Deep Fungal Infections
24
Deep fungal infections comprise 2 distinct groups of conditions: subcutaneous mycoses and systemic mycoses. Neither are common, and the subcutaneous mycoses, with some exceptions, are largely confined to the tropics and subtropics. In recent years, the systemic mycoses have become important opportunistic infectious complications in immunocompromised patients, including those with AIDS and patients receiving treatment for malignancies. They also include a group of primary respiratory tract infections, such as histoplasmosis and coccidioidomycosis, which may affect otherwise healthy individuals and those with underlying illness. The fungi that cause these respiratory tract infections are usually dimorphic or exist in a different morphologic phase (eg, yeast or mold) at different stages of their life cycle. Patients with subcutaneous fungal infections often present to a physician with signs of skin involvement. By contrast, patients with systemic mycoses only occasionally have skin lesions, either following direct involvement of the skin as a portal of entry or after dissemination from a deep focus of infection. There are a number of excellent texts about fungi and the diseases they cause.1-4
Treatment of these conditions remains difficult in many cases, although there is now a wide range of antifungal drugs with different modes of action.
SUBCUTANEOUS MYCOSES
AT-A-GLANCE
Subcutaneous mycoses:
■ Are usually sporadic.
■ Are contracted in the tropics and subtropics.
■ May cause chronic disability.
■ Are best diagnosed by histopathology, except for sporotrichosis.
■ Often require months of successful antifungal treatment.
The subcutaneous mycoses (Table 162-1), or mycoses of implantation, are infections caused by fungi that have been introduced directly into the dermis or subcutaneous tissue through a penetrating injury, such as a thorn prick. Although many are tropical infections, others, such as sporotrichosis, are also prevalent in temperate climates; any of these infections may present as an imported disease in a patient who has originated from an endemic area, sometimes after a lapse of
many years. The most common subcutaneous mycoses are sporotrichosis, mycetoma, and chromoblastomycosis. Rarer infections include lobomycosis and subcutaneous mucormycosis.
SPOROTRICHOSIS
SPOROTRICHOSIS
DEFINITIONS
Sporotrichosis is a subcutaneous or systemic fungal infection caused by the dimorphic fungus Sporothrix. Based on molecular techniques, there are now known to be at least 5 different species that vary in geographic distribution: Sporothrix schenckii, Sporothrix brasiliensis, Sporothrix globosa, Sporothrix luriei, and Sporothrix mexicana.5,6
HISTORICAL PERSPECTIVE
The fungus occurs in the natural environment, presumably in mold (cells growing in a chain) form, but develops as a yeast (cells growing as single cells) in infections. The most frequent site of this infection is the dermis or subcutis. There is also a systemic form of sporotrichosis whose clinical features range from pulmonary infection to arthritis or meningitis. One important characteristic of the diagnosis of cutaneous lesions is the scarcity of organisms in tissue, making confirmation of the diagnosis by microscopy potentially difficult.6 Sometimes in tissue, fungal cells are surrounded by an eosinophilic refractile fringe, the asteroid body, that is a characteristic of the organism, although a similar phenomenon may occur with other infectious organisms (eg, Schistosome eggs).
EPIDEMIOLOGY
Infections occur in both temperate and tropical countries. They are seen in North, South, and Central America, including the southern United States and Mexico, as well as in Africa, Egypt, Japan, and Australia.6
The countries where the highest rates of infection occur are Mexico, Brazil, and South Africa. However, sometimes hyperendemic areas are found where large numbers of cases occur.7 In the United States, infections are most common in the midwestern river valleys. Infections are now rare in much of Europe. In nature, the fungus grows on decaying vegetable matter such as plant debris, leaves, and wood. Although it is usually a cause of sporadic infection, Sporothrix also may affect groups of workers exposed to the organism, such as those using straw as a packing material, gardeners,
4
24
Eumycetoma: Ketoconazole 200 mg Itraconazole 200 mg Voriconazole 200 to 400 mg daily × several months
Actinomycetoma: Dapsone + streptomycin Sulfamethoxazole-trimethoprim + rifampin or streptomycin
Itraconazole 200 mg once daily or Terbinafine 250 mg once daily or IV amphotericin B (up to 1 mg/kg/day) Treatment continued for several months, until clinical resolution
Itraconazole 200 mg once daily Terbinafine 200 mg once daily treatment continued until 1 week after clinical resolution
Mixed granulomatous reaction with neutrophilic microabscesses Fungus is 3 to 5 µm, cigar-shaped or oval Distinctive asteroid body
Chronic inflammatory reaction with neutrophil abscesses and scattered giant cells and fibrosis Grains found at center
Mixed granulomatous response, with small neutrophilic abscesses and exuberant epidermal hyperplasia The organism may appear singly or in small groups of brownpigmented cells
The feet, legs, arms, or upper trunk are commonly involved Begins as a slowly expanding warty papule; may be a plaque-like lesion with an atrophic center. May develop satellite lesions from autoinoculation
The foot, lower leg, or hand is commonly involved; may affect head or back Characterized by a firm, painless nodule that spreads slowly with development of papules and draining sinus tracts; later signs include local swelling, chronic sinus formation, and bone involvement
Lymphangitic: dermal nodule that breaks down into a small ulcer Fixed: localized to one site, with granuloma formation and ulceration
North, South, Central Americas, including southern United States and Mexico, Africa, Egypt, Japan, Australia
Central and South America, Caribbean, Africa, South Asia, Australasia, Japan
Usually in dry tropical areas, such as Central America, Mexico, Sudan, and the Middle East
Filamentous bacteria (actinomycetoma): Nocardia sp. Madurella mycetomatis Streptomyces somaliensis Scedosporium apiospermum
Sporotrichosis
Sporothrix schenckii S. brasiliensisSporothrix brasiliensis Sporothrix globosa Sporothrix luriei Sporothrix mexicana
Chromoblastomycosis (chromomycosis) Philaophora verrucosa Fosecaea pedrosoi Fonsecaea compactum Wangiella dermatitidis Cladophialophora carrionii
Fungal (eumycetoma)
Mycetoma (maduromycosis, Madura foot)
Antifungal therapy is not effective Surgical removal is the main treatment
Ketoconazole 400 mg daily Itraconazole 100 to 200 mg daily Treatment with SSKI (similar to sporotrichosis treatment)
Surgical excision advised, but relapse may occur
treatment
Exophiala jeanselmei Wangiella dermatitidis More common in the tropics Lesions present as cysts. Cyst wall consists of palisades of macrophages and other inflammatory cells surrounded by a fibrous capsule; fungal hyphae may be found in the macrophage zone
Large sporangia or spore sacs in dif-f-f
Large, pop-bead organisms within histiocytes and multinucleated giant cells
Subcutaneous mucormycosis
Basidiobolus ranarum (Basidiobolus haptosporus) South America, Africa, Indonesia Develop around limb-girdle sites A firm, slowly spreading woody cellulitis Chronic granulomatous response with many eosinophils; fungi are present as large, strap-like hyphae without cross walls or septa Splendore-Hoeppli phenomenon
Conidiobolus coronatus
Facial involvement, beginning in the inferior nasal turbinates and spreading to the central part of the face; swelling is hard and painless
site; conjunctival mucosa also may be
The nasal mucosa is the main affected site; conjunctival mucosa also may be susceptible Characterized by polyps studded with white flecks
The nasal mucosa is the main affected
Characterized by polyps studded with
white flecks
susceptible
Caribbean, and South Africa
South America, the
Phaeohyphomycosis (phaeomycotic cyst, cystic chromomycosis)
Lobomycosis (keloidal blastomycosis, Lobo disease)
24
4
24
forestry workers, and those whose recreational activities bring them into contact with plant debris. A recent outbreak of sporotrichosis in Brazil (mainly caused by S. brasiliensis) has accentuated the role of exposure to other sources of infection, in this domestic or feral cats. The organism is thought to be introduced into the skin through a local injury.
CLINICAL FEATURES Cutaneous Findings: The 2 clinical varieties of sporotrichosis are the subcutaneous and systemic forms of disease.5,8,9 Subcutaneous sporotrichosis is by far the more common and includes 2 main forms: (a) lymphangitic and (b) fixed infections. The lymphangitic form is the more common and usually develops on exposed skin sites such as hands or feet. The first sign of infection is the appearance of a dermal nodule that breaks down into a small ulcer. Draining lymphatics become inflamed and swollen, and a chain of soft secondary nodules develops along the course of the lymphatic (Fig. 162-1); these also may break down and ulcerate. In the fixed variety, which accounts for approximately 15% of cases, the infection remains localized to 1 site, such as the face, and a granuloma develops that subsequently may ulcerate. Satellite nodules or ulcers may form around the rim of the primary lesion. Other clinical variants of subcutaneous sporotrichosis may mimic mycetoma, lupus vulgaris, and chronic venous ulceration. In some cases, deep extension of the infection may affect joints or tendon sheaths. Patients with AIDS who develop sporotrichosis often have multiple cutaneous lesions9 without prominent lymphatic involvement, but deep infections, such as arthritis, are also reported.
Noncutaneous Findings: In the much rarer systemic form of sporotrichosis, lesions can develop almost anywhere, although chronic lung nodules, with cavitation, arthritis, and meningitis have been described most frequently. These may coexist with cutaneous lesions of sporotrichosis.
2968
DIAGNOSIS Laboratory Testing: The best sources of diagnostic material are smears, exudates, and biopsies. Sporothrix is seen very rarely in direct microscopic examination because yeasts are usually present only in small numbers; the organism can be isolated readily on Sabouraud agar. In primary culture, the fungus grows as a mold, with compact, white colonies that darken with age. Microscopically, the hyphae produce small oval or triangular conidia either on specialized hyphae or elsewhere on the mycelium. Ideally, the organism should be converted to yeast phase on enriched media such as brain-heart infusion agar at 37°C (98.6°F) to complete the identification.
Pathology: Pathologically, sporotrichosis causes a mixed granulomatous reaction with neutrophil microabscesses. The fungus, if present, is usually in the form of small (3 to 5 µm) cigar-shaped or oval yeasts that may, on occasion, be surrounded by a thick, radiating eosinophilic fringe forming the distinctive asteroid body. Organisms are usually sparsely distributed in lesions, and it may be necessary to scan several sections to identify a single yeast. An intradermal sporotrichin skin test is available in some countries and may have a role to play in allowing the physician to identify the most appropriate laboratory investigations to instigate.
DIFFERENTIAL DIAGNOSIS
Conditions commonly confused with sporotrichosis are mycobacterial (see Chap. 157) and primary cutaneous Nocardia infections (see Chap. 158) and leishmaniasis (see Chap. 178). The nontuberculous mycobacterial infection caused by Mycobacterium marinum (fish-tank granuloma), in particular, closely resembles lymphangitic sporotrichosis.
CLINICAL COURSE AND PROGNOSIS
With the correct treatment, cases of sporotrichosis resolve readily, but untreated they can persist for more than 3 years.
MANAGEMENT Interventions: Although spontaneous remissions may occur, most patients are treated with antifungal chemotherapy.10 Treatments include itraconazole (200 mg daily) and terbinafine (250 mg daily), which are better tolerated, and intravenous amphotericin B for deep infection; as of this writing there has been little experience with voriconazole or posaconazole. In all cases, treatment is continued for at least 1 week after clinical resolution. A cheaper alternative is potassium iodide (saturated solution), 4 to 6 mL thrice daily, which is effective in the cutaneous types of sporotrichosis and should be continued for 3 to 4 weeks after clinical cure. The daily dose is built up slowly from
1 mL thrice daily over 2 to 3 weeks to avoid side effects such as hypersalivation and nausea. This is an inexpensive form of therapy, but it is unpalatable.
Prevention: There is no preventive management.
MYCETOMA (MADUROMYCOSIS, MADURA FOOT)
MYCETOMA
(MADUROMYCOSIS,
MADURA FOOT)
DEFINITIONS
Mycetoma is a chronic localized infection caused by different species of fungi or actinomycetes. It is characterized by the formation of aggregates of the causative organisms, known as grains that are found within abscesses. These either drain via sinuses onto the skin surface or involve adjacent bone, causing a form of osteomyelitis. Grains are discharged onto the skin surface via these sinuses. The disease advances by direct spread, and distant metastatic sites of infection are very rare. Mycetomas caused by species of fungi are known as eumycetomas, and those caused by aerobic actinomycetes or filamentous bacteria are known as actinomycetomas (see Chap. 158). The organisms are usually soil or plant saprophytes11 that are only incidental human pathogens.
HISTORICAL PERSPECTIVE
Mycetoma has been designated a neglected tropical disease by the World Health Organization.12
EPIDEMIOLOGY
Mycetomas are mainly, but not exclusively, found in the dry tropics where there is low annual rainfall.11,12
They are sporadic infections that are seldom common, even in endemic areas.13 Occasionally, nonimported cases are reported from temperate climates, although in these cases, the most common organism is Scedosporium apiospermum. Actinomycetomas caused by Nocardia sp. are most common in Central America and Mexico. In other parts of the world, the most common organism is a fungus, Madurella mycetomatis. The actinomycete Streptomyces somaliensis is isolated most often from patients originating from Sudan and the Middle East. The causative organisms of mycetoma have been isolated or detected by molecular methods from either soil or plant material, including Acacia thorns, in endemic areas. The organisms are implanted subcutaneously, usually after a penetrating injury. It is unusual to find any underlying predisposition in patients with mycetoma, and the persistence of the organism after the initial inoculation appears to be related to its ability to evade host defenses through a variety of adaptations, such as cell-wall thickening and melanin deposition.14
24
CLINICAL FEATURES Cutaneous Features: The clinical features of both fungal and actinomycete mycetomas are very similar.12 They are most common on the foot, lower leg, or hand, although head or back involvement also may occur. Infection of the chest wall is most characteristic of Nocardia infections (see Chap. 158). The earliest stage of infection is a firm, painless nodule that spreads slowly with the development of papules and draining sinus tracts over the surface (Fig. 162-2).
Complications: Local tissue swelling, chronic sinus formation, and later bone involvement distort and deform the original site of infection (Figs. 162-3 and 162-4). Lesions are seldom painful except in the late stages and where sinus tracts are about to emerge onto the skin surface.
Noncutaneous Findings: Dissemination from the initial site is exceptionally rare, although local lymphadenopathy may occur.
2969
4
24
DIAGNOSIS Laboratory Testing: Finding the mycetoma grains is the key to establishing the diagnosis, and these are generally discharged from the openings of sinus tracts. However, they also may be obtained by removing the surface crust from a pustule or sinus tract with a sterile needle and gently squeezing the edges. Grains are 250- to 1000-µm white, black, or red particles that can be seen with the naked eye (Table 162-2). Direct microscopy of grains is important
ORGANISMS HEMATOXYLIN AND EOSIN SECTION APPEARANCES
Eumycetoma
Dark grains Madurella mycetomatis, Madurella fahalii, M. sudanensis
Cement present, vesicles sometimes prominent
Trematosphaeria grisea Cement absent, compact outer layer Falciformispora senegalensis Cement in outer zone, dark periphery with vesicular center Exophiala jeanselmei Cement absent, often hollow Medicopsis romeroi Cement lacking, compact outer layer
Pale grains
Fusarium sp., Acremonium, Scedosporium apiospermum, Aspergillus nidulans, Neotestudina rosati
Compact, pigment lacking, interwoven fungal filaments (Scedosporium apiospermum may have prominent vesicles)
Actinomycetoma
Pale (white to yellow) grains
Actinomadura madurae Basophilic-stained fringe in layers Nocardia brasiliensis Small, pale blue, eosinophilic fringe
Yellow to brown grains Streptomyces somaliensis Grains fractured, basophilic, or pink
p g Actinomadura pelletieri Small, basophilic layers
Red to pink grains
Actinomadura pelletieri Small, basophilic layers
aHelpful rules of thumb:
■Black or dark grains are always produced by fungi;
■Red grains are always produced actinomycetes;
■But pale (white) grains may be produced by either fungi or actinomycetes.
2970
because it will show whether the grain is composed of the small actinomycete or broader fungal filaments. In general, it is not possible to distinguish the fine actinomycete filaments in potassium hydroxide (KOH) mounts or, for that matter, in hematoxylinand-eosin–stained material. In addition, black grains are always caused by fungi; red grains, by actinomycetes (Table 162-2). Final identification requires isolation of the causal agent in culture. In view of the number of possible species, a series of different culture media and conditions of incubation should be used. Morphologic and physiologic characteristics are used to distinguish between the genera and species. There are now a few examples where the organism has been identified using specific primers through use of the polymerase chain reaction (PCR). Serology is diagnostically helpful only in some cases (eg, in S. somaliensis), and even then, more as a guide to therapeutic response. In a few centers, molecular tools are used to identify organisms and this has resulted in changes in their nomenclature (see Table 162-2).
Pathology: Histologically, there is a chronic inflammatory reaction with neutrophil abscesses and scattered giant cells and fibrosis.11 Grains are found in the center of the inflammation. Their size and shape may help in the identification, although with nonpigmented (pale or white grain) eumycetomas, this is seldom sufficient (Fig. 162-5).
Imaging: X-ray changes include periosteal erosion and proliferation, as well as the development of lytic lesions in the bone. Bone scans or MRI may identify bone lesions and soft-tissue changes at an earlier stage.
DIFFERENTIAL DIAGNOSIS
Chronic bacterial or tuberculous osteomyelitis may resemble mycetoma. Actinomycosis (see Chap. 158) is also similar but usually develops close to certain sites, such as the mouth or the cecum, where the causative organisms are sometimes commensal.
CLINICAL COURSE AND PROGNOSIS
There is no spontaneous remission.
MANAGEMENT Medications: Of the fungal causes of mycetoma, some cases of M. mycetomatis infection respond to ketoconazole 200 mg, itraconazole 200 mg, or voriconazole 200 to 400 mg daily over several months. For the others, a trial of therapy with griseofulvin or terbinafine is worth attempting. However, responses to chemotherapy are unpredictable, although antifungals may slow the course of infection. Actinomycetomas (see Chap. 158) generally respond to antibiotics such as a combination of dapsone with streptomycin or sulfamethoxazole-trimethoprim plus rifampin or streptomycin. Amikacin, moxifloxacin, or imipenem also may be used in recalcitrant Nocardia infections. The responses in all but a few cases are good.15
Procedures: Surgery, usually amputation, is the definitive procedure and may have to be used in advanced cases. However, in defined lesions surgical dissection following antifungal therapy can produce excellent results.15
Prevention: Diagnosis of early lesions will form part of a new targeted strategy for mycetoma.
CHROMOBLASTOMYCOSIS (CHROMOMYCOSIS)
CHROMOBLASTOMYCOSIS
(CHROMOMYCOSIS)
DEFINITIONS
Chromoblastomycosis is a chronic fungal infection of the skin and subcutaneous tissues caused by pigmented (dematiaceous) fungi that are implanted into the dermis from the environment. In the ensuing inflammation, they form thick-walled single cells or cell clusters (sclerotic or muriform bodies), and these may elicit a marked form of pseudoepitheliomatous hyperplasia, which is often accompanied by transepidermal elimination of organisms.
HISTORICAL PERSPECTIVE
The infection can be caused by a number of different pigmented fungi, the most common being Phialophora verrucosa, Fonsecaea pedrosoi, Fonsecaea compactum, Wangiella dermatitidis, and Cladophialophora carrionii.16
EPIDEMIOLOGY
The fungi that cause chromoblastomycosis can be isolated in the environment from wood, plant debris, or soil.17 The majority of infections are caused by F. pedrosoi and C. carrionii. As with other subcutaneous
24
mycoses, infection follows implantation through a tissue injury. The infection is found as a sporadic condition in Central and South America, and rarely in North America. It occurs in the Caribbean region, Africa (particularly Madagascar), South Asia, Australasia, and Japan. It also may occur as an imported infection outside the usual endemic areas. The disease is most frequent in male rural workers.
CLINICAL FEATURES Cutaneous Findings: The initial site of the infection is usually on the feet, legs, arms, or upper trunk. The clinical features vary.17 The initial lesion is often a warty papule that expands slowly over months or years (Figs. 162-6 and 162-7). Alternatively, lesions may be plaque-like with an atrophic center. The more common verrucous form spreads slowly and locally. Individual lesions may be very thick and often develop secondary bacterial infection. Satellite lesions around the initial site of infection are local extensions of the infection and usually are produced by scratching.
Complications: Complications of chromoblastomycosis include local lymphedema, leading to elephantiasis and squamous cell carcinomas in some chronic lesions.
DIAGNOSIS Laboratory Testing: The typical sclerotic or muriform fungal cells can be seen in skin scrapings taken from the surface of lesions, particularly areas
2971
4
24
where there is a small, dark spot on the skin surface, using KOH mounts. In culture, these fungi are very similar in gross macroscopic appearance, producing black colonies with a downy surface. Their cultural identification depends on demonstrating the presence of different but specific types of sporulation, and either single or multiple sporulation mechanisms may be seen in each organism. Accurate differentiation between the different fungi may be difficult. At this stage, the choice of treatment does not depend critically on correct identification of the organisms, although there may be differences in the speed of response to azole drugs (see section “Management (mycetoma)”).
Pathology: The lesions also should be biopsied because the pathologic changes and presence of muriform cells are typical. The histology shows a mixed granulomatous response, with small neutrophil abscesses and often exuberant epidermal hyperplasia.18
The organisms, which are often seen either in giant cells or in neutrophil abscesses, appear singly or in small groups of brown pigmented cells, often with a single or double septum and thick cell wall.
DIFFERENTIAL DIAGNOSIS
The disease must be differentiated from podoconiosis or chronic tropical lymphedema with hyperplasia (mossy foot), which is a result of a reaction to soil microparticles. Other chronic verrucous lesions, such as tuberculosis, sporotrichosis, and blastomycosis, should also be considered. The identification of organisms in the lesions of chromoblastomycosis is essential.
CLINICAL COURSE AND PROGNOSIS
There is no spontaneous remission.
MANAGEMENT Medications: The main treatments for chromoblastomycosis are itraconazole, 200 mg daily19;
2972
terbinafine, 250 mg daily20; and, in extensive cases, IV amphotericin B (up to 1 mg/kg daily). The responses of these fungi to different antifungal agents do not appear to differ significantly, although there is some evidence that C. carrionii responds more rapidly to terbinafine and itraconazole. In any event, treatment is continued until there is clinical resolution of lesions, which usually takes several months. Extensive lesions often respond poorly to conventional treatment and combinations of antifungal drugs, for example, amphotericin B and flucytosine or itraconazole and terbinafine, have been used.
Procedures: Lesions can be spread by surgery, which should be used only as an adjunctive therapy after drug treatment. The local application of heat might be helpful in some instances.
PHAEOHYPHOMYCOSIS (PHAEOMYCOTIC CYST, CYSTIC CHROMOMYCOSIS)
PHAEOHYPHOMYCOSIS
(PHAEOMYCOTIC CYST,
CYSTIC CHROMOMYCOSIS)
Phaeohyphomycosis is a rare infection characterized by the formation of subcutaneous inflammatory cysts or plaques. It is caused by dematiaceous fungi, the most common of which are Exophiala jeanselmei and W. dermatitidis, but some 103 species have been described as causal agents.21 However, unlike in chromoblastomycosis, these organisms form short, irregular, pigmented hyphae in tissue. The infection may occur in any climatic area, although it is more common in the tropics. It also may appear in immunosuppressed patients, particularly those receiving long-term glucocorticoid therapy. The lesions present as cysts and may be mistaken for other similar structures, such as synovial or Baker cysts. The diagnosis is usually made after surgical excision. Histologically, the cyst wall consists of palisades of macrophages and other inflammatory cells surrounded by a fibrous capsule, and the fungal hyphae are found in the macrophage zone. Although the fungi in tissue lesions are usually pigmented, this is not always the case; cystic lesions caused by nonpigmented fungi are called hyalohyphomycotic cysts. The treatment is surgical excision, although relapse can occur, particularly in immunocompromised patients.
LOBOMYCOSIS (KELOIDAL BLASTOMYCOSIS, LOBO DISEASE)
LOBOMYCOSIS (KELOIDAL
BLASTOMYCOSIS, LOBO
DISEASE)
Lobomycosis is an uncommon infection seen in Central and tropical South America, often in remote rural areas. The source of the organism is unknown,
although similar lesions have been found on freshwater dolphins. Lobomycosis is characterized by the appearance of keloid-like skin lesions on exposed sites.22 Although it cannot be cultured in vitro, it is caused by a fungus, Lacazia loboi, that forms chains of rounded cells in tissue, each joined by a small tubule. Lesions may occur anywhere on the body but usually are found on exposed parts such as the legs, arms, and face. They can spread from site to site by autoinoculation. Antifungal drugs are not effective, and surgical removal is the main treatment.
SUBCUTANEOUS MUCOR- MYCOSIS (BASIDIOBOLO- MYCOSIS, SUBCUTANEOUS PHYCOMYCOSIS, AND CONIDIOBOLOMYCOSIS, [RHINO]-ENTOMOPHTHORO- MYCOSIS]
SUBCUTANEOUS MUCOR
MYCOSIS (BASIDIOBOLO
MYCOSIS, SUBCUTANEOUS
PHYCOMYCOSIS,
AND CONIDIOBOLOMYCOSIS,
[RHINO]-ENTOMOPHTHORO
MYCOSIS]
Subcutaneous mucormycosis is a rare tropical subcutaneous mycosis characterized by the development and spread of a chronic, firm, swelling involving subcutaneous tissue. There are 2 main varieties caused by different organisms.23 The first, most often caused by Basidiobolus ranarum (Basidiobolus haptosporus), is more common in children. It occurs in a wide variety of countries and environments from South America to Africa and Indonesia. The organism can be found in plant debris and in the intestinal tracts of reptiles and amphibians. Lesions usually develop around limb girdle sites and present with a firm, slowly spreading, woody cellulitis. The second form, caused by Conidiobolus coronatus, is seen in adults. The organism can be isolated from soil, plant debris, and some insects. The early infection starts in the region of the inferior turbinates of the nose. Spread involves the central part of the face, and once again, the swelling is hard and painless. It may cause very severe deformity of the nose, lips, and cheeks. These infections are distinct to those caused by related fungi. Histopathologically, a chronic granulomatous response with large numbers of eosinophils can be seen. The fungi are present as large, strap-like hyphae without cross walls or septa. They are also often surrounded by refractile eosinophilic material (Splendore-Hoeppli phenomenon). The organisms can be cultured readily on Sabouraud agar. Ketoconazole (400 mg daily) and itraconazole (100 to 200 mg daily) also may be useful in this condition, although experience as of this writing is limited to a few cases. Lesions also respond to oral treatment with potassium iodide, given in similar doses to those used in sporotrichosis (see “Management” under “Sporotrichosis”).
24
RHINOSPORIDIOSIS
RHINOSPORIDIOSIS
Rhinosporidiosis is a chronic infection caused by the organism Rhinosporidium seeberi, which causes the development of polyps affecting the mucous membranes. The organism has never been cultured, and it is now thought to be an aquatic protist and a member of the Mesomycetozoea. Rhinosporidiosis is seen most often in Southern India and Sri Lanka. Cases also have been described in South America, the Caribbean, and South Africa. Exposure to water (lakes, pools) is associated with the infection. The main site affected is the nasal mucosa, but the conjunctival mucosa also may be affected.24 The infection causes the development of polyps that are studded with white flecks; these are small cysts or sporangia containing small spores. These are best seen in histopathologic sections, where the large sporangia or spore sacs in different phases of development are readily seen. The only treatment is surgical excision.
SYSTEMIC MYCOSES
AT-A-GLANCE
■ Where the patient has lived or visited is important for diagnosis of systemic mycoses.
■ History of underlying disease states and their treatment is critical.
■ Erythema nodosum may be caused by some endemic mycoses (eg, coccidioidomycosis).
■ Skin biopsy is important in making the diagnosis.
■ Positive fungal culture must be interpreted with caution, as the organism identified may simply be colonizing the site.
■ Warn the laboratory if you are sending material from a suspected endemic mycosis case for culture, as these are dangerous pathogens and require containment facilities.
■ Treatment may require prolonged therapy with IV drugs such as amphotericin B, voriconazole, and caspofungin.
The systemic mycoses are fungal infections whose initial portal of entry into the body is usually a deep site such as the lung, GI tract, or paranasal sinuses. They have the capacity to spread via the bloodstream to produce a generalized infection. In practice, there are 2 main varieties of systemic mycosis: (a) the opportunistic mycoses and (b) the endemic respiratory mycoses. The chief opportunistic systemic mycoses seen in humans are systemic or deep candidiasis, aspergillosis, and systemic zygomycosis. These affect patients with severe underlying disease states, such as AIDS, or with neutropenia associated with malignancy, as well
2973
4
24
PREDISPOSITION INFECTION
Neutropenia (whatever cause) functional neutrophil defects
Aspergillosis, oropharyngeal, and/or systemic candidiasis, mucormycosis, infections caused by rare organisms
CD4 lymphopenia (eg, AIDS) Oropharyngeal candidiasis, cryptococcosis, and endemic respiratory mycoses such as histoplasmosis, nocardiosis
Biologic therapy (eg, anti– tumor necrosis factor or anti–interferon-γ)
Endemic mycoses (eg, histoplasmosis, coccidioidomycosis, Talaromyces infection)
Diabetes mellitus Mucormycosis
Heart valve surgery Various but mainly Candida albicans and non-albicans Candida sp.
Abdominal surgery Candidiasis
Abdominal surgery Candidiasis
as recipients of solid-organ transplantations, immunomodulating biologic therapies, or extensive surgery. With the use of combination antiretroviral therapy, the incidence of systemic mycoses in patients infected
with HIV has dropped considerably. In the neutropenic patient in particular, other fungi also may cause infection occasionally. Different underlying conditions predispose to different mycoses; Table 162-3 outlines a scheme for this. Generally, skin involvement is not common with most of these opportunistic infections, which can occur in any climate and environment. The clinical manifestations of the opportunistic mycoses are also variable because they depend on the site of entry of organism and the underlying disease. The endemic respiratory mycoses are histoplasmosis (classic and African types), blastomycosis, coccidioidomycosis, paracoccidioidomycosis, and infections due to Talaromyces marneffei. The clinical manifestations of these infections are affected by the underlying state of the patient, and many develop in the presence of particular immunodeficiency states, notably AIDS. However, they follow similar clinical patterns in all infections. These infections also may affect otherwise healthy individuals. They have well-defined endemic areas determined by factors that favor the survival of the causative organisms in the environment, such as climate. The usual route of infection is via the lung (Fig. 162-8). In practice, because of the tendency for both groups of infections to develop in predisposed patients, the distinction between opportunistic and endemic
Pathogenesis of endemic system mycoses
Entry from environment
A
Inhalation
Primary pulmonary infection Chronic pulmonary infection
Hematogenous dissemination from lung to other organs
(a) Acute (rapid) (b) Chronic for example
CNS
Primary cutaneous mycoses
B
Direct skin inoculation (rare)
- affects local lymph drainage
- usually no dissemination
2974
Skin
mycoses is blurred. This is particularly the case with cryptococcosis, which shares clinical and pathologic features of the 2 main types of respiratory systemic mycoses but is mainly seen now in untreated AIDS patients.
HISTOPLASMOSIS
HISTOPLASMOSIS
DEFINITION
Fungi of the dimorphic genus Histoplasma cause a number of different infections in animals and humans. These range from equine farcy, or equine histoplasmosis, a disseminated infection of horses caused by Histoplasma farciminosum to 2 human infections known as (a) classic or small-form histoplasmosis and (b) African histoplasmosis. These are caused, respectively, by 2 variants of Histoplasma capsulatum: (1) H. capsulatum var. capsulatum and (2) H. capsulatum var. duboisii. They can be distinguished because their respective yeast phases differ in size, the capsulatum variety producing cells from 2 to 5 µm in diameter and the duboisii form producing cells of 10 to 15 µm in diameter. The other important differences are in their epidemiology and clinical manifestations. They also show minor antigenic differences that are apparent in serodiagnosis but their mycelial phases are identical.
HISTORICAL PERSPECTIVE
The 2 types of human infections are referred to here as histoplasmosis and African histoplasmosis because this nomenclature is used most widely.
SMALL-FORM OR CLASSIC HISTOPLASMOSIS OR HISTOPLASMOSIS CAPSULATI
SMALL-FORM OR CLASSIC
HISTOPLASMOSIS OR
HISTOPLASMOSIS
CAPSULATI
DEFINITIONS
Histoplasmosis results from infection with the dimorphic fungus H. capsulatum var. capsulatum. A sexual state of this fungus, Ajellomyces capsulatus, also has been described. The infection starts as a pulmonary infection that, in most individuals, is asymptomatic and heals spontaneously, the only evidence of exposure being the development of a positive intradermal skin test reaction to a fungal antigenic extract, histoplasmin.25 However, there is, in addition, a symptomatic disease that includes respiratory tract infections and acute or chronic pulmonary histoplasmosis, as well as a disseminated infection that may spread to affect the skin or mucous membranes. Direct inoculation into the skin may occur as a result of a laboratory accident.
24
EPIDEMIOLOGY
Histoplasmosis occurs in many countries from the Americas to Africa, India, and the Far East. In the United States, it is endemic in the Mississippi and Ohio River valleys, where often more than 80% of the population may have acquired the infection asymptomatically. Exposure rates are usually lower in all other endemic areas, although high rates are also found in northern South America and some Caribbean islands. Histoplasmosis is not found in Europe. H. capsulatum is an environmental organism that can be isolated from soil, particularly when it is contaminated with bird or bat excreta. The disease is acquired by inhalation of spores, and epidemics of respiratory tract infection may occur in persons exposed to a spore-laden environment when exploring caves or cleaning sites heavily contaminated with bird droppings, such as bird roosts or barns. Although any person can acquire histoplasmosis through inhalation, it causes a distinctive disseminated infection in patients with disease affecting cellular immune capacity, such as AIDS or lymphoma.26,27
CLINICAL FEATURES
The spectrum of histoplasmosis includes both asymptomatic and benign symptomatic infections, and a progressive disseminated variety with bloodstream spread to multiple organs.25 Skin lesions may develop as a result of immune-complex formation in the primary infection (erythema multiforme) or from direct spread after dissemination from the lungs; rarely, infections may develop at a point of inoculation into the skin. Asymptomatic forms of histoplasmosis are, by definition, without signs or symptoms, but those exposed usually have a positive histoplasmin skin test. The percentage of skin test reactors in the community indicates the chances of exposure, and, in endemic areas, this may range from 5% to 90%. Occasionally, asymptomatic pulmonary nodules removed at surgical exploration or autopsy are found to contain Histoplasma.
Acute Pulmonary Histoplasmosis: In acute pulmonary histoplasmosis, patients are often exposed to large quantities of spores such as may be encountered in a cave or after cleaning a bird-infested area. Patients present with cough, chest pain, and fever, often with accompanying joint pains and rash—toxic erythema, erythema multiforme, or erythema nodosum. These skin rashes are not common, occurring in fewer than 15% of patients, but they may be precipitated by treatment of the acute infection. On chest radiography, there is often diffuse mottling, which may calcify with time.
Chronic Pulmonary Histoplasmosis: Chronic pulmonary histoplasmosis usually occurs in adults and presents with pulmonary consolidation and cavitation, closely resembling tuberculosis. Skin involvement is not seen.
2975
4
24
Acute Progressive Disseminated Histoplasmosis: In patients with acute disseminated histoplasmosis, there is widespread dissemination to other organs, such as the liver and spleen, lymphoreticular system, and bone marrow. Patients present with progressive weight loss and fever. This form is the type that is most likely to occur in untreated AIDS patients, who often develop skin lesions as a manifestation of disseminated infection (Fig. 162-9).28 There are papules, small nodules, or small molluscum-like lesions that subsequently may develop into shallow ulcers. These skin lesions are more common in HIV-positive patients than in others with disseminated histoplasmosis. Diffuse micronodular pulmonary infiltrates also may develop. Patients have progressive and severe weight loss, fever, anemia, and hepatosplenomegaly. The distinction between acute and chronic dissemination in histoplasmosis is somewhat artificial because these merely represent extremes of behavior, with progression occurring over a few months, on the one hand, and over several years, on the other. Intermediate forms occur, and other organs such as the meninges and heart may be affected.
Chronic Progressive Disseminated Histoplasmosis: Chronic disseminated histoplasmosis may appear months or years after a patient has left an endemic area. The most common clinical presenting features are oral or pharyngeal ulceration, hepatosplenomegaly, or adrenal insufficiency (Addison disease) resulting from adrenal infiltration. The mouth ulcers are often large, irregular, and persistent, and may affect the tongue as well as the buccal mucosa. The patients otherwise may appear well, but it is important
2976
to investigate for evidence of infection elsewhere (eg, by abdominal CT scan). Adrenal infection in particular should be excluded.
Primary Cutaneous Histoplasmosis: Primary cutaneous histoplasmosis is rare and follows inoculation of the organism into the skin, for instance, after accidental laboratory-acquired or postmortem room-acquired infection. The primary lesion is a nodule or indurated ulcer, and there is often local lymphadenopathy.
DIAGNOSIS Laboratory Testing: The diagnosis of histoplasmosis is established by identifying the small intracellular yeast-like cells of Histoplasma in sputum, peripheral blood, bone marrow, or biopsy specimens. Histoplasma must be separated from T. marneffei because the 2 organisms are of a similar size, although the latter shows characteristic septa formation. The identity of the organism should be confirmed by culture; it grows as a mold at room temperature. The white, cottony colonies develop at room temperature on Sabouraud glucose agar to produce 2 types of spores, the larger (8 to 15 µm in diameter), rounded, tuberculate macroconidia being typical; the smaller microconidia are infectious. Confirmation of the identity should be obtained by demonstrating ribosomal RNA using a DNA probe. Mycelial-phase cultures of H. capsulatum are very infectious, and laboratories receiving specimens should be warned about the suspected diagnosis. The intradermal histoplasmin skin test is an epidemiologic tool that is of no help in diagnosis. In patients with disseminated histoplasmosis, it is often negative. By contrast, serology is often useful in diagnosis. A rising complement-fixation titer indicates dissemination. Precipitins detected by immunodiffusion are also valuable because the presence of antibodies to specific H and M antigens correlates well with active or recent infection.28 A new development, particularly helpful in AIDS patients, has been serologic or urine tests for the detection of circulating Histoplasma antigens.29 PCRbased molecular diagnostic methods are available in some centers.
Pathology: In histopathologic sections, H. capsulatum is an intracellular parasite often seen in macrophages. The cells are small (2 to 4 µm in diameter) and oval in shape with small buds (Fig. 162-10). Mycelial forms are seen rarely in tissue.
DIFFERENTIAL DIAGNOSIS
The organism is the same size as a number of others causing deep mycoses such as T. marneffei and small forms of Blastomyces and Cryptococcus (see “Laboratory Testing” above). It is also similar in size to Leishmania sp., and in the tropics, kala azar is an important part of the differential diagnosis. These observations emphasize the importance of carrying out appropriate laboratory tests to confirm the diagnosis.
AFRICAN HISTOPLASMOSIS (LARGE-FORM HISTOPLAS- MOSIS OR HISTOPLASMO- SIS DUBOISII)
AFRICAN HISTOPLASMOSIS
(LARGE-FORM HISTOPLAS
MOSIS OR HISTOPLASMO
SIS DUBOISII)
African histoplasmosis is sporadic and uncommon even in AIDS patients.30 It is seen in patients from areas south of the Sahara and north of the Zambezi River in Africa. Infections seen outside Africa are all imported. The most common clinically involved sites are the skin and bone, although lymph nodes and other organs, including the lungs, may be affected. Skin lesions range from small papules resembling molluscum contagiosum to cold abscesses, draining sinuses, or ulcers. It is not clear if there is an asymptomatic form of African histoplasmosis as in classic histoplasmosis. The diagnosis is confirmed by culture and microscopy (direct microscopy or histopathology). The organisms of H. capsulatum var. duboisii are different from the smaller capsulatum forms. They are usually 10 to 15 µm in diameter, slightly pear-shaped, and clustered in giant cells. Histoplasma serology, using conventional tests, is often negative in African histoplasmosis.
CLINICAL COURSE AND PROGNOSIS
Prognosis depends on the site and type of infection. But the choice of therapy for histoplasmosis generally depends on the severity of the illness.
MANAGEMENT Medications: For patients with some disseminated or localized forms of the disease, oral itraconazole (200 to 400 mg daily) is highly effective. It also has been used for long-term suppressive treatment of the disease in AIDS patients after primary therapy
24
either with itraconazole or amphotericin B.31 However, there is now evidence that provided CD4 counts do not fall in patients on highly active antiretroviral therapy (HAART) therapy (see Chap. 173), suppressive treatment can be discontinued. In AIDS, some patients receiving treatment of histoplasmosis, an immune reconstitution syndrome has been reported after commencing HAART therapy with intestinal obstruction, uveitis, and arthralgia. Intravenous amphotericin B (up to 1 mg/kg daily) is given to patients with widespread and severe infections and is the main alternative used. Posaconazole and voriconazole are effective in some cases. In African histoplasmosis, itraconazole is also the treatment of choice, but once again, in severe cases amphotericin B may be used.30
BLASTOMYCOSIS (NORTH AMERICAN BLASTOMYCOSIS)
BLASTOMYCOSIS
(NORTH AMERICAN
BLASTOMYCOSIS)
Blastomycosis is a chronic mycosis caused by the dimorphic pathogen Blastomyces dermatitidis.32 Its chief sites of involvement are the lungs, but disseminated forms of the infection may affect skin, bones, CNS, and other sites.
EPIDEMIOLOGY
Blastomycosis is found in North America and Canada.33 Most cases, though, come from the Great Lakes region and southern states of the United States. It also occurs sporadically in Africa, with the largest numbers of cases coming from Zimbabwe,34 and cases also have been reported from the Middle East and India. It is thought that the natural habitat of Blastomyces is in some way related to wood debris and is close to rivers or lakes or in areas subjected to periodic flooding. However, it is difficult to isolate Blastomyces from the natural environment.35 Blastomycosis also may affect domestic animals such as dogs.
CLINICAL FEATURES
As with histoplasmosis, there is a subclinical form of the infection; its prevalence has not been defined in detail because of lack of a commercial Blastomyces skintest antigen and the extent of antigenic crossreactivity with fungi such as Histoplasma. Primary cutaneous blastomycosis is also very rare and follows trauma to the skin and the subsequent introduction of fungus, for instance, in laboratory workers or pathologists.36 After inoculation, an erythematous, indurated area with a chancre appears in 1 to 2 weeks with associated lymphangitis and lymphadenopathy. Pulmonary blastomycosis is very similar in clinical presentation to pulmonary tuberculosis.33,36,37 There may be no symptoms, or there may be low-grade fever, chest pain, cough, and hemoptysis, and unlike
2977
4
24
histoplasmosis, it often coexists with disseminated disease. Skin lesions are a common presenting feature of disseminated blastomycosis.36,38 They are often symmetric and usually affect the face and extremities. The early lesion is a papule or nodule, which may ulcerate and discharge pus. With time, this enlarges to form a hyperkeratotic lesion, often with central ulceration and/or scarring (Figs. 162-11 and 162-12). Oral lesions are less common. Multiple skin lesions are often found in disseminated infection. Other patients may present with nodules and abscesses, and in many patients lesions of different morphologies are present. African patients with blastomycosis have a higher frequency
2978
of skin and bone involvement.34 Although blastomycosis can affect almost any organ, other common sites for dissemination include the bone, the epididymis, and the adrenal gland. Less commonly, there is widespread rapid dissemination with multiple organ involvement, and B. dermatitidis can produce a form of adult respiratory distress syndrome. Skin lesions in widespread disseminated disease are usually papules, abscesses, or small ulcers. Widespread blastomycosis has been described in AIDS patients, but it is not common.39
DIAGNOSIS Laboratory Testing: The fungus can be found in KOH mounts of pus, skin scrapings, or sputum as thick-walled, rounded, refractile, spherical cells with broad-based buds (Fig. 162-13). In culture, the fungus grows as a mycelial fungus at room temperature. It produces small, rounded, or pear-shaped conidia. At higher temperature (37°C [98.6°F]) and on enriched media, it produces yeast forms with the characteristic buds. Molecular probes will confirm the identity. These are often found in giant cells or surrounded by neutrophils (Fig. 162-14). Precipitating antibodies to
B. dermatitidis are often present in the sera of infected patients, and a characteristic precipitin line, the E band, has been described in a high proportion of proven cases; there is also an enzyme-linked immunosorbent assay for blastomycosis. There is also an antigen detection system that is most accurate in urine samples.
Pathology: In tissue sections, the typical organisms with broad buds may be found, although it may be necessary to search several fields to find the characteristic cells.
DIFFERENTIAL DIAGNOSIS
The chronic skin granulomas must be differentiated from those caused by tuberculosis, other deep mycoses, nonmelanoma skin cancers, pyoderma gangrenosum, and drug reactions caused by bromides and iodides.
CLINICAL COURSE AND PROGNOSIS
As with histoplasmosis, the course depends on the site of infection and the presence of any underlying disease.
MANAGEMENT Medications: Treatment is similar to that used for histoplasmosis; itraconazole (200 to 400 mg daily) is used in the less-severe forms of the infection or when there is only localized spread. Voriconazole is also active against this infection. Treatment is usually given for at least 6 months. Followup surveillance is necessary because relapse can occur, particularly where there are deep sites of infection or the patient is immunosuppressed. Amphotericin B (up to 1 mg/kg daily) is generally used for the treatment of widespread disseminated forms of blastomycosis.
COCCIDIOIDOMYCOSIS (COCCIDIOIDAL GRANULOMA, VALLEY FEVER, SAN JOAQUIN VALLEY FEVER, DESERT RHEUMATISM)
COCCIDIOIDOMYCOSIS
(COCCIDIOIDAL
GRANULOMA, VALLEY
FEVER, SAN JOAQUIN
VALLEY FEVER, DESERT
RHEUMATISM)
DEFINITIONS
Coccidioidomycosis is the infection caused by the fungal species Coccidioides immitis and Coccidioides posadasii; C. posadasii is phenotypically identical to C. immitis and produces identical disease, but is mainly found outside California. Both show an unusual form of dimorphism, with a mold form at room temperature and the development of spherules, large spore-containing structures, in infected tissue. As with other endemic
24
mycoses, there are asymptomatic, acute and chronic pulmonary, and disseminated forms. The disease can affect otherwise healthy individuals or predisposed patients, including those with AIDS.
EPIDEMIOLOGY
C. immitis is endemic in some semidesert areas of South and Southwest of the United States, and C. posadasii elsewhere (Arizona, New Mexico, and Texas) and in parts of Mexico and Central and South America. The climate of the endemic areas is marked by very high summer temperatures and low annual rainfall, demonstrated by a characteristic vegetation with cacti and mesquite bushes. Skin tests with coccidioidin show that the incidence of exposure in endemic areas may be as high as 95%. The fungus is found in soil and can affect other animals as well as humans. Exposure may result from a brief visit to an endemic area, and local weather can determine exposure rates.40 For instance, dust storms may cause infection in large numbers of individuals. The usual route of infection is respiratory, although direct implantation into the skin can occur rarely.
CLINICAL FEATURES
As with other systemic mycoses, there is an asymptomatic or subclinical form of coccidioidomycosis that is common in endemic areas, judging by the percentages of skin test reactors to coccidioidin in the healthy population. The primary pulmonary form, which is the most common clinical type, presents as a chest infection with fever, cough, and chest pain. Complications such as pleural effusion may occur. Erythema multiforme or erythema nodosum,40 often accompanied by arthralgia or anterior uveitis, occurs from the third to the seventh week in approximately 10% to 15% of patients, and is more common in females. Sometimes an early, generalized, macular and erythematous rash is seen in some patients. The chronic pulmonary form of the disease presents with chronic cough and resembles tuberculosis. Skin lesions normally do not occur in this phase. In the rare primary skin infection,41 after inoculation, there is an indurated nodule that develops 1 to 3 weeks after local trauma. This is followed by regional lymphadenopathy. Disseminated coccidioidomycosis develops in fewer than 0.5% of infected individuals. It is mainly seen in patients from certain ethnic backgrounds (African Americans, Filipinos, and Mexicans),40 apparently independent of occupational exposure or socioeconomic class, in pregnant women, and in immunosuppressed patients, including those with AIDS.42,43 In disseminated disease, lesions may develop in the skin, subcutaneous tissues, bones, joints, and all organs. The skin lesions (Fig. 162-15) are papules, nodules, abscesses, granulomas, ulcers, or discharging sinuses in which there is underlying bone or joint disease. Some lesions appear as flat plaques with central atrophy. Meningitis is an important complication of dissemination and is usually
2979
4
24
not associated with signs of infection in other sites. In AIDS patients, persistent pneumonia, skin lesions, and widespread dissemination can all occur.
DIAGNOSIS Laboratory Testing: A characteristic of the laboratory findings is the ability of Coccidioides to form spore-containing spherules. These are large (up to 250 µm in diameter) and can be seen in KOH mounts of sputum, cerebrospinal fluid, or pus. In culture, colonies of Coccidioides are mycelial, fast growing, white, and cottony. On microscopy, there are chains of arthrospores at intervals on the older mycelium. Coccidioides in the mold phase is highly infectious, and cultures should be handled carefully. There is, as yet, no commercial molecular test for coccidioidomycosis. A variety of serologic tests are of value in the diagnosis and prognosis of coccidioidomycosis.44 Precipitins develop in approximately 90% of infected individuals within 2 to 6 weeks but are short-lived; complementfixing antibodies are characteristic of more-severe infections and, in active infection, increase to a maximum after 6 months. Skin tests with coccidioidin are of little value in diagnosing infections. Spherulin is an antigen obtained from spherules of C. immitis and may be better than coccidioidin for detecting sensitization. However, in severe infections, cutaneous anergy to both is common.
Pathology: Spherules containing large endospores can be seen in tissue sections, although there are a variety of less-distinct intermediate stages in spherule formation that also can be seen. Before endospores form, the cytoplasm of the immature spherule is basophilic and subsequently breaks up into spores. Mycelium is seen rarely in histopathologic sections.
2980
DIFFERENTIAL DIAGNOSIS
Physicians in endemic areas should be aware of the connection between erythema nodosum and coccidioidomycosis. It also may occur in visitors to endemic areas after only a short stay.
CLINICAL COURSE AND PROGNOSIS
As with histoplasmosis, the course depends on the site of infection and the presence of any underlying disease.
MANAGEMENT Medications: No specific therapy apart from rest is necessary in the primary pulmonary infection, and there is little evidence that the symptoms are either improved or shortened by giving an oral azole drug, even though it is widespread practice. For disseminated disease, the results of treatment are still variably, but amphotericin B (1 mg/kg daily), itraconazole (200 to 400 mg daily), or fluconazole (200 to 600 mg daily) can all be given.45 Experience with the newer antifungal agents, such as voriconazole and posaconazole, is limited at present. It is important to follow patients carefully, given the frequency of relapse. Meningitis and progressive disseminated infection involving multiple sites are all particularly refractory to therapy. Generally, soft-tissue coccidioidomycosis (skin and joint) has a better prognosis, and the mortality in patients who present with such lesions is low.
Prevention: A vaccine, Spherulin, for coccidioidomycosis has been studied, but the results were inconclusive and at present there is no immunization against this infection.45
PARACOCCIDIOIDOMYCOSIS (SOUTH AMERICAN BLASTOMYCOSIS, PARACOCCIDIOIDAL GRANULOMA)
PARACOCCIDIOIDOMYCOSIS
(SOUTH AMERICAN
BLASTOMYCOSIS,
PARACOCCIDIOIDAL
GRANULOMA)
DEFINITIONS
Paracoccidioides brasiliensis is a dimorphic fungus that causes a respiratory tract infection with a tendency to disseminate to the mucous membranes and lymph nodes. It is confined to Central and South America.46
EPIDEMIOLOGY
Paracoccidioidomycosis has been reported from most Latin American countries, but the infection is found most commonly in parts of Brazil, Colombia, and Argentina. The infection does not occur in the United States, although it has been reported in
Mexico. Exposure rates can be estimated by skin test reactivity and appear to be equal in both males and females, although the prevalence of positive reactors in endemic areas seldom exceeds 25%; work with a skin test derived from purified glycoprotein 43 antigen generally demonstrates that exposure rates are higher than previously believed. The active infection is seen predominantly in males. The mechanism is thought to be connected to the presence of a cytoplasmic estrogen receptor on the fungus, and, in vitro, estradiol suppresses the conversion of mycelium to yeast.47 The ecologic niche of the organisms is unknown, but the condition is much more frequent in rural areas; exposure is associated with proximity to water or areas of high atmospheric humidity.48
CLINICAL FEATURES
There are a number of different clinical patterns of paracoccidioidomycosis infection that depend on the predominant site of clinical involvement. These include the lung (pulmonary form), the mucous membranes (mucocutaneous form), and the lymph nodes (lymphatic form). Many patients have a mixed type of infection with involvement of different organ groups.46
Patients rarely present with an acute form of pulmonary infection, although this has been observed rarely and reported to subside while dissemination occurs. More usually, pulmonary infection tends to be chronic and slowly progressive with weight loss and chronic cough. The lesions may be bilateral and nodular on chest radiography, and there is often extensive fibrosis. Other sites of involvement include mucocutaneous areas. Oral or circumoral lesions are common in the mucocutaneous forms of paracoccidioidomycosis; lesions also occur in the nose, conjunctivae, or around the anus. These lesions may be small granulomas or ulcers. They heal with scarring, which may cause considerable deformity. The cervical lymph nodes are sometimes enlarged, tender, and tethered to the overlying skin; they rarely suppurate. Other systemic sites of involvement include the spleen, intestines, lungs, and liver. Paracoccidioidomycosis is uncommon in AIDS patients, although there is a widespread variety that is a more rapidly progressive form of disseminated infection occurring in young adults or older children without recognizable predisposition.49
DIAGNOSIS Laboratory Testing: Sputum, exudates, and scrapings can be screened using KOH. They show numbers of round yeasts with a characteristic form of multiple budding in which a parent cell is surrounded by large numbers of smaller buds. The organism is dimorphic and produces a cottony mycelial-phase growth on primary isolation at room temperature. Once again, the characteristic yeast phase can be
24
induced on enriched media such as brain–heart infusion agar at 37°C (98.6°F). Serology is very helpful in confirming the diagnosis, the main tests being the immunodiffusion assay and a complement-fixation test. Antibodies to pb27 and 87-kDa antigens have been found to be highly specific for this infection in immunoblotting. There are also antigen-detection tests useful for monitoring patients with disseminated disease.
Pathology: Histopathologically, there is a mixed granulomatous response with fibrosis. The organisms can be seen with special fungal stains such as methenamine silver (Grocott modification). In tissue, the characteristic budding pattern can be seen, although it may be necessary to search several fields to find the most typical structures (Fig. 162-16). In widespread infections, masses of small yeast forms may be mistaken for Histoplasma.
DIFFERENTIAL DIAGNOSIS
Differential diagnosis includes tuberculosis, leishmaniasis, and other deep mycoses.
CLINICAL COURSE AND PROGNOSIS
As with histoplasmosis, the course depends on the site of infection and the presence of any underlying disease.
MANAGEMENT Medications: The treatment of choice in most cases is itraconazole, which can produce remissions in 3 to 6 months.50 Voriconazole produces similar responses. Relapses can occur, and, where possible, patients should be reviewed periodically after primary therapy. In very extensive infections and in severely ill patients, such as those with the progressive disseminated type of infection, intravenous amphotericin B may be necessary. Severe pulmonary or intraoral fibrosis may remain after treatment.
2981
4
24
INFECTIONS CAUSED BY TALAROMYCES MARNEFFEI (PENICILLIOSIS, PENICILLIOSIS MARNEFFEI)
INFECTIONS CAUSED
BY
TALAROMYCES
MARNEFFEI
(PENICILLIOSIS,
I
I
PENICILLIOSIS MARNEFFEI)
DEFINITIONS
T. marneffei infection is a more recently recognized disease found in Southeast Asia. T. marneffei was originally thought to be a member of the common genus Penicillium.51 It shows an unusual pattern of dimorphism in that it develops yeast-like cells that reproduce with septal formation, dividing the cells into two. It is inhaled via the lungs, and it is not known whether there is a primary cutaneous form of the infection.
EPIDEMIOLOGY
The natural source of T. marneffei is unknown. Infections are confined to Southeast Asia, particularly Thailand, South China, and Vietnam. However, there are reports in other Asian countries, including Northeast India, and imported cases are seen in Europe and the United States. Natural infections are known to occur in bamboo rats of the genus Cannomys, which are large burrowing rodents. The infection affects otherwise healthy individuals as well as those with immune defects and is most common after the rainy season.52 Patients with AIDS, as well as those receiving rituximab biologic therapy, appear to be particularly susceptible to this infection.
CLINICAL FEATURES
There has been no work to demonstrate that there is a subclinical form of Talaromyces infection, even though this is likely. Patients usually present with localized pulmonary or disseminated disease. The chest signs are those of chronic pulmonary disease.53,54 More than 50% of AIDS patients with this infection have multiple skin lesions, which are umbilicated papules that may enlarge and ulcerate. They are usually widely scattered on the face and trunk. Other organs, including the liver, GI tract, spleen, and bone marrow, may be affected.
DIAGNOSIS Laboratory Testing: T. marneffei forms characteristic yeast-like cells that are divided by a septum in tissue and are best seen in histopathologic sections stained with methenamine silver. These cells are small (2 to 4 µm in diameter) and difficult to see in blood films or skin or bone marrow smears, but they may be highlighted with stains such as leishmanin. In culture, T. marneffei is a green or grayish mold that produces typical conidiophores and a diffusible red
2982
pigment. There is no commercial serologic test as yet, although both antigen detection systems and PCR have been used in diagnosis, the PCR for identification of cultures.
DIFFERENTIAL DIAGNOSIS
The main differential diagnosis is with other disseminated mycoses, such as histoplasmosis and cryptococcosis, which also can be found in the endemic area in AIDS patients. Biopsy and, when necessary, culture will distinguish between the different causes.
CLINICAL COURSE AND PROGNOSIS
As with histoplasmosis, the course depends on the site of infection and the presence of any underlying disease.
MANAGEMENT Medications: In severe cases, amphotericin B is necessary. In many cases, however, there is a good response to itraconazole (200 to 400 mg daily). In AIDS patients, this is continued after initial therapy to prevent relapse.54
CRYPTOCOCCOSIS
CRYPTOCOCCOSIS
DEFINITIONS
Cryptococcosis is the infection caused by the encapsulated yeasts Cryptococcus neoformans and Cryptococcus gattii. Although the main portal of entry is through inhalation into the lungs, the disease usually presents with signs of extrapulmonary dissemination such as meningitis. Cutaneous lesions can develop as a result of dissemination or, rarely, through inoculation. It is associated with HIV infection.55
EPIDEMIOLOGY
Cryptococcosis has a worldwide distribution although exposure rates probably differ markedly in different countries. C. neoformans has 2 variants: (a) C. neoformans var. neoformans and (b) C. neoformans var. grubii. These correspond to 3 clusters of serotypes: (a) D, (b) A, and (c) B or C.56 The neoformans and grubii varieties can be isolated from pigeon excreta and are more common in AIDS patients; the gattii form is found in the debris of certain eucalyptus trees in Australia, and California as well as some tropical areas, but it is less often isolated from AIDS patients. Two sexual varieties called Filobasidiella neoformans and Filobasidiella bacillispora correspond to the neoformans/grubii and gattii species, respectively. Clinically the main differences to be seen are those between the neoformans and gattii species, for example, a higher prevalence of
symptomatic pulmonary disease with the gattii species. Patients with certain immunodeficiency states caused by AIDS, malignant lymphomas, sarcoidosis, collagen disease, carcinoma, and those receiving systemic glucocorticoid therapy are particularly susceptible. The incidence of cryptococcosis in patients with established untreated AIDS varied in different countries, from 3% to 6% in the United States, to 3% in the United Kingdom, to more than 12% in parts of Africa (eg, Democratic Republic of the Congo). However, with the widespread use of HAART therapy the incidence has declined. Strains of serotype D are more likely to be found in skin lesions, which occur in 10% to 15% of cases of disseminated cryptococcosis.
CLINICAL FEATURES
The advent of the AIDS epidemic affected the epidemiology of cryptococcosis considerably, and in areas such as northern Thailand, it is one of the main secondary complications of HIV infection.55 There is probably a subclinical form of cryptococcosis because unaffected individuals may have positive skin tests. However, the most common clinical manifestation of disease is meningoencephalitis. This presents with classic signs of meningitis, changes in consciousness, mental changes, and nerve palsies. In AIDS patients, these signs may be only weakly expressed. Pulmonary infection can be found in approximately 10% of those with meningitis. Chest signs include the appearance of nodular shadows, cavitation, and pleural effusion. Patients with AIDS often present with fever and mild headache, and few other features of infection.55 Cutaneous lesions may develop in approximately 10% of cases, but are seldom pathognomonic.57-60 Acneiform papules or pustules progressing to warty or vegetating, crusted plaques, ulcers, and hard infiltrated plaques or nodules are characteristic of widespread systemic infection (Fig. 162-17). Cold abscesses, cellulitis, and nodular lesions also occur. In otherwise healthy patients and in those with sarcoidosis, lesions may be solitary, and in such patients, they may be the only clinical manifestation of infection. In primary cutaneous cryptococcosis with direct inoculation of organisms into the skin, the skin lesions are usually solitary nodules that break down and ulcerate. Local lymphadenopathy also develops. The term primary cutaneous cryptococcosis is also used loosely to describe solitary lesions of cryptococcosis, but in many such cases there is also evidence of dissemination to other internal organs. It is important to investigate all patients who present with cutaneous lesions for evidence of dissemination to other sites.58
DIAGNOSIS Laboratory Testing: Cryptococci are large (5 to 15 µm in diameter), budding cells with capsules that are best observed by direct microscopy of India ink or Nigrosin mounts (Fig. 162-18). The organism is not
24
difficult to grow in culture. Various biochemical features, such as the production of urease and the ability to pigment on Guizotia seed medium, are characteristic; molecular probes can be used to confirm the identity. Serologic tests are rapid and specific. The main test is an antigen-detection assay using latex agglutination or enzyme-linked immunosorbent assay, and this is simple and very rapid to perform on blood or cerebrospinal fluid. Very high titers are found in serum and cerebrospinal fluid from AIDS patients. Non-AIDS patients with single, localized skin lesions are often antigen negative.
Pathology: In tissue sections, the large pleomorphic yeasts stimulate either a granulomatous reaction
2983
4
24
or very little inflammation. The capsules of the cells can be stained using the mucicarmine or Alcian blue stains.
DIFFERENTIAL DIAGNOSIS
Cryptococcal skin lesions may mimic a range of other conditions, particularly other systemic mycoses in AIDS patients. It is important to biopsy and culture suspicious lesions in immunocompromised patients.
MANAGEMENT Medications: The most frequently used drug regimen in the non-AIDS patient is IV amphotericin B combined with flucytosine. In patients with single skin lesions and no other signs of infection, alternatives such as fluconazole or itraconazole can be used. Because there is a very high relapse rate in AIDS patients, the usual policy is to give a 10- to 14-day course of amphotericin B with or without flucytosine, followed by long-term fluconazole.61 However, it is possible to stop long-term suppressive therapy in patients receiving HAART. High-dose fluconazole given on its own is an alternative approach.
CUTANEOUS ASPECTS OF SYSTEMIC OPPORTUNISTIC MYCOSES
CUTANEOUS ASPECTS OF
SYSTEMIC OPPORTUNISTIC
MYCOSES
Skin lesions are not common with the opportunistic fungal infections, but they can occur in some patients, particularly in certain predisposed groups. When they occur, their presence may be very helpful because it is possible to biopsy easily accessible lesions to establish the diagnosis.
SYSTEMIC CANDIDIASIS
SYSTEMIC CANDIDIASIS
Systemic candidiasis follows dissemination of Candida sp. from the GI tract or via the bloodstream. Skin lesions can occur, especially in 2 situations: (a) in neutropenic patients, there is often a severe disseminated disease with widespread skin nodules and associated muscle pains,62 and (b) in IV drug abusers, candidiasis may present with a follicular, pustular rash in the beard area and scalp. Other lesions include retinal and vitreal deposits and abscesses around the costochondral junctions. Systemic candidiasis is usually treated with IV amphotericin B (conventional or lipid-associated), caspofungin, or fluconazole. Resistance to some azole drugs, such as fluconazole and ketoconazole, is more common with certain non-albicans Candida sp., and these antifungal agents should be avoided in infections caused by these species. Newly recognized species, such as Candida auris, have been found to cause
2984
systemic infection resistant to common therapeutic drugs such as fluconazole and amphotericin B.63
MUCORMYCOSIS (PHYCOMYCOSIS, ZYGOMYCOSIS)
MUCORMYCOSIS
(PHYCOMYCOSIS,
ZYGOMYCOSIS)
Mucormycosis is a rare disease caused by Mucoromycetes fungi such as Mucor, Lichtheimia, and Rhizopus. Cunninghamella bertholletiae and Saksenaea vasiformis are less-common causes. These fungi cause disease in patients with poorly controlled diabetes, neutropenia, or renal disease. Direct invasion through abrasions has been reported following trauma from a natural disaster (eg, during a mudslide or tsunami).64 They can invade necrotic burned areas or involve the facial skin secondary to invasive infection of the paranasal sinuses (Fig. 162-19). Mucormycosis also has been caused by close apposition of the skin with contaminated dressing materials in the case of Rhizopus rhizopodiformis65 or with wooden tongue depressors in the case of Rhizopus microsporus.66 These fungi have a tendency to invade blood vessels, causing widespread infarction. Infections may respond to IV amphotericin, and recent results with lipid-associated amphotericin B formulations have been encouraging.
OTHER OPPORTUNISTIC MYCOSES
OTHER OPPORTUNISTIC
MYCOSES
Other fungi causing systemic infections also may produce skin lesions in the process of bloodstream dissemination. The best known of these organisms are Aspergillus, Scedosporium, Trichosporon, and Fusarium. Skin infection is seen mainly in severely immunocompromised patients such as those with neutropenia. Aspergillus may produce large necrotic lesions such as ecthyma gangrenosum, but smaller papules and cold abscesses also can occur.67 Fusarium infections may produce widely distributed target-like lesions that may undergo central necrosis and, in some cases, digital cellulitis and superficial white onychomycosis precede dissemination.68 Treatment for all these infections is usually amphotericin B, although voriconazole is increasingly used with aspergillosis.
DIAGNOSIS Laboratory Testing: Laboratory confirmation of the diagnosis is fraught with difficulties chiefly because many of the organisms are also commensals in human sites; because they occur in severely ill patients, the capacity to produce diagnostic antibody titers is compromised. The interpretation of laboratory data is consequently difficult and has to be related to the
A
B
C
24
clinical state of the patient. Newer tests for aspergillosis and candidiasis, such as detection of galactomannan (aspergillosis) or PCR-based molecular assays, are proving helpful in some cases.
Pathology: Ideally, a histologic diagnosis should be made, although biopsy may be impossible because of the risk of bleeding.
MANAGEMENT
In many cases, the diagnosis of a systemic mycosis is presumptive, and treatment is given empirically.
ACTINOMYCOSIS AND NOCARDIOSIS
ACTINOMYCOSIS AND
NOCARDIOSIS
Actinomycosis is an infection caused by filamentous bacteria that form large granules (sulfur granules) in abscess cavities. Draining sinuses communicate from the center of the abscess to the skin or mucosal surface. Nocardiosis is an acute and chronic infection also caused by filamentous bacteria. These lead to localized skin, subcutaneous, and systemic infections. Actinomycosis and nocardiosis are discussed in detail in Chap. 158.

Figure 162-1 Sporotrichosis. An ulcerated nodule is seen on the thumb, with proximal lymphangitic spread represented by subcutaneous nodules. (Used with permission from Takeji Nishikawa, MD.)

Figure 162-2 Mycetoma. Brawny edema and crusted papules on the plantar surface.

Figure 162-3 Eumycetoma caused by Scedosporium leading to significant distortion of the forefoot.

Figure 162-4 Mycetoma. Chronic fibrotic involvement of the foot with lymphatic spread to the popliteal fossa.
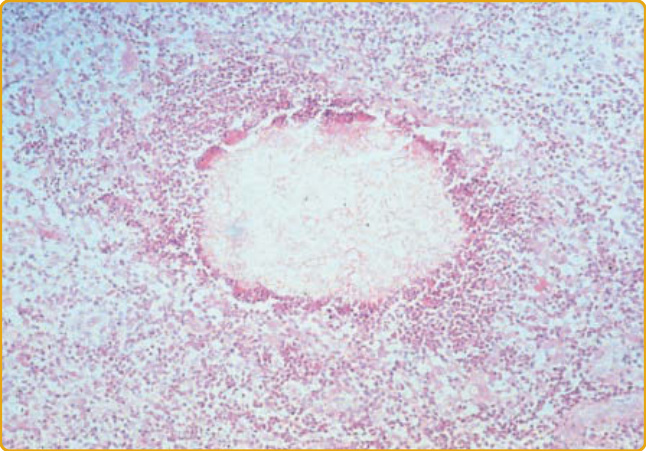
Figure 162-5 Pale eumycetoma grain (hematoxylin-andeosin stain).

Figure 162-6 Chromoblastomycosis. A solitary, large, verrucous plaque surrounded by a halo of erythema is seen on the calf. (Used with permission from Ted Rosen, MD, and Howard Rubin, MD.)

Figure 162-7 Closeup view of chromoblastomycosis. Note hyperkeratosis with pigmentation.
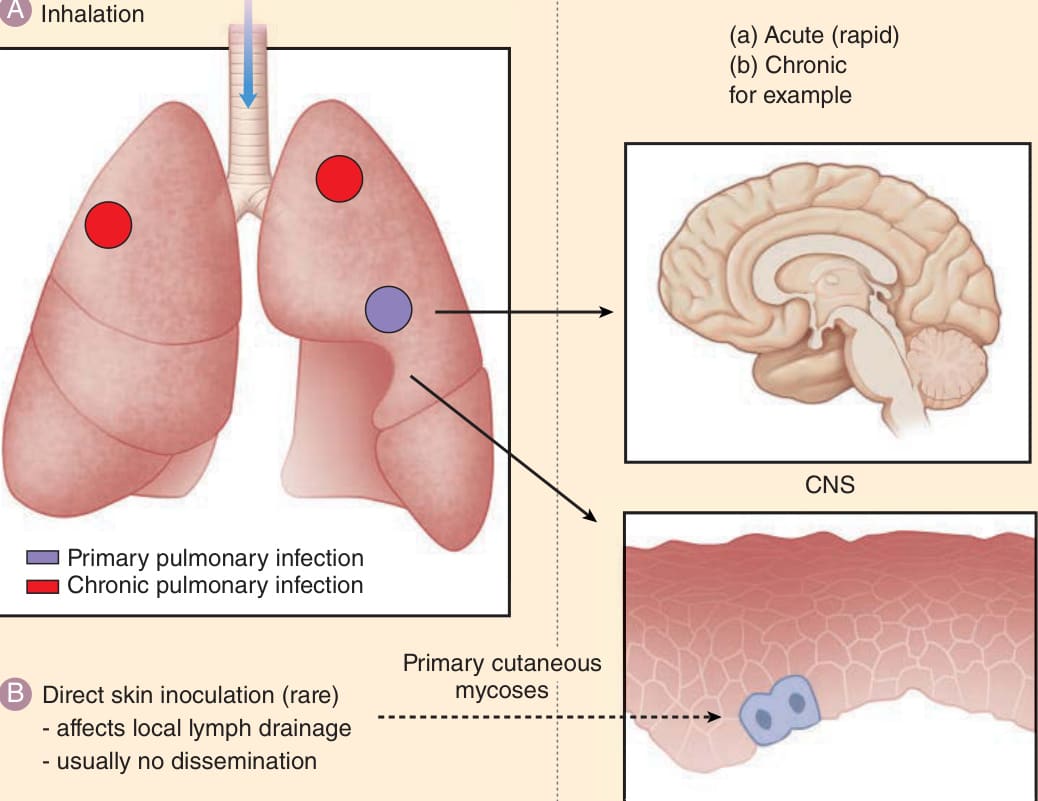
Figure 162-8 The route of infection and dissemination to the skin of the endemic (respiratory) mycoses.

Figure 162-9 Histoplasmosis, disseminated. Multiple erythematous keratotic papules and small plaques resembling guttate pattern psoriasis are seen on the chest and arm of a man with advanced HIV disease. (Used with permission from J. D. Fallon, MD.)
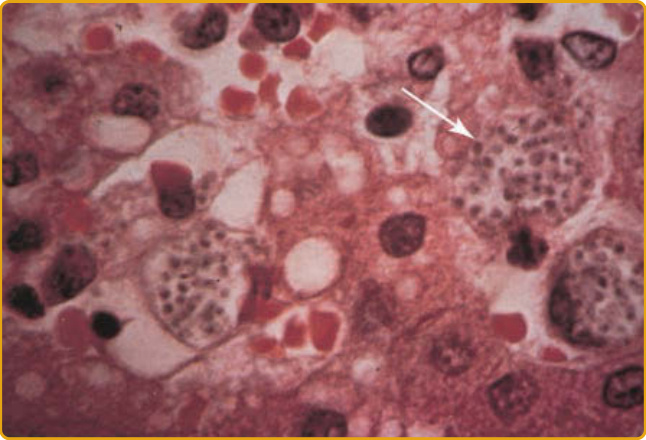
Figure 162-10 Histoplasmosis, disseminated. Lesional biopsy specimen shows dermal macrophages packed with dozens of tiny yeast forms of Histoplasma capsulatum (arrow).

Figure 162-11 Blastomycosis. Inflammatory plaque with ulceration resembling pyoderma gangrenosum on the calf. (Used with permission from Elizabeth M. Spiers, MD.)
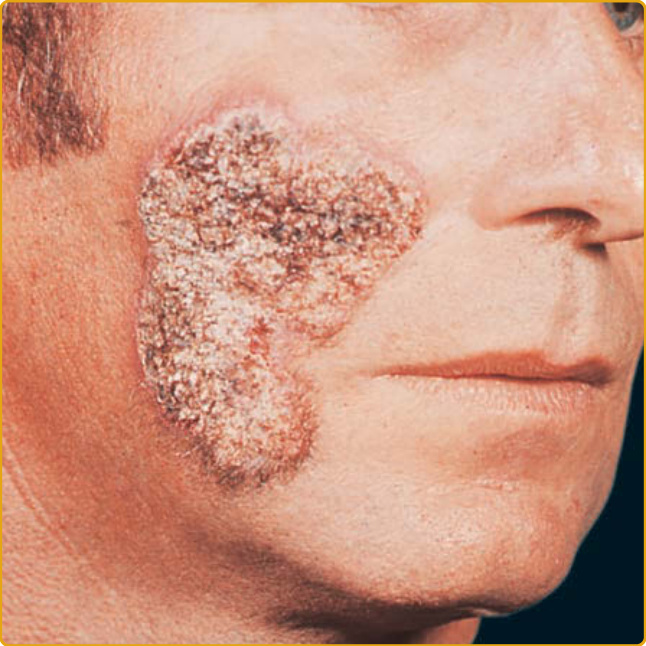
Figure 162-12 Blastomycosis. Chronic verrucous plaque on the cheek.
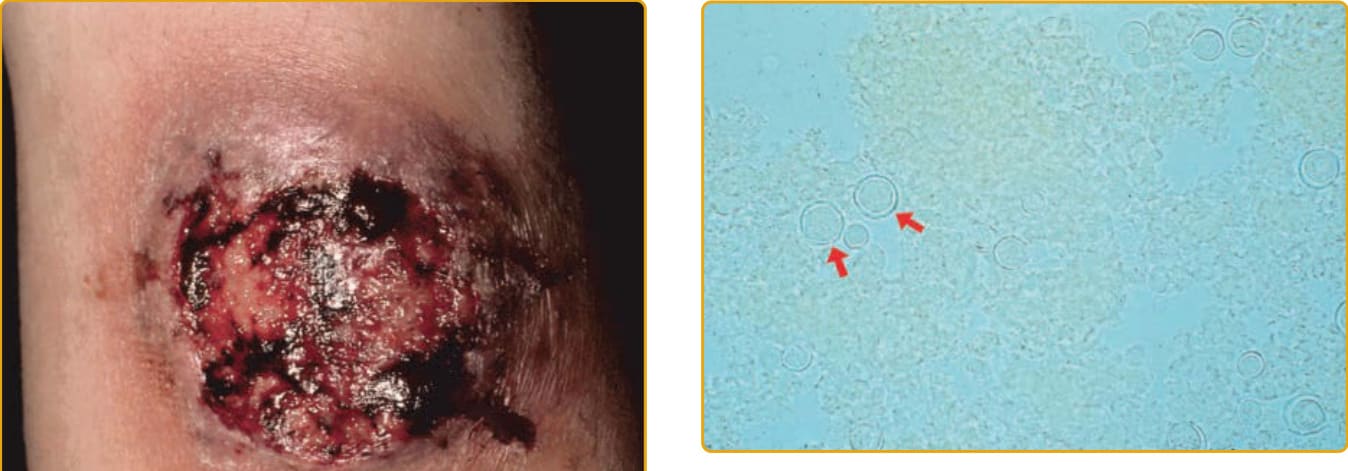
Figure 162-13 Direct preparation (potassium hydroxide) of Blastomyces (arrows).
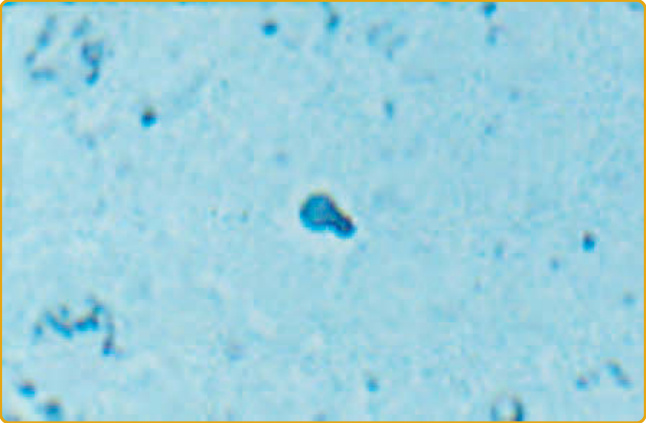
Figure 162-14 Blastomycosis. Lesional biopsy specimen shows a budding yeast form (Gomori methenamine silver stain).

Figure 162-15 Coccidioidomycosis, disseminated. Two intact and ulcerated papules/nodules are seen on the cheek and nose of this comatose patient with coccidioidomycotic meningitis. (Used with permission from Francis Renna, MD.)
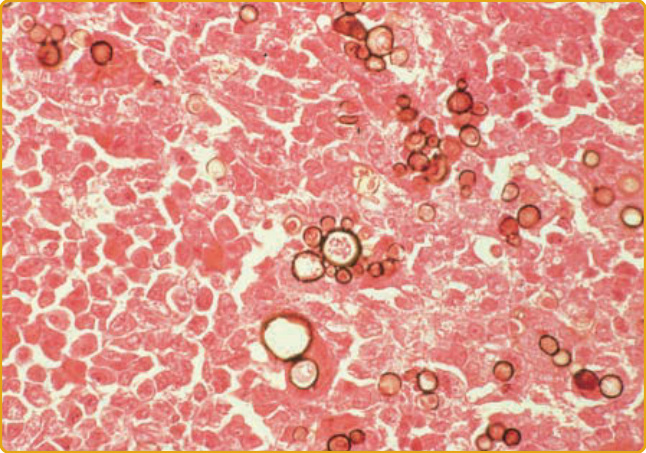
Figure 162-16 Biopsy of oral mucosal lesion showing multiple budding Paracoccidioides brasiliensis.
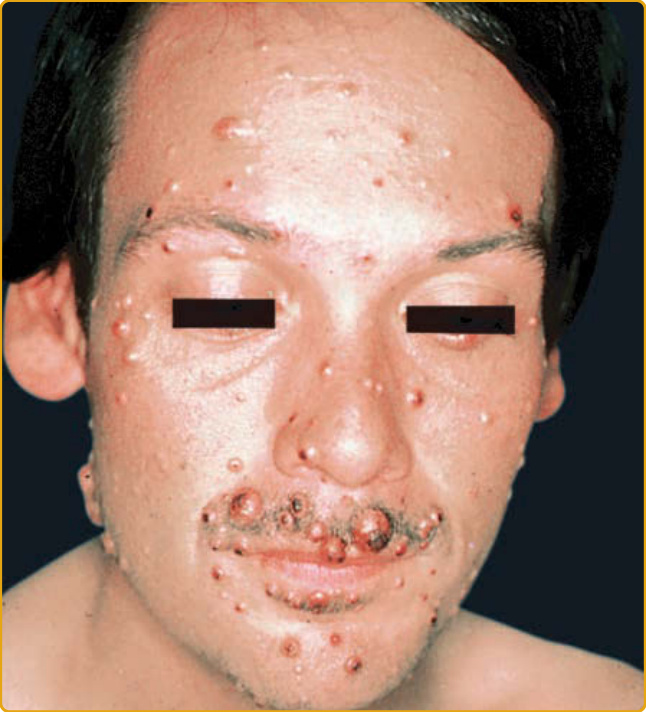
Figure 162-17 Cryptococcosis, disseminated. Multiple, discrete, skin-colored papules, and nodules resembling molluscum contagiosum are seen on the face of a male with advanced HIV disease. (Used with permission from Loïc Vaillant, MD.)
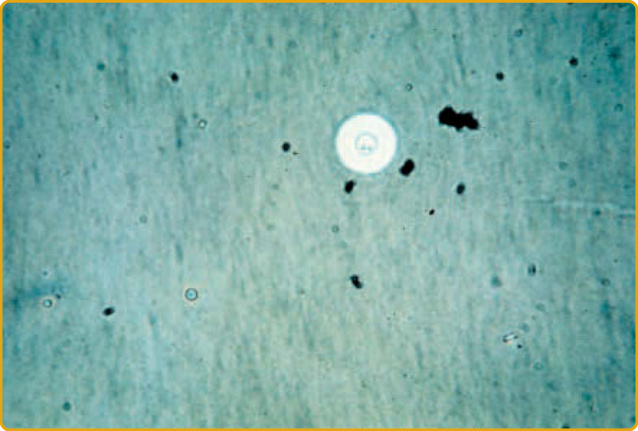
Figure 162-18 Cryptococcosis. India ink preparation of cerebrospinal fluid.

Figure 162-19 Mucormycosis. A, The face of this young woman with diabetes mellitus shows proptosis, unilateral facial edema, and a right-sided facial palsy associated with infection beginning in the right maxillary sinus. B, Ulcer. C, Hyphae in tissue.
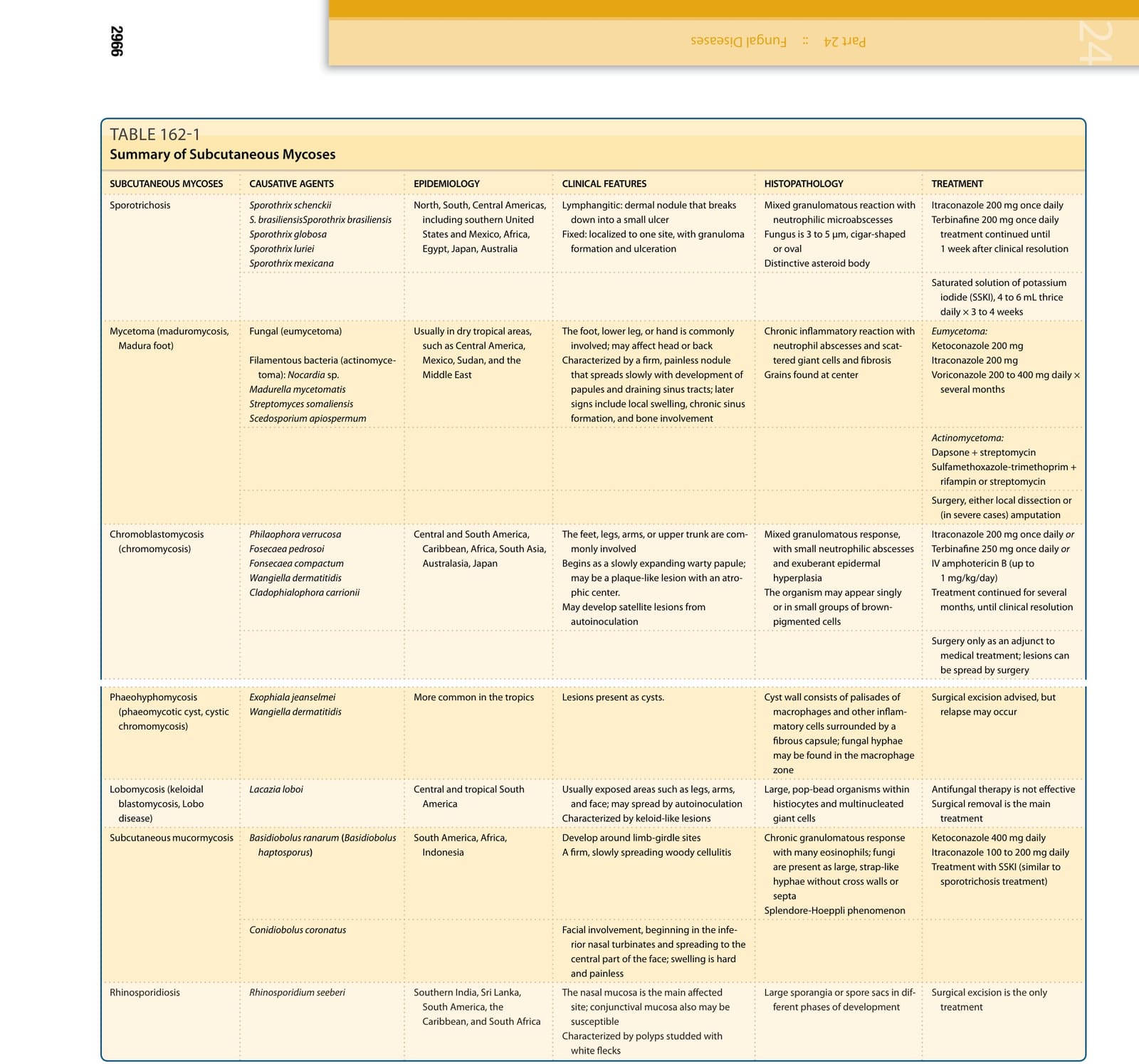
TABLE 162-1
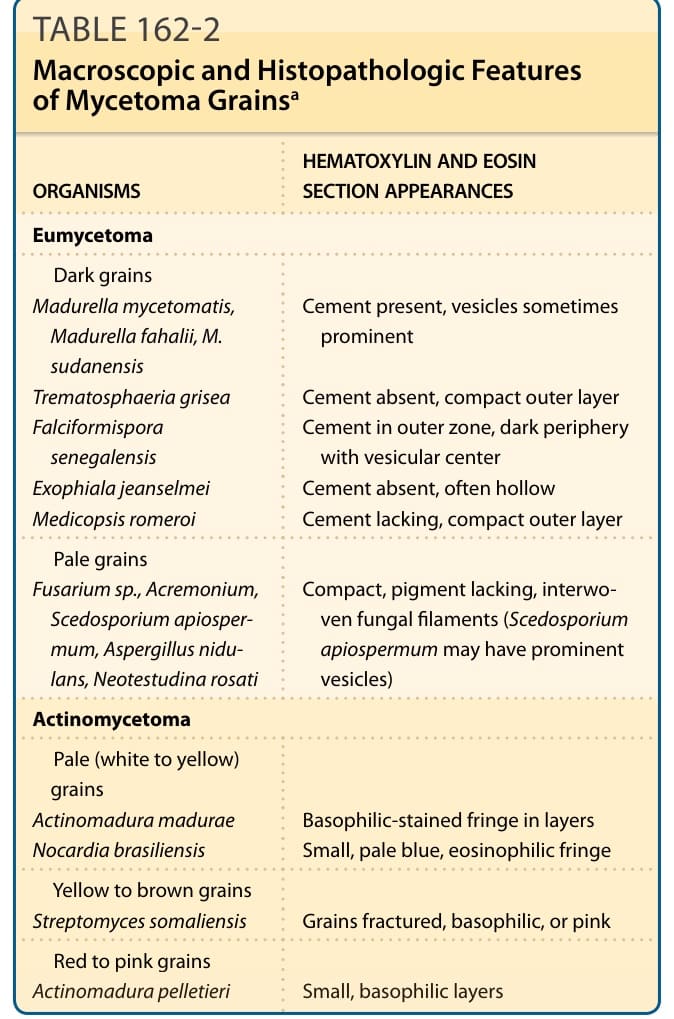
TABLE 162-2 Macroscopic and Histopathologic Features of Mycetoma Grainsa
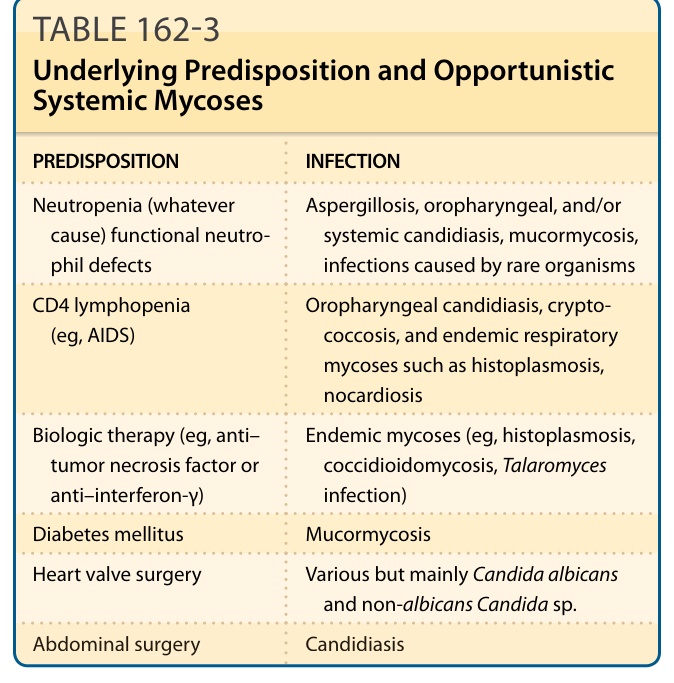
TABLE 162-3 Underlying Predisposition and Opportunistic Systemic Mycoses