vector from infected monkeys to humans. Short fever precedes eruption of 1 or
6 weeks, with resulting lifelong immunity
more pruritic, indurated papules with surrounding edema. Become necrotic and/or ulcerative, then
heal within 6 weeks with scarring.
more infectious, but these same people also tend to be toxemic and confined to bed. There are 2 main strains of variola virus: (a) variola major, the more common, severe, and often lethal form, and (b) variola minor, a milder less-lethal form. Today, the majority of the world’s population is susceptible to smallpox disease, as routine vaccination of civilians was discontinued in the United States in 1971 and worldwide in the 1980s. Those vaccinated before 1972 have uncertain levels of immunity remaining. Until 2002, only laboratory workers handling non– highly attenuated orthopoxviruses still were advised to receive routine vaccination. Since that time, military personnel and a small group of U.S. civilians who would serve as first-line responders in a bioterrorism attack have been vaccinated.9 The risk of adverse effects from the vaccine, particularly in immunocompromised patients and individuals with atopic dermatitis or other skin barrier defects, has prevented mass vaccination policies.
CLINICAL FEATURES Prodrome: An infected individual is asymptomatic during the incubation period of viral replication. A prodrome of high fever (39°C to 41°C [102.2°F to 105.8°F]), chills, myalgia, and severe headache develops within 7 to 17 days of exposure, with an average incubation of 10 to 12 days.7 The prodrome usually lasts 2 to 3 days, during which the affected individual is severely ill and often bedridden.
Cutaneous Findings: Approximately 1 day after the onset of fever, an enanthem of red macules develops on the mouth, tongue, and oropharynx and subsequently
3067
25
vesiculates and ulcerates, releasing high concentrations of transmissible virus particles in respiratory secretions. A skin rash (exanthem) usually follows a day later.7 The fever usually declines with appearance of the rash.10
The classic smallpox rash begins as macules on the face and extremities but quickly spreads to cover the body. Involvement of all parts of the body, including palms and soles, occurs within 24 to 48 hours. Smallpox tends to have a centrifugal distribution, meaning that lesions are most concentrated on the face and distal extremities. A key characteristic of smallpox is that all lesions progress synchronously through macular, papular, vesicular, and pustular stages. Each stage lasts 1 to 2 days. Macules become raised papules 2 to 3 mm in diameter within 1 or 2 days and then form vesicles 2 to 5 mm in diameter (Fig. 166-1) within another 1 or 2 days. Firm, deep-seated pustules 4 to 6 mm in diameter (Fig. 166-2) develop 4 to 7 days after the onset of the rash and may umbilicate or become confluent. After 8 to 10 days, the lesions begin to crust (Fig. 166-3). Fever may reoccur during the pustular stage, especially if a secondary bacterial infection has developed. Scabs begin separating 2 weeks after the onset of the rash and typically have all separated by 4 weeks. After their resolution, pitted scars (“pockmarks”) remain on 65% to 80% of survivors and can be disfiguring (Fig. 166-4).7 Scarring is most common on the face, where there are larger and more numerous sebaceous glands, which are particularly susceptible to infection and destruction by variola virus.4
Classic or ordinary smallpox, described above, is the most common type, accounting for 85% of smallpox outbreaks.2,4
In addition to ordinary smallpox, the WHO recognizes 3 other clinically recognizable forms of variola major, which differ in disease presentation and rash burden.2,10 These are modified smallpox, flat smallpox, and hemorrhagic smallpox. Modified smallpox (approximately 5% to 7% of all cases) is a mild, nonfatal form of variola major infection that occurs in previously vaccinated individuals. It has a
3068
milder prodrome, fewer lesions, and an accelerated and abbreviated course because the disease has been “modified” or attenuated by previous vaccination.2
Lesions tend not to progress to vesicles or pustules, crusting by day 10. Flat smallpox (also called malignant smallpox) is an uncommon form of variola major infection (approximately 5% of cases) in which lesions develop slowly and persist as soft, velvety vesicles that coalesce into confluent, edematous plaques with a flat appearance.2
It usually occurs in children and unvaccinated individuals lacking cellular immunity. Affected individuals become severely ill with toxic fever, and most die with hemorrhagic lesions and pneumonia.7
Hemorrhagic smallpox, also known as fulminant smallpox, involves hemorrhage into the skin or mucous membranes and is the rarest (<1% of cases) and deadliest form of smallpox.2 It is equally common in unvaccinated and vaccinated persons and is almost always fatal.2 In the early hemorrhagic form, massive hemorrhage from mucosal surfaces occurs before any rash develops and leads to death before the sixth day of illness.11 This form is more common in adults, and pregnant women are especially susceptible. In the late hemorrhagic form, hemorrhage occurs after onset of the typical rash and death occurs within 12 days.11 This form affects women and men equally.4
Variola sine eruption, is a brief febrile illness (48 hours or less) without a rash that can occur when a vaccinated individual is exposed to someone infected with variola major. This brief illness can be confirmed by serologic studies showing a rise in antibody titers against smallpox virus.7
Infections with the variola minor strain, the milder strain of smallpox, are clinically indistinguishable from cases of modified smallpox and mild cases of ordinary smallpox. Historically, outbreaks were diagnosed retrospectively as variola minor if the fatality rate was low (1% or less). Minor and major strains can now be differentiated by polymerase chain reaction (PCR).4
Noncutaneous Findings: Variola virus spreads by the blood to noncutaneous systems. It can infect the metaphyses of growing bones and lead to arthritis in up to 2% of affected children. Osteomyelitis variolosa is less frequent but may also cause bone deformities.12
Swelling of the eyelids and a mild conjunctivitis are common findings. Cough and bronchitis may be seen
25
in some cases of smallpox. A degree of encephalopathy often occurs, with symptoms ranging from headache and hallucinations to delirium and psychosis.4 Gross hematuria can occur with the hemorrhagic type of variola major.13
Complications: Secondary bacterial infection occurs commonly in skin lesions, as well as at regional lymph nodes, affecting 5% of individuals. Keratitis and corneal ulceration, common in malnourished individuals, result in blindness in 1% of cases. Variola virus or bacterial superinfection can lead to respiratory complications, including pneumonia, at days 8 to 10 of illness. Both arthritis and osteomyelitis can lead to limb deformities, including bone shortening, subluxation, and flail joints. Orchitis is less common and usually unilateral. Encephalitis is reported in 0.2% of cases.4
ETIOLOGY AND PATHOGENESIS
Smallpox is caused by the variola virus, a linear, doublestranded DNA virus of the genus Orthopoxvirus. Variola virus measures approximately 300 × 250 × 200 nm and has a brick-shaped appearance on electron microscopy (Fig. 166-5). Although the 2 major forms, variola major and variola minor, have approximately 98% genetic homology, variola major is markedly more virulent, with significantly higher mortality.14
Humans are the only natural reservoir of the variola virus. Smallpox usually spreads by implantation of droplets containing virus on to nasal, oral, or pharyngeal mucous membranes or alveoli of the lung.4 Household contacts of an infected individual and others with prolonged face-to-face exposure are at greatest risk of infection.9 Variola virus is less commonly spread by accidental inoculation into the skin, through the conjunctiva, and through contact with infected body fluids or highly contaminated fomites. Rarely, it is transmitted transplacentally, by long-range
3069
25
airborne viral particles, or by viral particles suspended in enclosed areas.15
The virus attaches to respiratory epithelial cells, travels to regional lymph nodes, and replicates at these sites. Transient primary viremia with uptake of the virus by macrophages occurs, and the virus spreads to the reticuloendothelial organs, where asymptomatic replication continues. A massive secondary viremia follows and causes the onset of symptoms (the prodromal period). The virus spreads to the skin and mucosa, along with other organs and tissues such as the liver and kidneys.7,16
Variola virus is transmissible beginning in the late prodromal phase by aerosolization of viral particles from the oropharynx. It is most infectious during the first week of the rash, which is when enanthem lesions have ulcerated and are releasing virus into mouth and pharynx secretions.4 The virus remains transmissible until all scabs have fallen off of skin lesions.16
DIAGNOSIS
An acute, generalized rash with characteristic wellcircumscribed, firm, deep-seated vesicles or pustules should raise concern for smallpox. The CDC protocol for evaluation of acute, generalized vesicular or pustular rashes, available on the CDC website (cdc.gov), should be consulted and followed whenever suspicion arises.17 Airborne and contact precautions should be implemented immediately. The next step is defining the suspicion for smallpox as high, moderate, or low, based on the CDC’s major and minor smallpox criteria. Major criteria include (a) febrile prodrome 1 to 4 days before rash onset; (b) classic smallpox lesions, defined as deep-seated, firm/hard, round, well-circumscribed vesicles or pustules; and (c) lesions in the same stage of development (ie, all vesicles or all pustules) on any one part of the body. Minor criteria include (a) centrifugal distribution, meaning that lesions are most concentrated on the face and distal extremities; (b) lesions first occurred on the oral mucosa/palate, face, or forearms; (c) patient appears toxic or moribund; (d) slow evolution of lesions, meaning that they evolve from macules to papules to pustules, with each stage lasting 1 to 2 days; and (e) lesions on palms and soles. Risk for smallpox is considered to be high if patients meet all major criteria. Patients with febrile prodrome plus 1 other major criteria or 4 or more minor criteria are considered to have a moderate risk for smallpox. Patients with febrile prodrome but fewer than 4 minor criteria or no febrile prodrome are considered to have a low risk for smallpox. The recommended workup depends on smallpox risk status. When the risk of smallpox is determined to be high, local and state health departments should be contacted immediately; they will lead diagnosis and management efforts, in coordination with the CDC. High-risk specimens should be tested only at laboratories with appropriate expertise and biosafety levels.
3070
Moderate- and low-risk cases should be worked up for more common causes of febrile exanthema, such as varicella zoster virus (VZV), herpes simplex virus (HSV), and enterovirus. The CDC recommends Tzanck smear to evaluate for HSV as well as direct fluorescent antibody assay to evaluate for HSV and VZV. PCR for VZV, HSV, and enterovirus should be performed. If possible, electron microscopy to distinguish between poxvirus and VZV should be performed, and the virus can be cultured. Biopsy to evaluate for erythema multiforme also can be considered. PCR for nonvariola Orthopoxvirus should be conducted and can be coordinated by the CDC. PCR for all orthopoxviruses, including variola, also can be performed. Multiple diagnostic methods are used to improve diagnostic certainty. For high-risk cases, the focus is on ruling out variola before any additional testing is performed. All testing should be performed by a biosafety level 3 laboratory. Electron microscopy can be performed under biosafety level 3 conditions at a local facility. All other testing should be performed by a Laboratory Research Network facility or by the CDC. These laboratories will perform variola-specific PCR, nonvariola Orthopoxvirus PCR, and PCR that tests for all orthopoxviruses. In high-risk cases, testing for VZV, HSV, and enterovirus will only be pursued once variola has been ruled out.18
Special Tests: Since the eradication of smallpox the positive predictive value of any one test is very low, so multiple methods of testing are used to confirm a diagnosis of smallpox. Real-time PCR (RT-PCR) is the quickest and most sensitive assay for detecting and differentiating between orthopoxviruses. As mentioned above, 3 different assays are used to evaluate a possible smallpox infection: (a) Orthopoxvirus RT-PCR, which detects all Orthopoxvirus including variola; (b) nonvariola Orthopoxvirus RT-PCR, which detects all Orthopoxvirus except for variola; and (c) RT-PCR assay that detects only variola. PCR is very useful for distinguishing viral species but cannot determine whether a virus is viable. Viral culture for virus isolation has the benefit of providing additional material for testing, but should only be performed by the CDC. Historically, orthopoxviruses could be differentiated by the morphology of the pocks they produced on the chorioallantoic membranes of chicken embryos, but this is not commonly performed today.16
Electron microscopy is most useful for confirming the presence of a virus and differentiating between poxvirus and varicella. It can distinguish between brick-shaped orthopoxviruses and icosahedral varicella viruses, but cannot distinguish among orthopoxviruses (ie, cannot distinguish variola from vaccinia, monkeypox, or cowpox).19
Serologic testing, including immunofluorescence and enzyme-linked immunosorbent assay, has limited usefulness in diagnosis of smallpox because orthopoxviruses are closely related and there is significant antibody cross-reactivity. Serologic testing cannot reliably distinguish between variola, vaccinia, and monkeypox
infection. However, it can be useful for confirming past exposure to Orthopoxvirus.19
As with serologic testing, current immunohistochemistry assays can identify Orthopoxvirus but cannot differentiate among species of Orthopoxvirus. However, immunohistochemistry can be helpful in identifying other microorganisms such as HSV, VZV, enterovirus, syphilis, and rickettsia.19
Laboratory Abnormalities: The white blood cell count may increase as the skin lesions of smallpox become pustular. Severe thrombocytopenia occurs in hemorrhagic smallpox, both early and late types. A marked decrease in the level of factor V (accelerator globulin) and increase in thrombin time are noted in the early hemorrhagic form, likely from disseminated intravascular coagulation. The late hemorrhagic form has a smaller degree of these coagulation disturbances.4
Pathology: Skin biopsy specimens from early papules show edema and dilation of the capillaries of the papillary dermis with a perivascular infiltrate of lymphocytes, histiocytes, and plasma cells. With progression, the cells of the epidermis become vacuolated and swollen and undergo ballooning degeneration. These vesicles have characteristic intracytoplasmic inclusion bodies called Guarnieri bodies. Pustules form with migration of polymorphonuclear cells into the vesicles. Eventually, the pustule becomes a crust, with new epithelium growing to repair the surface. Mucous membrane lesions show similar changes but also have extensive necrosis of the epithelial cells leading to rapid ulceration rather than vesiculation.20
The CDC algorithm recommends histopathologic and immunohistochemical analysis only after workup for VZV, HSV, and enterovirus and Orthopoxvirus PCR analysis are negative.18
DIFFERENTIAL DIAGNOSIS
25
Most Likely
■Papulovesicular eruption
■Coxsackievirus infection
■Extensive arthropod or mite infestation
■Varicella
■Disseminated zoster
■Generalized vaccinia
■Prodromal morbilliform eruption
■Erythema multiforme
■Drug eruption
■Hemorrhagic lesions (smallpox only)
■Meningococcemia
■Disseminated intravascular coagulation
■Mucosal lesions
■Hand-foot-and-mouth disease
■Stevens-Johnson syndrome
Consider
■Papulovesicular eruption
■Kaposi varicelliform eruption
■Eczema vaccinatum
■Extensive molluscum contagiosum (in immunosuppressed patients)
■Bullous impetigo
■Pityriasis lichenoides et varioliformis acuta
■Rickettsialpox
■Prodromal morbilliform eruption
■Measles
■Other viral infections
■Hemorrhagic lesions (smallpox only)
■Acute leukemia
■Viral hemorrhagic fevers
■Mucosal lesions
■Oral herpes simplex
Always Rule Out
Always Rule Out
■Papulovesicular eruption
■Papulovesicular eruption
■Secondary syphilis
■Secondary syphilis
■Hemorrhagic lesions (smallpox only)
■Hemorrhagic lesions (smallpox only)
■Acquired coagulopathy
■Acquired coagulopathy
■Mucosal lesions
■Mucosal lesions
■Stevens-Johnson syndrome
■Stevens-Johnson syndrome
with lesions most concentrated on the face and distal extremities. In contrast, chickenpox has a centripetal distribution, with lesions most concentrated on the trunk. Palms and soles may be affected in smallpox, but are rarely involved in chickenpox.17
Disseminated herpes zoster can appear similar to varicella but usually begins in a dermatomal distribution. The morbilliform prodromal rash of smallpox can be confused with coxsackievirus or measles infections. Human monkeypox clinically resembles smallpox but often manifests with lymphadenopathy. It is a zoonotic disease and is not spread as easily between persons. Secondary syphilis should be considered, especially when there are lesions on the palms and soles, but these lesions do not progress.
3071
25
The lesions of hemorrhagic smallpox can be similar to those of meningococcemia, viral hemorrhagic fevers such as Ebola, dengue or rift valley fever, severe acute leukemia, and other acute hemorrhagic eruptions, such as those associated with coagulopathies.
CLINICAL COURSE AND PROGNOSIS
Death from smallpox typically occurs during the second week of illness and is thought to be caused by toxemia associated with immune complexes with variola antigens, which induce hypotension/shock and multiorgan failure. Underlying host immune deficiencies likely play a role in the most severe flat and hemorrhagic forms of the disease.2 Encephalitis is an important factor in death from variola minor but not from variola major.4,7
The overall mortality rate for variola major is 30%, compared to less than 1% for variola minor.3,4 Mortality from ordinary smallpox ranges from less than 10% when lesions are discrete to 50% to 75% when lesions are confluent. Modified smallpox is associated with less than 10% mortality. In contrast, flat smallpox has a case fatality rate of more than 90%, and hemorrhagic forms have nearly 100% mortality. Those who survive the disease will have lifetime immunity.
MANAGEMENT
A patient suspected of having smallpox should be isolated in a negative-pressure room. Postexposure vaccination before the development of clinical symptoms can reduce disease occurrence and severity, as discussed below; however, vaccination after the development of clinical symptoms does not appear to provide any benefit.21
Treatments for smallpox infection have not been studied in humans but have been investigated under the Animal Efficacy Rule, which allows the U.S. Food and Drug Administration (FDA) to grant approval based on animal model studies when studies in humans are not ethical or feasible.22
Tecovirimat (SIGA Technologies, New York, NY), an Orthopoxvirus-specific antiviral medication, was added to the U.S. Strategic National Stockpile in 2013 for treatment of smallpox.23,24 In the event of a smallpox outbreak, it would be used under the Emergency Use Authorization. It works by targeting the F13L vaccinia gene that is highly conserved among orthopoxviruses and preventing viral egress from infected cells.21
It reduces morbidity and mortality of variola infection in nonhuman primates in both prelesional and postlesional settings.25
Brincidofovir (CMX001; Chimerix, Durham, NC), a lipid conjugate of cidofovir with broad-spectrum in vitro activity against double-stranded DNA viruses, is being studied as a potential smallpox therapy under the Animal Efficacy Rule. Initial studies in a rabbit model of smallpox were promising, with a significant reduction in mortality when treated after the first sign of clinical disease.25A
3072
A National Institutes of Health strategy for developing smallpox treatments is to identify broad-spectrum antivirals that have obtained regular FDA approval for other viral indications and then seek approval for use against orthopoxviruses under the Animal Efficacy Rule.23
Prevention: Vaccination with vaccinia virus (Table 166-3) is 90% to 96% effective in preventing smallpox disease when given before exposure to variola virus. For postexposure prophylaxis, vaccination within 2 to 3 days of exposure can protect against severe disease. Vaccination within 4 to 5 days may protect against death.3
Vaccination with vaccinia virus is not currently available to the general public, as the risk of smallpox outbreak is thought to be low, the risk of adverse effects is significant, particularly in the immunosuppressed and those with skin barrier defects, and postexposure prophylaxis is effective. However, vaccination is indicated for laboratory workers handling non–highly attenuated orthopoxviruses as well as individuals designated to respond to a suspected smallpox outbreak.9
In the event of an outbreak, the U.S. government has stockpiled enough smallpox vaccine to vaccinate the entire U.S. population.2 The 3 currently stockpiled vaccines are: ACAM2000 (Emergent, Gaithersburg, MD), Aventis Pasteur Smallpox Vaccine (APSV; Sanofi Pasteur, Lyon, France), and Imvamune (Bavarian Nordic, Zealand, Denmark). ACAM2000 and APSV contain replication-competent virus, meaning that they can replicate in mammalian cells. ACAM2000 vaccine, grown in cell culture, was licensed by the FDA in 2007 and replaced the previously licensed Dryvax vaccine, made in calf skin, which was destroyed.2,3,26
APSV, a calf-lymph-origin vaccine manufactured the 1950s, contains the same strain of virus used to produce Dryvax and ACAM2000. Imvamune contains a replication-deficient strain of vaccinia virus, which was attenuated by multiple passages through tissue
Indications
■Preexposure prevention of smallpox for laboratory workers, first responders, and some military personnel.
■Postexposure prophylaxis against severe disease and death.
Contraindications
Contraindications
■Contraindications in the preexposure setting:
■Contraindications in the preexposure setting:
■History of atopic dermatitis or current disruption of the skin barrier in self or close contact.
■History of atopic dermatitis or current disruption of the skin
barrier in self or close contact.
■Immunosuppression in self or close contact.
■Immunosuppression in self or close contact.
■Heart disease or significant cardiac risk factors.
■Heart disease or significant cardiac risk factors.
■Serious allergy to vaccine component.
■Serious allergy to vaccine component.
■Age younger than 12 months.
■Age younger than 12 months.
■Pregnancy, breastfeeding, or pregnant close contact.
■Pregnancy, breastfeeding, or pregnant close contact.
■Contraindications in the postexposure setting:
■Contraindications in the postexposure setting:
■No absolute contraindications in the case of an actual smallpox outbreak.
■No absolute contraindications in the case of an actual smallpox
outbreak.
aCurrent (as of this writing) Centers for Disease Control and Prevention (CDC) recommendations were issued in 2016.38
culture and cannot replicate in mammalian cells. It was designed for individuals at high risk for complications from vaccination with replication-competent virus. In the event of an outbreak, APSV and Imvamune would be used under Investigational New Drug or Emergency Use Authorization regulatory mechanisms.2
The primary strategy for postexposure protection in an outbreak is vaccination with replication-competent ACAM2000 and APSV. These are derived from the strain used during the eradication campaign, so confidence in their efficacy is high. ACAM2000 will be used first, and the older APSV will be used after supplies of ACAM2000 run out. The viral strain used in the Imvamune vaccine was not used in the eradication campaign, so its efficacy is less certain, and it requires 2 doses (a primary–booster sequence), so it is not optimal for emergency treatment.2
In the event of an outbreak of smallpox, individuals with known exposure to smallpox should be vaccinated with replication-competent smallpox vaccine unless they are severely immunodeficient and not expected to benefit from vaccine, such as those who have received bone marrow transplants within the past 3 months, individuals infected with HIV with CD4 cell counts <50 cells/µL (or age-adjusted equivalent levels in children), and individuals with severe combined immunodeficiency or complete DiGeorge syndrome. When minimal benefit from vaccination is expected, treatment with antiviral therapy is preferred, but there is no absolute contraindication to vaccination during an outbreak, and Imvamune is a reasonable option if antivirals are not available. Pregnant and breastfeeding women should be vaccinated with replication-competent vaccine.2
Vaccination with replication-competent vaccine also may be advised for individuals with no known exposure but high risk for infection. However, in the absence of known exposure, vaccination with replication-competent vaccine is relatively contraindicated for individuals with atopic dermatitis and individuals with HIV infection with CD4 counts 50 to 199 cells/µL (or age-adjusted equivalent levels in children). Instead, these individuals should be vaccinated with Imvamune if availability and time allow.2
Vaccination does not provide lifelong immunity. Most estimates suggest that primary vaccination gives full protection for 3 to 5 years and waning immunity for at least another 10 years. Revaccination may give significant protection for at least 30 years.27
VACCINIA AND SMALLPOX VACCINATION
VACCINIA AND SMALLPOX
VACCINATION
AT-A-GLANCE
■ The smallpox vaccine contains live vaccinia virus.
■ Smallpox vaccination is not currently available to the public.
25
■ Smallpox vaccination can cause serious adverse effects in some individuals.
■ Vaccination soon after exposure to smallpox can prevent severe disease and death.
■ The U.S. government has stockpiled enough smallpox vaccine to immunize all U.S. citizens in case of an outbreak.
Discussion here focuses on the features of vaccinia virus used as a smallpox vaccine; vaccinia virus is not known to cause natural infection. The discussion pertains specifically to replication-competent vaccinia used in ACAM2000 and APSV, and Dryvax vaccines. The Imvamune vaccine, which contains highly attenuated vaccinia incapable of replicating in human cells, is not discussed here because it produces no skin reaction and has no risk of secondary transmission.2
EPIDEMIOLOGY
Vaccinia is member of the Orthopoxvirus genus with similarities to cowpox. Although the original smallpox vaccination contained cowpox, over time vaccination strains became contaminated with vaccinia, which was similarly effective and eventually replaced cowpox as the main vaccination agent during the 19th century.3
Routine smallpox vaccination was discontinued in the United States in 1972 and globally after 1980. Vaccination of the military and a small group of voluntary public health and health care workers who would be first-line responders in a possible outbreak was reinitiated in the United States in 2002.2,9,28
Vaccination with the replication-competent vaccinia virus causes a major local skin reaction, which indicates that the vaccination has been effective. It carries risk of more severe adverse effects in some individuals, including young children and individuals with atopic dermatitis. Because of significant homology with other poxviruses, vaccination with vaccinia virus provides protection not only against smallpox but also against closely related orthopoxviruses including monkeypox and cowpox.4
CLINICAL FEATURES Cutaneous Findings: The normal local skin reaction to vaccination begins 3 to 5 days after administration, starting with a papule that develops into a vesicle (Jennerian vesicle) and then a pustule around days 7 to 9. It crusts and scabs over during days 10 to 14, with the scab detaching at days 17 to 21 and leaving a residual scar (Fig. 166-6). A robust local cutaneous reaction 7.5 cm or larger in diameter occurs in up to 16% of vaccinations (Fig. 166-7). This can be mistaken for bacterial cellulitis, but it peaks 6 to 12 days after vaccination and improves spontaneously without antibiotic therapy in 24 to 72 hours.29 In contrast, secondary bacterial infections usually occur within the first 5 days or 30 days after vaccination.
3073
25
Primary Vaccination Site Reaction
Day 4
Day 7
Day 14 Day 21
Minor local reactions that can occur near the primary site include intense surrounding erythema or edema and nearby satellite lesions.27
Noncutaneous Findings: Soreness almost universally occurs at the vaccination site, and lymphadenopathy/lymphangitis also may be seen. Systemic symptoms can occur and are considered normal reactions. Systemic symptoms include fever (greater than 37.7°C [99.9°F] and more common in children), chills, headache, myalgias, and malaise. They generally peak at days 8 to 10 and last 1 to 3 days. Approximately 30% of vaccine recipients feel too ill to carry out normal activities.30
3074
Cutaneous Complications: Adverse effects from vaccinia vaccinations were studied most extensively for the first-generation vaccine (Dryvax), which is no longer used. Fewer individuals have been vaccinated with the newer second-generation vaccines (ACAM2000, APSV, and Imvamune), so their adverse effects are less-well studied. However, because ACAM2000 is derived from the same viral strain used in manufacturing Dryvax, its safety profile is expected to be similar, if not identical.2,3 With a larger population of immunosuppressed individuals and rising prevalence of atopic dermatitis, the potential for adverse effects from replication-competent vaccines is higher than it was historically.3 Replicationcompetent vaccines are relatively contraindicated in these populations, and highly attenuated vaccinia vaccines like Imvamune have been developed for use in these populations. Adverse cutaneous reactions associated with replication-competent smallpox vaccination can be localized or generalized. Adverse events can occur at any age, but infants and children younger than the age of 5 years tend to be particularly affected. Adverse reactions are 10 times more common with primary vaccination than revaccination. Secondary bacterial infection, usually by staphylococci or group A streptococci, can occur at the primary site. Accidental vaccinia is the autoinoculation of vaccinia virus from the vaccination site to another area. It is the most common adverse event seen and accounts for about half of all adverse events. The most common sites of transfer are the eyelids (Fig. 166-8), nose, mouth, and genitalia. Lesions are seen at these areas
7 to 10 days after vaccination, and they usually follow the time course of the original primary lesion. The lesions may be more attenuated if autoinoculation occurs more than 5 days after vaccination as the host immune response is developing.28 Accidental inoculation to the eyes can lead to conjunctivitis, keratitis, or iritis. Vaccinia keratitis can cause corneal ulceration with scarring and visual loss. Generalized, nonspecific, immune-mediated reactions, including morbilliform and roseola-like rashes, may develop. Vaccination can lead to generalized vaccinia, in which macular, papular, or, less commonly, vesicular lesions can be disseminated to normal skin without evidence of autoinoculation. Generalized vaccinia can be limited or extensive and can occur anywhere on the body (Fig. 166-9). It is thought to be
25
caused by spread of vaccinia virus via the bloodstream and usually occurs 6 to 9 days after primary vaccination and progresses through the typical stages of vaccinia lesions. The condition is self-limited in immunocompetent individuals but is often more severe in the setting of immunodeficiency.27
Hypersensitivity reactions such as erythema multiforme can also develop (Fig. 166-10). These rashes typically self-resolve over several days. In rare cases, Stevens-Johnson syndrome can develop and requires hospitalization and supportive care. Eczema vaccinatum is the localized or generalized spread of vaccinia virus in individuals with atopic dermatitis or, less frequently, other chronic dermatoses such as Darier disease. An affected individual feels ill with fever, malaise, and lymphadenopathy. Eczema vaccinatum can occur in the primary vaccine recipient, with onset usually at the same time or soon after the appearance of lesions at the vaccination site. Papules, pustules, or vesicles can occur anywhere on the body, but have a predilection for areas with prior lesions of atopic dermatitis (Fig. 166-11). The number of lesions can range from several to hundreds; the most serious cases result in substantial loss of skin barrier.
3075
25
The severity of eczema vaccinatum is independent of the severity or activity of the atopic dermatitis or other underlying skin disease. It also can be acquired by secondary transmission, usually by children in contact with a recently vaccinated family member.31,32
Vaccination of individuals with severe impairment of the immune system leads to progressive vaccinia, also called vaccinia necrosum and vaccinia gangrenosa. In these individuals, the primary lesion at the site of vaccination does not heal but instead enlarges and progresses to a painless ulcer with central necrosis (Fig. 166-12). Viral replication is not halted and viremia occurs, with similar metastatic lesions developing at distant sites in the skin, bone, and/or viscera. Most cases have occurred in individuals with defective cell-mediated immunity, but cases also have been described in those with humoral defects.7 The degree
3076
of immune impairment may correlate with the risk for development of progressive vaccinia.33
Noncutaneous Complications: CNS complications can occur in previously healthy individuals. Postvaccinial encephalopathy most commonly affects children younger than 2 years of age, causing cerebral edema without inflammation. Symptoms develop abruptly 6 to 10 days after vaccination and can include fever, headache, seizures, hemiplegia, aphasia, and transient amnesia. Postvaccinial encephalitis and encephalomyelitis occur 11 to 15 days after vaccination, with fever, malaise, vomiting, and headache that progress to confusion, seizures, amnesia, spinal cord signs, and coma.34 These complications are thought to be autoimmune reactions, because vaccinia virus is not found in either sampled cerebrospinal fluid or tissue. Other neurologic events reported to occur in temporal association with smallpox vaccination include transverse myelitis, paralysis, seizures, and polyneuritis, but causality has not been established.4,35
Myocarditis/pericarditis is the most common serious adverse effect following immunization with ACAM2000. In Phase 3 clinical trials, the incidence was 5.7 per 1000 first-time vaccinees. The risk for myocarditis with APSV is expected to be similar.2
Smallpox vaccination of a woman during pregnancy can rarely lead to fetal or congenital vaccinia; approximately 50 cases are reported in the literature. Transmission to the fetus can occur at any time during the pregnancy and results in lesions on the skin, mucous membranes, and placenta. The appearance can be similar to that of generalized vaccinia or progressive vaccinia, and lesions can be extensive (Fig. 166-13). It is unknown whether infection is through the blood or by direct contact with infected amniotic fluid. No reliable intrauterine diagnostic test exists to confirm fetal infection. ACAM2000 has not been studied in pregnant women.3
ETIOLOGY AND PATHOGENESIS
Smallpox vaccination involves the introduction of vaccinia virus into the outer layers of the intact skin by multiple punctures (scarification) with a bifurcated needle that has been dipped in the vaccine (Fig. 166-14). Two to 3 punctures are recommended for primary vaccination and 15 punctures are recommended for revaccination.9
After inoculation, the replication- competent virus rapidly multiplies locally and occasionally at regional lymph nodes. When replication-competent vaccine is administered, viable, transmissible vaccinia virus is present at the resulting skin lesion until the lesion scabs and separates. A major cutaneous reaction is expected and is the primary indication of an effective immune response. The area heals with scarring at the injection site. Infection is usually limited by the host response with the development of antibody-mediated and cell-mediated immunity.16 Adverse events and complications occur when the virus spreads outside of the local area, either by transfer or because of host inability to contain the response.
Studies suggest that immunoglobulin M antibodies, detected as early as day 4 of vaccination, may play a role in preventing potentially deadly early viral spread.36 Neutralizing immunoglobulin G antibodies and cellular immunity start to become detectable around day 7 of vaccination and are responsible for maintaining the long-term host-immune response to the virus.
25
DIAGNOSIS
Recent personal history of vaccinia vaccination supports the diagnosis. History of recent vaccinia vaccination of a close contact should raise suspicion for secondary transmission.
CLINICAL COURSE AND PROGNOSIS
Typically a papule develops at the inoculation site several days after administration and evolves into a vesicle and then a pustule. A scab typically forms within 2 weeks and falls off within 3 weeks, leaving a scar (see Fig. 166-6). Potentially fatal adverse reactions from smallpox vaccination are eczema vaccinatum, progressive vaccinia, and postvaccinial CNS disease, described above. The mortality rate for eczema vaccinatum is 30% to 40%.3
Progressive vaccinia is universally fatal if untreated. CNS complications have a 15% to 25% fatality rate. Individuals with postvaccinial encephalopathy, encephalitis, or encephalomyelitis may recover in approximately 2 weeks, but 25% of survivors are left with residual sequelae (eg, mental impairment, paralysis).34
Most fatalities from secondary transmission occur in infants younger than 1 year of age who develop eczema vaccinatum after contact with a recently vaccinated individual. Fetal vaccinia often results in fetal or neonatal death.31,34
Management: Symptomatic treatment alone is needed for minor local events (robust take, lymphangitis, intense erythema, or edema) and typical systemic symptoms (headache, malaise, myalgia, fever) occurring after vaccination. Secondary bacterial infections should be treated with appropriate antimicrobial therapy. Uncomplicated cases of accidental secondary transmission of vaccinia do not require therapy. Extensive vaccinial lesions distant from the vaccination site and secondary transmission of vaccinia can be treated by IV administration of vaccinia immune globulin (VIG) or cidofovir to speed recovery. VIG is an FDA-approved sterile solution of the immunoglobulin fraction of plasma from persons vaccinated with vaccinia. The Strategic National Stockpile contains limited quantities of both VIG and cidofovir. Cidofovir is used under an Investigational New Drug protocol. Generalized vaccinia usually requires only symptomatic treatment, but if severe, such as in those with immunodeficiency, VIG may be beneficial. With severe eczema vaccinatum in which there is significant loss of the skin barrier, meticulous skin care and fluid and electrolyte repletion are needed. Early treatment with VIG has been shown to reduce mortality from eczema vaccinatum (from 30% to 40% down to 7%, based on preeradication era data).33 VIG administration and care in an intensive care unit also reduces the case fatality rate of progressive vaccinia from 100% to 20% to 30%.34
Treatment of neurologic complications is supportive care; there is no evidence that VIG is effective in these cases.
3077
25
Given the rarity of fetal vaccinia, inadvertent vaccination during pregnancy is not ordinarily a reason for termination. There is no indication for prophylactic administration of VIG to the pregnant woman, but it might be considered for a viable infant born with vaccinial lesions.27,37
Prevention: Vaccinia virus can be isolated from the vaccination site as soon as a papule forms and until the scab separates, approximately two week after vaccination.9 To prevent inadvertent transmission of the live, replication-competent virus to other sites on the body or to unvaccinated individuals, the vaccination site should be covered with gauze and an overlying semipermeable membrane bandage until scabs have shed. Contact precautions and frequent hand washing are important when caring for the vaccination site. As a consequence of elevated risks of adverse events, preevent vaccination is contraindicated for individuals who have a history of atopic dermatitis or a currently disrupted skin barrier, are immunosuppressed, are allergic to any component of the vaccine, or are pregnant or breastfeeding. Vaccination is also contraindicated for individuals with household contacts who have a history of atopic dermatitis or a currently disrupted skin barrier, are immunosuppressed, or are pregnant. Preevent vaccination of individuals younger than 18 years of age is not recommended, and preevent vaccination of children younger than 1 year of age is contraindicated. The CDC also recommends against vaccination of individuals with known cardiac disease.38
MONKEYPOX
MONKEYPOX
AT-A-GLANCE
■ Monkeypox is a member of the Orthopoxvirus genus, along with variola and vaccinia.
■ Since the eradication of smallpox, monkeypox is the main Orthopoxvirus affecting human populations.39
■ Its clinical presentation is similar to that of smallpox, with a key difference being that lymphadenopathy is more common in monkeypox.39
In contrast to smallpox, which was described in writings as far back as 340 ad, monkeypox is a relatively recently recognized disease. It was first identified in 1958 as an illness of cynomolgus monkeys, hence its name. Monkeypox was first documented to cause human illness in 1970 in Zaire (the present Democratic Republic of the Congo), when it was isolated from a patient with suspected smallpox infection.39
3078
EPIDEMIOLOGY
Human monkeypox is a disease acquired mainly from infected animals. The disease is endemic to the Congo Basin of Central Africa, with the majority of human monkeypox infections occurring in the Democratic Republic of Congo, but cases are also reported in the Central African Republic, the Republic of Congo, and Sudan.39 The majority of cases are in children. Transmission occurs mainly during handling of infected animals or contact with their body fluids. Personto-person spread via respiratory droplets and close contact can occur as with smallpox, but usually in a more limited manner. Outbreaks in the Democratic Republic of Congo in 1996-1997 showed sustained human-to-human transmission for the first time, and the incidence of human monkeypox infection has been rising. This may reflect decreased immunity after the discontinuation of routine smallpox vaccination which is protective against monkeypox.4,39 In spring 2003, the first cases of human monkeypox in the Western Hemisphere were identified in the Midwest region of the United States (72 reported cases, 37 laboratory confirmed). All cases were associated with contact with infected pet prairie dogs previously housed with rodents imported from Ghana.40,41
CLINICAL FEATURES Prodrome: Similar to smallpox, symptoms of monkeypox manifest after a 7- to 17-day incubation period. A prodrome of fever, chills, malaise, headache, myalgias, and back pain occurs, lasting 1 to 4 days.39 Some individuals experience sore throat, cough, or shortness of breath. Diarrhea and abdominal pain also may be reported.4,42
Cutaneous Findings: As with ordinary smallpox, a rash generally develops 1 to 3 days after the onset of fever, initially consisting of monomorphic macules and papules. Most commonly, the eruption begins on the face and/or trunk, with the lesions spreading in a centrifugal pattern to become generalized. They then progress over 14 to 21 days to vesicles and pustules that umbilicate, crust, and desquamate (Figs. 166-15 and 166-16). Dyspigmented and pitted scars result. Monkeypox lesions can involve the oral and genital mucous membranes.43
In the outbreak in the United States, only 1 patient (a child) had a generalized rash as extensive as those seen in cases in Africa. The other affected individuals had only localized lesions, mostly on the hands, that were associated with direct contact with the infected animals from Ghana (Figs. 166-17 and 166-18). This may indicate that West African strains of monkeypox virus are less virulent than those of Central Africa.40,42
Noncutaneous Findings: Significant lymphadenopathy develops 1 to 2 days before the onset of the rash, usually in submandibular, cervical, or inguinal areas (Fig. 166-19). Conjunctivitis and keratitis may occur. Confusion and seizures are rare.44,45
Complications: Secondary skin and soft-tissue infections may occur (approximately 20% of cases). Affected individuals may also develop pneumonitis (12%), encephalitis (less than 1%), and ocular complications, including scarring with corneal lesions.43
ETIOLOGY AND PATHOGENESIS
Monkeypox is caused by the monkeypox virus, a zoonotic virus. Like variola and vaccinia viruses, it is a type of Orthopoxvirus with a brick shape on electron microscopy. The monkeypox viral genome is 96% identical to that of the variola virus at the central
25
region, which encodes essential enzymes and structural proteins. The end regions that encode virulence and host-range factors are substantially different, and the range of hosts for the monkeypox virus is much wider than that for variola virus.46 In addition to humans, hosts for monkeypox include cynomolgus and other monkeys, other primates (apes, gorillas, chimpanzees, orangutans), and nonprimate animals such as rabbits, mice, guinea pigs, rats, squirrels, and giant anteaters. Monkeypox is mainly transmitted through abraded skin after a bite or scratch from an infected animal or by contact with its infected bodily fluids. The virus multiplies locally at the site of injury and is rapidly transported to regional lymph nodes, where multiplication continues. Invasion of the bloodstream
3079
25
disseminates the virus to distant sites. The monkeypox virus is also transmissible from person to person via aerosolization of the virus or contact with lesions or body fluids during the first week of the rash, although its transmissibility is significantly lower than that of smallpox.39 Monkeypox rarely may be transmitted by contaminated fomites.47
The longest documented chain of person-to-person spread is believed to have affected 6 individuals, which suggests that monkeypox has less potential for the type of epidemic spread seen with smallpox.39
DIAGNOSIS Laboratory Testing: Leukocytosis, elevated transaminase levels, and low blood urea nitrogen levels are often seen. Lymphocytosis and thrombocytopenia occur less often.48
Pathology: On examination of skin biopsy specimens, features of monkeypox are indistinguishable from those of smallpox. There is similar dermal papillary edema, acute inflammation, and ballooning degeneration of keratinocytes (Fig. 166-20). Cytoplasmic eosinophilic inclusion bodies ( Guarnieri bodies) are also seen. Focal necrosis may occur.45
Special Tests: PCR analysis of a swab, crust, or other material can confirm monkeypox virus infection. Electron microscopy and serologic tests can confirm
3080
Orthopoxvirus infection, but cannot distinguish monkeypox from variola or vaccinia.
DIFFERENTIAL DIAGNOSIS
Varicella causes a milder and shorter/absent viral prodrome, has a centripetal distribution, and is not associated with lymphadenopathy. Orf and bovine stomatitis, caused by poxviruses of the Parapoxvirus genus, can produce similar but more localized skin lesions. Also in the differential diagnosis are drug eruptions, eczema herpeticum, and rickettsialpox (see Table 166-2). Immunocompromised individuals may develop extensive molluscum lesions that can look similar.
CLINICAL COURSE AND PROGNOSIS
In Africa, mortality ranges from 1% to 10% and mainly occurs in children. Death usually occurs during the
second week of disease and is secondary to bacterial superinfection, GI complications, or pulmonary complications. These are likely compounded by poor nutrition and inaccessibility of medical care.4,40 All individuals affected by the 2003 outbreak in the United States survived.49
Scars left by the rash may improve over time.
MANAGEMENT
Contact and droplet precautions should be instituted, and suspected cases should be isolated in a negative air pressure room if possible. Postexposure prophylaxis with vaccinia virus is the preferred treatment strategy.46 It is recommended for those within 4 days of direct exposure to monkeypox virus and should be considered up to 14 days after exposure, including in children younger than 12 months of age, pregnant women, and people with skin conditions, as the risk of contracting monkeypox is considered greater for most individuals than the risk of developing complications from vaccination.46
However, vaccination is contraindicated in individuals with severe immunodeficiency in T-cell function, even if they have been directly exposed, as their risk of severe complications from vaccination approaches or exceeds their risk from monkeypox exposure. Other treatment options include tecovirimat, which can be used under an Investigational New Drug protocol to treat monkeypox infection and is maintained in the U.S. Strategic National Stockpile.50 Tecovirimat prevents death and reduces severity of monkeypox infection in nonhuman primate models, even when administered after the appearance of clinical symptoms.21,51 Cidofovir and brincidofovir also can be used.52 However, the efficacy of these drugs against monkeypox infection in humans has not been studied and is uncertain.
Prevention: Global eradication of monkeypox is more difficult than smallpox eradication, because of the wide range of animal hosts. Vaccination with the Dryvax smallpox vaccine containing vaccinia was found to be effective in preventing human monkeypox. Observation of cases in Africa showed that vaccination was 85% protective against monkeypox, and those who were not fully protected developed only mild disease.45 The newer ACAM2000 vaccine has similar immunogenicity to Dryvax and showed equal protection against monkeypox virus in a nonhuman primate model.53,54 However, vaccination with vaccinia virus is not currently in use in monkeypox-endemic areas because the risk of severe adverse events is thought to outweigh the potential benefit.39
The CDC currently recommends preexposure vaccination for laboratory workers, investigators of monkeypox cases, and health care providers who may care for patients with monkeypox, provided they have no contraindication to smallpox vaccination (Table 166-4).46
25
Indications
■Preexposure vaccination for laboratory workers, investigators of monkeypox cases, and health care providers who may care for patients with monkeypox.
■Postexposure vaccination for those within 4 days of direct exposure to monkeypox virus; should be considered up to 14 days after exposure.
Contraindications
Contraindications
■Contraindications in the preexposure setting:
■Contraindications in the preexposure setting:
■Same as for vaccination against smallpox with vaccinia virus (see Table 166-3).
■Same as for vaccination against smallpox with vaccinia virus
(see Table 166-3).
■Contraindications in the postexposure setting:
■Contraindications in the postexposure setting:
■Severe immunodeficiency in T-cell function, defined as HIV-infected individuals with CD4 count <200 cells/µL (or age-adjusted equivalent level in children), recipients of high-dose immunosuppressive therapy, and people with lymphosarcoma, hematologic malignancies, or primary T-cell congenital immunodeficiencies.46
■Severe immunodeficiency in T-cell function, defined as
HIV-infected individuals with CD4 count <200 cells/µL (or age-adjusted equivalent level in children), recipients of high-dose immunosuppressive therapy, and people with lymphosarcoma, hematologic malignancies, or primary T-cell congenital immunodeficiencies.46
aCurrent Centers for Disease Control and Prevention (CDC) recommendations issued in 2003 and 2016.38,36
PARAPOXVIRUS INFECTIONS
The Parapoxvirus genus includes 3 viruses that produce disease in humans: pseudocowpox virus (the cause of milker’s nodule), orf virus, and bovine papular stomatitis virus. These entities, sometimes grouped together as “barnyard pox,” are clinically and histologically indistinguishable.13 They are distinguished primarily by clinical history and PCR assay. Unlike the orthopoxviruses, parapoxviruses tend to cause localized rather than systemic disease in healthy individuals. Milker’s nodule and orf are reviewed here.
MILKER’S NODULE
MILKER’S NODULE
AT-A-GLANCE
■ Milker’s nodules are caused by pseudocowpox, also known as paravaccinia, a virus transmitted by cows.
■ Lesions are clinically indistinguishable from orf and bovine papular stomatitis.
■ Unlike the Orthopoxvirus cowpox, pseudocowpox does not immunize against smallpox.1,55
EPIDEMIOLOGY
Pseudocowpox is present worldwide, but disease develops only in individuals in close contact with
3081
25
cattle. It is an occupational disease of milkers, veterinarians, and meat industry workers. Most cases are in newly employed milkers who have not developed immunity.1 Cases are mostly sporadic, but small epidemics have been reported. No natural cases of human-to-human transmission have been reported.
CLINICAL FEATURES
Paravaccinia inoculation usually occurs on the hands or, less commonly, the face. The incubation period for milker’s nodule is 4 to 7 days. In a minority of cases, the infected individual develops mild systemic symptoms, such as a transient low-grade fever.56
Cutaneous Findings: After the incubation period, 1 to several lesions usually develop. In rare cases, numerous lesions may develop. Lesions progress through 6 typical stages, each lasting approximately a week. A lesion begins as a red, and occasionally pruritic, macule that develops into a raised papule (Fig. 166-21). It evolves into a papulovesicle with a target-like appearance—a red center surrounded by a white or gray ring and outer red halo. The lesions then develop into bluish or violaceous tender nodules. Some ulcerate or have a central depression (Fig. 166-22A), which results in formation of eschars with crust. Lesions usually heal in 4 to 8 weeks and typically resolve without scarring.56
The clinical presentation of milker’s nodule is virtually identical to that of orf and bovine papular stomatitis.13,57
Noncutaneous Findings: Lymphangitis is often present in the skin surrounding the primary lesion(s). Lymphadenopathy is not common.
Complications: Secondary bacterial infection can occur but is rare. Erythema multiforme, morbilliform eruptions, and erythema nodosum have been reported in cases of milker’s nodule.
3082
A
B
ETIOLOGY AND PATHOGENESIS
Milker’s nodule is caused by the pseudocowpox virus, also known as paravaccinia, which is a member of the Parapoxvirus genus. Although historically pseudocowpox and bovine papular stomatitis sometimes were considered to be the same entity, they are genetically distinct.57 Pseudocowpox most commonly causes lesions on the teats of cows while bovine papular stomatitis most commonly causes lesions in the oral cavity.13
Humans can become accidental hosts for pseudocowpox after contacting infected animals or contaminated fresh meat. Pseudocowpox virus is transferred by direct inoculation into the skin, often through a break in the skin barrier.58 Cases of transmission from contaminated fomites to individuals with burn injury have been reported (see Fig. 166-22B).59
DIAGNOSIS Pathology: Histopathologic findings depend on the stage of the lesion. Early lesions show vacuolization and ballooning of cells in the upper third of the epidermis, which sometimes leads to multilocular vesicles. Intracytoplasmic inclusion bodies may be seen. Epidermal necrosis may be observed focally with ulceration and crust as the lesion progresses. Neutrophils are seen in the epidermis and superficial papillary dermis with epidermal necrosis. Mature lesions have finger-like
epidermal projections, papillary dermal edema, and a mixed inflammatory infiltrate that includes lymphocytes, histiocytes, and eosinophils. Regressing lesions have decreasing acanthosis and inflammation.58,60
Special Tests: When blister fluid or crusts are viewed with electron microscopy, Parapoxvirus virions typically are smaller than orthopoxviruses and have an ovoid (as opposed to brick-like) shape with a crisscross filament pattern.57 Electron microscopy cannot differentiate among Parapoxvirus species. RT-PCR can confirm Parapoxvirus genus and distinguish between pseudocowpox, orf, and bovine papular stomatitis.13,57
DIFFERENTIAL DIAGNOSIS
Milker’s nodules are clinically indistinguishable from orf and bovine papular stomatitis, but clinical history helps with differentiation: cattle are the source of infection for milker’s nodules and bovine papular stomatitis while sheep or goats are the source of infection for orf. PCR can distinguish among the 3 viruses. Milker’s nodules must also be differentiated from the Orthopoxvirus cowpox. Cowpox is very rare in humans and, contrary to its name, is rarely transmitted from cows. It has a longer incubation period and causes more pain and lymphadenopathy. It is a moresevere infection that may cause death in individuals who have atopic dermatitis or are immunocompromised. Large lesions of milker’s nodule also can be confused with anthrax, pyogenic granuloma, giant herpetic lesions, and keratoacanthoma (Table 166-5).
Most Likely
■Few to multiple lesions
■Bovine papular stomatitis
■Cowpox
■Herpetic whitlow
■Solitary lesion
■Pyogenic granuloma
■Pyoderma
Consider
■Few to multiple lesions
■Atypical mycobacterial infection
■Sporotrichosis
■Solitary lesion
■Tularemia
■Giant herpetic lesion
■Giant molluscum
■Erysipeloid
Always Rule Out
Always Rule Out
■Few to multiple lesions
■Few to multiple lesions
■Anthrax
■Anthrax
■Primary inoculation tuberculosis
■Primary inoculation tuberculosis
■Solitary lesion
■Solitary lesion
■Keratoacanthoma
■Keratoacanthoma
■Syphilitic chancre
■Syphilitic chancre
25
CLINICAL COURSE AND PROGNOSIS
Milker’s nodule is a self-limited illness. Most cases heal without scarring. Infection does not produce lifelong immunity; up to 12% of individuals have second infections.57
MANAGEMENT
Because the disease is self-limited, treatment, if needed, is symptomatic. Surgical curettage of large lesions may help speed healing.61
Prevention: As discussed above, there is no crossimmunity between orthopoxviruses and parapoxviruses, so smallpox vaccination does not prevent milker’s nodules. Prevention mainly consists of isolation of infected animals and contact precautions.
ORF
ORF
AT-A-GLANCE
■ Orf virus is usually transmitted to humans from sheep or goats.
■ Orf infection looks similar to milker’s nodule and progresses through similar clinical stages before resolving spontaneously.
Orf, also known as contagious pustular dermatosis, infectious pustular dermatitis, scabby mouth disease, and sore mouth disease, is a self-limited zoonotic viral infection that usually affects the hands of people handling infected animals. The disease is endemic in sheep and goats, and it is transmitted to humans through contact with infected tissue or fomites. Orf shares clinical characteristics with milker’s nodule and bovine papular stomatitis. It may be mistaken for more serious and life-threatening disorders such as tularemia, anthrax, and erysipeloid (see Table 166-5). The name orf is derived from the Nordic word Hrufa, meaning boil or scab.59 Walley first identified orf as a contagious disease in sheep in 1890, and Newson and Cross first described the disease in humans in 1934.59
EPIDEMIOLOGY
Orf virus is a member of the Parapoxvirus genus, which also includes pseudocowpox and bovine papular stomatitis. Although sheep and goats are the most common sources of infection, the virus also has been found in mountain goats, gazelles, musk oxen, and reindeer. The nostrils and lips of infected animals are
3083
25
affected, as well as the teats of ewes suckling young. Human disease is most often seen in farmers, shepherds, veterinarians, and butchers, but anyone who has contact with small ruminants is at risk.62 The disease has been reported in children with exposure to farms or petting zoos.63 Humans develop disease after contact with animals or fomites such as barn doors, feeding troughs, wire fencing, bottles, and harnesses. Multiple cases of orf infection following the Muslim feast of the sacrifice (Eid al-Adha), during which lambs are slaughtered, have been reported.64 According to the CDC, the disease is not transmitted from human to human.
CLINICAL FEATURES Cutaneous Findings: Orf lesions usually develop on the hands but can occur anywhere, including the face and perianal area.61,65 A solitary lesion is the most common presentation, but multiple lesions are possible.65
As with milker’s nodule lesions, orf lesions evolve through 6 clinical stages, each lasting roughly 1 week (Table 166-6).65,66 A red macule appears a few days after inoculation and develops into a red papule by 1 week after the inoculation. During the second week, the lesion evolves into a targetoid nodule with a red papule surrounded by a white ring and enclosed by a peripheral halo of erythema (Fig. 166-23). During the third week, considered the acute stage, the lesion becomes weepy (Fig. 166-24). It may appear as a flattopped, crusted, hemorrhagic pustule 2 to 3 cm in
TIME AFTER EXPOSURE CLINICAL MANIFESTATIONS
3-7 days 1-4 papules on hand (typically only 1 lesion): begin as a red maculopapular lesion
↓
Vesicle
↓
10-14 days Target lesion with red center, white middle ring, and red halo
↓
14-21 days Acute weeping stage
↓
21-28 days Regenerative dry stage with black dots
↓
28-35 days Papillomatous stage
↓
35 days Regressive stage with dry crust and
35 days Regressive stage with dry crust and eventual shedding of the scab
eventual shedding of the scab
Adapted from Clark J, Diven D. Poxviruses. In: Tyring SK, Moore AY, Lupi O, eds. Mucocutaneous Manifestations of Viral Diseases. 2nd ed. London, UK: Informa Healthcare; 2010:51, with permission.
3084
diameter (Fig. 166-25A).59 During the fourth week, the lesion enters the regenerative stage, during which it dries out and black dots composed of pyknotic cells form on its surface (Fig. 166-25B). During the fifth week, papillomas develop on the surface of the lesion. In the final, regressive stage, a dry crust forms at the periphery of the lesion and gradually extends centrally. The crust may shed and reform several times before the lesion flattens and heals.65 Lesions are typically painless.59
Noncutaneous Findings: Systemic findings are uncommon in immunocompetent individuals but can include lymphadenopathy and lymphangitis. Rarely, fever and malaise may occur.65
Complications: Orf lesions can become secondarily infected.67 An estimated 7% to 18% of individuals with orf infections develop erythema multiforme.68
Vesiculopapular, papular (see Fig. 166-25A), and bullous-pemphigoid like eruptions also may develop.69,70
A
B
Additionally, secondary spread within active atopic dermatitis skin lesions has been reported.71 Rare complications include giant orf lesions and Stevens-Johnson syndrome.62,72
ETIOLOGY AND PATHOGENESIS
Orf is an ovoid crosshatched particle approximately 250 nm long × 150 nm wide.64 The virus is very stable and can survive heating, drying, and solvents. It is transmitted to humans from animals or fomites through a crack in the skin and replicates within the epidermis. Orf virus encodes immunomodulatory genes that interfere with host response and allow time for viral replication within epidermal cells. Orf virus interferon resistance protein and virus interleukin-10 inhibit interferon and inflammatory cytokine production. Additionally, granulocyte-macrophage colony-stimulating factor inhibitory factor inhibits the biologic activity of granulocyte-macrophage colony-stimulating factor and interleukin-2.73 Clearance of the infection occurs
25
when host immune response eventually overcomes orf’s immunomodulatory proteins.
Risk Factors: Exposure to infected animals is the greatest risk factor for orf infection. Infections tend to occur most often during the spring and summer months, which is lambing season, as young animals are most susceptible to infection.63 Vaccination of sheep with a commercially available unattenuated, live orf vaccine with the intent of conferring immunity is a risk factor for humans.63
Immunocompromised individuals have an increased risk of developing giant (greater than 3 cm in diameter) orf lesions and may have difficulty clearing them.63,74
DIAGNOSIS
Clinical appearance and history of ungulate exposure are usually diagnostic. Dermoscopy of orf lesions shows central ulceration surrounded by white structureless areas, white shiny streaks, dotted and hairpin vessels, and fine peripheral scale.75
Pathology: In the maculopapular and target stages, intranuclear and intracytoplasmic inclusions are present in vacuolated epidermal cells, with an accumulation of neutrophils, basophils, dendritic cells, and lymphocytes (Fig. 166-26). During the acute stage, multilocular vesicles form and the epidermis degenerates. Papillomatosis and acanthosis subsequently develop, and marked finger-like downward projections of the epidermis may be seen (Fig. 166-27).65
Special Tests: RT-PCR testing, which is available through the CDC, is the most rapid and accurate way
3085
25
to make the diagnosis when clinical uncertainty exists. Electron microscopy cannot definitively distinguish between Orthopoxvirus and Parapoxvirus.
DIFFERENTIAL DIAGNOSIS
A variety of bacterial and infectious diseases can present with findings similar to those of orf (see Table 166-5). Milker’s nodule and bovine papular stomatitis are clinically and histologically indistinguishable from orf, but are associated with different animal exposure. The lesion of anthrax is more hemorrhagic with rapid progression to an eschar. Herpetic whitlow may resemble orf but tends to be more painful. Tularemia and syphilis are associated with chancres. Sporotrichosis begins as a single necrotic nodule but is followed by multiple nodules arising in a linear fashion along the lymphatics. Primary inoculation tuberculosis and atypical mycobacterial infection can give rise to ulcerative lesions that may take months to years to heal.
CLINICAL COURSE AND PROGNOSIS
Orf usually resolves within 4 to 6 weeks without treatment. Typically, scarring does not occur. Immunocompromised individuals can develop progressive, destructive lesions that may require interventions such as debridement, antiviral therapy such as cidofovir cream, or imiquimod topical immunomodulatory therapy.63,74,76 Recurrence is uncommon but has been reported.74
MANAGEMENT
Supportive care is the most appropriate intervention for immunocompetent patients. Application of compresses, culture of lesion specimens, and antibiotic coverage may be appropriate if secondary bacterial infection is suspected. Immunocompromised patients may require medical intervention, as described above.
3086
Prevention: Barrier precautions, such as use of gloves and good hand hygiene, help prevent orf infection. Individuals with an impaired skin barrier from either abrasions or intrinsic skin disease (eg, atopic dermatitis) should be particularly vigilant about avoiding contact with infected animals or potential fomites.
MOLLUSCIPOXVIRUS INFECTION: MOLLUSCUM CONTAGIOSUM
AT-A-GLANCE
■ Molluscum contagiosum is a common benign cutaneous infection with associated signs isolated to the skin.
■ Children are most commonly affected.
■ Severe inflammatory responses can occur at the site of the lesions, which are sometimes mistaken for secondary bacterial infection or cellulitis.
■ A number of associated skin findings, including eczematous reactions surrounding the lesions, more diffuse autoeczematization-type reactions, or lichenoid, Gianotti-Crosti type lesions may develop.
Molluscum contagiosum (MC) is a common benign cutaneous viral infection specific to humans that occurs worldwide and is transmitted by skin-to-skincontact. Since the eradication of smallpox, MC virus is the primary poxvirus affecting humans.77
MC infection was first described clinically by Bateman in 1817. Henderson and Paterson identified its characteristic intracytoplasmic viral inclusion bodies in 1841.78
EPIDEMIOLOGY
MC infection most commonly affects children, sexually active adults, athletes participating in contact sports, and individuals with impaired cellular immunity.77 The infection is most prevalent before the age of 14 years, with a median age of 5 years in a retrospective study of 170 children at Johns Hopkins.79,80 A metaanalysis estimates that 5.1% to 11.5% of children ages 0 to 16 years are affected at any given time, but true prevalence is likely higher, as some infections may be subclinical.79
Seropositivity to MC virion surface protein in unaffected individuals ranges from 6% in Japan to approximately 30% in the United Kingdom.81,82
MC lesions are mainly limited to the skin, but rarely develop on mucosal surfaces, including the eye.77 In children, lesions are usually on exposed areas, whereas in adults, many cases are limited to the genital area,
suggesting sexual transmission.83 Genital and perianal lesions can also develop in children, but are rarely associated with sexual transmission in this age group.84
The prevalence of sexually transmitted MC infections in adults has risen over the past several decades, with a large Spanish study noting a threefold increase in the yearly incidence (from 1.3% to 4%) in a sexually transmitted disease unit between 1988 and 2007.85 An earlier study showed an 11-fold increase in patient visits for MC in the United States between 1966 and
1983. One theorized explanation is that reduced transmission in childhood may result in more adults who are immunologically naïve and vulnerable to sexual transmission.85
MC infections are more common in individuals infected with HIV. Data from the 1980s and early 1990s suggested a prevalence of 5% to 18% in this population, but with the increased use of antiretroviral therapy, the rate may now be lower.86
Transmission may occur via direct skin or mucous membrane contact, or via fomites. Bath towels, swimming pools, and public or shared baths are reported as sources of infection.87 Autoinoculation and koebnerization also play a role in the spread of lesions. Vertical transmission from mother to neonate during the intrapartum period has been reported.88,89
MC lives in the epidermis and does not remain latent in the body after the cutaneous lesions have cleared.77
CLINICAL FEATURES Cutaneous Findings: MC often presents as small pink, pearly, or skin-colored papules that enlarge to 2 to 5 mm in size. As they enlarge they may become flat-topped, dome-shaped, and opalescent. Lesions may have a central dell or umbilication (Fig. 166-28A),
A B
25
from which a white curd-like substance containing the virus can be expressed with pressure. Children usually develop multiple papules, often in exposed sites like the face and extremities or intertriginous sites, such as the axillae and popliteal fossae. Lesions may be grouped in clusters or appear in a linear array. The latter often results from koebnerization or development of lesions at sites of trauma. In adults, lesions typically develop in the genital area. Immunosuppressed patients typically have moresevere and extensive disease, and may develop giant molluscum as large as 2.5 cm in diameter.90,91
Noncutaneous Findings: MC is not associated with systemic complications. Complications: Although many patients are asymptomatic, pruritus may be a significant problem, particularly in those patients with underlying atopic dermatitis. Chronic conjunctivitis and punctate keratitis may develop in patients with eyelid lesions. Secondary bacterial infection can occur, particularly if patients scratch their lesions. Approximately 19% to 39% of children with MC develop an erythematous, eczematous dermatitis surrounding their molluscum lesions, known as molluscum dermatitis.87,92 This is more common in children with atopic dermatitis; roughly half of children with both atopic dermatitis and MC develop molluscum dermatitis.92
In approximately 20% of patients, molluscum lesions may become inflamed, with erythema and swelling (see Fig. 166-28B), and these inflamed lesions may become pustular or fluctuant.87,92 The development of inflamed MC lesions suggests a robust immune response and tends to be associated with a subsequent decline in the number of lesions.92
3087
25
A small subset of individuals with MC develop a Gianotti-Crosti–like reaction consisting of pruritic monomorphous, edematous, erythematous papules or papulovesicles, centered on the elbows and knees, which lasts for several weeks. This eruption also tends to be followed by reduction in the number of MC lesions and may be considered a favorable prognostic sign.92
ETIOLOGY AND PATHOGENESIS
MC virus is a large, brick-shaped double-stranded DNA poxvirus with genomic similarities to other poxviruses. It shares two-thirds of the viral genes of vaccinia and variola viruses.80 There are 4 clinically indistinguishable subtypes of MC virus. MC virus genotype 1 is responsible for 98% of disease in the United States.93,94 MC virus genotype 2 is primarily seen in adults and immunocompromised individuals and is most commonly transmitted by sexual contact. The incubation period of the virus estimated to be approximately 2 to 6 weeks.95
MC virus replicates in the cytoplasm of epithelial cells. Viral inclusion bodies known as Henderson- Paterson bodies develop in the basal layer of the epidermis and enlarge as cells rise through the epidermis, pushing cellular organelles against the sides of the cell.90 Proliferation and enlargement of the virionpacked cells causes disintegration of the stratum corneum and the formation of a dimple-like ostium through which the virions are released when the inclusion bodies rupture.90
Molluscum lesions can persist for a long time without significant inflammatory cell infiltration because the MC virus possesses multiple genes that impede host immune response.90 These include genes coding for (a) a homolog of a major histocompatibility class 1 heavy chain, which may interfere with antigen presentation; (b) a chemokine homolog that inhibits chemotaxis; (c) a protein that inhibits apoptosis by preventing activation of the death effector domain of caspase 8; and (d) a glutathione peroxidase homolog that prevents apoptosis in cells damaged by ultraviolet radiation and hydrogen peroxide.77,90,96 Eventually the immune system detects the virus and mounts a localized response involving plasmacytoid dendritic cells, interferon-induced dendritic cells, natural killer cells, and cytotoxic T lymphocytes, ultimately clearing the infection.97
Risk Factors: A 2014 metaanalysis of risk factors found an association between recent history of swimming and development of MC, with the relative risk of MC among swimmers approximately twice that of nonswimmers.98
Altered skin barrier function and immunity in atopic dermatitis may be a risk factor for MC, with 18% to 47% of MC patients having a history of atopic dermatitis.80,92,99-101 Atopic dermatitis may be somewhat overrepresented because children with atopic dermatitis may be assessed by physicians more often than those without, in whom molluscum may go undiagnosed.99 Individuals with atopic dermatitis
3088
may have more widespread involvement and pruritus, as well as increased risk of developing molluscum dermatitis.80,101
HIV is a risk factor for MC infection, and affected individuals are at higher risk for extensive prolonged disease.102 MC infection is associated with a CD4+ count of <200 cells/µL.103 Additionally, MC eruption can occur in association with immune reconstitution inflammatory syndrome after initiation of antiretroviral therapy.104
Individuals with a DOCK8 (dedicator of cytokinesis 8) mutation, which results in T-cell and B-cell deficiency, are at risk for extensive molluscum infections.90,105
Patients receiving immunosuppressive medications for organ transplants or other indications also have increased risk. MC infections have been reported in patients taking methotrexate, alone or in combination with a tumor necrosis factor-α inhibitor or cyclosporine, for treatment of Crohn disease, mycosis fungoides, mixed connective tissue disease, psoriasis, and exfoliative dermatitis.106 Additionally, treatment with Janus kinase inhibitors and fingolimod also are implicated in the development of MC virus infections.107,108
DIAGNOSIS
Clinical diagnosis is usually straightforward and can be aided by dermoscopic examination where MC lesions typically have a central polylobular white-yellow amorphous structure surrounded by a peripheral crown of blood vessels (red corona).109,110 The appearance corresponds to hyperplastic squamous epithelium expanding into the dermis, separated by septae of compressed dermis.109 Punctiform, radial, and mixed patterns also may be seen.111
Pathology: Evaluation of the central contents of the lesion using a crush preparation and Wright or Giemsa staining can be carried out when necessary (Fig. 166-29). Histopathologic examination reveals a hypertrophied and hyperplastic epidermis. Above the
basal layer, enlarged cells containing large, intracytoplasmic inclusions (Henderson-Paterson bodies) can be seen (Fig. 166-30).
Special Tests: PCR confirmation can be performed but is usually not necessary.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis includes verrucae, pyogenic granulomas, amelanotic melanoma, basal cell carcinomas, and appendageal tumors. Fungal infections caused by Cryptococcus, histoplasmosis, and Penicillium must be considered in immunocompromised hosts (Table 166-7).
Most Likely
■Verrucae
Consider
■Pyogenic granuloma
■Papular granuloma annulare
■Epidermal inclusion cyst
■Sebaceous hyperplasia
Always Rule Out
Always Rule Out
■Appendageal tumors
■Appendageal tumors
■Basal cell carcinoma
■Basal cell carcinoma
■Amelanotic melanoma
■Amelanotic melanoma
■Cryptococcosis/histoplasmosis/penicilliosis
■Cryptococcosis/histoplasmosis/penicilliosis
25
CLINICAL COURSE AND PROGNOSIS
MC infections typically resolve spontaneously within months to years. Each individual lesion lasts approximately 2 months, but the total duration of infection is longer because lesions spread by autoinoculation.90
In the largest prospective cohort of children with MC infection, the average duration was 13.3 months.112 A retrospective review of 170 children with MC evaluated in the Division of Pediatric Dermatology at the Johns Hopkins Children’s Center found that treatment did not shorten time to resolution.80 Lesions typically resolve without scarring, but scratching or destructive treatments may result in scarring. In patients infected with HIV, MC may resolve with initiation of antiretroviral therapy and improvement in CD4 cell counts.102
MANAGEMENT
It is important to discuss the risks and benefits of individual therapies with families before embarking on treatment of this essentially benign condition, which typically resolves without complication in the immunocompetent individual. For some children, no treatment is the best option as the child’s native immune response may clear the MC without additional intervention. Nevertheless, treatment may be warranted for persistent, pruritic, spreading, or cosmetically undesirable lesions, as well as to prevent autoinoculation or transmission to others.113 However, robust analysis of the comparative efficacy of treatments is lacking. A 2017 Cochrane Database analysis of treatments for MC identified only 22 randomized controlled trials of MC treatments and concluded that no single intervention is convincingly effective for the treatment of MC.114 The analysis did not include several therapies commonly used by pediatric dermatologists because of insufficient data.113,115
In the absence of compelling evidence for the superiority of any particular treatment, multiple therapies are used, including destructive, immunomodulatory, cytotoxic, and antiviral therapies.113
Physically destructive therapies include curettage, cryotherapy, CO2 laser, pulsed-dye laser, and electrodessication.116 They may work by rupturing the intracytoplasmic sacs containing MC viral proteins and triggering an immunologic response that clears the infection.77
Chemically destructive therapies include potassium hydroxide, silver nitrate, trichloracetic acid, phenol, and the blistering agent cantharidin, which is likely the most commonly used therapy.77,115,117 Cantharidin 0.7% in a collodion base is applied to the lesions and washed off after 2 to 6 hours.118 This substance, which was originally extracted from the blister beetle, causes dissolution of desmosomal plaques, resulting in acantholysis and intraepidermal blistering, with extrusion of the molluscum bodies.118,119 Cantharidin is the preferred treatment for children because it is painless at time of application, in contrast with curettage and cryotherapy, which are painful and may be traumatic for children. However, families must be counseled regarding the small risk of
3089
25
extreme reaction or scarring, and cantharidin should not be used on the thin skin of the face and genital areas. MC typically resolves after an average of 2.1 treatments with cantharidin.120 A randomized controlled trial of cantharidin treatment versus placebo for treatment of MC that was published in 2014 found no significant difference, but was limited by sample size and short duration of follow up.117,121 Parent and physician satisfaction with the therapy is high; 78% to 95% of parents say they would use cantharidin treatment again for molluscum reoccurrence.120,122,123
Immunomodulatory therapies include intralesional interferon-α or interferon-β, intralesional Candida antigen injection, cimetidine, and imiquimod.77,90 Oral cimetidine has been used with some success, although evidence is contradictory.124,125 Although imiquimod cream is favored by some physicians and may be effective for genital lesions, randomized controlled trials have found it ineffective in children.115,126-129
The cytotoxic therapy podophyllotoxin and antiviral therapy cidofovir, which can be administered topically or IV, are also used. For genital molluscum, the 2014 United Kingdom national guidelines recommend either nontreatment or treatment with podophyllotoxin 0.5%, imiquimod 5% cream, or liquid nitrogen therapy.130 Podophyllotoxin and imiquimod should be avoided during pregnancy and breastfeeding.130
Immunosuppressed patients may be unresponsive to traditional therapies. Treatment of the underlying disease is thought to be the most effective therapy for resolving MC infection. In HIV patients, MC infection may improve as CD4 count rises. A recent systematic review of 13 studies found little evidence to support any particular intervention for MC in HIV.102 Combination therapies may be tried.77 Some clinicians recommend that adolescents and adults with new-onset MC infection undergo evaluation for HIV infection and/or other causes of an immunocompromised state.83
Medium-strength topical steroids sometimes are used to treat molluscum dermatitis and Gianotti- Crosti–like reactions. Data on whether treating these secondary eruptions raises the risk of MC recurrence are contradictory, and this issue needs further study.87,92
Prevention/Screening: Spread through autoinoculation can be reduced by treating existing lesions, avoiding scratching, and using antipruritics as necessary. As mentioned above, treating molluscum dermatitis with topical steroids may reduce autoinoculation via scratching but potentially raises the risk of relapse by dampening the immune response to molluscum, and should be considered on a case-by-case basis until studied further.87,92
MC infection should not prevent children from attending school or playing sports.131 To prevent spread to others, the CDC advises covering lesions that could contact other individuals with clothing or bandages. This is especially important when participating in contact sports and sharing equipment like helmets and baseball gloves. The CDC recommends avoiding swimming unless all lesions can be covered by watertight bandages.
3090
ACKNOWLEDGMENTS
The authors acknowledge the contributions of Drs. Caroline Piggott and Wynnis Tom, former authors of this chapter.

Figure 166-1 Day 3 of rash in a young woman with smallpox, with fluid accumulating in several vesicles. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA.)

Figure 166-2 Pustular smallpox lesions with characteristic highest density on the face and extremities. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA.)

Figure 166-3 Crusted lesions on the foot at day 21 of the rash of smallpox. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by Paul B. Dean, MD.)

Figure 166-4 Scars and pockmarks remain after the crusts have fallen off. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by J. Noble, Jr., MD.)
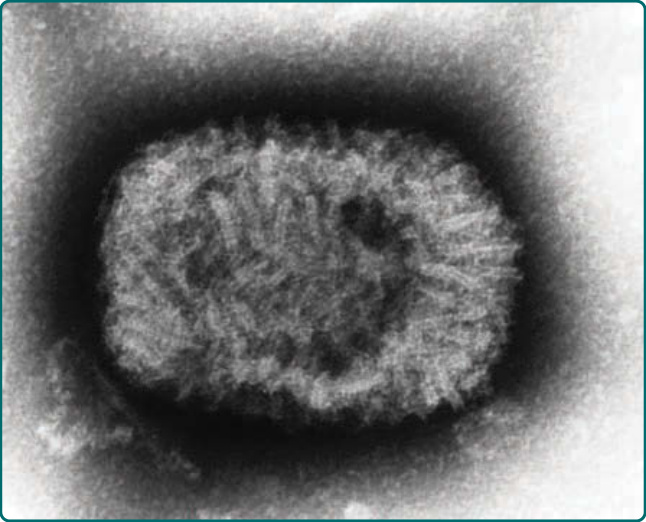
Figure 166-5 Electron micrograph of the variola virus. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by J. Nakano.)
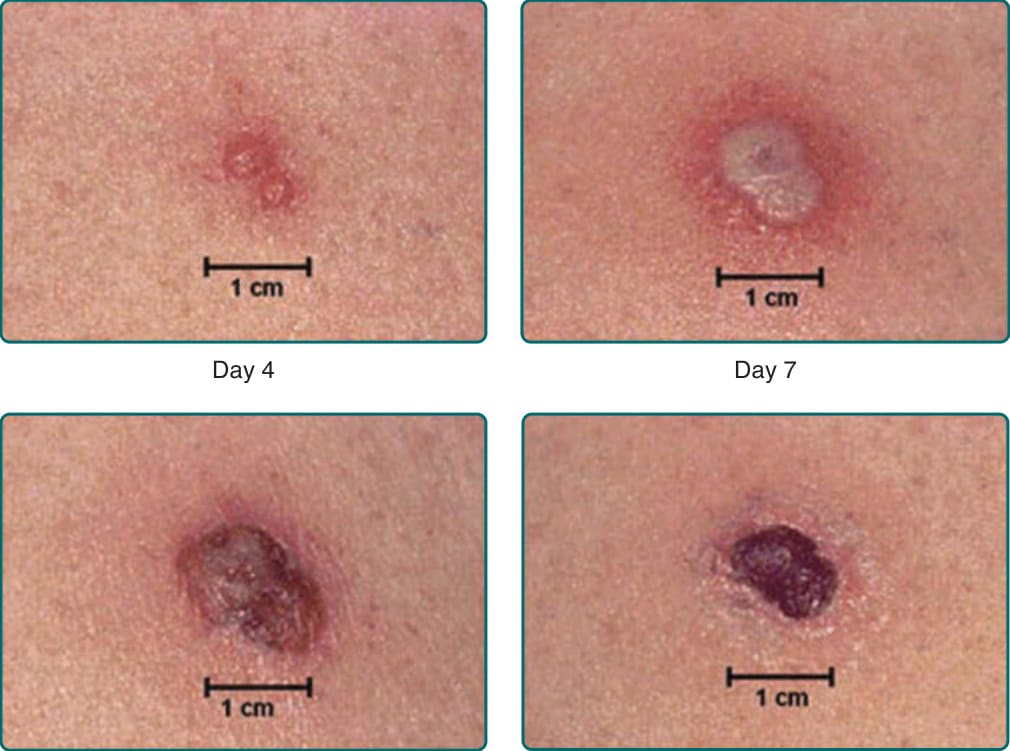
Figure 166-6 Normal progression seen at the smallpox vaccination site. (From the Centers for Disease Control and Prevention [CDC], Atlanta, GA, USA.)

Figure 166-7 A robust take after smallpox vaccination. (From the Centers for Disease Control and Prevention [CDC], Atlanta, GA, USA.)

Figure 166-8 Inadvertent inoculation of vaccinia to the eyelid. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by Michael Lane, MD.)

Figure 166-9 Generalized vaccinia in an 8-month-old infant. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by Allen W. Mathies, MD of the California Emergency Preparedness Office, Immunization Branch.)
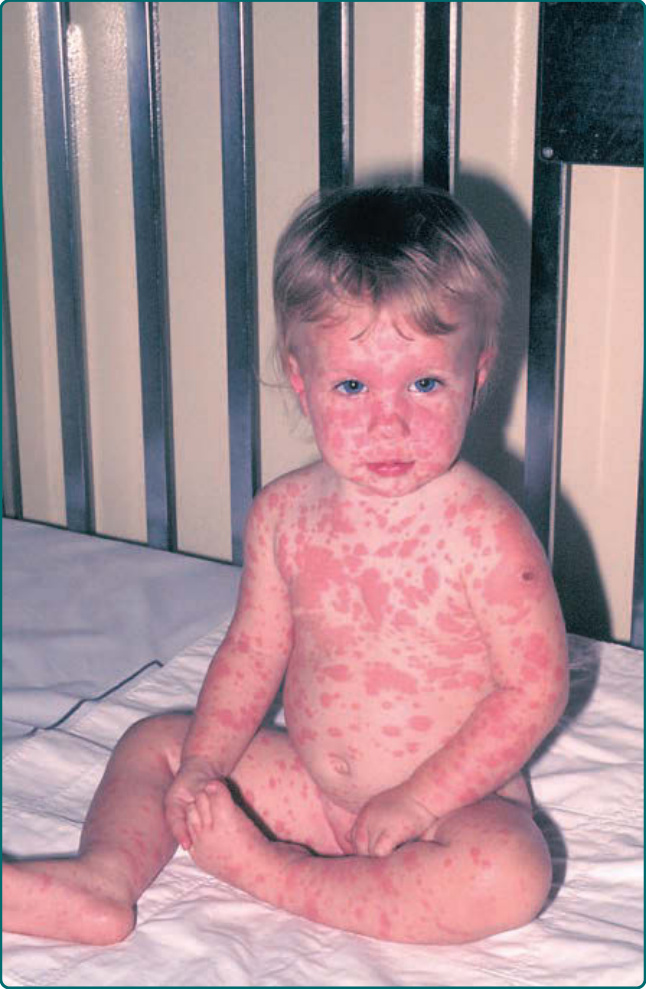
Figure 166-10 Erythema multiforme following vaccination in a 1-year-old child. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by Allen W. Mathies, MD and John Leedom, MD of the California Emergency Preparedness Office, Immunization Branch.)

Figure 166-11 Eczema vaccinatum with lesions in areas of active dermatitis.

Figure 166-12 A 22-month-old male with Bruton hypogammaglobulinemia developed progressive vaccinia. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by Arthur E. Kaye, MD.)
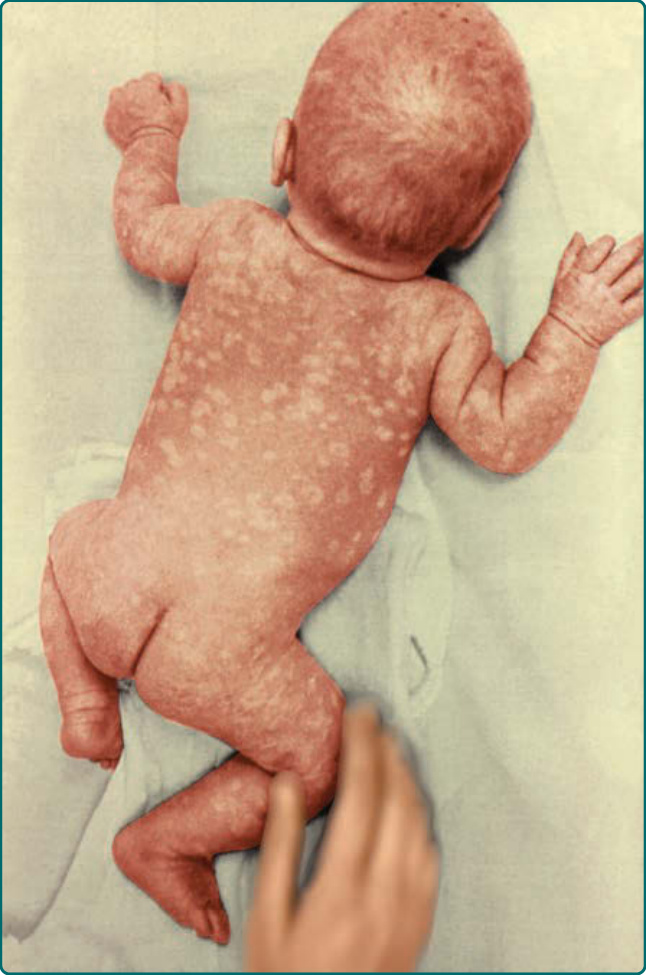
Figure 166-13 Extensive scarring in an otherwise healthy infant from contracting vaccinia in utero. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by Arthur E. Kaye, MD.)

Figure 166-14 Bifurcated needle used for smallpox vaccination. (From the Centers for Disease Control and Prevention [CDC] Public Health Image Library, Atlanta, GA, USA, and contributed by James Gathany.)
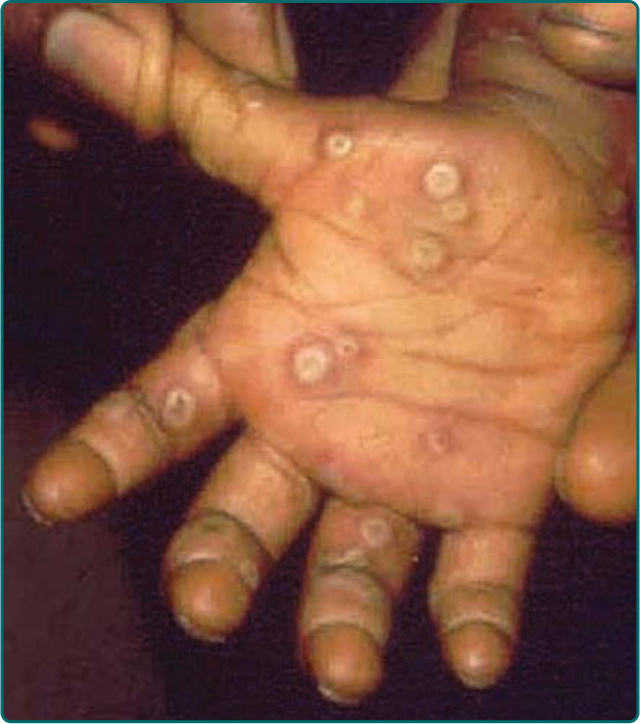
Figure 166-15 Umbilicated pustular lesions on the palm from monkeypox. (Used with permission from the Joint Pathology Center, Silver Spring, MD, USA.)

Figure 166-16 A 5-year-old male from the Democratic Republic of Congo with late desquamative monkeypox lesions. (Used with permission from the Joint Pathology Center, Silver Spring, MD, USA.)

Figure 166-17 The primary inoculation site of monkeypox virus in a 3-year-old child, 14 days after being bitten by a prairie dog. (Copyright © Marshfield Clinic, Inc. All rights reserved. Reprinted with permission from Marshfield Clinic, Inc., Marshfield, WI, USA.)

Figure 166-18 Monkeypox lesions resolving in the same 3-year-old child. (Copyright © Marshfield Clinic, Inc. All rights reserved. Reprinted with permission from Marshfield Clinic, Inc., Marshfield, WI, USA.)
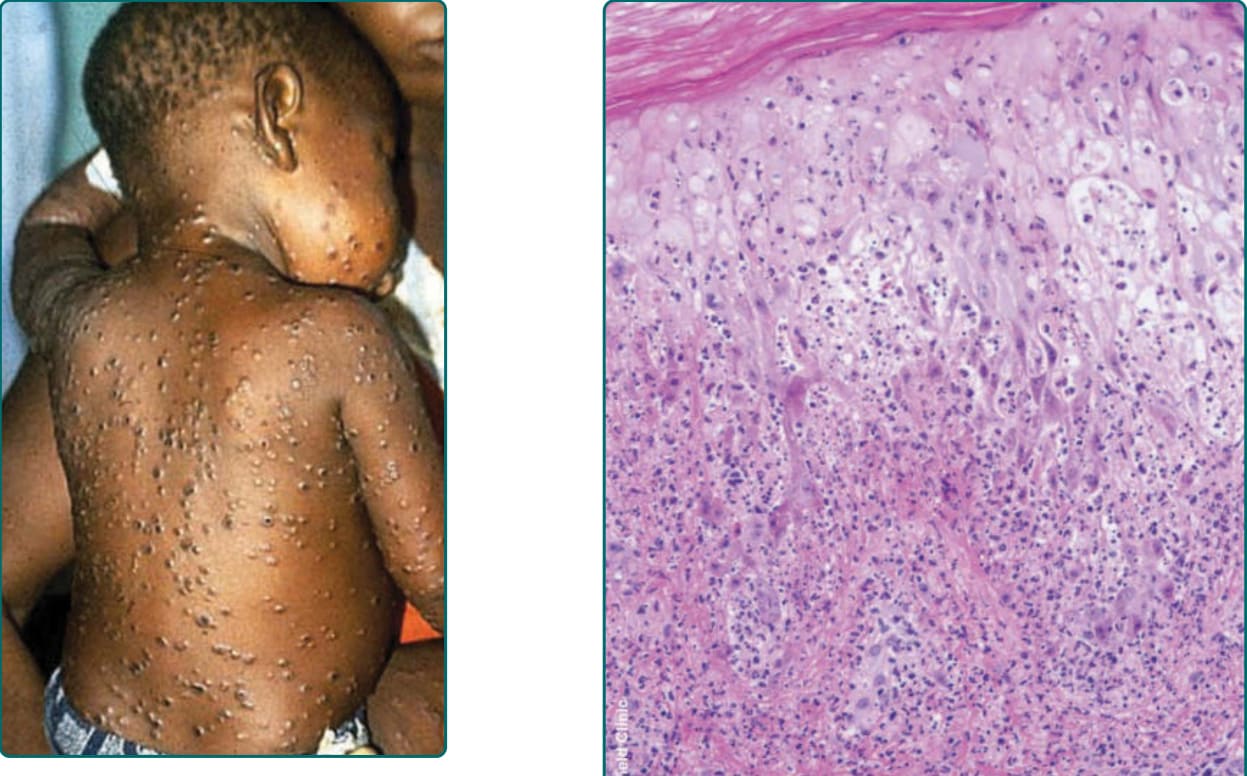
Figure 166-19 Significant postauricular lymphadenopathy with pustular skin lesions in a 2-year-old female with monkeypox. (Used with permission from the Joint Pathology Center, Silver Spring, MD, USA.)
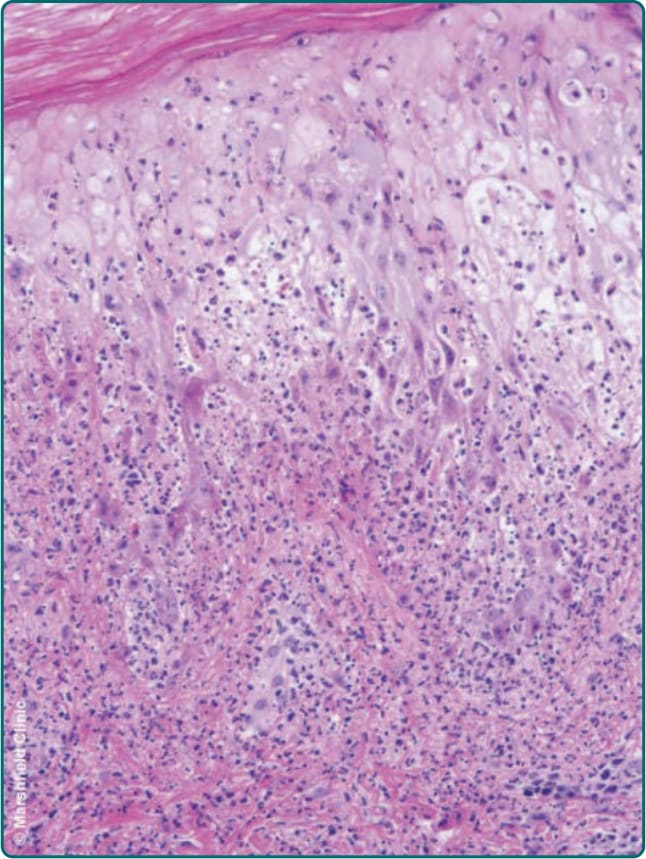
Figure 166-20 Histopathology of a monkeypox lesion with dermal papillary edema, acute inflammation, and ballooning degeneration of keratinocytes. (hematoxylin and eosin [H&E]. (Copyright © Marshfield Clinic, Inc. All rights reserved. Reprinted with permission from Marshfield Clinic, Inc., Marshfield, WI, USA.)

Figure 166-21 A milker’s nodule on the hand. (From the National Institute for Occupational Safety and Health [NIOSH], Atlanta, GA, USA, with permission.)
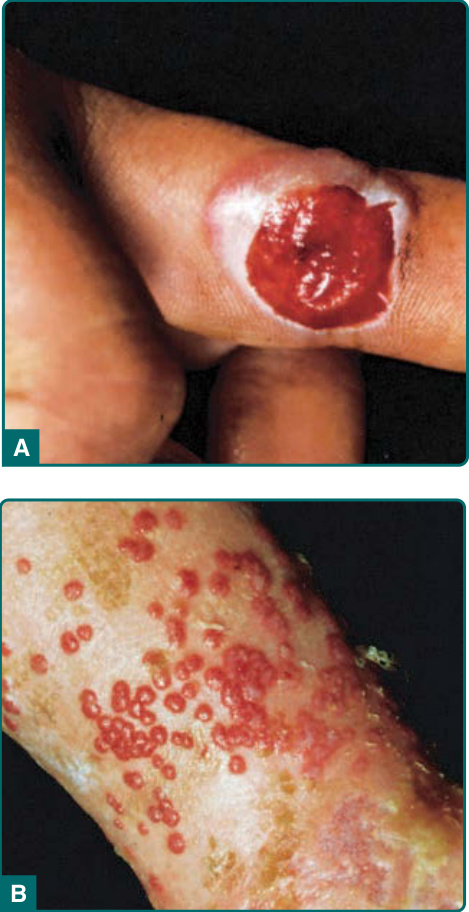
Figure 166-22 A, Firm, eroded milker’s nodule. B, Multiple lesions at the site of a second-degree scalding burn sustained in a milking barn.

Figure 166-23 The target phase of orf shows a white circle with central and peripheral erythema.
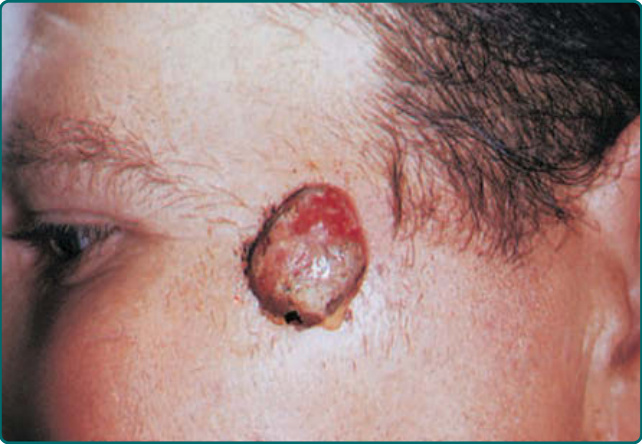
Figure 166-24 In the acute phase, there is weeping of the surface overlying an elevated tumor.

Figure 166-25 A, Multiple orf papulonodules with unusually extensive hemorrhagic crust during the acute weeping stage, 16 days after a goat bite to multiple fingers. A diffuse papular eruption that developed after the primary orf lesions is also visible. B, Twenty-two days after the goat bite, the primary orf lesions have begun to dry out and flatten, and the secondary eruption is resolving. (Used with permission from Victoria R. Barrio, MD.)
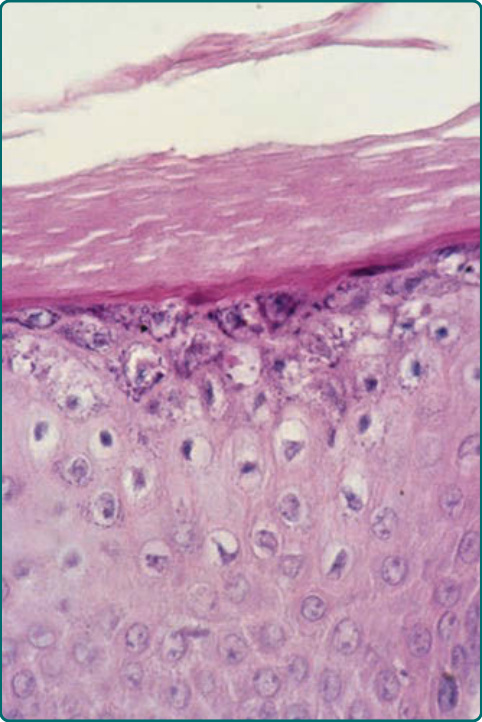
Figure 166-26 Orf histopathology. In the target phase, there are superficial vacuolated epidermal cells with inclusion bodies.
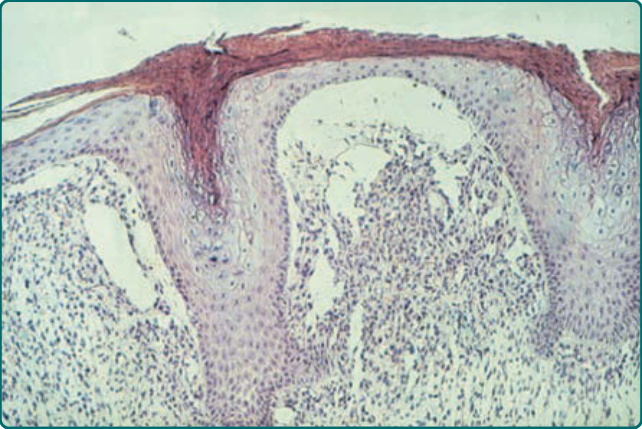
Figure 166-27 Orf histopathology. Later in the target stage, there are finger-like projections of the epidermis and a dense inflammatory infiltrate accompanied by massive edema in the papillary body.

Figure 166-28 Molluscum contagiosum. A, Discrete, solid, skin-colored papules, 1 to 2 mm in diameter with central umbilication. B, Multiple, scattered, and discrete lesions, some of which are inflamed.
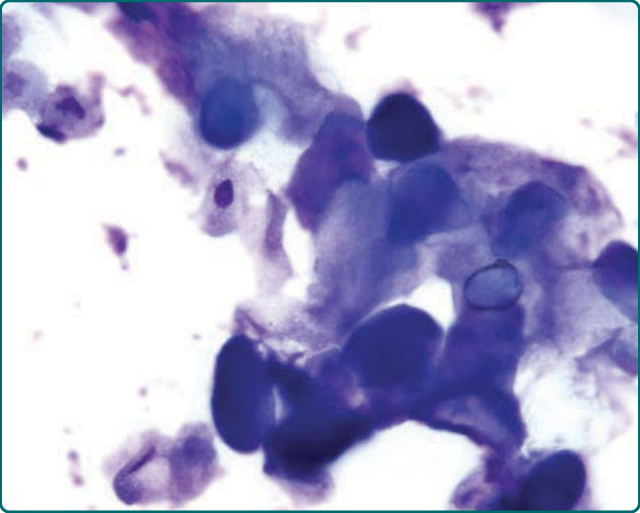
Figure 166-29 Microscopic examination (Giemsa stain) of cellular material from the area of central umbilication shows intracytoplasmic molluscum inclusion bodies.
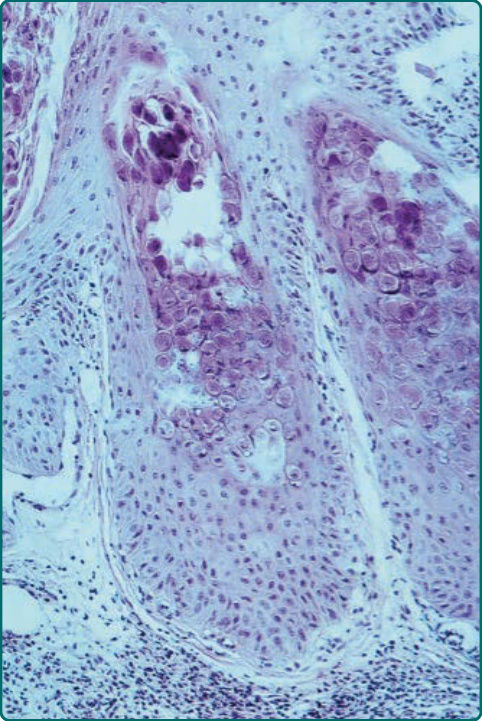
Figure 166-30 Molluscum contagiosum. Histopathology (skin biopsy, hematoxylin and eosin [H&E]) shows downgrowth of infected epidermal cells bearing large eosinophilic cytoplasmic inclusion bodies (Henderson-Paterson bodies).
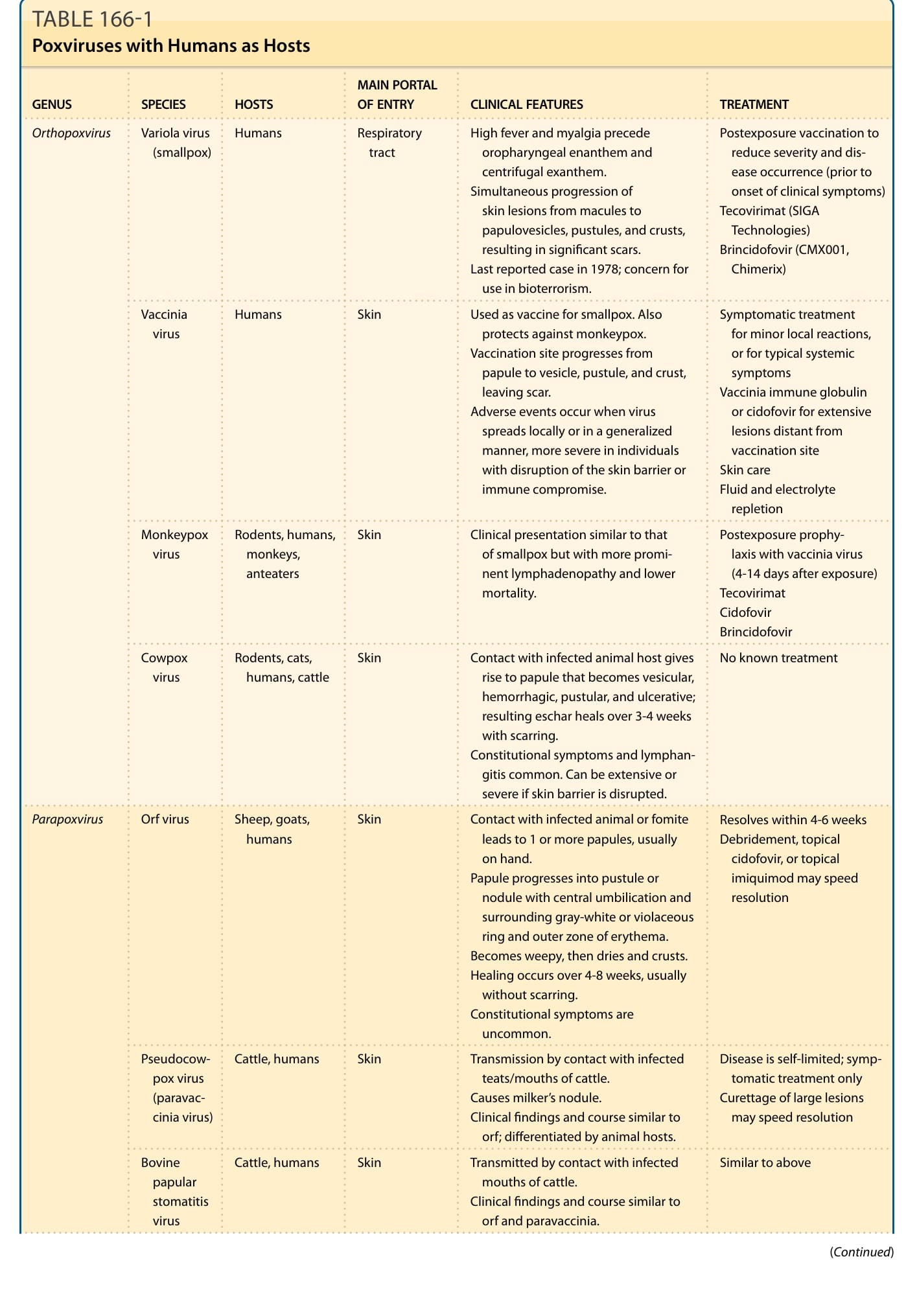
TABLE 166-1 Poxviruses with Humans as Hosts
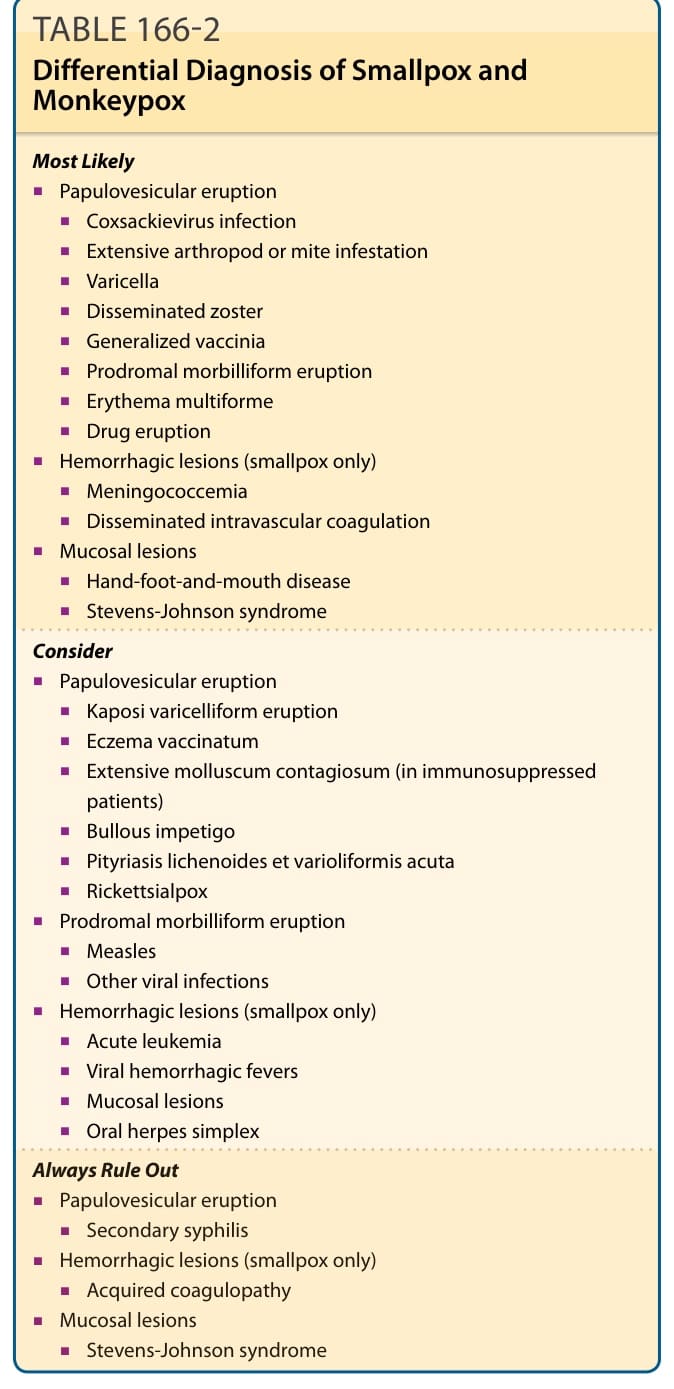
Table 166-2 outlines the differential diagnosis of smallpox. The exanthem of smallpox is most often confused with that of chickenpox (varicella). Smallpox lesions are deep-seated and firm, whereas chickenpox vesicles are more superficial (“dewdrops on a rose petal”). Smallpox lesions progress simultaneously, so all lesions on any one part of the body are in the same stage (eg, all papules or all vesicles), whereas chicken pox lesions appear in crops, so multiple different stages (a mix of papules, vesicles, pustules, and crusts) are seen at once. Chickenpox lesions progress more quickly than smallpox lesions, evolving from macule to papule to vesicle to crust in less than 24 hours. In contrast, each stage of smallpox lasts 1 to 2 days. Overall, chickenpox has a shorter disease course, with all lesions crusting within 4 to 6 days from initial appearance.16 In contrast to smallpox, which is preceded by a severe febrile prodrome with prostration, headache, backache, chills, vomiting, or abdominal pain, chickenpox is not preceded by a significant prodrome, and patients do not appear toxic. Smallpox has a centrifugal distribution,
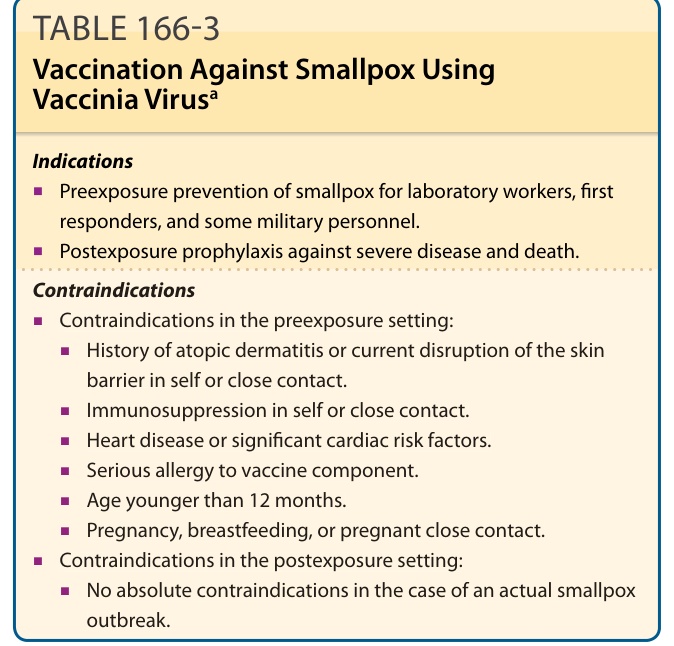
TABLE 166-3 Vaccination Against Smallpox Using Vaccinia Virusa
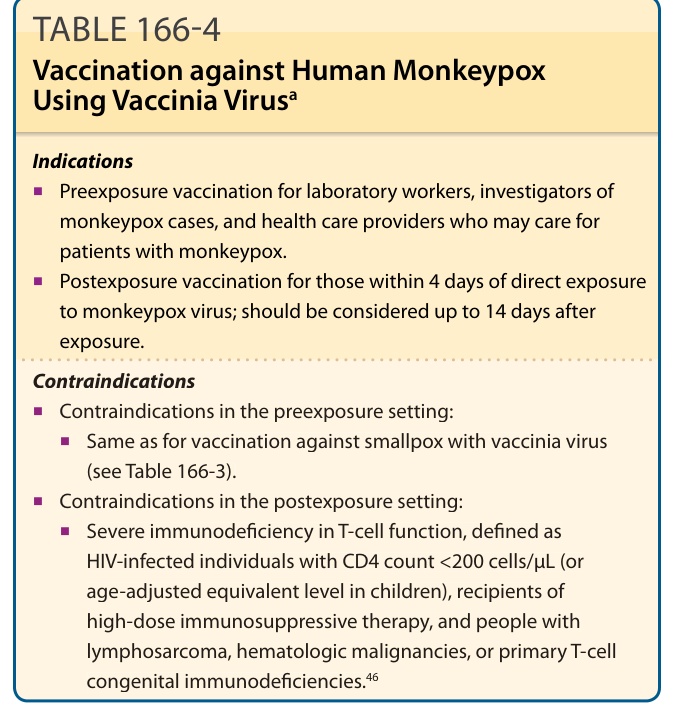
TABLE 166-4 Vaccination against Human Monkeypox Using Vaccinia Virusa
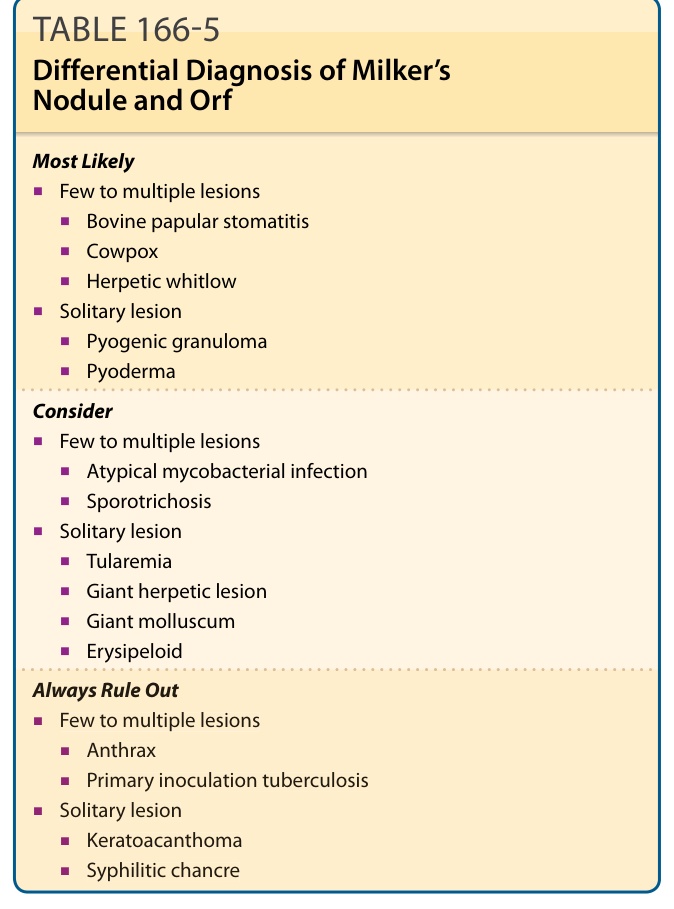
TABLE 166-5 Differential Diagnosis of Milker’s Nodule and Orf
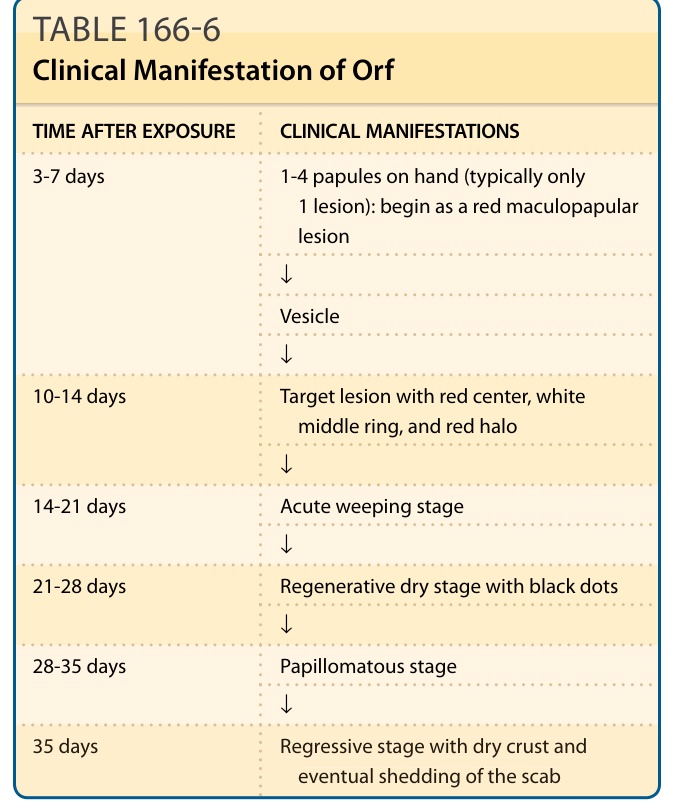
TABLE 166-6 Clinical Manifestation of Orf
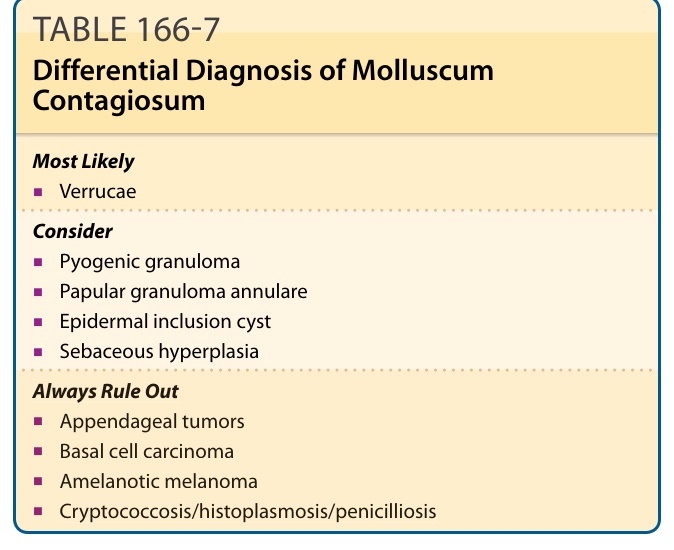
TABLE 166-7 Differential Diagnosis of Molluscum Contagiosum