Exanthematous Viral Diseases
PART25
Viral Diseases
MEASLES
AT-A-GLANCE
■ Prodrome of fever, cough, coryza, and conjunctivitis
■ Koplik spots on the buccal mucosa are pathognomonic
■ Morbilliform eruption lasts 3 to 5 days
■ Severe complications include pneumonia and postmeasles encephalomyelitis
■ Vitamin A treatment may reduce morbidity and mortality
Measles, or rubeola, is a highly contagious, viral disease that remains an important cause of morbidity and mortality worldwide. The incidence and mortality rates are highest in developing countries, particularly in Africa and Asia where large populations are unvaccinated.
EPIDEMIOLOGY
EPIDEMIOLOGY
A measles vaccine was first licensed in the United States in 1968. Prior to the introduction of the vaccine, approximately 90% of Americans were infected with measles prior to 15 years old.1
By 2000, endemic transmission of measles within the United States ceased and measles was declared eliminated.2 However, measles outbreaks continue to occur in the United States partly because of travel to countries with higher rates of measles and the spread of the virus in U.S. communities with pockets of unvaccinated people.3 For instance, a multistate
outbreak in late 2014 as a consequence of transmission at Disneyland in Anaheim, California, was responsible for 111 of the total 189 cases of measles in the United States in 2015.4
Worldwide, measles rates have also precipitously declined as the result of the implementation of measles vaccine programs. As of 2014, 85% of children across the globe had received at least 1 dose of the measles vaccine.5 Despite this improvement, measles is still a leading cause of childhood mortality with 114,900 deaths in 2014.5 The epidemiology of measles in the developing world is highly dependent on funding resources, public health infrastructure and political stability.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Measles virus is a highly contagious, single-stranded, enveloped RNA virus that is a member of the Paramyxoviridae family. Humans are the only natural hosts. Transmission occurs via person-to-person contact or airborne respiratory secretions. Infectious droplets have been reported to remain airborne for up to 2 hours, allowing for easy transmission in public spaces.6
The measles virus enters the host via the respiratory mucosa or conjunctiva where it can replicate, spread locally to lymphatic nodes and later disseminate into the bloodstream. The humoral immune system controls viral replication and confers antibody protection, whereas the cell-mediated response eliminates infected cells. A transient immunosuppression occurs during measles virus infection, causing depressed delayed-type hypersensitivity and T-cell counts, as well as an increased risk of bacterial infections.7
25
CLINICAL FEATURES
CLINICAL FEATURES
Measles infection is characterized by an incubation period, prodrome and exanthem. The incubation period from acquiring the virus to developing fever ranges between 7 and 21 days. The prodrome consists of fever (as high as 40.5°C [104.9°F]), malaise, conjunctivitis (palpebral, extending to lid margin), coryza, and cough (brassy or barking) and can last up to 4 days. Koplik spots are the pathognomonic enanthem of measles and develop during the prodrome. The spots begin as small, bright red macules that have a 1- to 2-mm blue-white speck within them and are typically found on the buccal mucosa near the second molars (Fig. 163-1). Koplik spots typically occur 48 hours prior to the onset of the rash and only last 12 to 72 hours. Koplik’ spots may be absent if a patient presents several days into the patient’s rash.8
The measles exanthem consists of nonpruritic, erythematous macules and papules progressing in a cranial-to-caudal direction. The exanthem begins on the forehead and behind the ears (Fig. 163-2) and spreads to involve the neck, trunk, and extremities (Fig. 163-3). The hands and feet are involved. Lesions may coalesce, especially on the face and neck. The rash usually peaks within 3 days and begins to disappear in 4 to 5 days in the order that it appeared. Desquamation and brownish dyspigmentation in fair patients can occur as the rash resolves.8
DIAGNOSIS
DIAGNOSIS
The laboratory diagnosis of measles is based on virus detection or positive serologic findings. The measles virus can be isolated using real-time reverse transcription polymerase chain reaction (PCR) from nasopharyngeal aspirates, throat swabs, blood or urine. Viral
2990
detection is most successful when collection occurs within 3 days of the rash’s onset. Serologic studies are also very useful in confirming the diagnosis of measles. Enzyme-linked immunoassays are commonly used. A positive serum immunoglobulin (Ig) M antibody for measles confirms the diagnosis. IgM testing is typically positive on the first day of the rash and remains positive for at least 30 days afterward. Within the first 72 hours of the rash, the IgM assay may be falsely negative, so repeat testing should be considered if there is a high clinical suspicion.9
IgG confirmation of a measles diagnosis requires
documentation of a fourfold increase in titers, therefore serum samples should be drawn during the rash and weeks later during the convalescent stage. In the United States, measles should be reported to the local or state health department which can also help with selecting and processing laboratory tests.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Uncomplicated measles is self-limited, lasting 10 to 12 days. An infected patient is considered to be contagious 5 days prior to the onset of the rash until 4 days after the onset of the rash. Complications from measles infection occur in approximately 40% of cases.8 Complications include severe diarrhea; pneumonia (either viral or superimposed bacterial infection); otitis media; transient immunosuppression with lymphopenia and decreased cell-mediated immunity; encephalitis, and a rare form of a progressive neurodegenerative disease termed subacute sclerosing panencephalitis. Most deaths are attributed to either respiratory illness or encephalitis. In developing nations, measles remains a major cause of infant mortality. Patient groups at risk for complications include infants, the elderly, pregnant women, the immunocompromised, and the malnourished.
MANAGEMENT
MANAGEMENT
The management of measles is supportive as there are no specific antiviral therapies approved Table 163-2). Treatment focuses on antipyretics, fluids,
Most Likely
■Drug hypersensitivity reaction
■Rubella
Consider
■Henoch-Schönlein purpura (atypical cases)
■Other viral infection (parvovirus, enterovirus, adenovirus, human herpesvirus-6, Epstein-Barr virus)
■Rocky Mountain spotted fever (atypical cases)
Always Rule Out
Always Rule Out
■Graft-versus-host disease (recent bone marrow transplantation)
■Graft-versus-host disease (recent bone marrow transplantation)
■Kawasaki disease
■Kawasaki disease
25
■First-line
■First-line
■Immunoglobulin, IMa
■Immunoglobulin, IMa
■Measles vaccine
■Measles vaccine
■Supportive care
■Supportive care
■Treat secondary infections
■Treat secondary infections
■Vitamin Aa
■Vitamin Aa
■Second-line
■Second-line
■Ribavirina
■Ribavirina
aIn select cases; please see text.
and managing complications related to bacterial superinfection, respiratory compromise, and neurologic sequela. In the hospitalized setting, patients should be on standard and airborne transmission precautions for 4 days after the rash onset (entire duration of illness in immunocompromised patients).10 The World Health Organization recommends that vitamin A should be administered to all children with measles regardless of their country of residence.8 Vitamin A deficiency is associated with increased disease severity and risk for complications, likely through depressing cell-mediated immunity. A 2005 Cochrane review of vitamin A supplementation to treat measles in children found an association between using vitamin A (200,000 international units per day or 100,000 international units per day for infants) on 2 consecutive days and a reduced risk of measles mortality in children younger than 2 years old.11
Ribavirin is a medication that has been used in children with severe disease or an immunocompromised state. A randomized trial of 100 children found decreased duration of symptoms, hospital stay, and risk of complications in children receiving ribavirin compared to supportive therapy.12 However, larger studies are needed prior to recommending this therapy as part of routine practice. Postexposure prophylaxis plays an important role in curtailing outbreaks and decreasing morbidity of the virus. Individuals at risk for severe illness and complications (infants younger than 1 year of age, pregnant women, unimmunized, and immunocompromised) should be given measles immunoglobulin if presenting within 6 days of exposure. Measles immunoglobulin can be given either via an IM (0.5 mL/kg; maximum dose: 15 mL) or IV route (400 mg/kg). In healthy individuals, the measlesmumps-rubella (MMR) vaccine should be given to boost immunity if it can be administered within 72 hours of measles exposure.10
PREVENTION (IMMUNIZATIONS)
PREVENTION
(IMMUNIZATIONS)
The incidence of measles has decreased worldwide as a direct result of immunization. Two doses of the
2991
25
live-attenuated measles vaccine (with the first dose at or after 12 months of age) produces detectable levels of antibody in 99% of individuals, conferring lifelong immunity.10 The measles vaccine is typically administered in the form of combination vaccines: MMR vaccine or MMR and varicella vaccine. The second dose of the vaccine should be administered no sooner than 28 days later. The American Academy of Pediatrics, recommends MMR at age 12 to 15 months and then again prior to school entry, between 4 and 6 years old. Measles vaccine administration is contraindicated in individuals who have a moderate to severe illness, as well as in those who have had an immediate anaphylactic reaction to a previous measles vaccine. It is also contraindicated in pregnant women and those with impaired immune systems (HIV infection, immunosuppressive therapy). Hypersensitivity reactions can occur to components of the vaccine, such as gelatin, neomycin, or egg white cross-reacting proteins.10
RUBELLA
AT-A-GLANCE
■ Also called German measles and 3-day measles.
■ Epidemic disease; worldwide distribution.
■ Short prodrome; rash duration of 2 to 3 days.
■ Enlargement of cervical, suboccipital, and postauricular glands.
■ High risk of fetal malformations with congenital infection (microcephaly, congenital heart disease, and deafness), particularly in the first trimester.
EPIDEMIOLOGY
EPIDEMIOLOGY
Rubella virus has a worldwide distribution with outbreaks occurring most frequently in late winter and early spring months. Humans are the only hosts for infection.13 School-age children, adolescents, and young adults most often develop the disease. Epidemics occasionally occur in developing countries, especially where vaccines are unavailable. Since introduction of the rubella vaccine in the United States in 1969, the incidences of rubella and congenital rubella syndrome have drastically declined with no widespread epidemics occurring in the United States. Since 2003, fewer than 20 cases are reported annually in the United States.14 Occasional outbreaks have largely been attributed to failure to vaccinate susceptible individuals. Yet, recent serologic surveys indicate that approximately 10% of the United States–born population older than age 5 years is susceptible to rubella.13,14 Epidemiologic studies have identified that individuals born outside the country or in a vaccine-poor area have an increased risk of rubella.13
2992
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Rubella is an enveloped positive-stranded RNA virus in the Togaviridae family that is spread through direct or droplet contact from nasopharyngeal secretions.13
Infected individuals shed virus for 5 to 7 days before and up to 14 days after onset of rash,15 with viremia unlikely after the rash occurs. In most individuals, infection leads to lifelong immunity. Congenital rubella occurs when a nonimmunized, susceptible, pregnant woman is exposed to the virus. Transplacental infection of the fetus occurs during the viremic stage. The risk is greatest to a fetus exposed to the virus in the first trimester. Congenitally infected infants may shed the virus through urine, blood, and nasopharyngeal secretions for up to 12 months after birth, thus being a potential source of viral exposure to other susceptible individuals.13,15
CLINICAL FINDINGS
CLINICAL FINDINGS
HISTORY
Primary rubella infection is typically a mild, subclinical disease, particularly in adults.13,15 The prodrome is characterized by low-grade fever, myalgia, headache, conjunctivitis, rhinitis, cough, sore throat, and lymphadenopathy; symptoms that may last up to 4 days and often resolve with appearance of rash. Up to 50% of children with primary rubella infection may have a subclinical infection or present only with lymphadenopathy or rash (no prodrome).15 Conversely, older adults may have more-severe and persistent prodromal symptoms that may make distinction from rubeola difficult in some situations. The presence of Koplik spots in the mouth favors rubeola. As the prodrome resolves and the rash begins to appear, some patients develop an enanthem consisting of tiny red macules on the soft palate and uvula (Forchheimer spots).16 This enanthem is not diagnostic for rubella.
CUTANEOUS LESIONS
The exanthem, occurring 14 to 17 days after exposure, is characterized by pruritic pink to red macules and papules that begin on the face, quickly progressing to involve neck, trunk, and extremities (Fig. 163-4).15 Lesions on the trunk may coalesce, whereas those on the extremities often remain more discrete. The rash usually begins to disappear in 2 to 3 days, unlike rubeola, which can be more persistent and clears the head and neck first. Desquamation may follow resolution of the rash.
RELATED PHYSICAL FINDINGS
Lymphadenopathy is usually most severe in the posterior cervical, suboccipital, and postauricular lymph
nodes, and is noted up to 7 days before the rash appears.13 Enlargement of the nodes may persist for several weeks. Adults, particularly women (up to 70%), may develop arthritis of small and large joints with rubella infection.13 Joint symptoms often first appear as the rash fades and can last several weeks. In some individuals, the symptoms may become persistent or recurrent, and joint swelling may progress to joint effusion.
DIAGNOSIS
DIAGNOSIS
Diagnosis is typically made using serology to detect rubella-specific IgM antibody (up to 8 weeks after infection) or to document a fourfold rise in antibody titer in acute and convalescent-phase serum.16 As with measles, rubella cases should be reported to local or state health departments. Viral culture (nose, throat, blood, urine, cerebrospinal fluid [CSF], and synovial fluid) is sensitive but often difficult because of the influence of timing, collection procedure, and transport on the specimen.17 Reverse transcription PCR may be used to detect rubella virus from throat swab or oral fluid with subsequent genotyping of strains to identify a source during outbreaks.17 Complete blood cell count usually shows leukopenia with relative neutropenia. Increased numbers of atypical lymphocytes or abundant plasma cells may be noted as well. Patients with meningeal involvement have lymphocytes in the CSF.
25
CONGENITAL RUBELLA SYNDROME
CONGENITAL RUBELLA
SYNDROME
Women who are infected with rubella during pregnancy may only exhibit minor clinical symptoms, however the effects of rubella infection on the fetus can be profound.15 The greatest risk of fetal malformation is in the early stages of pregnancy. Up to 85% of fetuses exposed to rubella within the first 12 weeks of gestation develop serious sequelae such as microcephaly with mental retardation; congenital heart disease (ventricular septal defect, patent ductus arteriosus, pulmonary artery stenosis); sensorineural deafness; cataracts; glaucoma; low birthweight; and fetal death.14-16 Neonatal manifestations of congenital infection include growth retardation, interstitial pneumonitis, radiolucent bone disease, hepatosplenomegaly, thrombocytopenia, and dermal erythropoiesis (“blueberry muffin lesions”).13
Diagnosis of congenital rubella infection is obtained by isolating rubella virus in the throat, cataracts, urine, or CSF of the affected neonate. Serologic testing is not as sensitive, but is easily available for confirmatory testing. IgM antibody can be detected from birth to 1 month of age; IgG antibody titers may be stable or increase over several months. Laboratory confirmation of congenital infection in children older than age 1 year is difficult as viral isolation is rare.13,15
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Rubella is typically a self-limited disease. Infants who have congenital rubella are infectious until viral shedding from the nasopharynx and urinary tract ends.
Most Likely
■Drug hypersensitivity reaction
■Rubeola (measles)
Consider
■Other viral infection (enterovirus, adenovirus, parvovirus, human herpesvirus-6)
Always Rule Out
Always Rule Out
■Streptococcal scarlet fever For the differential diagnosis of congenital rubella syndrome with blueberry muffin lesions, see Table 163-10.
■Streptococcal scarlet fever For the differential diagnosis of congenital rubella syndrome with
2993
blueberry muffin lesions, see Table 163-10.
25
The majority of infants (85%) infected in utero excrete virus in the first month of life; 1% to 3% of infants infected in utero continue to excrete virus in the second year of life.13,16 Pregnant women caring for these infants are at risk for developing rubella. Clinical course depends on how severely affected the fetus is from intrauterine infection. Rarely, rubella infection may lead to encephalitis (1 in 6000 cases), with mortality rates varying from 0% to 50%.16 Other rare complications include peripheral neuritis, optic neuritis, encephalitis, myocarditis, pericarditis, hepatitis, orchitis, hemolytic anemia, thrombocytopenia, and hemophagocytic syndrome.15
MANAGEMENT
MANAGEMENT
Treatment of primary, uncomplicated rubella is supportive. Standard and droplet precautions are recommended for patients with rubella for 7 days after rash onset.13 In nonpregnant individuals, rubella vaccine administration within 3 days of exposure theoretically may prevent illness, although this is yet to be proven.13
Limited data indicate that IM immunoglobulin (0.55 mL/kg) as postexposure prophylaxis for rubellasusceptible patients may decrease infection, viral shedding, and rate of viremia.13,18
Neonates with congenital rubella syndrome require supportive care as well as appropriate attention to significant health issues. These infants are contagious and should be isolated to prevent transmission to susceptible individuals.13,15 Contact isolation is recommended for these infants until they are at least 12 months old or repeated cultures are negative after 3 months of age.13
PREVENTION (IMMUNIZATIONS)
PREVENTION
(IMMUNIZATIONS)
Rubella vaccine is typically administered as part of a threefold vaccine (MMR) or fourfold vaccine (MMR and varicella) at 12 to 15 months of age and again at 4 to 6 years of age. Seroconversion after a single dose of MMR vaccine occurs in 95% of individuals.13,14 It is imperative that individuals at risk for rubella infection are immunized, such as health care workers, military recruits, college students, and recent immigrants.13
Potential adverse reactions to rubella vaccine occur in susceptible individuals and include fever (6 to 12 days after vaccine), morbilliform rash, lymphadenopathy, and arthralgia. Febrile seizures occur more frequently in children 1 to 2 years old when receiving the first MMR vaccine.13
Pregnant women should not receive the rubella vaccine because of the theoretical risk to the fetus.19
Any woman receiving the rubella vaccine should not become pregnant for 28 days. Infants of vaccinated breastfeeding mothers may become infected with rubella via breastmilk. Typically, they develop a mild
2994
erythematous exanthem of macules and papules with no serious effects.16
Certain immunosuppressed and immunodeficient patients should not be vaccinated with live-attenuated virus vaccines, including rubella. Vaccine strain rubella virus has been found in cutaneous granulomas in immunodeficient hosts.20
ERYTHEMA INFECTIOSUM AND PARVOVIRUS B19 INFECTION
AT-A-GLANCE
■ Erythema infectiosum (fifth disease): childhood illness with “slapped cheeks” followed by an erythematous, lacy eruption on the trunk and extremities.
■ Symmetric polyarthritis, particularly of the small joints in adults.
■ Papular purpuric gloves-and-socks syndrome: pruritic erythema, edema, and petechiae of the hands and feet, fever, and oral erosions in adolescents.
■ Aplastic crisis in patients with increased red blood cell turnover, chronic anemia in immunocompromised persons, and fetal hydrops.
EPIDEMIOLOGY
EPIDEMIOLOGY
Erythema infectiosum (fifth disease) is worldwide in distribution, can occur throughout the year, and can affect all ages. It tends to occur in epidemics, especially associated with school outbreaks in the late winter and early spring. Serologic studies show increasing prevalence of antibodies with age—from 15% to 60% of children 5 to 19 years of age to more than 90% in the elderly.21 Previous infection with B19 seems to confer lifelong immunity. The incubation period for erythema infectiosum is from 4 to 14 days. Low-grade fever and nonspecific complaints occur at the time of viremia, 6 to 14 days after inoculation, followed by rash at day 17 or 18.22
Parvovirus B19 is thought to be transmitted primarily by the respiratory route via aerosolized droplets during the viremic phase.22 After the rash of erythema infectiosum appears, B19 is usually not found in respiratory secretions or serum, suggesting that persons with erythema infectiosum are infectious only before the onset of the rash. The virus seems to be effectively spread after close contact. The secondary attack rate among susceptible household contacts is approximately 50%. Transmission may occur via blood transfusion, from blood products, and vertically from mother to fetus.23
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The B19 virus belongs to the family Parvoviridae and the genus Erythrovirus. B19 lacks an envelope and contains single-stranded DNA. It is the smallest single-stranded DNA-containing virus known to infect humans, measuring 18 to 26 µm in diameter. Parvoviruses are widespread in veterinary medicine, but animal parvoviruses are not thought to be transmissible to humans.24
The more serious manifestations of parvovirus infection relate to the fact that the virus infects and lyses erythroid progenitor cells. The blood group P antigen (globoside) is a receptor of parvovirus. Because some individuals lack P antigen, they are not susceptible to infection with B19.25 In patients with increased red blood cell destruction or loss who depend on compensatory increases in red cell production to maintain stable red cell indices, B19 infection may lead to transient aplastic crisis. Such patients include those with anemia associated with acute or chronic blood loss. When parvovirus infects the erythroblasts in a developing fetus with decreased red cell survival, the result may be hemolysis and anemia. Anemia may trigger congestive heart failure, edema (fetal hydrops), and possibly fetal death. Additionally, parvovirus B19 DNA can be detected in nonerythroid tissues and is associated with increased inflammatory gene expression in these tissues.26 Immune complex deposition also has been implicated in some of the manifestations of B19 infection, including erythema infectiosum.
CLINICAL FEATURES
CLINICAL FEATURES
PARVOVIRUS B19 IN CHILDREN
Most infections caused by B19 are asymptomatic and unrecognized. Fifth disease, the most common clinical picture associated with the virus, usually begins with nonspecific symptoms such as headache, coryza, and low-grade fever approximately 2 days before the onset of the rash.27 Patients may have headache, pharyngitis, fever, malaise, myalgia, coryza, diarrhea, nausea, cough, and conjunctivitis coinciding with the rash. Approximately 10% of children with erythema infectiosum develop arthralgia or arthritis. Large joints are affected more often than small joints.28 Occasionally, children may present with chronic joint complaints suggestive of juvenile idiopathic arthritis. The characteristic rash begins with confluent, erythematous, edematous plaques on the malar eminences, the “slapped cheeks” (Fig. 163-5). As the facial rash fades over 1 to 4 days, pink to erythematous macules or papules appear on the trunk, neck, and extensor surfaces of the extremities. These lesions have some central fading, giving them a lacy or reticulated appearance (Fig. 163-6).27 The rash can be morbilliform, confluent, circinate, or annular, and there are reports of palmar and plantar involvement.28 The eruption
25
typically lasts 5 to 9 days, but can recur for weeks or months with triggers such as sunlight, exercise, temperature change, bathing, and emotional stress. In some outbreaks, pruritus is a major feature of the rash in children.28
There have been occasional reports of parvovirus B19 associated with generalized petechiae, and vascular purpura, including Henoch–Schönlein purpura.29,30
A microvesicular eruption also has been reported.31 An enanthem consisting of erythema of the tongue and pharynx and red macules on the buccal mucosa and palate can occur.
2995
25
PARVOVIRUS B19 IN ADULTS
Acute arthropathy is the primary manifestation of B19 viral infection in adults.32 It occurs mainly in women and affects the knees and the small joints of the hands. Other joints, such as the spine and costochondral joints, are occasionally involved. This symmetric polyarthritis is usually of sudden onset and is self-limited but can be persistent or recurrent for months. It may mimic Lyme arthritis or rheumatoid arthritis. The constitutional symptoms are usually more severe in adults than in children. Fever, adenopathy, and a mild arthritis without a rash is the usual course. Women are more likely than men to have joint complaints and rash, whereas men often present with only a flu-like illness.32 Some adults may have fatigue, malaise, and depression for weeks after the infection. Asymptomatic infection can certainly occur in adults as well as in children. Numbness and tingling of the fingers and pruritus have been reported with or without a rash.33 It has been suggested that if pruritus is a complaint in a patient with acute-onset arthritis, parvovirus should be considered as a possible cause. The rash in adults, if present at all, is usually macular and blotchy or lacy, often on the extremities, and rarely demonstrates the characteristic slapped-cheek appearance.32 Other cutaneous manifestations associated with B19 infection in adults include purpura, vesicles and pustules, palmoplantar desquamation, a morbilliform exanthema, occasional oral petechiae and small erosions, and livedo reticularis.
PAPULAR PURPURIC GLOVES- AND-SOCKS SYNDROME
In 1990, a unique syndrome of pruritic erythema and edema of the hands and feet with petechiae, fever, and oral erosions was described.34 This rare exanthem, now known as papular purpuric gloves-and-socks syndrome, seems to affect teenagers and adults. However, it also can affect children.35 Patients usually have mild prodromal symptoms of fatigue and low-grade fever, myalgia, and arthralgia. Subsequently, itchy, painful, symmetric edema and erythema of the distal hands and feet occurs. Purpuric papules appear on the hands and feet with abrupt demarcation at the wrists and ankles. The enanthem, if present, arises on the lips, soft palate, and buccal mucosa. The syndrome resolves spontaneously within 2 weeks. Importantly, papular purpuric gloves-and-socks syndrome is contagious when the eruption is present, in contrast to erythema infectiosum.
DIAGNOSIS
DIAGNOSIS
LABORATORY TESTING
In patients with erythema infectiosum, laboratory results are usually normal. Patients with aplastic crisis
2996
have reticulocytopenia and anemia, the severity of which depends on the degree of underlying anemia. Reticulocytopenia, anemia, lymphopenia, neutropenia, and thrombocytopenia can occur in healthy individuals with B19 infection, although these are usually not significant enough to cause clinical symptoms. The erythrocyte sedimentation rate is rarely elevated, and in some cases of parvovirus-associated arthritis, rheumatoid factor has been positive. Detection of recent infection is usually performed with assays for IgM antibody. IgM can be detected within a few days after onset of illness and is present for up to 6 months in many cases, although there is a decline in titer in the second month after onset. The sensitivity of IgM ranges from 62% to 70%. IgG can be identified by the seventh day of illness and lasts for years and is therefore best for documenting past infection. Parvovirus antibody is often not detectable in immunodeficient persons. PCR is used to detect B19 DNA. This technique is considered one of the most sensitive approaches for detection of the virus within a number of different specimens including serum or plasma, amniotic fluid, placental or fetal tissue, or bone marrow. It is considered the test of choice in an immunocompromised patient, and to confirm fetal infection. One caveat is that parvovirus DNA fragments may be present for more than a year after infection, however this does not always indicate that the viable virus is present.36 PCR should be used along with IgM and IgG in pregnant patients.37
PATHOLOGY
The histopathologic changes in the skin of patients with erythema infectiosum include a sparse superficial perivascular lymphocytic infiltrate that is not considered diagnostic. Immunohistochemical techniques can be used to detect B19 parvovirus antigen in a number of different tissues.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
PROGNOSIS AND CLINICAL COURSE
PROGNOSIS AND
CLINICAL COURSE
Parvovirus B19 infection in healthy individuals is selflimited. The eruption of erythema infectiosum and the parvovirus arthropathy usually resolve in 1 to 2 weeks, but can recur or persist for months. If untreated, transient aplastic crisis can be fatal, but most patients recover in 1 week. Chronic anemia from B19 usually resolves if treated with γ-globulin. Fetal hydrops can lead to fetal death if not treated.
Most Likely
■Drug reaction
■Enteroviral infection
■Erysipelas on the cheek
■Erythema infectiosum
■Hand-foot-mouth disease
■Papular purpuric gloves-and-socks syndrome
Consider
■Atypical measles
■Collagen vascular disease (systemic lupus erythematosus, dermatomyositis)
■Erythema infectiosum
■Measles
■Papular purpuric gloves-and-socks syndrome
■Roseola
■Rubella
Always Rule Out
Always Rule Out
■Kawasaki disease
■Kawasaki disease
■Rocky Mountain spotted fever
■Rocky Mountain spotted fever
■Scarlet fever
■Scarlet fever
COMPLICATIONS
COMPLICATIONS
An increasing number of complications from parvovirus B19 are now recognized. Subclinical infection is quite common. However, this virus can be responsible for a variety of hematologic, rheumatologic, and neurologic abnormalities.
TRANSIENT APLASTIC CRISIS
Parvovirus B19 is the most common cause of transient aplastic crisis in patients with chronic hemolytic anemias,38 as well as in other conditions of decreased red cell production or increased red cell destruction. The aplastic crisis may be the initial manifestation of the underlying hematologic disease. Patients typically have fever and constitutional complaints, followed 1 week later by fatigue, pallor, and worsening anemia.38
Cutaneous manifestations are rarely seen with the aplastic crisis. The hemoglobin may fall below 4 µg/dL and is not associated with reticulocyte production. Bone marrow examination shows hypoplasia or aplasia of the erythroid series. Red blood cell transfusion may be necessary, and most patients recover in 1 week, although the problem can be fatal if untreated. Transient red cell aplasia can occur in healthy persons without underlying hematologic abnormalities.38 It is likely that the aplasia is missed in individuals without disorders of shortened erythrocyte survival because the hemoglobin does not drop low enough to cause symptoms.
CHRONIC B19 INFECTION
In immunocompromised patients, B19 infection can cause a serious, prolonged anemia from persistent
25
lysis of red blood cell precursors.39 Parvovirus-related chronic anemia has been reported in HIV-infected patients, as well as in transplantation recipients and those with congenital immunodeficiencies, acute leukemias, lupus erythematosus, and during the first year of life without immunodeficiency. These patients respond dramatically to IV γ-globulin, suggesting that antibody is the main defense to human parvovirus infection.39
FETAL B19 INFECTION
Fetal infection with B19 may result in either an unaffected fetus or spontaneous abortion (especially in the first half of pregnancy), hydrops fetalis in the second half of pregnancy, congenital anemia, and even late fetal death.37 Nonimmune fetal hydrops is the most common complication of intrauterine infection with B19. Because B19 virus can infect erythroid precursors, extensive hemolysis can occur in the fetus, leading to severe anemia, tissue anoxia, high-output heart failure, and generalized edema. The fetus may show ultrasonographic evidence of subcutaneous edema, ascites, pleural effusion, pericardial effusion, placental edema, and polyhydramnios. The overall risk of fetal death is not clearly known, but recent studies suggest that this risk is approximately 6.5% with maternal infection.37 The risk of fetal death for a woman with unknown serologic status is estimated to be less than 2.5% after a household exposure and less than 1.5% after a significant work exposure. It seems that in B19-infected pregnant women, 33% to 50% of fetuses are infected, with an adverse outcome in 10% of infected fetuses.37,40 Furthermore, approximately 50% of women of childbearing age are immune to parvovirus infection because of prior infection. Because parvoviruses are known teratogens in animals, there has been much concern about whether they cause birth defects in humans, but it appears that parvovirus B19 is not a common cause of birth defects.
OTHER COMPLICATIONS
There are reports of B19 infection causing encephalitis, meningitis, brachial neuritis, a myasthenia-like syndrome, and motor weakness. Parvovirus infection has been blamed for a granulomatosis with polyangiitis (Wegener) illness, polyarteritis nodosa, Kawasaki disease, and a systemic lupus erythematosus-like picture.41-43 In addition, there are reports of other hematologic complications, including idiopathic thrombocytopenic purpura, transient neutropenia, myocarditis, a hemophagocytic syndrome, and the Blackfan-Diamond syndrome.
TREATMENT
TREATMENT
There is no specific treatment available for parvovirus B19 infection. Erythema infectiosum is a benign
2997
25
■Erythema infectiosum
■Erythema infectiosum
Supportive treatment of fatigue, malaise, pruritus, arthralgia IV immunoglobulin Oxygen and/or blood transfusion may be necessary Possible intrauterine exchange transfusion
Supportive treatment of fatigue,
■Chronic anemia
■Chronic anemia
malaise, pruritus, arthralgia IV immunoglobulin Oxygen and/or blood transfusion may
■Transient aplastic crisis
■Transient aplastic crisis
■Hydrops fetalis
■Hydrops fetalis
be necessary Possible intrauterine exchange
transfusion
condition, and usually no treatment is necessary. Supportive therapy for relief of fatigue, malaise, pruritus, and arthralgia may be needed. The chronic anemia of persistent B19 infection may be treated successfully with commercially available IV immunoglobulin,, which contains neutralizing anti-B19 antibodies. Transient aplastic crisis, which can be life-threatening, may require oxygen therapy and blood transfusion. Serologic testing for B19 IgG and IgM should be offered to pregnant women who are exposed to parvovirus B19. Infected pregnant women are followed by frequent ultrasonograms. Evidence of hydrops fetalis warrants umbilical cordocentesis to check for anemia, viral DNA, IgG, and IgM. The management of infected fetuses is controversial. Some physicians advocate observation because spontaneous resolution is common. Fetuses with severe anemia and compromise are usually managed with intrauterine exchange transfusion, but this procedure does carry risk Table 163-5).
PREVENTION
PREVENTION
There is currently no vaccine to prevent parvovirus B19 infection. Vaccine development has been problematic; however, Phase II clinical trials have been completed.44 It is not known whether immunoglobulin given around the time of exposure prevents infection or alters the course of the disease. Because patients with erythema infectiosum are no longer infectious by the time they develop the illness, control measures directed toward these individuals are not likely to be effective. If these persons are hospitalized, no special precautions need to be taken. Because the virus is transmitted before the rash appears, the disease is easily spread in situations of close prolonged contact such as schools, day care centers, workplaces, and homes. Patients with aplastic crisis or immunosuppression with chronic B19 anemia may have high-titer viremia and are particularly infectious. These individuals should be placed in respiratory and contact isolation if hospitalized, and pregnant health care providers should not care for them directly. Hospital workers are at risk of contracting nosocomial infections from these patients and could spread the virus to patients if adequate precautions are not taken.
2998
EPSTEIN-BARR VIRUS
AT-A-GLANCE
■ Epstein-Barr virus is also known as human herpesvirus 4.
■ In developed countries, primary infection most often occurs during adolescence/early adulthood.
■ Infectious mononucleosis is characterized by the triad of fever, lymphadenopathy, and pharyngitis.
■ Morbilliform exanthem with primary infection; most common after administration of ampicillin or amoxicillin.
■ Oral hairy leukoplakia, nasopharyngeal carcinoma, Burkitt lymphoma, Hodgkin disease, Kikuchi histiocytic necrotizing lymphadenitis, and certain types of cutaneous T-cell lymphoma are associated with Epstein-Barr virus infection.
Ebstein-Barr virus (EBV), also known as human herpesvirus 4, is a ubiquitous viral infection. Primary infection occurs early in life followed by lifelong, latent infection. EBV has been implicated in a diverse set of inflammatory dermatologic disorders and neoplasms. The manifestations of EBV infection are strongly influenced by the patient’s age and immunologic status.
EPIDEMIOLOGY
EPIDEMIOLOGY
EBV is a worldwide pathogen with more than 90% of adults latently infected.45 The age of onset of primary EBV infection is in part dependent on geographic location and socioeconomic status. Patients from developing countries or of lower socioeconomic status are more likely to acquire EBV during early childhood. Early childhood EBV infection is frequently asymptomatic or nonspecific in presentation and does not present with infectious mononucleosis, a manifestation characteristic of EBV infection during adolescence and young adulthood. Within in the United States, 50% of 6- to 8-year-old children are seropositive for EBV.46
The rest of the population acquires EBV infection later in life with 89% of the population becoming seropositive by 18 to 19 years old.46 Risk factors for early seropositivity include lower household income, parental education level, uninsured status, and being Mexican American or Black (non-Hispanic).46
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
EBV is an enveloped, double-stranded DNA virus with a genome that encodes approximately 100 proteins.
EBV exists as 2 distinct types, EBV-1 and EBV-2, but no specific differences in symptoms or disease associations have been identified between the two. EBV-1 is found worldwide and EBV-2 infection occurs most often in Africa.47
EBV is typically transmitted via saliva from patients with recent primary infection or from low-grade viral shedding in patients with latent EBV infection. After infectious mononucleosis, viral shedding continues for a median duration of 6 months.48 The virus also has been isolated from breastmilk, cervical epithelial cells, and semen.49
EBV often first infects oropharyngeal epithelial cells with subsequent infection of B-lymphocytes in the oropharynx.50 EBV infects B lymphocytes through the binding of the EBV glycoprotein gp350 with CD21 on the surface of B cells. The infected B cells are then activated, and their population is expanded.51 These B lymphocytes allow dissemination of the virus throughout the lymphoreticular system. A clonal expansion of cytotoxic T lymphocytes allows recovery from primary and reactivation infection and is the source of the atypical lymphocytes associated with EBV infection.52 Symptoms occur after a 4- to 8-week incubation period and likely result from this immunologic response. EBV establishes an indefinite latent infection within B cells. EBV can periodically reactivate and be shed in oral secretions. An impaired cellular immune system can result in poorly controlled primary EBV infection, EBV reactivation, and promote EBV-induced malignancy. Both X-linked lymphoproliferative disease and GATA2 deficiency are inherited immunodeficiencies particularly associated with impaired immune responses to EBV infection.53
CLINICAL FEATURES
CLINICAL FEATURES
INFECTIOUS MONONUCLEOSIS
EBV is transmitted through bodily fluids, especially saliva, and then infects the oropharyngeal epithelium. An incubation period of 30 to 50 days occurs prior to symptoms.54 The most common manifestation of EBV infection in adolescents and adults is infectious mononucleosis, also referred to as the “kissing disease.” Infectious mononucleosis presents with the classic triad of fever, lymphadenopathy, and pharyngitis in approximately 50% of cases.55 Fevers can last 1 to 3 weeks and lymphadenopathy can be tender and frequently found in the posterior cervical chain. Accompanying pharyngitis can vary in intensity from mild erythema to grossly enlarged tonsils with white exudate that can impact breathing. Other systemic features include fatigue, headache, mild transaminitis, cytopenias, and atypical lymphocytosis. EBV can infect nearly every organ. Complications of infectious mononucleosis occur in approximately 20% of patients and include airway obstruction, autoimmune hemolytic anemia or thrombocytopenia,
25
neutropenia, myocarditis, and hepatitis. Splenomegaly occurs in 50% of patients and typically resolves by the fourth to sixth week of illness.56 Splenic rupture is a rare, potentially life-threatening complication more common in young men. The risk of splenic rupture is estimated at 0.1% and is spontaneous in greater than 50% of cases.57 EBV also is associated with various neurologic complications that typically occur within 1 month of illness including aseptic meningitis, transverse myelitis, peripheral neuritis, Guillain-Barré syndrome, and cranial nerve palsies.55
EBV infection during pregnancy is not thought to be teratogenic.58
Cutaneous eruptions with infectious mononucleosis occur in up to 25% of cases and can adopt a morbilliform, scarlatiniform, urticarial, erythema multiforme-like, or petechial morphology.59 Eruptions also frequently occur when patients with infectious mononucleosis are treated with antibiotics, classically ampicillin. This association was first described in the 1960s and coined the ampicillin rash.60 Beginning 7 to 10 days after the initiation of ampicillin, patients develop a generalized, pruritic, morbilliform rash with an erythematous or copper color that resolves in a week (Fig. 163-7). This eruption also has been reported with other antibiotics, such as amoxicillin, cephalexin, erythromycin, and levofloxacin. Ampicillin rash was originally cited as occurring in up to 100% of antibiotic-exposed patients, but the current literature indicates a much lower rate of only 30%.59 The rash is thought to be a result of EBVinduced antibodies that are produced in response to
2999
25
the administered drug and form complement-fixing immune complexes.61 The exanthem does not usually indicate a permanent allergy to the medication.62
NON–SEXUALLY RELATED ACUTE GENITAL ULCERS
EBV infection also has been implicated in the development of non–sexually related acute genital ulcers or Lipschütz ulcers.63 Lipschütz ulcers frequently occur in prepubertal or adolescent females and present as painful, multiple ulcers with red-purple ragged edges on the medial or outer surface of the labia minora. The ulcers are often deep with a necrotic or fibrinous base and can adopt a “kissing” pattern if symmetric.49 Inguinal lymphadenopathy can also be frequently found on exam. Less common locations for Lipschutz ulcers include the labia majora and inner thighs. Ulcers can also occur in males with involvement of the scrotum (Fig. 163-8). EBV-associated genital ulcers are not recurrent and self-resolve in 2 to 6 weeks. Patients may be misdiagnosed as having herpes simplex infections, Behçet disease, or as victims of sexual abuse. The role of EBV in these ulcers has been confirmed by the detection of EBV DNA via PCR from ulcers and serology confirming acute infection.64 Other infectious implicated in causing Lipschütz ulcers include cytomegalovirus (CMV), group A Streptococcus, mumps, Salmonella, toxoplasmosis, influenza A virus, and Mycoplasma pneumoniae.49
OTHER NONNEOPLASTIC ASSOCIATIONS WITH EPSTEIN-BARR VIRUS
EBV infection also is associated with multiple inflammatory dermatologic conditions, including
3000
Gianotti-Crosti syndrome when the infection occurs in young children, erythema multiforme, leukocytoclastic vasculitis, erythema nodosum, erythema annulare centrifugum, pityriasis lichenoides, granuloma annulare, and cold urticaria.49
NEOPLASTIC CONDITIONS
The latent infection established by EBV is linked to the development of several malignancies, including nasopharyngeal carcinoma, Burkitt lymphoma, and Hodgkin lymphoma Table 163-6).65 EBV-associated malignancies occur mainly in patients who are immunocompromised because of HIV infection or congenital immunodeficiency, and those who receive immunosuppressant therapy, such as organ transplant recipients. Latent EBV infection of lymphocytes may allow for their transformation, immortalization, and eventual malignant transformation.66 Different EBV genes are expressed in each type of malignancy and the biology is quite complex. Nasal-type extranodal natural killer/T cell lymphoma (ENK/T) is strongly associated with EBV.67
Hallmarks of this aggressive, non-Hodgkin lymphoma include a natural killer–cell phenotype (expression of CD2, CD56, and cytoplasmic CD3 but a lack of surface CD3), angioinvasion and necrosis.68 ENK/T is rare in the United States, Europe, and Africa, but is endemic in Asia, especially Southern China, and among native populations of Central and South America. Males are more commonly affected than females in a 2:1 ratio, and the tumor typically presents around 50 years of age.69 The nasal type presents with an ulcerated midfacial tumor, previously termed lethal midline granuloma, that can lead to nasal obstruction, facial swelling, sinusitis, and destruction of the underlying sinuses and palate. Extranasal ENK/T can also occur and involve the skin, soft tissue, GI tract, and testes. Radiation therapy is typically used for localized disease and combined with chemotherapy for advanced stages.
B-cell neoplasms
B-cell neoplasms
■EBV+ diffuse large B-cell lymphoma of the elderly
■EBV+ diffuse large B-cell lymphoma of the elderly
■Endemic Burkitt lymphoma
■Endemic Burkitt lymphoma
■Hodgkin lymphoma T-cell and natural killer cell neoplasms
■Hodgkin lymphoma T-cell and natural killer cell neoplasms
■Angioimmunoblastic T-cell lymphoma
■Angioimmunoblastic T-cell lymphoma
■Extranodal natural killer/T-cell lymphoma
■Extranodal natural killer/T-cell lymphoma
■Hydroa vacciniforme–like lymphoproliferative disease
■Hydroa vacciniforme–like lymphoproliferative disease
■Subcutaneous panniculitis-like T-cell lymphomaa
■Subcutaneous panniculitis-like T-cell lymphomaa
Hemophagocytic syndrome Leiomyosarcomab
Hemophagocytic syndrome Leiomyosarcomab
Posttransplantation lymphoproliferative disorder
Posttransplantation lymphoproliferative disorder
aMost cases of subcutaneous panniculitis T-cell lymphoma are sporadic but Epstein-Barr virus (EBV) positivity has been reported in Asian patients.
bEBV-associated smooth muscle tumors have been reported in immunocompromised children.
Another rare EBV-driven T-cell disorder is hydroa vacciniforme–like lymphoproliferative (HVLL) disease. HVLL disease affects children from Asia and Central and South America. Patients present similarly to photoinduced, self-resolving hydroa vacciniforme with the development of vesicles, crusting, and varicelliform scarring.70 However, HVLL is distinguished by systemic symptoms (fever, weight loss, hepatosplenomegaly, and lymphadenopathy), extensive facial edema, ulcerations and scarring, and lesions located in photoprotected sites.70 Histopathology reveals a monoclonal proliferation of T cells with a CD8 phenotype and less often a natural killer–cell phenotype.71 The clinical course is variable and patients can have prolonged periods of relapsing fevers and skin eruptions. Severe cases can progress to develop hematophagocytic syndrome and natural killer/T-cell lymphoma.70
GATA2 deficiency has been implicated in some cases of HVLL.53
Lymphomatoid granulomatosis is a rare, angioinvasive proliferation of EBV-infected B cells and a reactive, polyclonal T-cell population.72 Pulmonary involvement is seen in almost all patients presenting with cough, fever, and cavitary lung nodules that at times can mimic Wegner granulomatosis.66 Cutaneous involvement may be a presenting feature and is documented in up to 40% of cases.73 As a result of the angiocentric and destructive proliferation, patients may present with stellate ulceration and subcutaneous nodules for which the differential may include medium-vessel vasculitis/vasculopathy and angioinvasive opportunistic infections.74 A diagnosis of lymphomatoid granulomatosis should prompt a workup of an underlying immunodeficiency, as it has been described in the setting of immunosuppressive medications, congenital immunodeficiency, and autoimmune disease.75 Lymphomatoid granulomatosis most often presents in the fourth to sixth decade of life and requires the initiation of chemotherapy. EBV is also strongly associated with other B-cell neoplasms, including Burkitt lymphoma, Hodgkin lymphoma, and EBV+ diffuse large B-cell lymphoma of the elderly.
DIAGNOSIS
DIAGNOSIS
The diagnosis of infectious mononucleosis should be considered in adolescents and young adults who present with fever, fatigue, pharyngitis, and lymphadenopathy. Suggestive features of primary EBV infection include splenomegaly, posterior, as opposed to anterior, cervical lymphadenopathy and lymphocytosis with a predominance of atypical lymphocytes (defined as more than 10% of total lymphocytes). Other nonspecific laboratory abnormalities include mild neutropenia, thrombocytopenia, and transaminitis. Heterophile antibody and EBV-specific antibodies can be used to confirm an EBV infection. The monospot test is a heterophile antibody test frequently used to confirm infectious mononucleosis in adolescents
25
and adults with classic symptoms because of its rapid turnaround time and high specificity in the appropriate clinical setting. A heterophile antibody is an antibody that recognizes antigens on erythrocytes from a different specifies; in the case of the monospot test, it is antibodies against horse red blood cells produced in a person with an EBV infection. The sensitivity of rapid diagnosis heterophile antibody tests is approximately 85%.76 The monospot test may be negative in the first week of infection and is not a sensitive test for children younger than 4 years old.77
EBV-specific antibodies are often employed to confirm EBV infection in young children and when a suspicion for EBV infection remains high despite a negative heterophile antibody test. Host IgM and IgG antibodies form against viral capsid antigen (VCA) and are positive during acute infection. IgM VCA wanes 3 months after clinical illness and IgG VCA remains positive for life. EBV nuclear antigen (EBNA) is expressed when the virus establishes latency; consequently, IgG to EBNA becomes positive usually 6 to 12 weeks after symptoms develop. A positive IgM VCA and negative IgG EBNA confirms acute infection, whereas a positive IgG EBNA argues against an acute EBV infection. Lastly, antibodies to early antigen also can be tested and are present at the onset of the illness. IgG to early antigen exists as 2 subsets, anti-D and anti-R. Anti-D antibodies occur during recent infection and resolve with recovery. The clinical significance of anti-R antibodies is not clear.78
PCR-based assays to detect EBV viral load can be useful in detecting infection in immunocompromised states where a host’s antibody production may be compromised. EBV serum PCR studies are also frequently used to monitor for posttransplantation lymphoproliferative disease as trending high viral loads serve as a marker for impending posttransplantation lymphoproliferative disease.79 PCR testing on tissue also may be used to identify EBV-induced neoplasms. The histopathology of the morbilliform exanthem associated with EBV is nonspecific with a mild perivascular infiltrate of inflammatory cells. Specific cutaneous manifestations of EBV may show their own characteristic histopathologic features.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Recovery from infectious mononucleosis is typically over 2 to 3 weeks without specific treatment.65 Disease may be more protracted in older adults. Chronic active EBV infection occurs rarely. It begins as a primary
3001
25
Most Likely
■Cytomegalovirus mononucleosis
■Group A streptococcal infection
■Toxoplasmosis
Consider
■Adenovirus
■Enterovirus
■Measles
■Rubella
■Viral hepatitis
Always Rule Out
Always Rule Out
■Drug rash with eosinophilia and systemic symptoms syndrome
■Drug rash with eosinophilia and systemic symptoms syndrome
■Primary exanthem of HIV
■Primary exanthem of HIV
EBV infection and persists for more than 6 months with severe illness and histologic evidence for organ disease. EBV DNA or antigens can be demonstrated from tissue, and usually EBV antibody titers are significantly elevated.
MANAGEMENT
MANAGEMENT
Treatment for uncomplicated infectious mononucleosis is symptomatic Table 163-8). Acetaminophen or nonsteroidal antiinflammatory agents may be useful in treating the fever or throat discomfort. Because splenomegaly is often an associated finding, contact sports should be avoided until the spleen has returned to its normal size to avoid splenic rupture. Systemic corticosteroids have been used to reduce the duration of fever or pharyngeal symptoms in infectious mononucleosis. However, a large metaanalysis failed to show any clinical benefit and therefore systemic steroids should not be used to treat typical cases of infectious mononucleosis.80 Acyclovir has some activity against EBV through the inhibition of the EBV DNA polymerase. A reduction of viral shedding has
First-line therapy Fever, throat discomfort, myalgia, headache Acetaminophen/ nonsteroidal antiinflammatory drugs
Splenomegaly Avoid contact sports until spleen size normalizes to prevent splenic rupture
Second-line
Impending airway
Systemic corticosteroids
Second-line therapy Impending airway obstruction, thrombocytopenia, hemolytic anemia
Systemic corticosteroids
therapy
obstruction, thrombocytopenia, hemolytic anemia
3002
been documented with acyclovir treatment, but clinical benefit has not; as a result, acyclovir is not routinely used in the management of EBV infection.81
A commercial vaccine against EBV is not currently available, but investigations are underway with the goal of reducing EBV infection burden, particularly in high-risk patients.82
GIANOTTI-CROSTI SYNDROME
AT-A-GLANCE
■ Papular acrodermatitis of childhood.
■ Common, self-limited dermatosis.
■ Monomorphic dome-shaped or flat-topped papules symmetrically distributed on face and extensor extremities.
■ Associated with multiple viral triggers and immunizations.
■ Historically associated with hepatitis B infection, but now more often triggered by Epstein-Barr virus.
Gianotti-Crosti syndrome (GCS), also known as infantile papular acrodermatitis and papular acrodermatitis of childhood, is a common, self-limited exanthem. GCS typically affects children between the ages of 3 months and 15 years, with the peak age of onset being 1 to 6 years.83 Adult cases are uncommon and almost exclusively occur in women. GCS was first described in 1953 by one of Italy’s first pediatric dermatologists, Fernandino Gianotti, and his chairman, Professor Agostino Crosti, in Milan.84 Since this time, GCS is widely known to dermatologists and pediatricians alike as a distinct childhood exanthem with varying infectious triggers.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
GCS is believed to be an immune reaction to a preceding virus, bacterium, or vaccine, and not related to direct infection of the skin. In cases of EBV-associated GCS, EBV antigen was unable to be isolated from involved skin.85 The likelihood of developing GCS is likely dependent upon how a host immunologically responds to a preceding infection. Both young age and a history of atopic dermatitis are host risk factors associated with GCS.86
Viral infections are the most common trigger of GCS. An association between GCS and hepatitis B was first published in the 1970s, and, for some time thereafter, hepatitis B was thought to be the exclusive
A B
25
cause of GCS. More recent studies implicate numerous other infections agents. In most developed countries, EBV is frequently cited as the most common cause of GCS.87 Other important viral causes include molluscum pox virus, CMV, echovirus, poxvirus, poliovirus, coxsackievirus (A6, A16, B4, and B5), parvovirus B19, HIV, hepatitis A, hepatitis C, mumps virus, human herpesvirus-6, vaccinia virus, rubella virus and parainfluenza virus.83 Often overlooked, GCS complicates approximately 5% of cases of molluscum contagiosum, and therefore a recent history or concurrent molluscum should be explored in children with GCS.88
Bacterial pathogens include M. pneumoniae, Borrelia burgdorferi, Bartonella henselae, and group A β-hemolytic Streptococcus.83 Lastly, a number of vaccines have been documented as preceding the onset of GCS, including influenza, diphtheria-pertussis-tetanus (DPT), bacillus Calmette-Guérin, Haemophilus influenzae type b, MMR, hepatitis B, Japanese encephalitis, and oral polio vaccine. Despite these varied infectious triggers, the clinical morphology of GCS remains consistent.
CLINICAL FEATURES
CLINICAL FEATURES
GCS presents with an abrupt onset of symmetrically distributed, monomorphous papules or papulovesicles on the face, extensor surface of extremities, and buttocks (Fig 163-9). Papules range between 1 and 5 mm in size, are pink to red-brown in color, often are dome shaped or flat-topped, and can coalesce to form large plaques. Infrequently, lesions may be hemorrhagic or have scale. Involvement of the trunk, palms, soles, or mucosal surfaces makes a diagnosis of GCS unlikely. Pruritus is the most common accompanying symptom. Patients with GCS are typically well appearing. GCS can be preceded by malaise, pharyngitis, low-grade fever, and lymphadenopathy (typically cervical, axillary, or inguinal). Noncutaneous findings may also reflect the underlying infectious process triggering GCS, such as hepatomegaly and lymphadenopathy in
the setting of hepatitis B infection or splenomegaly in the setting of EBV.
DIAGNOSIS
DIAGNOSIS
GCS is a clinical diagnosis. Usually, no further workup is needed. A skin biopsy is rarely needed owing to the characteristic features of GCS. In the setting of hepatomegaly, splenomegaly, or hepatitis, a laboratory workup for viral hepatitis (hepatitides A, B, and C, EBV, and CMV) should be performed.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Most Likely
■Id reaction
■Papular urticaria
Consider
■Erythema infectiosum
■Erythema multiforme
■Follicular eczema
■Hand-foot-mouth disease
■Lichen planus
■Lichenoid drug eruption
■Molluscum contagiosum
■Pityriasis lichenoides et varioliformis acuta
■Pityriasis rosea
Always Rule Out
Always Rule Out
■Henoch-Schönlein purpura
■Henoch-Schönlein purpura
■Infectious mononucleosis
■Infectious mononucleosis
3003
■Scabies
■Scabies
25
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE
AND PROGNOSIS
GCS is self-limited; however, families should be counseled that it might last longer than most rashes associated with viruses. GCS gradually fades over 10 to 60 days. GCS resolves without scarring but can resolve with temporary, postinflammatory hyperpigmentation or hypopigmentation. Reactive lymphadenopathy associated with GCS may take months to fully resolve.
MANAGEMENT
MANAGEMENT
No treatment is necessary in the majority of cases. In some patients, medium-potency topical steroids may decrease the duration of lesions when applied once daily for 1 to 2 weeks. However, patients should be monitored closely because worsening of findings with topical steroid use has been documented.89 Oral antihistamines or topical antiitch lotions may diminish severe pruritus.
HUMAN CYTOMEGALOVIRUS
AT-A-GLANCE
■ Cytomegalovirus is also known as human herpesvirus 5.
■ High prevalence in the population.
■ Establishes latent infection and is capable of reactivation in immunosuppressed states.
■ Primary infection is mainly asymptomatic; it is the cause of severe morbidity and mortality in utero and in immunocompromised patients.
■ Petechiae and blueberry muffin syndrome occur with congenital infection.
■ Congenital infection is major cause of hearing loss.
■ Infected cells are cytomegalic with intranuclear inclusions.
EPIDEMIOLOGY
EPIDEMIOLOGY
Human cytomegalovirus (HCMV) is ubiquitous around the world. The seroprevalence in the population increases with age, with 10% to 20% of children infected before they reach puberty. By adulthood, the prevalence of HCMV is 40% to 100%. For unclear reasons, there is a higher prevalence in developing countries and areas of low socioeconomic status. HCMV is the most common congenital viral infection in
3004
humans, with an incidence of 0.5% to 2% of live births in the United States.90 Ten percent to 15% of congenital infections exhibit sequelae.90 Nearly all HIV-infected patients are infected with HCMV.91 It is a significant cause of morbidity in bone marrow transplant and solid-organ transplant patients.
CLINICAL FEATURES
CLINICAL FEATURES
CONGENITAL HUMAN CYTOMEGALOVIRUS INFECTION History: Congenital HCMV (cytomegalic inclusion disease of the newborn) occurs mostly in children of primiparous women with primary infection during pregnancy. Fifty-five percent of maternal primary HCMV infections result in intrauterine HCMV infection of the fetus, and approximately one-third of those are symptomatic. Reactivation or secondary HCMV infection of a HCMV-immune woman during pregnancy rarely results in symptomatic HCMV infection for the baby.90
Cutaneous Lesions: Cutaneous findings in the newborn include a petechial rash secondary to thrombocytopenia, jaundice caused by hepatitis and blueberry muffin lesions from dermal erythropoiesis. In one study, approximately 70% of children with symptomatic congenital HCMV infections had petechiae and jaundice.92 Dermal erythropoiesis, also known as thrombocytopenic purpura or blueberry muffin syndrome, also can be seen with congenital rubella, toxoplasmosis, and blood dyscrasias. These purpuric lesions are present at birth and evolve during the first 24 to 48 hours of life. They are papular and range from 2 to 10 mm in diameter. Lesions are initially dark-blue to violaceous and fade to red or copper-brown. They regress during the first 6 weeks of life despite continued presence of the virus. Histology shows plaquelike aggregates of nucleated cells and nonnucleated erythrocytes in the reticular dermis.93
Related Physical Findings: Related findings include hepatosplenomegaly in virtually all newborns, microcephaly, periventricular calcifications, ventriculomegaly, encephalitis, chorioretinitis, hearing loss or neurodevelopmental sequelae, intrauterine growth retardation, and postnatal failure to thrive. After congenital HCMV infection, approximately 50% of symptomatic and 10% of asymptomatic children have hearing loss.90,94
PERINATAL HUMAN CYTOMEGALOVIRUS INFECTIONS History: Perinatal infection with HCMV is very different from congenital HCMV infection, and is without diffuse visceral or CNS involvement. Transmission of the virus occurs via cervical secretions, breastmilk, or
blood transfusions between 4 and 16 weeks of age. It is usually asymptomatic, although it may be manifested by self-limited lymphadenopathy, hepatosplenomegaly, or afebrile pneumonitis.90
Cutaneous Lesions: There are usually no cutaneous findings with perinatal HCMV infection. Uncommon presentations for HCMV infection in infants and children include GCS, gray pallor, hepatosplenomegaly with self-limited respiratory deterioration in preterm infants, and cutaneous vasculitis.95,96
Perineal ulcers have been reported in an immunocompetent preterm infant.97
HUMAN CYTOMEGALOVIRUS INFECTION IN IMMUNOCOMPETENT ADULTS AND CHILDREN History: Although primary HCMV infection in the immunocompetent patient is usually asymptomatic, some can present with an infectious mononucleosis– like picture. Approximately 10% of infectious mononucleosis cases are caused by HCMV. Symptoms and signs are indistinguishable from EBV-induced mononucleosis, including fever, malaise, splenomegaly, hepatitis, and peripheral and atypical lymphocytosis. Unlike EBV mononucleosis, HCMV-induced mononucleosis patients do not typically have pharyngitis and lymphadenopathy.98 Given the lack of heterophile antibodies, HCMV mononucleosis is also known as heterophile-negative mononucleosis. HCMV mononucleosis can occur between 3 and 6 weeks after exposure to CMV-positive blood products.98
Reactivation of various herpesviruses, including HCMV, EBV, human herpesvirus (HHV)-6, and HHV-7, has been reported in the setting of druginduced hypersensitivity syndrome (see Chap. 45) and other severe cutaneous adverse drug reactions, which, in some cases, might lead to multiorgan failure after the causative drug is discontinued.99
Cutaneous Lesions: A few patients with HCMV mononucleosis develop a rubelliform or morbilliform eruption; if given ampicillin, 80% to 100% of patients develop a morbilliform rash within 1 week.100 There are reports of erythema nodosum and urticaria associated with acute HCMV mononucleosis.101 Cutaneous ulcers caused by CMV have been reported in patients with severe cases of drug-induced hypersensitivity syndrome.102
HUMAN CYTOMEGALOVIRUS AND THE IMMUNOCOMPROMISED History: Immunocompromised patients are at risk for both HCMV primary infection and reactivation, resulting in persistent viremia and disseminated systemic disease. Immunosuppressive agents, such as azathioprine and cyclophosphamide alone, can reactivate HCMV disease, as can systemic corticosteroids
25
in conjunction with other immunosuppressive agents. CMV infection in this setting is defined as evidence of CMV replication with or without disease symptoms. CMV disease is defined as CMV infection with these symptoms: viral syndrome with fever, malaise, leukopenia, and thrombocytopenia; or tissue invasive disease with variable pneumonitis, enteritis, hepatitis, retinitis, and CNS disease.103
Solid-Organ Transplantation Recipients: Solid-organ transplantation recipients who are not infected with HCMV but who receive an organ from an HCMV-positive individual are at highest risk of developing HCMV disease posttransplantation. Additional risk factors include higher levels of immunosuppression and allograft rejection.
Bone Marrow Transplantation Patients: The risk of HCMV disease in bone marrow transplantation patients is lower with the use of seronegative donors and of leukocyte-depleted blood products.104
Risk factors for both first and subsequent CMV infection in seropositive patients include myeloablative conditioning, graft-versus-host disease, lymphoma/ myeloma, and low CD3 graft content.105
HIV-Infected Patients: HCMV retinitis was seen in up to 25% of HIV-infected patients before the use of highly active antiretroviral therapy.106 Other clinical manifestations of HCMV infection include immune recovery vitreitis, encephalopathy, peripheral polyradiculopathy, pneumonitis, and colitis.107
Asymptomatic CMV coinfection in HIV-infected patients on highly active antiretroviral therapy may impair CD4:CD8 ratio normalization.108
Cutaneous Lesions: Cutaneous manifestations of HCMV disease in immunocompromised patients are rare compared with involvement of other organs. Perianal and rectal ulceration are most common.109
Also seen are indurated hyperpigmented nodules or plaques, papular and purpuric eruptions, vesiculobullous lesions, purpura, petechiae, indurated plaques, and, occasionally, verrucous and necrotic nodules.110-112
Some of these cutaneous manifestations may be caused by infection of the endothelium of cutaneous blood vessels.109
DIAGNOSIS
DIAGNOSIS
The gold standard for diagnosis of HCMV infection is viral culture from blood using human fibroblasts. Because it takes days to several weeks to see the cytopathic effect in culture, culture has been supplanted by PCR for the diagnosis of active HCMV infection.103,113 The diagnosis of congenital HCMV infection can be made by detection of virus in urine or saliva via PCR.113 HCMV PCR also can be used to identify primary infection in children younger than 12 months of age as they shed the virus for long periods of time.
3005
25
HCMV serology (IgG) is the most reliable method to determine past infection and is used as part of pretransplantation screening. In immunocompetent individuals, IgM is usually positive during primary infection, although the reported sensitivity of IgM varies. Rheumatoid factor and EBV IgM may yield false-positive results.114 IgG may be negative during active infection, but a subsequent fourfold rise in IgG titer is indicative of infection. In immunocompromised patients, quantitative nucleic acid amplification testing for CMV is the most widely used test for diagnosis, and monitoring response to treatment.103
The characteristic histologic feature of CMV infection is cytomegalic cells with nuclear inclusions. In the skin, enlarged endothelial cells with large intranuclear inclusions and a clear halo (owl’s eye cells) are seen in small dermal vessels.115 Cytopathic changes seen in the vascular lumen vary according to the stage of infection of each cell, including intranuclear and intracytoplasmic inclusions (Fig. 163-10). Histologic diagnosis is specific but sensitivity is low. The diagnosis of invasive CMV disease can be challenging because the presence of the virus does not mean causality given that the virus establishes latency after primary infection.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
PROGNOSIS AND CLINICAL COURSE
PROGNOSIS AND
CLINICAL COURSE
HCMV disease in immunocompetent individuals is usually self-limited. Immunocompromised patients with systemic HCMV disease have a poor prognosis
3006
Most Likely
■Causes of dermal (extramedullary) hematopoiesis
■Congenital infection
■Enterovirus
■Herpes simplex virus infection
■Rubella
■Toxoplasmosis
■Hereditary spherocytosis
■Rhesus and ABO incompatibility
■Twin–twin transfusion syndrome
Consider
■Langerhans cell histiocytosis
■Neonatal lupus erythematosus
Always Rule Out
Always Rule Out
■Congenital leukemia
■Congenital leukemia
■Neuroblastoma with skin metastases
■Neuroblastoma with skin metastases
and suffer direct effects of CMV disease in addition to indirect effects such as allograft rejection, higher risk of other infections, graft-versus-host disease, and secondary malignancies.103
COMPLICATIONS
COMPLICATIONS
Possible complications of postnatal HCMV infection include interstitial pneumonia, hemolytic anemia, splenic infarction, thrombocytopenia and hemolytic anemia, hepatitis, Guillain-Barré syndrome, meningoencephalitis, myocarditis, arthritis, and GI/genitourinary syndromes (colitis, esophagitis, cervicitis, and urethral syndromes).
MANAGEMENT
MANAGEMENT
HCMV infection in immunocompetent hosts is usually asymptomatic or self-limited, not requiring treatment with antiviral drugs. Ganciclovir, valacyclovir, foscarnet, and cidofovir have been approved for systemic
Most Likely
■Epstein-Barr virus mononucleosis
Consider
■Toxoplasmosis
■Viral hepatitis
Always Rule Out
Always Rule Out
■Lymphoma
■Lymphoma
treatment of HCMV disease. Ganciclovir and valacyclovir are also used for HCMV prophylaxis.103 Oral valganciclovir for 6 months improves hearing and neurodevelopmental outcomes in patients with symptomatic congenital HCMV infection.116
PREVENTION
PREVENTION
Prevention of HCMV infection in HCMV-negative transplanted patients can be achieved with use of blood and tissues from HCMV-negative donors. Preemptive (at time of high risk for disease but before symptoms) or prophylactic treatment with ganciclovir, valganciclovir, or valacyclovir can be used for immunocompromised individuals who are at risk of infection from blood transfusions or organ transplantation with ganciclovir. Risk stratification for preemptive versus prophylactic treatment depends on various risk factors, including type of transplant, immunosuppression, and other host factors.103 There are currently no candidate vaccines that are near licensure.116
HUMAN HERPESVIRUS 6
AT-A-GLANCE
■ Causes exanthem subitum (roseola infantum, sixth disease).
■ Febrile seizures often without rash in children.
■ High seroprevalence in general population by 1 year of age.
■ Reactivation in immunocompromised individuals is a cause of morbidity.
Consistent with other herpesviruses, HHV-6 infection is chronic, existing in a latent stage with the ability to reactivate. HHV-6 primary infection often presents either as an acute febrile illness or as the distinct illness exanthem subitum (ES), also known as roseola infantum and sixth disease.
EPIDEMIOLOGY
EPIDEMIOLOGY
HHV-6 is a common viral infection with up to 80% of the population acquiring the infection by 2 year of age.117 Primary infection typically occurs between the ages of 6 months and 2 years when maternal passive immunity wanes.117 Primary infection exhibits seasonal variation with the highest incidence in spring; summer and fall epidemics also have been reported.
25
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
HHV-6 is a member of the β-Herpesviridae subfamily and exists as 2 distinct species: HHV-6a and HHV-6b. HHV-6b causes ES and reactivates in immunocompromised hosts. It is unclear what diseases, if any, are caused by HHV-6a.118
HHV-6 infects a wide range of human cells, including monocytes/macrophages, natural killer cells, and neuronal cells, such as astrocytes, and preferentially infects activated CD4+ T lymphocytes. The immune regulatory protein CD46 is the cellular receptor for HHV-6 infection.119 HHV-6 viral DNA may also integrate into host cell chromosomes in up to 1% of the general population, thereby serving as an alternative means of HHV-6 persistence.120
As the salivary glands are an important site of viral replication, HHV-6 transmission occurs via shared saliva and can readily be detected in the saliva of adults and children.117 In transplantation recipients, most cases of HHV-6 infection constitute reactivation of latent infection; however, transmission of HHV-6 from the donor organ has been infrequently described.121
The incubation period for HHV-6 infection is 5 to 15 days, with an average of 10 days. Viremia in immunocompetent children lasts 3 to 4 days in ES, whereas viremia from HHV-6 reactivation in allogeneic bone marrow transplantation patients lasts weeks.120
CLINICAL FEATURES
CLINICAL FEATURES
HHV-6 primary infection in early childhood may be subclinical or can present with nonspecific symptoms, including high fever, irritability, rhinorrhea, and diarrhea. The fever lasts approximately 3 to 7 days and is followed by the characteristic rash of roseola in only 23% of cases.122,123
HHV-6 infection can also occur when the virus reactivates in the setting of immunosuppression. HHV-6 reactivation is particularly common in stem cell transplantation patients where reactivation occurs in 50% of patients and peaks 2 to 4 weeks posttransplantation.124 HHV-6 reactivation is thought to occur less frequently in solid-organ transplantation patients. Reactivation may be asymptomatic or result in fever, diarrhea, morbilliform rash, and transient myelosuppression.
EXANTHEM SUBITUM
HHV-6 is the cause of ES, also known as roseola, which was first described in 1910.125 The hallmark of ES is the development of “rose”-colored macules and papules measuring 2 to 5 mm and surrounded by a white halo (Fig. 163-11). The exanthem lasts 3 to 5 days and is widespread spread on the neck and trunk, and occasionally occurs on the face and proximal extremities. A unique feature of ES is that
3007
25
A
B
it presents 1 day before to 1 to 2 days after the fever resolves, as opposed to most viral exanthems where eruptions occur at the onset of the illness. Children with ES may also have palpebral edema resulting in a “sleepy” appearance and erythematous papules on the soft palate (Nagayama spots) that may precede the viral exanthem.
PITYRIASIS ROSEA
See Chap. 31 and “Human Herpesvirus 7” below.
ROSAI-DORFMAN DISEASE
The HHV-6 genome has been detected in tissue from patients with sinus histiocytosis with massive lymphadenopathy or Rosai-Dorfman disease (see Chap. 117), and immunohistochemical studies suggest a possible pathogenic involvement.126,127
DRUG-INDUCED HYPERSENSITIVITY SYNDROME
Although HHV-6 reactivation is well-described in drug hypersensitivity reactions (see Chap. 45), its role in driving systemic inflammation in this setting is unclear.
DIAGNOSIS
HHV-6 primary infection in childhood and in the setting of ES is typically a clinical diagnosis and laboratory testing is rarely needed. A challenge in the laboratory
3008
testing of HHV-6 is distinguishing between latent versus active replicating infection. Most patients older than 2 years of age are seropositive for HHV-6 and approximately 5% of healthy adults are IgM-positive at any given time.128 A fourfold increase of HHV-6 IgG during the convalescent stage is suggestive of HHV-6 infection. Quantitative real-time PCR is increasingly being used to detect HHV-6 infection with intermediate and high levels of HHV-6 DNA suggestive of active, as opposed to latent, infection. Real-time PCR testing also can be performed on any tissue. Qualitative real-time PCR does not distinguish latent from active infection. Because of the low sensitivity and longer turnaround time, viral culture is rarely employed.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
HHV-6 primary infection and ES in childhood is generally benign and self-limited. Fever typically resolves in 1 week and the rash over 3 to 5 days. The most common complication of a primary infection is the development of a febrile seizure. Febrile seizures occur in 8% of children with primary infection.102
Rare complications of primary infection also include hepatitis, mononucleosis-like syndrome, meningoencephalitis, hemophagocytic syndrome, pneumonitis, and thrombocytopenia.122 Treatment is not typically needed for the immunocompetent patient. Although HHV-6 in transplantation recipients is linked to various complications, establishing
pathogenicity is challenging given that these hosts are frequently coinfected by other viral infections and the limitations of PCR technology to distinguish between latent and active infection. In bone marrow transplantation recipients, complications include subacute encephalitis, bone marrow suppression, pneumonitis, and thrombotic microangiopathy. The role of HHV-6 in triggering or increasing the severity of acute graft-versus-host disease is controversial.129
MANAGEMENT
MANAGEMENT
There are no controlled clinical trials, and no compounds have been formally approved for treatment of HHV-6 infection. The same drugs used for HCMV treatment and prophylaxis have been used for HHV-6. The activities of various antiviral compounds against HHV-6 have been tested in vitro.130
Several case reports support the clinical effectiveness of ganciclovir in HHV-6 treatment and prophylaxis.131 Foscarnet and cidofovir might also prove to be useful.131
PREVENTION
PREVENTION
Prophylaxis with ganciclovir may prevent HHV-6 reactivation in bone marrow transplantation and stem cell transplantation recipients, but low-dose prophylaxis may facilitate the development of resistance.132
Preemptive therapy (treatment after systemic detection of virus but before clinical symptoms of disease) has been proposed instead.
HUMAN HERPESVIRUS 7
AT-A-GLANCE
■ Human herpesvirus 7 causes a small subset of cases of exanthem subitum.
■ Primary infection typically occurs later in life than human herpesvirus 6 infection.
EPIDEMIOLOGY
EPIDEMIOLOGY
In seroconversion studies, 10% of ES cases are caused by HHV-7.133 Primary infection occurs during childhood, but later than, and at a slower rate than, infection with HHV-6. Both viruses are ubiquitous in adulthood and have a worldwide distribution. HHV-7 can be isolated from saliva samples of healthy seropositive adults.134
25
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
HHV-7 is a member of the β-Herpesviridae family. Even though it has significant homology to HHV-6, it is serologically and biologically distinct. HHV-7 establishes persistent infection in salivary glands, and transmission is likely through saliva.134 Latent virus can be activated in vitro from peripheral blood mononuclear cells, and its DNA can be found in CD4+ T cells. Similar to many other herpesviruses, HHV-7 can downregulate expression of CD4 and major histocompatibility complex class I, which may play a role in establishment of latency or pathogenesis.134,135 Reactivation of HHV-7 occurs more often than reactivation of HHV-6.136
CLINICAL FEATURES
CLINICAL FEATURES
EXANTHEM SUBITUM
HHV-7 causes a small subset of ES cases. When HHV-7 is associated, ES tends to occur later in life than when HHV-6 is associated.134 The rash associated with HHV-7 is lighter in color and occurs later in the course of the disease than HHV-6–associated ES.134
PITYRIASIS ROSEA
HHV-7 DNA has been isolated from skin biopsy specimens, peripheral blood mononuclear cells, and plasma of patients with pityriasis rosea (see Chap. 31) and not controls.137 However, these findings have not been confirmed by other studies. It is possible that the inflammatory milieu in pityriasis rosea activates HHV-7 and HHV-6 within the lesions, but there is no evidence for causality.
LICHEN PLANUS
HHV-7 DNA and virion-like structures have been found in lesional lichen planus skin samples compared to nonlesional skin and psoriatic skin samples.89 Although suggestive, further studies are needed to establish a causal relationship.
DIAGNOSIS
DIAGNOSIS
There is limited cross-reactivity between HHV-7 and HHV-6 in serologic studies. Because of high prevalence, a single positive IgG is not sufficient to establish a diagnosis. PCR is widely available and is useful for timely diagnosis. Diagnosis of active infection by PCR can only be made from acellular material such as CSF, serum, or plasma, because the virus is latent in peripheral blood mononuclear cells and tissue.
3009
25
Most Likely
■Drug hypersensitivity reaction
■Enterovirus (including coxsackie, echovirus)
■Human herpesvirus–associated exanthem subitum
Consider
■Adenovirus
■Epstein–-Barr virus
■Fifth disease (erythema infectiosum, parvovirus)
■Measles/rubeola
■Rubella (German measles)
Always Rule Out
Always Rule Out
■Kawasaki disease
■Kawasaki disease
■Scarlet fever
■Scarlet fever
Immunohistochemical studies for viral antigens in biopsy specimens can be performed.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
ES is a self-limiting disease that does not require specific antiviral treatment. Disease in immunocompromised patients can be more serious and require treatment. Complications of HHV-7–associated ES include acute hemiplegia and febrile seizures with CSF findings consistent with encephalitis and hepatitis.138
MANAGEMENT
MANAGEMENT
Treatment for HHV-7 has not been evaluated in clinical trials but can be guided by treatment recommendations for HHV-6.
ENTEROVIRUSES
Human enteroviruses cause a variety of exanthems and clinical syndromes. They are small, single-stranded RNA picornaviruses and include echovirus, coxsackieviruses A and B, and poliovirus.139 Most enterovirus infections are benign. However, nonpolio enteroviruses are also the most common cause of aseptic (viral) meningitis and, rarely, can cause life-threatening infections
3010
involving encephalitis, myocarditis, or sepsis.139 Severe infections are more common in neonates and immunocompromised individuals. Enteroviruses are one of the most common causes of nonspecific exanthems. Infected patients present with scattered, pink, small macules and papules that fade within 1 week. Exanthems may also include petechiae and purpuric macules and therefore may be confused with more life-threatening infections such as Rocky Mountain spotted fever or meningococcemia. Well-described exanthems caused by enteroviruses include hand-foot-mouth disease; coxsackievirus A6– associated atypical hand-foot-mouth disease; herpangina; eruptive pseudoangiomatosis; and the Boston exanthem.
HAND-FOOT-MOUTH DISEASE
HAND-FOOT-MOUTH
DISEASE
AT-A-GLANCE
■ Hand-foot-mouth disease is a viral exanthem seen mostly commonly in children in summer and fall.
■ Erosions in the mouth and papulovesicles on the palms and soles.
■ Caused by enteroviruses including coxsackievirus A16 and enterovirus 71.
■ Self-resolving without serious sequelae in the majority of cases, but may have serious complications when caused by enterovirus 71.
Hand-foot-mouth disease (HFMD) is the bestrecognized enteroviral exanthem with a worldwide distribution.
EPIDEMIOLOGY
Children younger than 10 years of age are most frequently affected, and infected adults rarely show signs of infection. In temperate climates, HFMD is most common in the summer and fall.
ETIOLOGY AND PATHOGENESIS
Traditionally, HFMD has been caused by coxsackievirus A16 and enterovirus 71. Other causes of often HFMD include coxsackieviruses A5, A6, A7, A9, A10, A16, B1, B2, B3, and B5, echoviruses, and other enteroviruses.140
Viral transmission is via the fecal–oral route and, less commonly, respiratory inhalation. Once inhaled or ingested, virus replication ensues in the oropharynx and/or GI tract with subsequent viremia. The incubation period of HFMD is believed to be short,
lasting 3 to 6 days, with viral shedding lasting up to 5 weeks.141
CLINICAL FEATURES
HFMD usually begins with a nonspecific prodrome involving low-grade fever (38°C to 39°C [100.4°F to 102.2°F]) that lasts 1 to 2 days, malaise, and, occasionally, abdominal pain or upper respiratory tract symptoms. Sore throat or a sore mouth is common and can lead to poor oral intake and dehydration. The hallmark of HFMD is the development of a vesicular eruption on the palms and soles. The lesions start as bright pink macules and papules that progress to small 4- to 8-mm vesicles with surrounding erythema. Vesicles quickly erode and form yellow to gray, oval or “football-shaped” erosions surrounded by an erythematous halo. Cutaneous vesicles are found on the palms, soles (Figs. 163-12B and 163-12C), sides of hands and feet, buttocks and, occasionally, external genitalia. In classic HFMD, nearly all patients also develop an enanthem consisting of similarly appearing oral erosions involving the tongue (Fig. 163-12A) buccal mucosa, hard palate, and, less frequently, the oropharynx.
DIAGNOSIS
HFMD is a clinical diagnosis and laboratory tests are typically not needed. If laboratory confirmation is required, viral culture or PCR based assays can be performed. The virus can be recovered from skin vesicles as well as throat and stool swabs. PCR is frequently performed on the CSF and serum when working up systemic viral infection.142
Skin biopsies are not typically performed. Nonspecific findings, such as intraepidermal blister formation from vacuolar and degeneration of keratinocytes, are seen as in other viral blisters.143
CLINICAL COURSE AND PROGNOSIS
The cutaneous vesicles in HFMD typically crust over and fade in in 7 to 10 days. Onychomadesis has occasionally been reported as a consequence of coxsackievirus A16 and enterovirus 71 infections. Patients with HFMD rarely experience complications. The most common serious complication associated with HFMD is aseptic meningitis. Aseptic meningitis is rarely life threatening, and patients typically do not develop permanent sequela. However, enterovirus 71, an important cause of HFMD outbreaks in Asia, is associated with severe illness. Epidemics of enterovirus 71 are associated with severe neurologic disease, including encephalitis, encephalomyelitis, and polio-like syndromes. Enterovirus 71 infection may also lead to myocarditis, pulmonary edema, pulmonary hemorrhage, and death.144
25
A
B
C
MANAGEMENT
Treatment is typically supportive with attempts to reduce discomfort and dehydration. Novel antiviral agents and vaccine development targeting enterovirus 71 is an active area of investigation because of the strain’s virulence, geographic spread, rising prevalence, and risk for devastating brainstem encephalitis.145
3011
25
COXSACKIEVIRUS A6– ASSOCIATED ATYPICAL HAND-FOOT-MOUTH DISEASE
COXSACKIEVIRUS A6–
ASSOCIATED ATYPICAL
HAND-FOOT-MOUTH
DISEASE
AT-A-GLANCE
■ Papulovesicles, vesicles and erosions on the palms, soles, extremities and perioral area.
■ Oral erosions occur less frequently than in classic hand-foot-mouth disease.
■ Large bullae and purpuric macules may occur.
■ Self-resolving without serious sequela in the majority of cases.
An emerging cause of HFMD disease in many countries around the world is coxsackievirus A6 (CVA6).146
Within the United States, CVA6 was first isolated as the cause of clinically atypical HFMD disease in 2011, and is now commonly identified in HFMD outbreaks.147
Compared to classic HFMD, CVA6 infection frequently results in a cutaneous presentation that is more varied and extensive in distribution. Presumably because of a lack of previous immunity, adults may also present with CVA6-associated HFMD.148
ETIOLOGY AND PATHOGENESIS
Similar to other enteroviruses, CVA6 is transmitted via a fecal–oral route and less often via respiratory secretions.
CLINICAL FEATURES
In keeping with classic HFMD, CVA6-associated HFMD frequently presents with erythematous macules and vesicles on the palmoplantar surfaces and buttocks. However, the exanthem is not limited to those sites. Papulovesicles, rounded vesicles, and erosions commonly involve the upper and lower extremities and the perioral area, occasionally leading to a misdiagnosis of bullous impetigo (Fig. 163-13). Diffuse involvement with the exanthem extending onto the trunk may also occur.149 In a review of 81 patients with CVA6 disease, the exanthem involved greater than 10% body surface area in 61% of patients.147
CVA6 infection can result in the development of large bullae measuring greater than 2 cm, typically in children younger than 1 year of age (Fig. 163-14) and acrally distributed petechiae and purpura, often in children older than 5 years of age, which may be confused for leukocytoclastic vasculitis.147 Localization of vesicles and erosions of atopic dermatitis is also well described and has been termed eczema coxsackium, highlighting that this presentation may mimic eczema
3012
herpeticum (Fig. 163-15). Clinical features more suggestive of eczema coxsackium include concurrent oral aphthae, palmoplantar macules and vesicles, perioral involvement, the lack of herpetiform grouping of vesicles, and the onset occurring the context of family or community outbreak. The CVA6 exanthem generally resolves in 1 to 2 weeks. Oral ulcerations, a defining feature in classic HFMD, found in nearly 100% of patients, are seen less frequently in CVA6 infection and are documented in CVA6-associated HFMD in only 50% of cases.147 Viral prodrome symptoms associated with CVA6 infection include fever, sore throat, headache, cough, and diarrhea.
DIAGNOSIS
In complicated cases, CVA6 infection can be confirmed by performing enterovirus reverse-transcriptase PCR on samples collected by swabs from stool, throat, the base of skin vesicles, or serum samples.150 PCR is more sensitive in the detection of CVA6 than enterovirus culture. Skin biopsies of this exanthem have revealed intraepidermal vesiculation with a predilection for the stratum granulosum and upper stratum spinulosum and a neutrophil rich infiltrate.151
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
Despite the occasionally extensive cutaneous presentation, CVA6 is not generally associated with severe systemic illness. Therefore, CVA6 infections appear to be more in keeping with CVA16 than enterovirus
Most Likely
■Eczema herpeticum
Consider
■Autoimmune blistering disorder (eg, liner immunoglobulin A bullous dermatosis)
■Disseminated herpes zoster
■Drug eruption
■Stevens-Johnson syndrome
■Erythema multiforme
■Leukocytoclastic vasculitis
■Varicella
Always Rule Out
Always Rule Out
■Herpes simplex virus infection
■Herpes simplex virus infection
25
- The 2 most common complications of CVA6 are desquamation of the hands and feet, which often occurs weeks after the exanthem resolves, and onychomadesis, which occurs 1 to 2 months later. Onychomadesis may occur in the absence of any history of the HFMD exanthema, and all patients with CVA6-associated HFMD should be made aware of this complication.152 Patients with onychomadesis can be expected to have normal nail growth after the shedding is complete.
MANAGEMENT
The management of CVA6 HFMD is supportive and focuses on managing pain, and local wound care for larger vesicles and bullae.
ERUPTIVE PSEUDOANGIOMATOSIS
Cherry and colleagues first described a syndrome in 1969 in which 4 children with acute echovirus infection (2 with echovirus 25 and 2 with echovirus 32) developed small, 2- to 4-mm, red papules that resembled angiomas on the face and extremities.153 The papules blanched on pressure and were surrounded by a small, 1- to 2-mm, halo. The eruption was short lived and typically resolved within 10 days.154 Patients often had associated fever, malaise, headache, diarrhea, and respiratory complaints. While echovirus was first linked to eruptive pseudoangiomatosis, the etiology in most cases cannot be identified. Adenovirus, CMV, arthropod bites, and immunocompromised states also have been identified in eruptive pseudoangiomatosis cases. Other children and adults have been described with similar outbreaks. Although a virus is likely to cause eruptive pseudoangiomatosis, echoviruses have not been consistently confirmed as the causative agent.155-158
UNILATERAL LATEROTHORACIC EXANTHEM
AT-A-GLANCE
■ Unilateral laterothoracic exanthem is also called asymmetric periflexural exanthem of childhood.
■ Typically affects children 1 to 5 years of age.
■ Pink papules that start in a large flexural region, become bilateral, but remain asymmetric.
3013
■ Probably viral etiology.
25
Unilateral laterothoracic exanthem (ULE), also known as asymmetric periflexural exanthem of childhood, has a seasonal variation and occurs most frequently in late winter and early spring. It typically occurs in children between 1 and 5 years of age, but may be seen from 8 months to 10 years of age.159
Rare cases in adults have been reported.160 There is a slight female predominance, and it is more common in whites.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The etiology of ULE is unknown, but because of its seasonality, associated viral symptoms and lack of response to antibiotics, a viral trigger is suspected. The pathogenesis is also unknown.
CLINICAL FEATURES
CLINICAL FEATURES
ULE typically presents with 1- to 2-mm, pinpoint, pruritic, pink papules with a surrounding pale halo localized to a large flexural region like the axillae or groin. The papules then spread centrifugally (Fig. 163-16). ULE can become bilateral and more widespread within 5 to 15 days, but a unilateral and asymmetric distribution remains. A variety of morphologies also have been described, including macules, papules, morbilliform, annular, scarlatiniform, and annular.159 Pruritus may be severe. In cases of ULE, a preceding viral syndrome consisting of mild upper respiratory tract, low-grade fever, or GI tract symptoms can often be elicited. In the area of the eruption, enlargement of regional lymph nodes are frequently identified.
3014
DIAGNOSIS
DIAGNOSIS
ULE is a clinical diagnosis and no laboratory tests are indicated.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
The rash typically lasts from 2 to 6 weeks but may last as long as 2 months. Resolution is spontaneous and without scarring. During the healing stage, desquamation and postinflammatory pigment change also may be present as the exanthem resolves.
Most Likely
■Allergic or irritant contact dermatitis
■Scarlet fever
Consider
■Other viral exanthems
Always Rule Out
Always Rule Out
■Atopic dermatitis
■Atopic dermatitis
■Herpes zoster
■Herpes zoster
25
ETIOLOGIC AGENT CHARACTERISTIC EXANTHEM OR ASSOCIATED RASH EXTRACUTANEOUS MANIFESTATIONS, ENANTHEMS
Measles (Rubeola) Paramyxoviridae Nonpruritic, erythematous macules and papules with craniocaudal spread Fever, malaise, conjunctivitis, coryza, cough, Koplik spots
Rubella (3-day measles; German measles) Togaviridae Pruritic pink to red macules and papules on the face, progressing to neck, trunk, and extremities
Low-grade fever, myalgia, headache, conjunctivitis, rhinitis, cough, sore throat, lymphadenopathy; Forchheimer spots
Erythema Infectiosum (fifth disease) Parvovirus (B19) Confluent, erythematous, edematous plaques on malar eminence (slapped cheek); lesions may recur for weeks or months
Papular purpuric gloves-and-socks syndrome
Erythema of the tongue, pharynx and red macules on the buccal mucosa and palate; acute arthropathy in adults
Itchy, painful, symmetric edema and erythema of the distal hands and feet with abrupt demarcation at the wrists and ankles
Epstein-Barr virus Epstein-Barr viruses 1 and 2 (human herpesvirus 4)
Fatigue, low-grade fever, myalgia and arthralgia; enanthem on the lips, soft palate and buccal mucosa
“Ampicillin rash” in individuals treated with antibiotics; Gianotti-Crosti syndrome; erythema multiforme, leukocytoclastic vasculitis, erythema nodosum, erythema annulare centrifugum, pityriasis lichenoides, granuloma annulare, cold urticaria
Gianotti-Crosti syndrome (popular acrodermatitis of childhood; infantile popular acrodermatitis)
Fever, lymphadenopathy and pharyngitis (Infectious mononucleosis); acute genital ulcers (Lipschütz ulcers) with associated inguinal lymphadenopathy; neoplastic conditions (see Table 163-6)
Various viral and bacterial pathogens Symmetrical monomorphic papules or papulovesicles on the face, extensors, and buttocks
Malaise, pharyngitis, low-grade fever, and lymphadenopathy
Human cytomegalovirusa Cytomegalovirus (human herpesvirus-5) Erythema nodosum, morbilliform eruption similar to ampicillin rash of Epstein-Barr virus infection; urticaria
Infectious mononucleosis–like symptoms
Exanthem subitum (roseola infantum, sixth disease) Human herpesvirus-6 Rose-colored macules and papules surrounded by a white halo over the neck and trunk High fever, irritability, rhinorrhea, and diarrhea; palpebral edema; Nagayama spots
Hand-foot-mouth disease Coxsackievirus A16 and Enterovirus 71 Vesicular eruption of the palms and soles, with “football-shaped” erosions surrounded by an erythematous halo
Low-grade fever, malaise, abdominal pain or upper respiratory tract symptoms, sore throat or sore mouth; oral erosions of the tongue, buccal mucosa, hard palate, and oropharynx
Atypical hand-foot-mouth disease Coxsackievirus A6 Papulovesicles, vesicles, and erosions of the palms, soles, extremities, and perioral; oral mucosa less frequently involved
Fever, sore throat, headache, cough, and diarrhea
Eruptive pseudoangiomatosis Echovirus 25, echovirus 32 Small papules resembling angiomas on the face and extremities Fever, malaise, headache, diarrhea, and respiratory complaints
Unilateral thoracic
Unknown, likely viral
Pinpoint pink papules with pale halo localized
Unilateral thoracic exanthema (symmetric periflexural exanthema of childhood)
Mild upper respiratory tract, low-grade
Unknown, likely viral trigger Pinpoint pink papules with pale halo localized to large flexural region; unilateral and asymmetric distribution; pruritus
exanthema (symmetric periflexural exanthema of childhood)
trigger
Mild upper respiratory tract, low-grade fever or GI symptoms
to large flexural region; unilateral and asymmetric distribution; pruritus
fever or GI symptoms
aCongenital infections, infections in neonates, and immunocompromised individuals are discussed in the text.
MANAGEMENT
MANAGEMENT
Treatment for ULE is typically focused on controlling pruritus. This can be done with topical corticosteroids, antiitch lotions, and oral antihistamines.
SUMMARY

Figure 163-1 Measles. The pathognomonic Koplik spots of measles appear as tiny white lesions—“grains of sand”— surrounded by an erythematous halo. They precede the generalized rash by 1 to 2 days. (Image used with permission from the Fitzsimmons Army Medical Center Dermatology Archive.)

Figure 163-2 The morbilliform eruption of measles in a toddler.
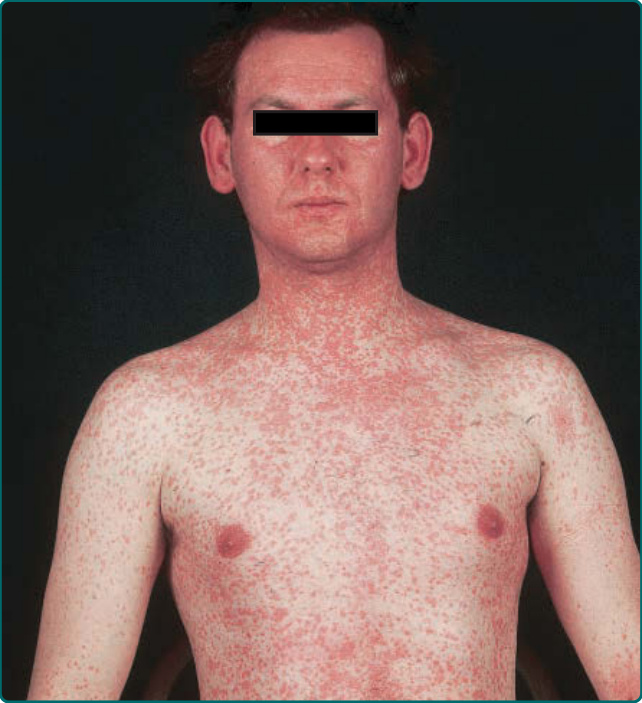
Figure 163-3 Measles. Classic morbilliform exanthem with red papules spreading from forehead and postauricular area to neck, trunk and then extremities. (Used with permission from Wolff K, Johnson R, Saavedra AP, et al. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology, 8th ed. New York, NY: McGraw-Hill; 2017.)

Figure 163-4 Rubella. Erythematous macules and papules appearing initially on the face and spreading to trunk, arms, legs within 24 hours.

Figure 163-5 Erythema infectiosum. Child with the characteristic “slapped cheeks.”

Figure 163-6 Reticulate and annular erythema of the torso and upper limbs in acute parvovirus B19 infection. (Image from Mage V, Lipsker D, Barbarot S, et al. Different patterns of skin manifestations associated with parvovirus B19 primary infection in adults. J Am Acad Dermatol. 2014;71(1):62-69, with permission. Copyright © American Academy of Dermatology.)

Figure 163-7 Morbilliform rash in Epstein-Barr virus infection. (From Rabach I, Berti I, Bibalo C, Longo G. A curious rash. J Pediatr. 2013;162(5):1071-1072, with permission.)

Figure 163-8 Two scrotal ulcers in a patient with documented Epstein-Barr virus infection.

Figure 163-9 A and B, Erythematous edematous monomorphous dome-shaped papules on the extensor extremities in a toddler with Gianotti-Crosti syndrome.
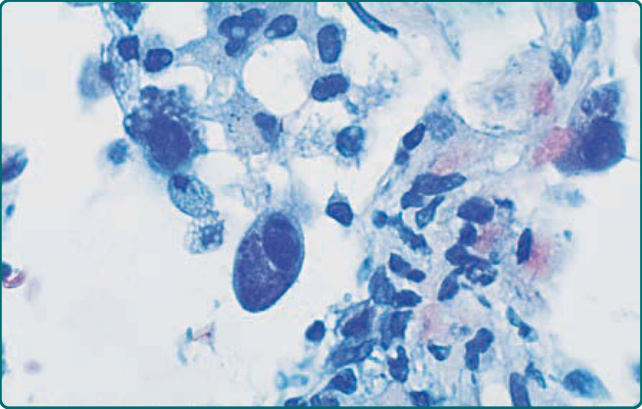
Figure 163-10 Intracellular inclusions in a cell infected by human cytomegalovirus. (From Konstadt JW, Gatusso P, Eng A, et al. Disseminated cytomegalovirus infection with cutaneous involvement in a heart transplant patient. Clin Cases Dermatol. 1990;2:3.)

Figure 163-11 A and B, Exanthem subitum in an infant showing truncal pink macules and some papules that appeared 1 day after defervescence.
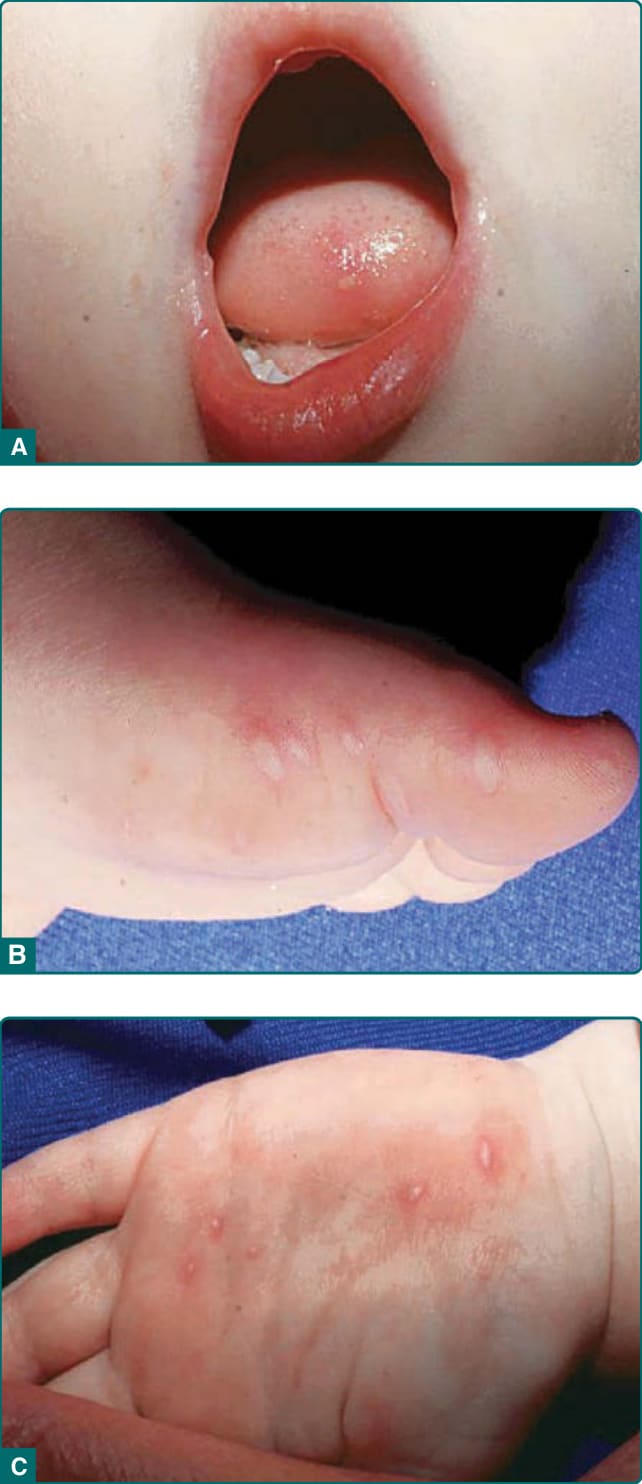
Figure 163-12 Classic hand-foot-mouth disease in a toddler. A, Vesicles and surrounding erythema on the tongue. B and C, Elliptical, “football-shaped” vesicles with halo of erythema on the palms and soles.

Figure 163-13 Coxsackievirus A6–associated hand-footmouth disease with perioral distribution.

Figure 163-14 Coxsackievirus A6–associated hand-footmouth disease with large bullae on the sole of an infant. (Image used with permission from Dr. Ilona Frieden.)

Figure 163-15 Eczema coxsackium. Localization of vesicles and erosions to affected areas of atopic dermatitis in a coxsackievirus A6–infected patient.

Figure 163-16 Rough pink papules in the right axilla, characteristic of unilateral laterothoracic exanthem. (Used with permission from Antonio Torrelo, MD.)
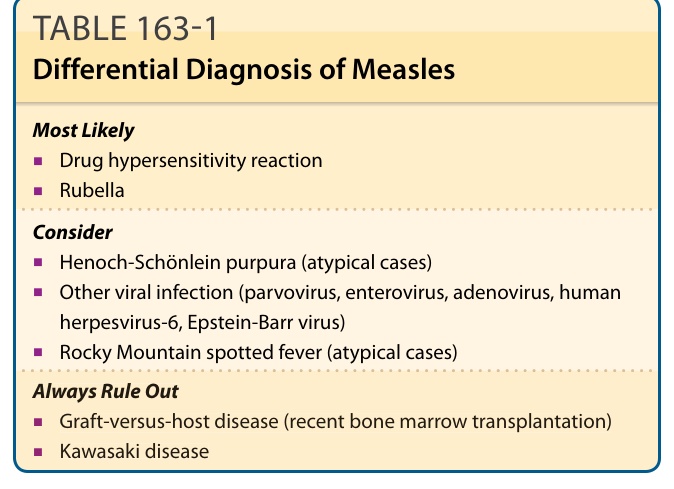
Table 163-1 outlines the differential diagnosis of measles.
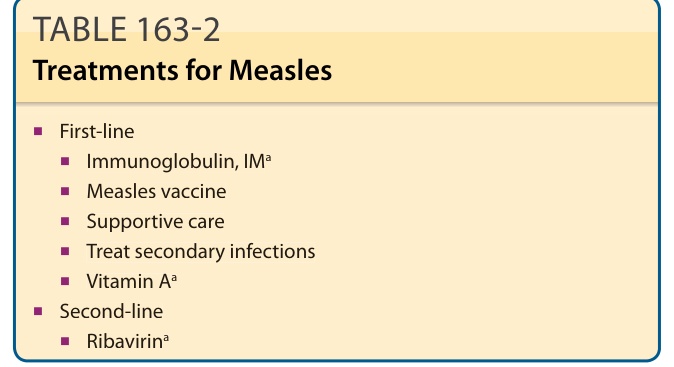
TABLE 163-2 Treatments for Measles
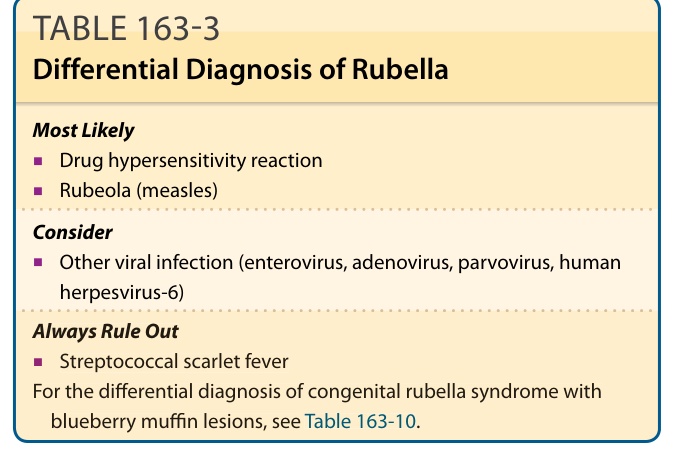
Table 163-3 outlines the differential diagnosis of rubella.
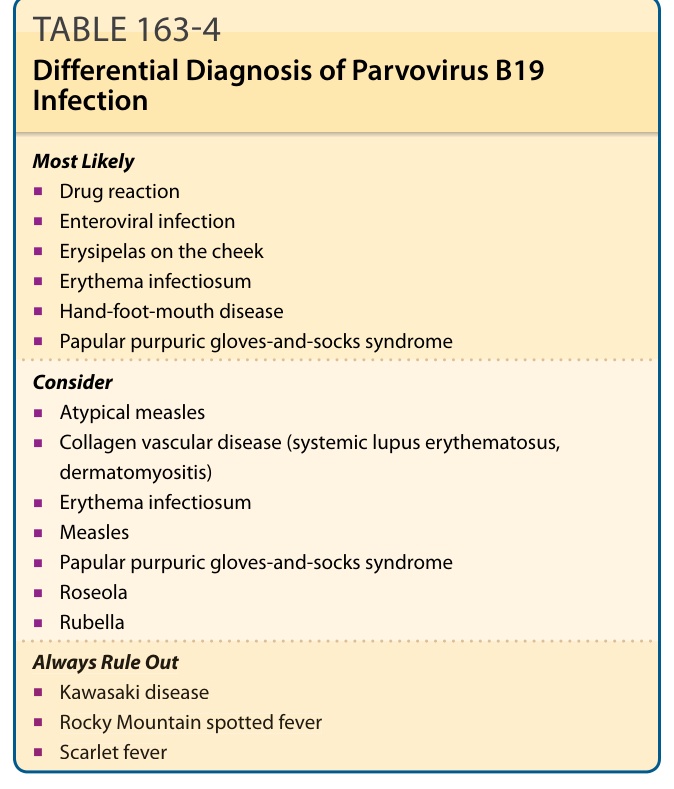
Table 163-4 outlines the differential diagnosis of parvovirus B19 infection.
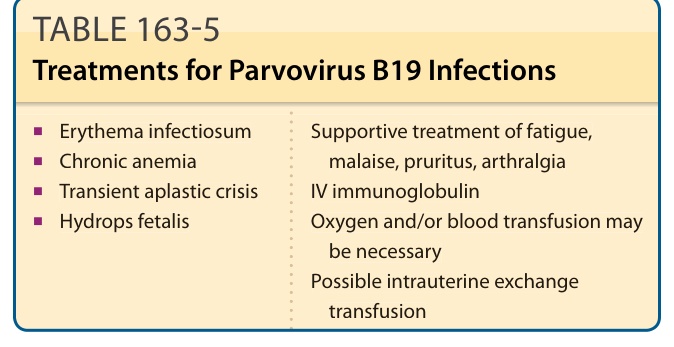
TABLE 163-5 Treatments for Parvovirus B19 Infections
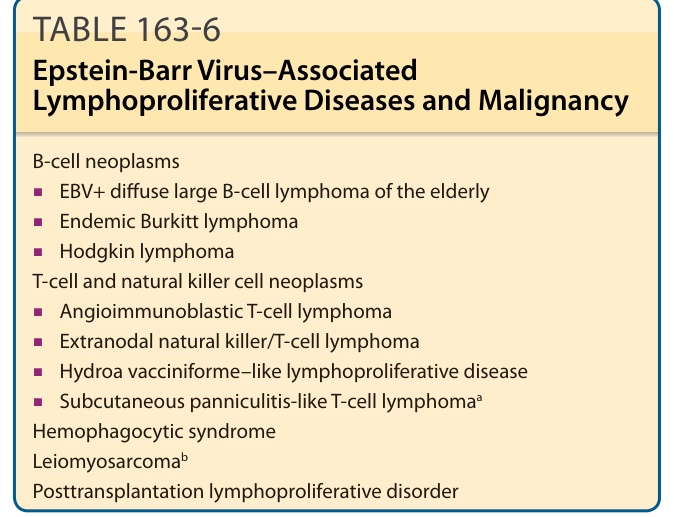
TABLE 163-6 Epstein-Barr Virus–Associated Lymphoproliferative Diseases and Malignancy
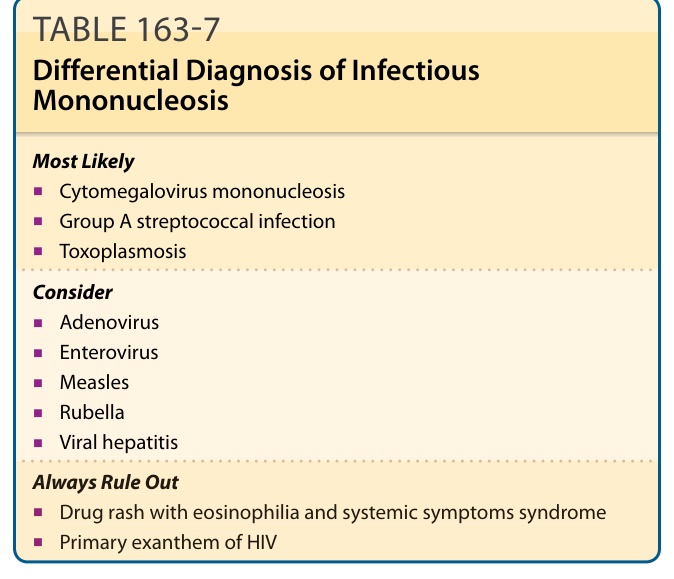
Table 163-7 outlines the differential diagnosis of infectious mononucleosis.
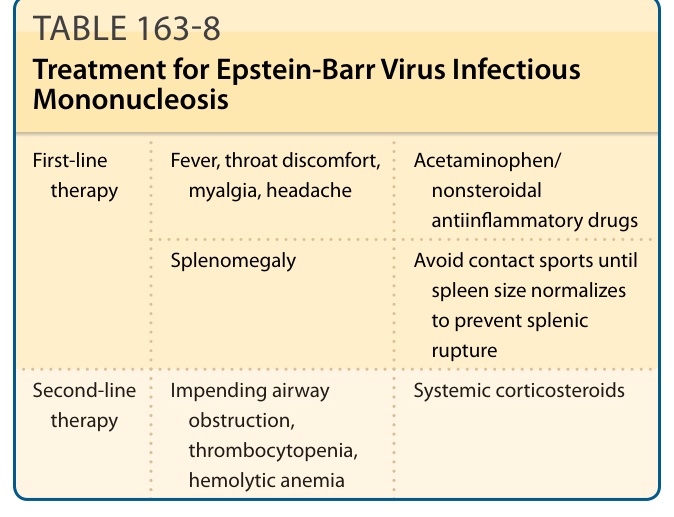
TABLE 163-8 Treatment for Epstein-Barr Virus Infectious Mononucleosis
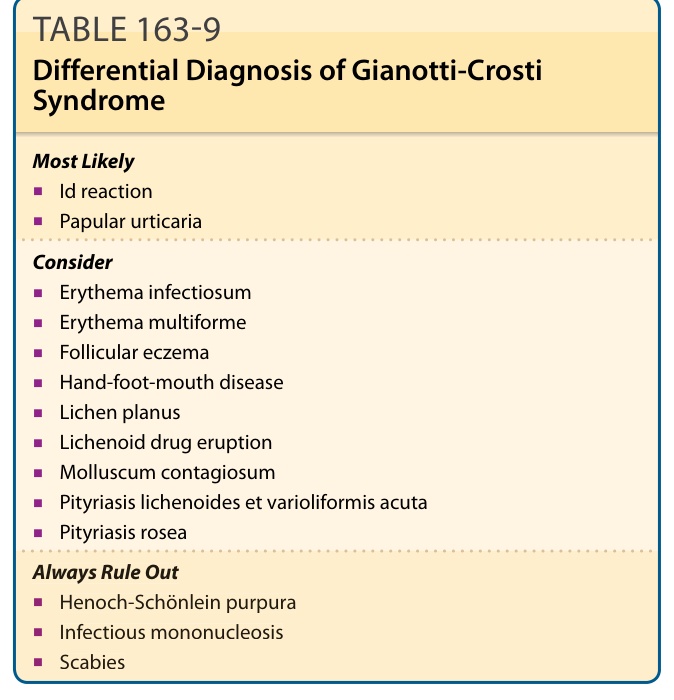
Table 163-9 outlines the differential diagnosis of GCS.
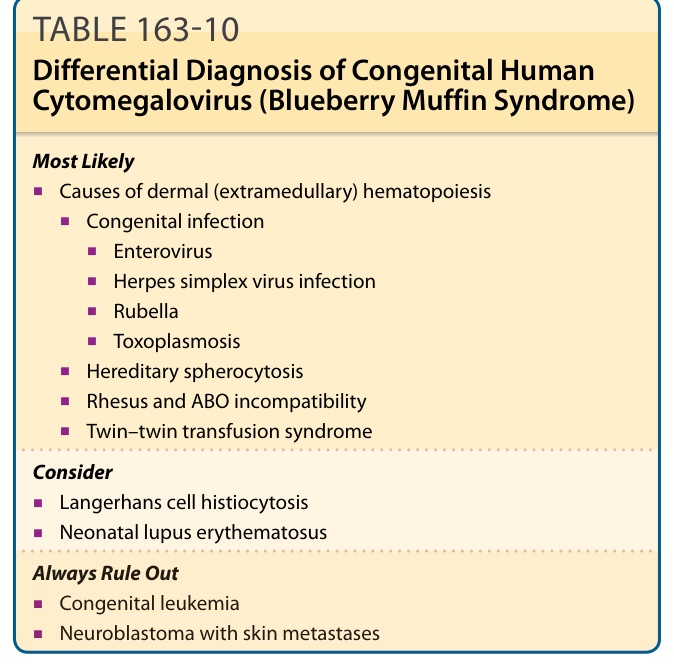
Tables 163-10 and 163-11 outline the differential diagnosis of HCMV blueberry muffin syndrome and mononucleosis infection, respectively.
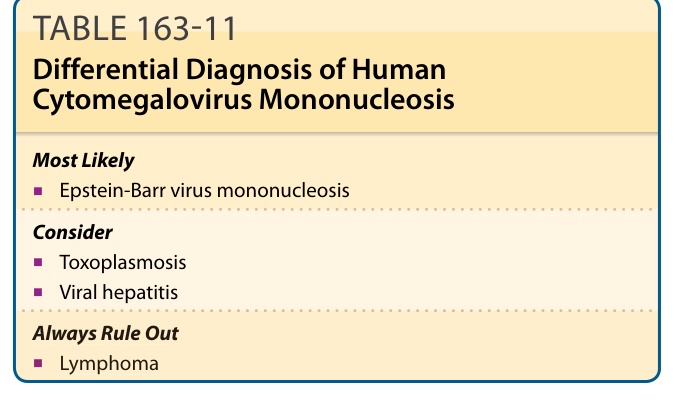
TABLE 163-11 Differential Diagnosis of Human Cytomegalovirus Mononucleosis
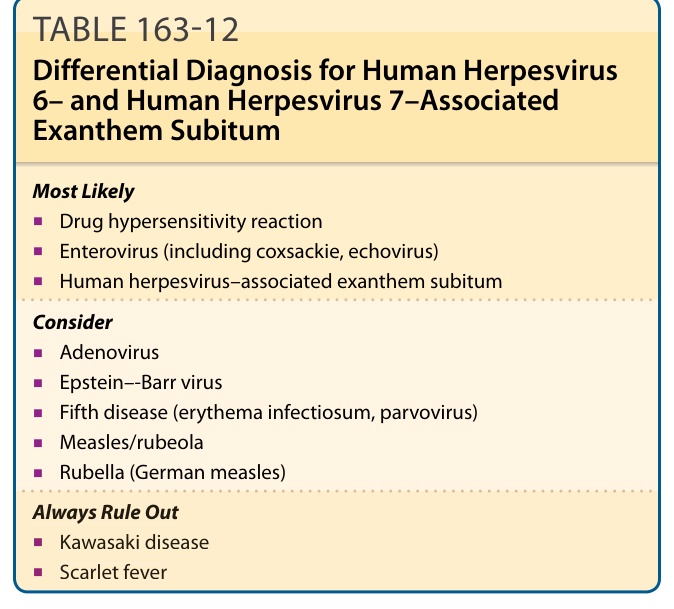
TABLE 163-12 Differential Diagnosis for Human Herpesvirus 6– and Human Herpesvirus 7–Associated Exanthem Subitum
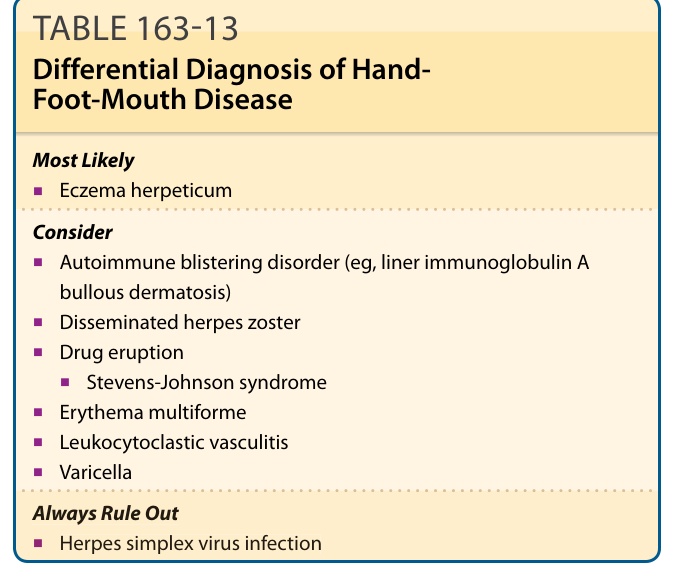
Table 163-13 outlines the differential diagnosis of HFMD.
Table 163-14 outlines the differential diagnosis of ULE.
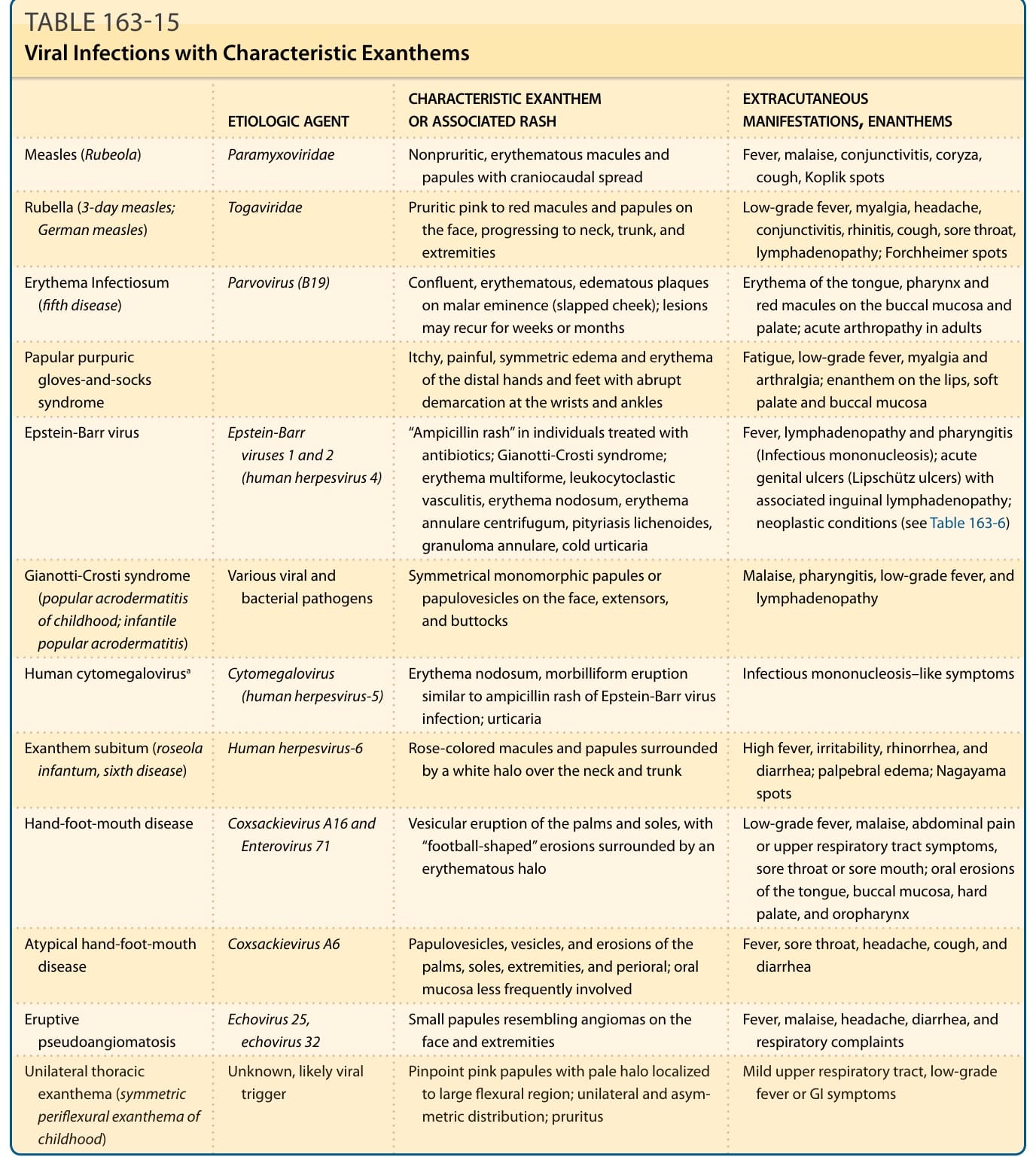
TABLE 163-15 Viral Infections with Characteristic Exanthems