Herpes Simplex
25
AT-A-GLANCE
■ Herpes simplex viruses (HSVs) are common human DNA viral pathogens that intermittently reactivate. After replication in the skin or mucosa, the virus infects the local nerve endings and ascends to the ganglia where it becomes latent until reactivation.
■ There are two types of HSV: HSV-1 and HSV-2. HSV-1 is mostly associated with orofacial disease, whereas HSV-2 usually causes genital infection, but both can infect oral and genital areas and cause acute and recurrent infections.
■ Most of the adult population is seropositive for HSV-1, and the majority of infections are acquired in childhood. About one-fourth of adults are infected with HSV-2 in the United States. Acquisition of HSV-2 correlates with sexual behavior.
■ Most primary HSV infections are asymptomatic or not recognized, but they can also cause severe disease. Most recurrences are not symptomatic and most transmissions occur during asymptomatic shedding.
■ Genital herpes is the most prevalent sexually transmitted disease worldwide and is the most common cause of ulcerative genital disease; it is an important risk factor for acquisition and transmission of HIV.
■ HSV can cause diseases involving the eye, CNS, and neonatal infection. Cellular immunity defects are a risk factor for severe and disseminated disease.
■ Diagnosis is made by polymerase chain reaction, viral culture, or serology, depending on the clinical presentation.
■ Treatment is with acyclovir, valacyclovir, or famciclovir. Regimens and dosages vary with the clinical setting. Resistance is rare, other than in immunocompromised patients.
Herpes simplex virus (HSV) infections are common worldwide and are caused by 2 closely related types of HSV. Their main clinical manifestations are mucocutaneous infections, with HSV Type 1 (HSV-1) being mostly associated with orofacial disease, and HSV Type 2 (HSV-2) usually being associated with genital infection. HSV-1 is increasingly becoming a more common cause of genital mucosal infections in young women in the United States than HSV-2.1
EPIDEMIOLOGY
The incidence of primary infection with HSV-1, which is responsible for the vast majority of recurring labial herpes, is greatest during childhood, when 30% to 60% of children are exposed to the virus. Rates of infection with HSV-1 increase with age and reduced socioeconomic status. From 20% to 40% of the population has had episodes of herpes labialis. The frequency of recurrent episodes is extremely variable, and, in some studies, averages approximately once per year. From 2005 to 2010 the seroprevalence of HSV-1 in the United States was 30% in persons 14 to 19 years of age, 50% in persons 20 to 29 years of age, and 62% in persons 30 to 39 years of age.2 The rate of HSV-1 declined by 7% from 1999-2004 to 2005-2010. Acquisition of HSV-2 correlates with sexual behavior and the prevalence of infection in one’s potential sexual partners. Antibodies to HSV-2 are rare in people before the onset of intimate sexual activity and rise steadily thereafter. From 2005 to 2010 the seroprevalence of HSV-2 in the United States was 1.2% in persons 14 to 19 years of age, 9.9% in persons 20 to 29 years of age, and 19% in persons 30 to 39 years of age.2 The rate of HSV-2 seropositivity did not change significantly from 1999-2004 to 2005-2010. Although most persons infected with HSV-1 or HSV-2 are asymptomatic, they still can transmit the virus.3 Even though HSV-2–asymptomatic persons shed virus less frequently than symptomatic persons, the amount of HSV-2 shed during asymptomatic shedding is similar in symptomatic and asymptomatic groups.4 In one study, 21% of genital swabs were positive for HSV by polymerase chain reaction (PCR) in persons who were HSV-2 seropositive, and 12% of oral swabs were positive for HSV by PCR in persons who were HSV-1 seropositive.5 It is estimated that more than 70% of HSV-2 transmission is associated with asymptomatic shedding. The rate of transmission is no higher in persons with frequent symptomatic recurrences than it is in persons with infrequent recurrences. The average risk of transmission for couples discordant for genital herpes (ie, one partner has genital herpes and the other does not) varies from 5% to 10% per year.6 As with other sexually-transmitted infections, the rate of acquisition of HSV-2 infection is higher for women than for men. Asymptomatic HSV-2 infection is more common among men and persons who are also seropositive for HSV-1, suggesting that prior infection with HSV-1 reduces one’s likelihood of experiencing symptomatic HSV-2 infection.7 Studies show that genital HSV infections significantly increase the risk for acquisition and transmission of HIV. Randomized trials with acyclovir reduced the frequency of genital ulcers and slightly
25
reduced HIV viral loads, but did not reduce transmission of HIV.8
CLINICAL FINDINGS
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
The clinical manifestations of HSV infection depend on the site of infection and the immune status of the host. Primary infections with HSV, namely those that develop in persons without preexisting immunity to either HSV-1 or HSV-2, are usually more severe, frequently involve systemic signs and symptoms, and have a higher rate of complications, compared to episodes associated with reactivation of HSV.
OROFACIAL INFECTIONS
Herpetic gingivostomatitis (Fig. 164-1) and pharyngitis are most commonly associated with a primary HSV-1 infection. The symptoms of primary oral herpes may resemble those of aphthous stomatitis and include ulcerative lesions involving the hard and soft palate, tongue, and buccal mucosa, as well as neighboring facial areas. Patients with pharyngitis exhibit ulcerative and exudative lesions of the posterior pharynx that can be difficult to differentiate from streptococcal pharyngitis. Other common symptoms include fever, malaise, myalgias, pain on swallowing, irritability, and cervical adenopathy. Reactivation of virus from these primary infections involves the perioral facial area, mainly the lips, with the outer one-third of the lower lip being the most commonly affected area (Fig. 164-2). Other facial locations include the nose, chin, and cheek, and account for fewer than 10% of cases (Fig. 164-3). Two-thirds of labial lesions involve the vermilion border, and the rest occur at the junction of the border with the skin.
3022
In patients with frequent recurrences, lesions may differ slightly in location with each episode. Immunocompetent patients tend not to experience recurrent intraoral lesions, but can present with clusters of tiny vesicles and ulcers, or linear fissures on the gingivae and anterior hard palate that are mildly symptomatic. Prodromal symptoms precede herpes labialis in 45% to 60% of episodes. Patients experience pain, burning, or itching at the site of the subsequent eruption. Even in the immunocompetent patient, the severity of recurrent herpes labialis is extremely variable and may vary from that of prodromal symptoms alone without the subsequent development of lesions (aborted episodes) to extensive disease induced by severe local sunburn. The progression of classical herpes lesions has been divided according to the following stages based on their features: prodromal, erythema, and papule
(the developmental stage); vesicle, ulcer, and hard crust (disease stage); followed by dry flaking and residual swelling (resolution stage). The lesions usually resolve within 5 to 15 days. Triggers for oral herpes recurrences include emotional stress, illness, exposure to sun, trauma, fatigue, menses, chapped lips, and the season of the year. Other well-documented triggers include exposure to ultraviolet irradiation, trigeminal nerve surgery, oral trauma, epidural administration of morphine, and abrasive, laser, and chemical facial cosmetic procedures. The exact mechanism by which these diverse factors trigger HSV reactivation is unknown. HSV-2 causes a primary orofacial infection that is indistinguishable from that associated with HSV-1, except that it is usually in adolescents and young adults, following genital–oral contact. HSV-2 orolabial infections are 120 times less likely to reactivate than orolabial HSV-1 disease.
GENITAL INFECTIONS
Genital herpes is the major clinical presentation of HSV-2 infection, but HSV-1 is becoming a more common cause of genital herpes in young women.9,10 Because of their epidemiology, acquisition of HSV-1 in a person with prior HSV-2 infection is unusual, but HSV-2 acquisition in the presence of previous HSV-1 infection is common, and infection of the genital tract with both HSV-1 and HSV-2 has been described. Patients with previously known HSV-1 genital infection who develop frequent genital herpes recurrences should be tested for HSV-2 infection. Viremia occurs in approximately 25% of persons during primary genital herpes.
A B
25
The clinical course of acute first-episode genital herpes among patients with HSV-1 and HSV-2 infections is similar. These infections are associated with extensive genital lesions in different stages of evolution, including vesicles, pustules, and erythematous ulcers that may require 2 to 3 weeks to resolve (Fig. 164-4). In males, lesions commonly occur on the glans penis or the penile shaft; in females, lesions may involve the vulva, perineum, buttocks, vagina, or cervix. There is accompanying pain, itching, dysuria, vaginal and urethral discharge, and tender inguinal lymphadenopathy. Systemic signs and symptoms are common and include fever, headache, malaise, and myalgias. Herpetic sacral radiculomyelitis with urinary retention, neuralgias, and constipation, can occur. HSV cervicitis occurs in more than 80% of women with primary infection. It can present as purulent or bloody vaginal discharge; examination reveals areas of diffuse or focal friability and redness, extensive ulcerative lesions of the exocervix, or, rarely, necrotic cervicitis. Cervical discharge is usually mucoid, but it is occasionally mucopurulent. The rates of recurrence for genital HSV-2 infections vary greatly among individuals and over time within the same individual. Infections caused by HSV-2 reactivate approximately 16 times more frequently than HSV-1 genital infections, and average 3 to 4 times per year, but may appear virtually weekly. Recurrences tend to be more frequent in the first months to years after initial infection. The classical clinical manifestations of recurrent HSV-2 infection include multiple small, grouped, vesicular lesions in the genital area (Fig. 164-5), but which can occur anywhere in the perigenital region, including the groin, buttocks, and thighs; the lesions may recur at the same site or change
3023
25
A B
location. The recurrence of genital lesions may be heralded by a prodrome of tenderness, itching, burning, or tingling, and the outbreaks are less severe than primary infection. Without treatment, the lesions usually heal in 6 to 10 days. Herpetic cervicitis is less common in recurrent disease, occurring in 12% of patients. It may present without external lesions. Signs and symptoms that are less classical for genital HSV infection and that can divert one from the correct diagnosis include small erythematous lesions, fissures, pruritus, and urinary symptoms. HSV can cause urethritis, usually manifested only as a clear mucoid discharge, dysuria, and frequency. Occasionally, HSV can be associated with endometritis, salpingitis, or prostatitis. Symptomatic or asymptomatic rectal and perianal infections are common. Herpetic proctitis presents with anorectal pain, anorectal discharge, tenesmus, and constipation, with ulcerative lesions of the distal rectal mucosa. Genital herpes can recur at nongenital sites as well.
OTHER CUTANEOUS FINDINGS
HSV can infect any skin site (Fig. 164-6). The common theme among virtually all of these cutaneous presentations is the requirement that virus have penetrated otherwise normal and well-keratinized tissues. Herpetic whitlow (Fig. 164-7) is infection of the fingers by HSV acquired by direct inoculation or by direct spread from mucosal sites at the time of primary infection. Whitlow occurs in children who suck their fingers during a primary gingivostomatitis outbreak. It is also a well documented occupational hazard for medical personnel. It is usually caused by HSV-1, but HSV-2 whitlow may develop as a manifestation of primary inoculation following manual–genital contact with an infected partner. The infected region becomes erythematous and
3024
edematous. Lesions are usually present at the fingertip and can be pustular and very painful. Fever and local lymphadenopathy are common. Whitlow is often misdiagnosed as a bacterial paronychial infection, but surgical drainage, often needed for a bacterial infection, is unnecessary and potentially harmful, while antiviral therapy speeds healing. Whitlow may recur. Cutaneous herpes can be transmitted between athletes involved in contact sports, such as wrestling (herpes gladiatorum) and rugby (herpes rugbiorum or scrum pox), and may occur as outbreaks or small epidemics among team members. In these instances, multiple herpetic lesions may appear across the thorax, ears, face, arms, and hands, in which infection is facilitated by trauma to the normally-keratinized skin during sport activities (Fig. 164-8). Concomitant ocular herpes can occur.
25
A
B
Eczema herpeticum (Kaposi varicelliform eruption; Fig. 164-9) results from widespread infection following inoculation of virus to skin damaged by eczema. It is usually a manifestation of primary HSV-1 infection in a child with atopic dermatitis; the expression of antimicrobial peptides in the skin may be a factor in controlling susceptibility to eczema herpeticum in these patients. Cathelicidin and beta-defensins are antimicrobial peptides that inhibit HSV replication. Skin lesions from patients with eczema herpeticum have lower levels of cathelicidin and beta-defensins than do skin lesions from persons with atopic dermatitis or psoriasis.11 Mycosis fungoides, Sézary syndrome, Darier disease, various bullous diseases of the skin (particularly if patients are receiving immunosuppressive therapy), and second-degree and third-degree burns also can be complicated by cutaneous dissemination of HSV. The severity of eczema herpeticum ranges from mild to fatal, with mortality rates of up to 10% being reported before antiviral therapy was available. Mortality was primarily caused by bacterial superinfection and bacteremia. Common pathogens include Staphylococcus aureus, beta-hemolytiic Streptococcus, and Pseudomomas aerugionosa. In a typical severe primary attack, vesicles develop in large numbers over areas of active or recently healed atopic dermatitis, particularly the face, several days after exposure and continue to appear in crops for several more days. The vesicles become pustular and markedly umbilicated and quickly progress to monomorphic erosions. Patients commonly have high fever and adenopathy. Viremia with infection of internal organs can be fatal. Recurrences are usually far milder than the first infection. Arriving at the correct diagnosis can be delayed
3025
25
because of secondary impetigo involving the lesions, but it should be considered in children with infected eczema, particularly if the child is more systemically ill than one might anticipate with impetigo. Eczema herpeticum of the young infant is a medical emergency, and early treatment with acyclovir can prove lifesaving. Recurrent HSV infection is the most common precipitating event in cases of recurrent erythema multiforme (see Chap. 43). HSV-associated erythema multiforme is usually an acute, self-limited, recurrent disease, that lasts approximately 3 weeks. The lesions are usually symmetric, occurring on acral extremities and the face, and there is grouping of lesions over the elbow and knees as well as nailfold involvement. Mucosal involvement is usually mild and restricted to the mouth. Constitutional symptoms are rare, and the skin lesions heal without scarring.
NEONATAL HERPES
The neonate is a special category of immunodeficient host. The prevalence of neonatal herpes varies from 1 case per 12500 to 1700 live births.12 Primary maternal genital herpes is associated with a risk of neonatal infection of 25% to 50% for vaginally-delivered babies, and accounts for 50% to 80% of cases of neonatal HSV infection. In contrast, recurrent maternal infection is associated with a risk of transmission of less than 3%, and transplacental antibodies likely play a role in decreasing the risk of infection.13 Other risk factors for development of neonatal herpes include vaginal delivery, presence of cervical HSV infection, use of invasive monitors, isolation of HSV from the genital tract, and prolonged rupture of membranes. Neonatal herpes infections manifest in 1 of 3 forms: skin, eye, and mouth involvement; encephalitis; or
3026
disseminated disease (Fig. 164-10). The encephalitic and disseminated disease forms account for more than 50% of cases of neonatal herpes. It is important to remember that more than 20% of neonates with neurologic and disseminated disease do not develop cutaneous vesicles. Without therapy, the overall mortality of neonatal herpes is 65%, and fewer than 10% of untreated neonates with CNS infection will develop normally. With current therapeutic modalities, most babies with skin, eye, and mouth disease survive and have normal development at age 1 year. For treated babies with encephalitis, mortality is 64%, with approximately 30% developing normally within 2 years after infection. Suppressive oral acyclovir for 6 months in neonates who survive CNS disease results in improved neurologic outcomes.14 For treated babies with disseminated disease, mortality is 30%, with approximately 80% of the survivors apparently developing normally within 2 years after infection.12
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
OCULAR INFECTIONS
HSV is a leading cause of recurrent keratoconjunctivitis and its associated corneal opacification and visual loss. It is usually caused by HSV-1, except in neonates in whom HSV-2 is more prevalent. The majority of HSV eye disease is caused by reactivation of the virus in the trigeminal ganglia, but primary infections of the eye can also occur. Usually, the initial manifestation of herpetic eye disease is a superficial infection of the eyelids and conjunctiva (blepharoconjunctivitis), or corneal surface (dendritic or geographic epithelial ulcer with pain and blurred vision). Deeper involvement of the cornea (stromal keratitis) or anterior uvea (iritis) represents more serious forms of the disease and can cause permanent visual loss. Acute retinal necrosis is a rare but rapidly progressive disease characterized by retinal arteriolar sheathing, uveitis, and peripheral retinal opacification with variable pain and visual loss. Retinal detachment is common and it is usually associated with HSV-1 infection.
NEUROLOGIC DISORDERS
All HSV infections involve the nervous system, as neurons are the sole proven site of virus latency. HSV meningitis is manifested by headache, fever, stiff neck, and mild photophobia with lymphocytic pleocytosis in the cerebrospinal fluid. Most cases result from HSV-2 infection, which resolve spontaneously in 2 to 7 days. HSV infection may involve the sacral nerves with autonomic nervous system dysfunction, numbness, pelvic pain, tingling, urinary retention, constipation, and cerebrospinal fluid pleocytosis. Symptoms usually resolve in a few days, but in some cases, the neurologic residua take weeks to months to disappear, occasionally becoming permanent. Reactivation of HSV or varicella-zoster virus is associated with Bell’s
palsy with acute, peripheral facial paresis caused by compression of the facial nerve in the temporal bone. HSV encephalitis is the most commonly identified acute, sporadic viral encephalitis in the United States, accounting for 10% to 20% of all cases. Nearly all of the cases arising after the neonatal period are caused by HSV-1. HSV encephalitis usually presents with acute focal neurologic symptoms, fever, and involvement of the temporal lobe. PCR of the cerebrospinal fluid for HSV DNA is the most common diagnostic technique.
COMPLICATIONS
COMPLICATIONS
All manifestations of HSV infection seen in the immunocompetent host also can be seen in immunocompromised patients, but they are usually more severe, more extensive, and more difficult to treat; for many of them, recurrences are more frequent. Patients with defects in T-cell immunity, such as those with AIDS or transplantation recipients, are at particular risk for progressive mucocutaneous or visceral infections, but the degree of dissemination depends on the level of immunodeficiency of the host. Recurrent and persistent ulcerative HSV lesions are among the most common and defining opportunistic infections in patients with AIDS.15 Genital herpes is very common in patients with HIV and can be persistent and severe. Oropharyngeal HSV in immunocompromised patients can present with widespread involvement of skin (Fig. 164-11), the mucosa, and extremely painful, friable, hemorrhagic, and necrotic lesions, similar to mucositis caused by cytotoxic agents. The lesions can spread locally to involve the esophagus. Esophagitis presents with odynophagia, dysphagia, substernal pain, and
25
multiple ulcerative lesions. Esophagitis can also arise directly by reactivation of HSV and its spread to the esophagus via the vagus nerve. Tracheobronchitis and pneumonitis can also occur by spreading of the virus from oropharyngeal HSV. HSV can reactivate from visceral ganglia of the autonomic nervous system or disseminate hematogenously to other visceral organs (causing pneumonitis, hepatitis, pancreatitis, or meningitis) and the GI tract. Most of these severe infections are caused by HSV-1, but HSV-2 can cause them as well.
ETIOLOGY AND PATHOGENESIS
RISK FACTORS
RISK FACTORS
The risk of severe HSV disease and the recurrence rate correlate with the level of cellular immune competence of the host. Patients with mild decreases in cellular immunity may experience only an increased number of recurrences and a slower resolution of lesions, while severely compromised patients are more likely to develop disseminated, chronic, or drug-resistant infections. CD8+ and CD4+ T-lymphocyte subsets, natural killer cells, and inflammatory cytokines like interferon-γ are important in mediating protection against HSV. Innate immunity is also important and polymorphisms in TLR2 are associated with increased rates of genital lesions in seropositive persons.16 Mutations in proteins important for interferon responses, including STAT1, TYK2, and UNC-93B, are associated with herpes simplex encephalitis.17 Constant immune surveillance and engagement are required to maintain latency, mainly by HSV-specific CD8+ lymphocytes. T-cells reactive to HSV-1 are clustered around latently infected neurons in ganglia from HSV-1 seropositive persons. Dendritic cells and HSV-2–specific CD8+ lymphocytes localize to sites of reactivation, rapidly contain virus-infected cells,18 and persist in the skin for weeks after lesions are cleared.19 These virus-specific CD8 cells are oligoclonal CD8αα+ cells that persist in the dermal–epidermal junction, and produce cytotoxic granules.20
Patients with defects in humoral immunity have no increase in HSV disease severity, but the humoral immune response is important in reducing virus titers at the site of inoculation and in regional neural tissues during primary infection. The transfer of HSV-specific antibodies from mother to child is a key factor in protecting against neonatal herpes.
DIAGNOSIS
LABORATORY TESTING
LABORATORY TESTING
The method of choice for diagnosis of HSV infection depends on the clinical presentation. In many instances,
3027
25
the history and clinical findings may be sufficient, but the social, emotional, and therapeutic implications of a diagnosis dictate that it be confirmed by laboratory testing when possible. For patients with active lesions, virus can be isolated in cell culture. In culture, HSV causes typical cytopathic effects, and most specimens will prove positive within 48 to 96 hours after inoculation. The sensitivity of culture depends on the quantity of virus in the specimen. Even in the most experienced centers, only approximately 60% to 70% of fresh genital lesions are culture positive. Isolation of virus is most successful when lesions are cultured during the vesicular stage and when specimens are taken from immunocompromised patients or from patients suffering from a primary infection. PCR is more sensitive than viral isolation and has become the preferred method for diagnosis. PCR has been extensively used for the diagnosis of CNS infections and neonatal herpes. It is also useful for the detection of HSV in late-stage ulcerative lesions. Both viral culture and PCR assays enable typing of the isolate as HSV-1 or HSV-2. This information helps to predict the frequency of reactivation after a first episode of HSV infection. Serologic detection of IgG antibodies to HSV can be helpful in certain settings, but the results are often misinterpreted. The main function of serologic testing is to differentiate a primary episode from a recurrent infection (Table 164-1). A positive serologic test result can be useful in patients with recurrent, genital lesions that are not present at the time of examination, thereby making a positive culture unobtainable. Serologic testing also can be helpful for counseling patients with initial episodes of disease and their partners, especially during pregnancy, and in counseling partners of patients with genital herpes about their risk of acquiring HSV. Type-specific serologic assays are based on antigenic differences between HSV-1 and HSV-2 glycoprotein G. These tests are often used to counsel patients about the meaning of the test results in terms of the natural history of the disease, disease transmission, and the emotional and social implications of the diagnosis.
PATHOLOGY
PATHOLOGY
Direct fluorescent antibody staining of lesion scrapings also can be used, but its sensitivity is lower than that of viral culture. The Tzanck test is helpful in rapid diagnosis of herpesvirus infections, but it is less sensitive than culture and staining with fluorescent antibody, with positive results in fewer than 40% of cultureproven cases. It is performed by scraping the base of a freshly-ruptured vesicle and staining the slides with Giemsa or Wright stain (the Papanicolaou staining method also can be used), followed by examination for multinucleated giant cells that are diagnostic of herpetic infection (Fig. 164-12). Both HSV and varicellazoster virus will cause these changes. In skin biopsy specimens, epithelial cells are enlarged, swollen, and often separated. Multinucleated cells with intranuclear eosinophilic inclusion bodies can be seen.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of orolabial herpes includes aphthous ulcers, syphilis, and herpangina. Diseases that can mimic genital herpes include
CLASSIFICATION VIRUS ISOLATED
SEROLOGY (ACUTE) SEROLOGY (CONVALESCENT)
HSV-1 IgG HSV-2 IgG HSV-1 IgG HSV-2 IgG
Primary HSV-1 HSV-1 − − + −
Primary HSV-2 HSV-2 − − − +
Primary HSV-1 plus previous HSV-2 infection (rare) HSV-1 − + + +
Primary HSV-2 plus previous HSV-1 infection HSV-2 + − + +
Recurrent HSV-1 HSV-1 + − or + + − or +
Recurrent HSV-2 HSV-2 − or + + − or + +
Recurrent HSV-2 HSV-2 − or + + − or + +
3028
−, Negative; +, positive; HSV, herpes simplex virus.
DISEASE OR CONDITION DIFFERENCES FROM HERPES
Orolabial Aphthous ulcers Not preceded by vesicles, located only on mucosa
Syphilis Painless, not preceded by vesicles
Herpangina Posterior portion of mouth (soft palate, tonsils)
Erythema multiforme Partial involvement of oral mucosa with targetoid plaques with vesicular or erosive centers; lesions may be confluent
Stevens-Johnson syndrome Diffuse erosive mucositis plus generalized skin lesions
Genital Chancroid Deep ulceration with exudate
Syphilis Painless, not preceded by vesicles
Lymphogranuloma venereum Painless ulcer, unimpressive primary lesions
Granuloma
Painless ulcer, exuberant lesions
Granuloma inguinale Painless ulcer, exuberant lesions
inguinale
chancroid, syphilis, and lymphogranuloma venereum (Table 164-2).
CLINICAL COURSE AND PROGNOSIS
Although most patients with HSV infections are asymptomatic, primary infections can be severe. Most recurrences are asymptomatic, but symptomatic recurrences are milder than symptomatic primary infections. The frequency and severity of recurrent HSV-1 and HSV-2 disease decrease over time; therefore, the need for continued suppressive therapy should be reevaluated.
MANAGEMENT
INTERVENTIONS
INTERVENTIONS
COUNSELING
All sexually-active persons should be educated regarding the nature and risks of acquiring and transmitting sexually-transmitted infections, including HSV. Studies show that approximately one-half of patients with asymptomatic HSV-2 infection have mild, unrecognized disease and can be taught to recognize the symptoms and signs of genital herpes. Also, patients should be counseled regarding safer sex practices. It must be emphasized that the majority of transmission occurs in asymptomatic phases and from people who have no classical lesions. Patients with genital herpes should be counseled to refrain from sexual intercourse during outbreaks and for 1 to 2 days after, and to use
25
condoms between outbreaks. Suppressive antiviral therapy is also an option for individuals concerned about transmission to a partner. Pregnant women who are known to have genital herpes should be reassured that the risk of transmitting herpes to the baby during childbirth is extremely low. Recommendations for the management of pregnant women with recurrent genital herpes include clinical evaluation at delivery, with delivery by cesarean section indicated if there are signs and symptoms of active infection (including prodrome). But cesarean section delivery may not reliably prevent neonatal HSV infection when membranes are ruptured for long periods (≥24 hours). Women with primary HSV infection during pregnancy should be treated with antiviral therapy. For women at or beyond 36 weeks of gestation who are at risk for recurrent HSV infection, suppressive antiviral therapy has been recommended, as this decreases viral shedding, the incidence of active lesions near term, and the need for cesarean delivery because of HSV.21 Close followup; sequential PCR or cultures for HSV of infants born to seropositive mothers who are shedding virus at the time of delivery; prophylactic therapy with intravenous acyclovir for infants born to mothers with primary infection; and intravenous acyclovir, if HSV is detected in infants of seropositive mothers, all have been suggested.12
Women who are known by history and serologic tests not to have genital herpes should be counseled about signs and symptoms of HSV and how to avoid acquiring the infection during pregnancy. Serology is helpful in counseling a couple in which the male partner has recurrent genital herpes and the pregnant wife is susceptible.
MEDICATIONS (SEE CHAP. 191)
Many HSV infections require no specific treatment. Keeping lesions clean and dry while they heal by themselves may be all that is required. Treatment is warranted for infections that are likely to prove protracted, highly symptomatic, or complicated. Acyclovir has a highly favorable therapeutic index because of its preferential activation in infected cells and preferential inhibition of the viral DNA polymerase. It must be phosphorylated to be active, and it requires the viral thymidine kinase for phosphorylation. Acyclovir inhibits HSV-1 and HSV-2 replication by 50% at a concentration of 0.1 and 0.3 µg/mL (range: 0.01 to 9.9 µg/mL), respectively, but is toxic at concentrations of greater than 30 µg/mL. Any strain that requires more than 3 µg/mL of acyclovir to be inhibited is said to be relatively drug resistant. Valacyclovir, the l-valyl ester of acyclovir, is an oral prodrug of acyclovir that achieves 3- to 5-fold higher bioavailability after oral administration, and can be used in a more convenient dosage regimen. Famciclovir is the well absorbed oral form of penciclovir. Similar to acyclovir, famciclovir is converted by phosphorylation to its active metabolite penciclovir triphosphate. The efficacy and adverse effect profile of famciclovir is comparable to that of acyclovir. Penciclovir 1% cream is approved by the U.S. Food
3029
25
ACCEPTABLE REGIMEN ALTERNATIVES
DISEASE
DURATION COMMENTS ADULTS PEDIATRICa
Primary infection Acyclovir, 200 mg orally 5 times a day Acyclovir, 400 mg orally 3 times a day Valacyclovir, 1 g orally twice a day Famciclovir, 250 mg orally 3 times a day
Acyclovir 15 mg/kg orally 5 times a day 7-10 days or until resolution of symptoms
Recurrent infection: episodic treatment Topical penciclovir, 1% cream q2h while awake Topical docosanol, 10% cream 5 times a day Acyclovir, 400 mg orally 5 times a day Famciclovir, 500 mg orally 2 or 3 times a day Valacyclovir, 2 g orally twice a day for 1 day Famciclovir, 1500 mg single dose or 750 mg twice a day for 1 day
IV acyclovir for severely ill individuals No studies have been done in adults; regimens are extrapolated from their effectiveness in primary genital herpes
4-5 days or until lesions are healed
Treatment is generally not warranted
Recurrent infection: prophylaxis Acyclovir, 400 mg orally twice a day
Start just before and during precipitating event, such as intensive ultraviolet light exposure
Recurrent infection:
Acyclovir, 400 mg orally twice a day Valacyclovir, 500 mg once a day Valacyclovir, 1 g once a day
There are no pediatric
Recurrent infection: suppression of confirmed frequent recurrences
Acyclovir, 400 mg orally twice a day Valacyclovir, 500 mg once a day Valacyclovir, 1 g once a day
There are no pediatric studies, but children with confirmed frequent recurrences may benefit from suppressive oral acyclovir therapy
suppression of confirmed frequent recurrences
studies, but children with confirmed frequent recurrences may benefit from suppressive oral acyclovir therapy
aOral dosage of acyclovir in children should not exceed 80 mg/kg/day. Children who weigh 40 kg or more should receive the adult dose. Note: The doses are for patients with normal renal function. Neither valacyclovir nor famciclovir is approved by the U.S. Food and Drug Administration for use in children.
and Drug Administration (FDA) for the treatment of herpes simplex labialis. Docosanol 10% cream is approved by the FDA for nonprescription treatment of recurrent herpes labialis. Docosanol is a long-chain saturated alcohol that inhibits entry of lipid-enveloped virus into the cell. It decreases healing time by 18 hours when compared with placebo. The current recommendations for antiviral treatment depend on the clinical disease, on host immune status, and whether one is treating a primary or recurrent episode or considering suppressive therapy (Tables 164-3 to 164-5).22 For disseminated or severe herpes infections, the treatment of choice remains intravenous acyclovir 10 to 15 mg/kg every 8 hours. The dose of intravenous acyclovir for neonatal herpes is 20 mg/kg per dose given every 8 hours. For first episodes of genital HSV-2 infections, oral acyclovir, famciclovir, or valacyclovir all speed healing and resolution of symptoms, and decrease viral shedding. When compared with placebo, acyclovir decreases time to healing from 16 to 12 days, the duration of pain from 7 to 5 days, and the duration of constitutional symptoms from 6 to 3 days. Valacyclovir was compared with acyclovir in the treatment of primary
3030
episodes and shown to be equivalent. Antiviral treatment of initial herpes episodes does not decrease subsequent recurrences, probably because HSV establishes latent infection within hours after infection and days before symptoms evolve. Treatment of recurrent episodes of genital herpes with famciclovir, acyclovir, or valacyclovir reduces the time of healing from approximately 7 to 5 days, time of cessation of viral shedding from 4 to 2 days, and duration of symptoms from 4 to 3 days when compared with placebo. Valacyclovir and acyclovir are equivalent; valacyclovir was similar to famciclovir in one study, but slightly superior to famciclovir to suppress genital herpes in another study. For persons with frequent or complicated genital recurrences, longterm suppressive therapy with acyclovir or its analogs is the most effective management strategy. Suppressive therapy was effective during the first year after acquisition of genital herpes. Suppressive therapy reduces the rate of shedding in healthy persons and those with HIV. Suppressive therapy with valacyclovir was more effective to reduce the burden of genital herpes disease than episodic therapy. Because genital herpes is not progressive in the normal host and because the
25
ACCEPTABLE REGIMEN ALTERNATIVES
DISEASE
DURATION COMMENTS ADULTS PEDIATRICa
Primary infection Acyclovir, 200 mg orally 5 times a day Acyclovir, 400 mg orally 3 times a day Valacyclovir, 1 g orally twice a day Famciclovir, 250 mg orally 3 times a day
Recurrent infection Acyclovir, 400 mg orally 3 times a day Acyclovir, 200 mg orally 5 times a day Acyclovir, 800 mg orally twice a day Valacyclovir, 500 mg orally twice a day Valacyclovir, 1 g orally once a day Valacyclovir, 1 g orally twice a dayb
Famciclovir, 500 mg,b 250 mg, 125 mg orally twice a day Famciclovir, 1 g orally twice a day for 1 day (patient initiated) Famciclovir, 500 mg, then 250 mg twice daily for 2 days
Suppression of recurrences Acyclovir, 400 mg orally twice a day Acyclovir, 800 mg orally once a day Valacyclovir, 500 mg, 1000 mg orally once a dayc
Valacyclovir, 250 mg orally twice a dayc
Valacyclovir, 500 mg twice a day or 1000 mg orally once a dayb
Famciclovir, 250 mg orally twice a day Famciclovir, 125 mg, 250 mg orally 3 times a day
Reduction of
Acyclovir, 40-80 mg/kg/day orally divided in 3 to 4 doses (maximum 1 g/day)
7–10 days or until clinical resolution occurs.
For children ≥12 years of age: Acyclovir, 200 mg orally 5 times a day for 5 days Acyclovir, 800 mg orally twice a day for 5 days Acyclovir, 800 mg 3 times a day for 2 days
For children ≥12 years of age: Acyclovir, 400 mg orally twice a day
Duration of the therapy is controversial; some authorities will offer treatment for 1 year and then reassess the need to resume it
Valacyclovir, 500 mg orally once a day Safer sex practices should
Reduction of transmission Valacyclovir, 500 mg orally once a day Safer sex practices should continue to be used
transmission
continue to be used
aOral dosage of acyclovir in children should not exceed 80 mg/kg/day. Children who weigh 40 kg or more should receive the adult dose.
bHIV patients.
cThe high once-a-day and twice-daily doses of valacyclovir are more effective in patients who present with more than 10 recurrences per year. Note: The doses are for patients with normal renal function. Neither valacyclovir nor famciclovir is approved by the U.S. Food and Drug Administration for use in children.
rate of recurrences varies over time and may decrease after some years, it is wise to recommend a “holiday” from treatment every year or so to reassess the continuing need for treatment. Sunscreen has shown benefit in some, but not all trials, but there is no evidence for lysine or gammaglobulin.23 Novel antivirals that inhibit the HSV helicase–primase complex24,25 were effective for treatment of recurrent genital herpes in Phase II trials, but are not licensed. The use of antiviral suppressive therapy during the late phase of pregnancy to avoid neonatal herpes also has been advocated, but a formal study of the approach would require a very large number of participants because of the rare incidence of neonatal herpes. A more achievable goal is to decrease the need for cesarean deliveries caused by herpes recurrences during labor. Studies show that antiviral therapy in late pregnancy (beginning at 36 weeks) prevents clinical recurrences, cesarean sections associated with genital herpes, and the risk of HSV-viral shedding at delivery. Orolabial HSV infections warrant antiviral treatment less often than do genital infections. Primary
HSV gingivostomatitis should be treated with oral acyclovir. The pediatric dose is 15 mg/kg of acyclovir suspension orally 5 times a day for 7 days. When it is started within 3 days of onset of the disease, this regimen decreases the duration of oral and extraoral lesions, fever, and eating and drinking difficulties. Valacyclovir and famciclovir may be equally effective, but they have not been studied in this setting and are not currently approved for use in children. Severely ill children may need to be hospitalized for hydration, and IV acyclovir may be necessary. Treatment of recurrent herpes labialis with antiviral drugs in immunocompetent hosts has shown only modest benefits.23 Oral infections are inherently briefer and less symptomatic than genital herpes. Treatment is only effective if used very early in the disease, especially in the prodromal or erythema lesion stages. Patients who wish treatment should have the medication available and be vigilant for the earliest signs and symptoms of a recurrence. When treatment is thought to be required, penciclovir 1% cream every 2 hours while awake, for 4 days can be used. Treatment should be initiated as early as possible. When initiated within
3031
25
ACCEPTABLE REGIMEN ALTERNATIVES
DISEASE
DURATION COMMENTS ADULTS PEDIATRICa
Neonatal herpes IV acyclovir, 20 mg/kg every 8 h 14-21 days For infants with CNS disease, 6 months of acyclovir suppression is effective (see text)
Disseminated infection IV acyclovir, 10-15 mg/kg 3 times a day IV acyclovir, 10 mg/kg 3 times a day 14-21 days
Herpes gladiatorum, herpetic whitlow
Acyclovir, 200 mg orally 5 times per day Acyclovir, 400 mg orally 3 times a day Valacyclovir, 1 g orally twice a day Famciclovir, 250 mg orally 3 times a day
Acyclovir, 40-80 mg/kg/day orally divided into 3 to 4 doses (maximum: 1 g/day)
Eczema
Acyclovir, 200 mg orally 5 times a day Acyclovir, 400 mg orally 3 times a day Valacyclovir, 1 g orally twice a day IV acyclovir, 10-15 mg/kg 3 times a day
7-10 days or until resolution of symptoms
No studies have been done; regimens are extrapolated from the treatment of genital herpes. Consider suppressive antiviral therapy for patients with frequent recurrences
Acyclovir, 40-80 mg/kg/day
Eczema herpeticum Acyclovir, 200 mg orally 5 times a day Acyclovir, 400 mg orally 3 times a day Valacyclovir, 1 g orally twice a day IV acyclovir, 10-15 mg/kg 3 times a day
14-21 days No studies have been done. Use IV
Acyclovir, 40-80 mg/kg/day orally divided into 3 to 4 doses (maximum: 1 g/day); IV acyclovir 10-15 mg/kg 3 times daily
herpeticum
14-21 days No studies have been done. Use IV acyclovir in severely ill individuals. Consider suppressive antiviral therapy for patients with recurrences. Ocular involvement should be treated in consultation with an ophthalmologist
orally divided into 3 to 4 doses (maximum: 1 g/day); IV acyclovir 10-15 mg/kg 3 times daily
acyclovir in severely ill individuals. Consider suppressive antiviral therapy for patients with recurrences. Ocular involvement should be treated in consultation with an ophthalmologist
aOral dosage of acyclovir in children should not exceed 80 mg/kg/day. Children who weigh 40 kg or more should receive the adult dose. Note: The doses are for patients with normal renal function. Neither valacyclovir nor famciclovir is approved by the U.S. Food and Drug Administration for use in children.
1 hour of first symptoms of recurrence, penciclovir sped the healing of lesions (4.8 days vs 5.5 days) and decreased the duration of pain (3.5 days vs 4.1 days). This regimen is approved by the FDA. Docosanol 10% cream is approved by the FDA for nonprescription treatment of herpes simplex labialis. It is applied 5 times a day at the first sign of recurrence of herpes simplex labialis. There has been no direct comparison with topical penciclovir. Oral acyclovir, 400 mg 5 times a day for 5 days, affords marginal benefit if begun in the earliest hour or two of the outbreak. Famciclovir, 500 mg 3 times a day for 5 days, when started within 48 hours after experimental ultraviolet radiation, decreased the median time to healing from 6 to 4 days, but is not useful for the more usual sporadic cases of herpes labialis. Valacyclovir (2 g twice daily for 1 day) decreased the mean duration of cold sore episodes by 1 day when compared with placebo, if started in the prodrome period. Similarly, a single dose of famciclovir (1500 mg) reduced time to healing of herpes labialis lesions by approximately 2 days compared with placebo. Creams and ointments containing 5% and 10% acyclovir are not beneficial in recurrent herpes labialis. The use of suppressive acyclovir for herpes labialis is controversial. In one small study, oral acyclovir, 400 mg twice a day, was effective in decreasing recurrences of herpes labialis. In another study, suppressive therapy with valacyclovir was more effective than episodic therapy with valacyclovir for herpes labialis. In studies with skiers (who have significant sun exposures), acyclovir 400 mg twice a day, was shown to reduce recurrences in one study, whereas acyclovir, 800 mg twice daily, failed to prevent recurrences in
3032
another study. Both perioperative famciclovir (125 or 250 mg orally twice daily given 1 to 2 days before to 5 days after the procedure) and valacyclovir (500 mg twice daily for 14 days, starting either a day before or the day of the procedure) appeared to reduce the recurrence of orofacial HSV in patients undergoing facial laser resurfacing. Valacyclovir also suppresses recurrences of herpes gladiatorum. Herpetic eye disease should always be treated in consultation with an ophthalmologist. Options usually involve topical antivirals, including vidarabine, trifluridine, acyclovir, or ganciclovir. Topical antivirals are effective in shortening the duration of dendritic and geographic keratitis, and are used to prevent corneal epithelial disease in patients with blepharitis and conjunctivitis, as well as patients on topical steroid therapy for corneal stromal inflammation and iridocyclitis. Oral acyclovir is also effective for dendritic and geographical epithelial keratitis. Suppressive antiviral therapy reduces the rates of all types of recurrent ocular HSV disease, and it is most important for patients with a history of HSV stromal keratitis because it can prevent additional episodes and potential loss of vision.
Antiviral Resistance: Virtually all clinically relevant drug resistance has been seen in immunocompromised patients. The primary mechanism of acyclovir resistance is selection of viral mutants defective or deficient in thymidine kinase expression. Most mutants that are thymidine kinase deficient are somewhat attenuated for virulence in vivo. The treatment of resistant HSV infection is complicated. Very few people who claim to be “resistant”
to one of the antiviral drugs actually harbor resistant virus. There is a common misconception that treatment prevents all recurrences. One should suspect resistance only in people who continue to have culture-proven or PCR-proven outbreaks of unaltered frequency and severity, especially if the lesions do not heal by themselves. When resistance is suspected, virus should be cultured and tested for sensitivity to acyclovir. These tests are expensive but are available through commercial reference laboratories. Foscarnet does not require activation by HSV thymidine kinase and is usually effective in the treatment of acyclovir-resistant HSV. The drug requires IV therapy and can cause numerous adverse reactions, including nephrotoxicity, electrolyte disturbances, anemia, and seizures. Rare foscarnetresistant HSV strains have been reported. Cidofovir also does not require activation by HSV thymidine kinase. Cidofovir has been used in cases of acyclovir-resistant HSV and topical cidofovir has been used with success to treat progressive herpetic lesions. Intravenous cidofovir is associated with considerable nephrotoxicity and requires the coadministration of saline hydration and probenecid. A few patients with acyclovir-resistant genital herpes have responded to imiquimod 5% cream. Imiquimod causes severe inflammation in some patients with recurrent herpes labialis. Resiquimod reduced the rate of new lesions in 1 study of persons without drug-resistant virus, but had no effect on genital herpes in 4 other studies. Continuous intravenous acyclovir also has been used to treat acyclovir-resistant HSV. Long-term suppressive acyclovir therapy reduced the rate of drug-resistant HSV disease in hematopoietic stem cell transplant recipients.
PREVENTION
Strategies to prevent HSV infection have proved inadequate. HSV infection can be prevented by total abstinence, as indicated by very low seroprevalence rates in cloistered nuns. Condoms reduce rates of transmission if used routinely. Male circumcision reduced the rate of HSV-2 infection in one study, but not in another study. Other than these public health approaches, most efforts involve antiviral therapy and vaccines directed at genital herpes.
Antiviral Therapy: Acyclovir, famciclovir, and valacyclovir all decrease both symptomatic and subclinical shedding of HSV-2, from approximately 8% of the days in the placebo group to 0.3% to 0.6% of the days in the treatment group, when assessed by culture. Once-daily valacyclovir reduced shedding by PCR from 14% to 3% in patients with newly diagnosed genital herpes. Valacyclovir 500 mg once daily was effective in reducing the transmission of HSV-2 between partners by 48%, and reduced clinical disease in the susceptible partner by 7% in a randomized, placebo-controlled trial involving immunocompetent, heterosexual couples in stable relationships.6 This therapy can be recommended for individuals concerned about transmission to a partner, in conjunction
25
with the use of condoms. Frequency of HSV-2 shedding was reduced with high-dose acyclovir (800 mg 3 times daily) or high-dose valacyclovir (1 g 3 times daily) compared with standard dose valacyclovir (500 mg daily); however, the high-dose therapies did not reduce recurrence rates compared with standard dose valacyclovir.26 Tenofovir gel applied vaginally within 12 hours before and 12 hours after coitus reduced the incidence of HSV-2 by approximately 50%.27 Oral tenofovir and emtricitabine-tenofovir had a modest effect on reducing acquisition of HSV-2.28
Vaginal microbicides are also being studied, mostly focusing on decreasing HIV transmission, but some of the compounds also have anti-HSV activity and may also affect HSV transmission.
Vaccines: No vaccine is licensed to protect against acquisition of HSV (prophylactic) or to reduce the number of recurrent episodes (therapeutic).29 A recombinant HSV-2 glycoprotein D vaccine was ineffective at preventing genital herpes disease, infection, or HSV shedding.30 Several candidate vaccines are under development to prevent recurrent genital HSV.31 A replication-defective mutant, deleted for 2 essential viral proteins, is currently in a clinical trial. Initial results with a subunit vaccine containing HSV-2 gD2 and ICP4 protein showed a 50% reduction in HSV-2 genital shedding after vaccination. A Phase II study of a vaccine consisting of HSV-2 peptides linked to heat shock protein with an adjuvant, showed a 15% reduction in HSV-2 genital shedding.
ACKNOWLEDGMENTS
The author recognizes the contribution of Adriana Marques, who was a coauthor of this chapter in the previous edition. Much of the text is based on the chapter from the prior edition.

Figure 164-1 Primary herpetic gingivostomatitis. (Used with permission from Clyde S. Crumpacker, MD.)

Figure 164-2 Herpes simplex virus infection. Erythema and early vesicles caused by recurrent herpes labialis of the upper lip. (Used with permission of the William Weston Collection.)

Figure 164-3 Recurrent facial herpes simplex with grouped vesicles and crusting. (Used with permission from Clyde S. Crumpacker, MD.)

Figure 164-4 A, Primary genital herpes with vesicles. (Used with permission from Clyde S. Crumpacker, MD.) B, Primary herpetic vulvitis.

Figure 164-5 A, Genital herpes. Recurrent infection of the penis. Group of vesicles with early central crusting on a red base arising on the shaft of the penis. This “textbook” presentation, however, is much less common than small asymptomatic erosions or fissures. B, Genital herpes. Recurrent vulvar infection. Large, painful erosions on the labia. Extensive lesions such as these are uncommon in recurrent genital herpes in an otherwise healthy individual.

Figure 164-6 Recurrent genital herpes on the abdomen (zosteriform herpes simplex).

Figure 164-7 Herpes simplex virus infection. Herpetic whitlow. Painful, grouped, confluent vesicles on an erythematous, edematous base at the distal finger where the first (and presumed primary) symptomatic infection occurred.
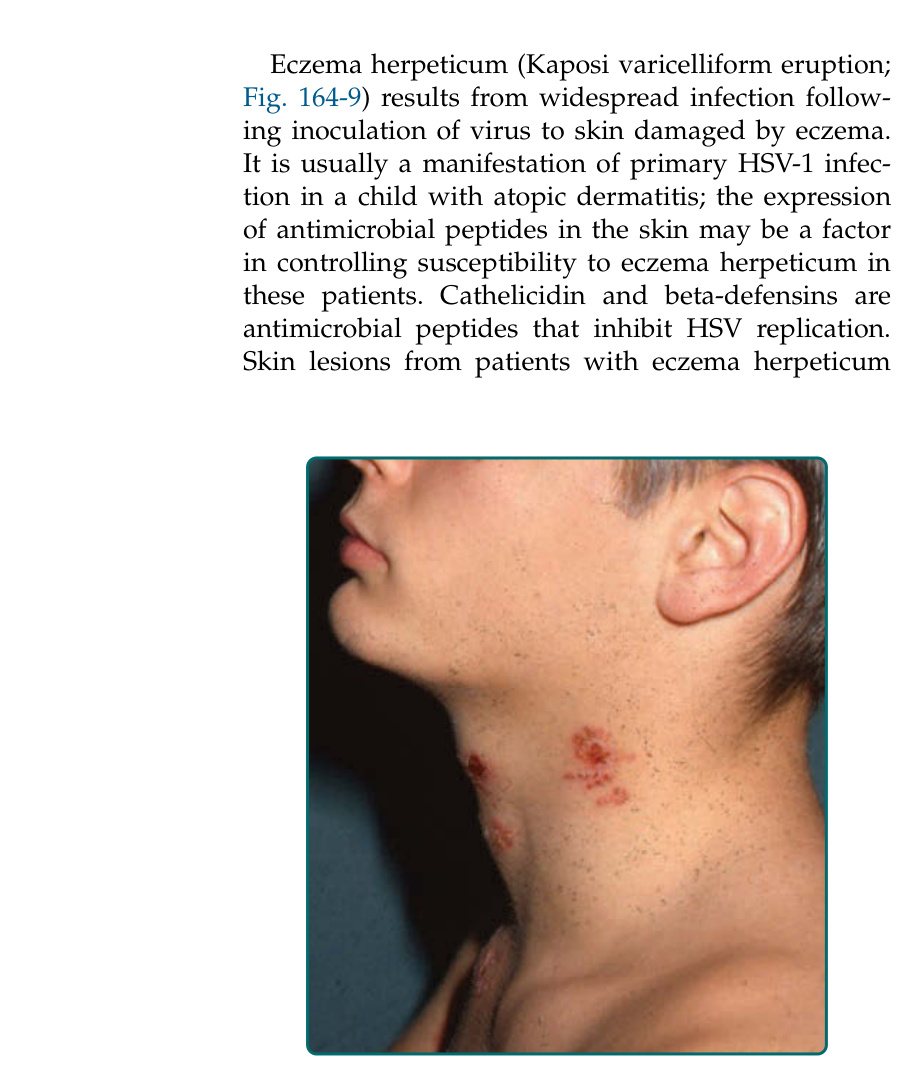
Figure 164-8 Herpes simplex gladiatorum with lesions on the neck.

Figure 164-9 Two examples of eczema herpeticum. Confluent and discrete crusted erosions associated with erythema and edema of the face of a child (A) and man (B) with atopic dermatitis. Note the monomorphic vesicles and punched out erosions. (Image A, Used with permission from Anna L. Bruckner, MD.)

Figure 164-10 Neonatal herpes simplex virus Type-2.
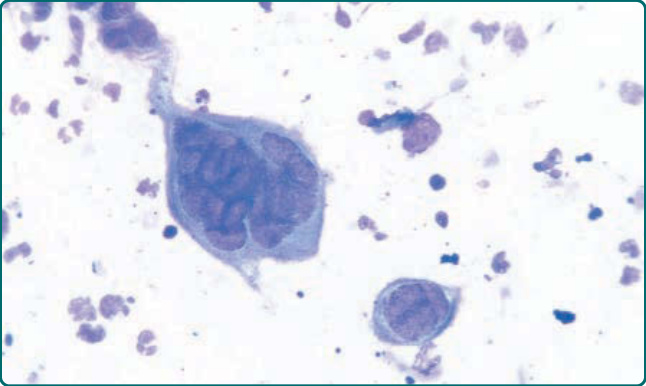
Figure 164-12 Herpes simplex virus: Positive Giemsa smear for Tzanck cells. A giant, multinucleated keratinocyte on a Giemsa-stained smear obtained from a vesicle base. Compare size of the giant cell to that of neutrophils also seen in this smear.
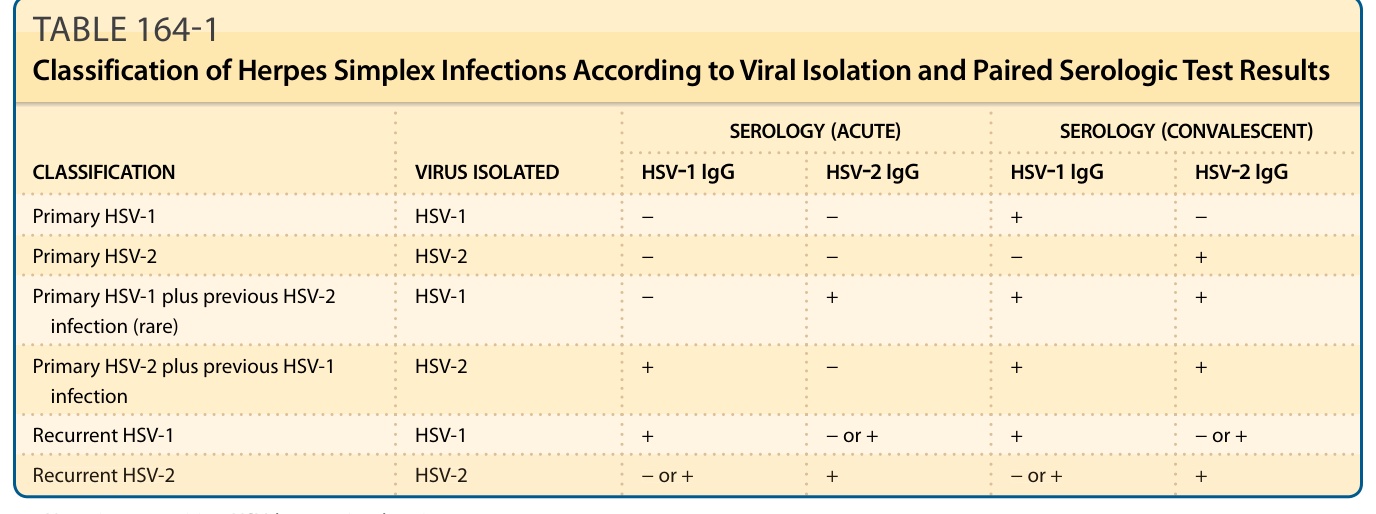
TABLE 164-1 Classification of Herpes Simplex Infections According to Viral Isolation and Paired Serologic Test Results
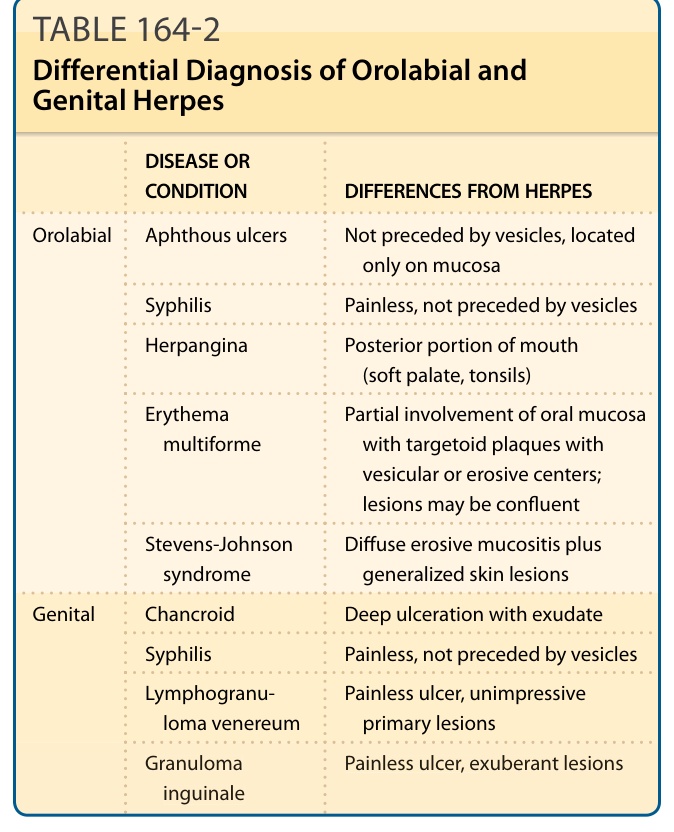
TABLE 164-2 Differential Diagnosis of Orolabial and Genital Herpes
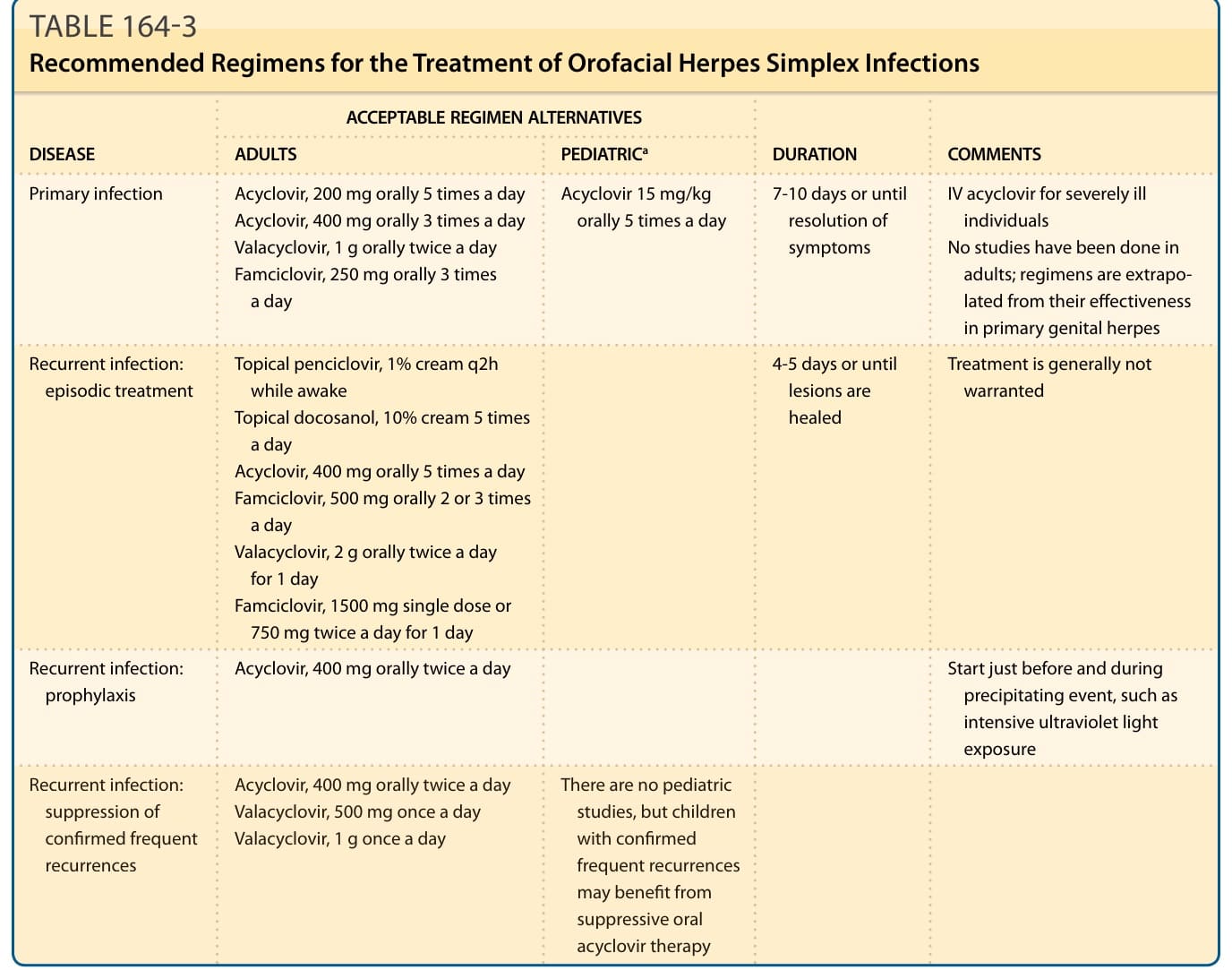
TABLE 164-3 Recommended Regimens for the Treatment of Orofacial Herpes Simplex Infections
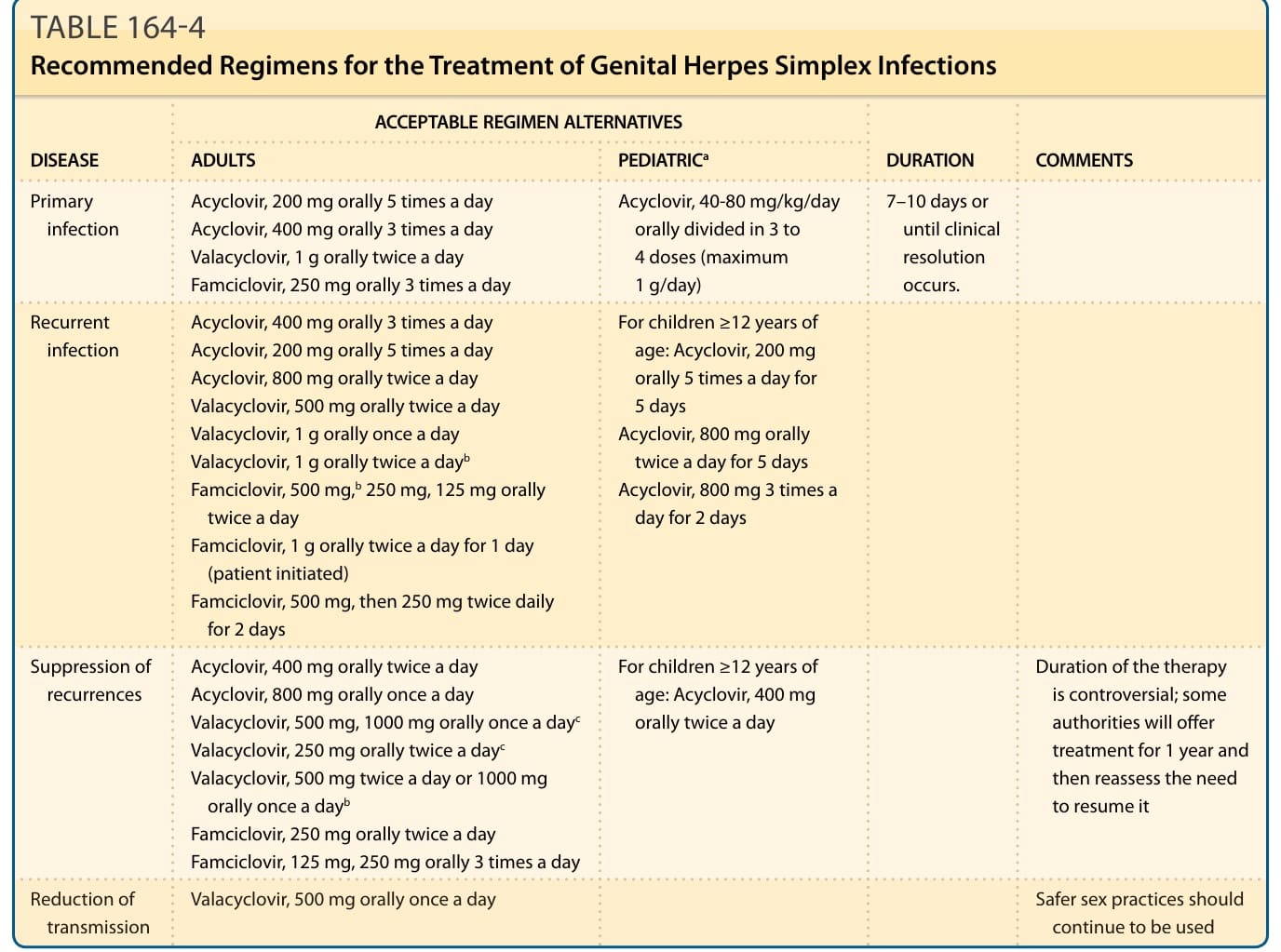
TABLE 164-4 Recommended Regimens for the Treatment of Genital Herpes Simplex Infections
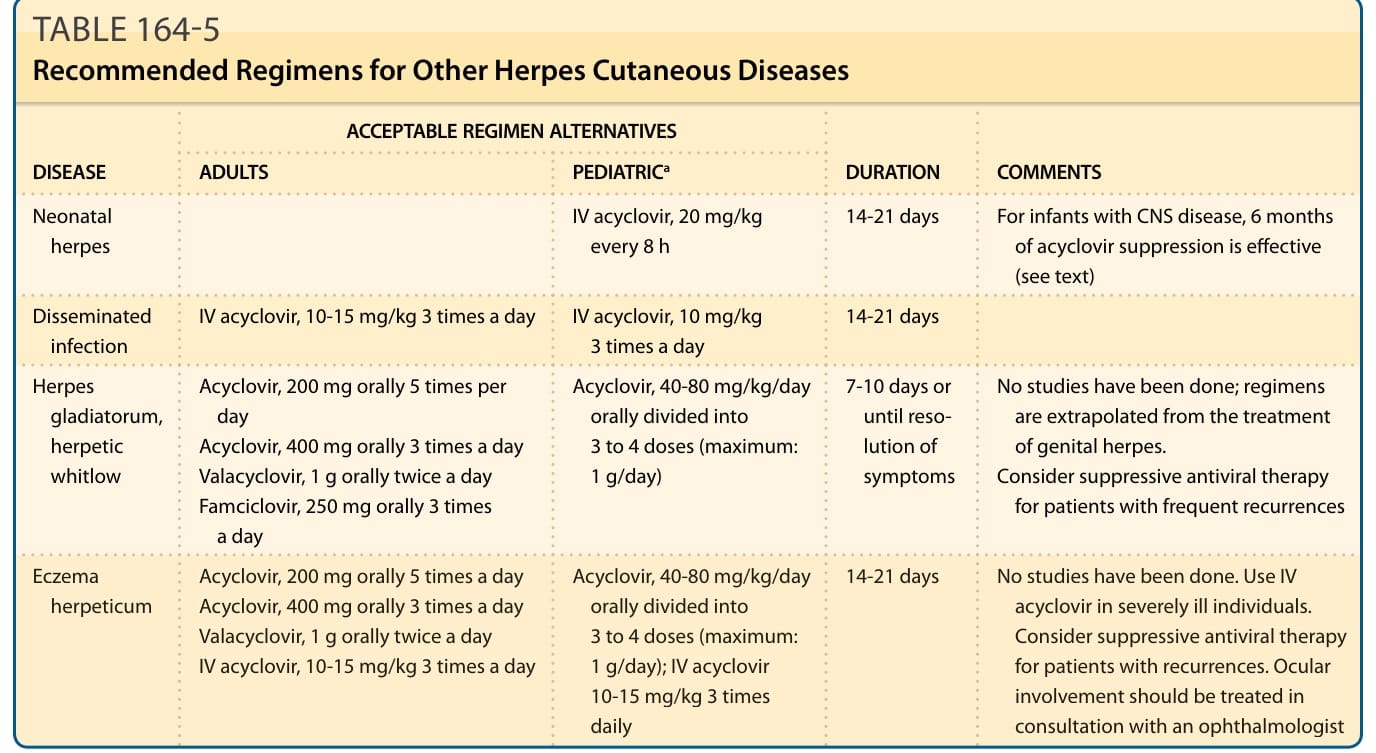
TABLE 164-5 Recommended Regimens for Other Herpes Cutaneous Diseases