Yeast Infections
4
24
This chapter reviews the spectrum of cutaneous yeast infections caused by Candida and Malassezia yeasts, both of which are frequent commensal organisms on human hosts. Candida behaves as an opportunistic pathogen, producing fairly characteristic patterns of inflammatory skin, mucosal, and nail infection, with the potential to produce invasive and sometimes lifethreatening disseminated disease. Malassezia, by contrast, produces several superficial cutaneous patterns is rarely a culprit in systemic disease.
CANDIDIASIS
AT-A-GLANCE
■ Candida species produce a variety of inflammatory mucosal and cutaneous manifestations.
■ Favored areas of involvement include the oral mucosa and lips, fingers and nails, intertriginous zones, and genitalia.
■ A variety of conditions can predispose patients to chronic mucocutaneous candidiasis with diffuse skin, mucosal, and nail involvement.
■ Candida can cause invasive disease, including bloodstream infection, and is the most common culprit in fatal fungal sepsis.
■ Risk factors for infection include extremes of age, malnutrition, obesity, diabetes, and immune deficiency.
■ In mucocutaneous disease, morphology can be very helpful in making a clinical diagnosis, although confirmatory testing with potassium hydroxide preparations, culture, and histopathology (and in invasive disease, serology and polymerase chain reaction) also may be helpful.
■ Treatment includes topical imidazoles and nystatin, and in more-severe disease, systemic agents, including oral azoles and echinocandins.
EPIDEMIOLOGY
EPIDEMIOLOGY
Candida yeasts are found throughout the environment and are also common commensals of the human skin, oropharyngeal, respiratory, GI, and genital mucosa. Candidal colonization has been reported in the oral mucosa of more than 40% of healthy adults, with higher rates of carriage in women and smokers.1 At least 15 of the more than 200 Candida species have been implicated
in human disease. Although Candida albicans is the most commonly implicated Candida species in localized mucocutaneous candidiasis, an increasing number of other species have been implicated in mucocutaneous disease, including Candida glabrata, Candida tropicalis, Candida krusei, Candida parapsilosis, and Candida dubliniensis. Additionally, while albicans is still the single most common species, non-albicans species collectively now account for the majority of invasive candidiasis and candidemia.2 Other specific risk factors for infection are described below (see section “Risk Factors”).
CLINICAL FEATURES
CLINICAL FEATURES
CUTANEOUS FINDINGS
Localized Candida infection in the skin classically presents as beefy-red patches and plaques with satellite papules and pustules at the periphery (Fig. 161-1). Intertriginous areas, particularly the axillae, inframammary folds, groin folds, and infrapannus area, are frequently affected, and maceration may be an additional feature in these sites (Fig. 161-2A, B). Candida also may be implicated in miliaria arising on occluded skin surfaces, manifesting as small monomorphous vesicles (Fig. 161-3). On oropharyngeal mucosal surfaces, background erythema with adherent whitish material may be seen, as in the pseudomembranous form of oropharyngeal candidiasis (thrush) (Fig. 161-4A, D), however an erythematous form, characterized by a shiny depapillated lingual surface, as in median rhomboid glossitis, also occurs, and may be seen in those who wear dentures (Fig. 161-4B). Additionally, fissuring and crusting at the oral commissures may be seen in angular cheilitis (also known as perleche; Fig. 161-4C). In breastfeeding women, nipple candidiasis may present with shiny erythema of the areola and nipple, which may be associated with flaking of the skin, and thrush may concurrently be apparent in the infant’s mouth.3 On genital skin and mucosa, including the vulva, glans penis, and prepuce, Candida may present with patchy erythema or erythematous plaques with associated itching and burning sensation. In patients with vulvovaginitis, a thick, white, curdlike discharge is typical. Pustules are seen more frequently in balanitis and balanoposthitis than in vulvitis (Fig. 161-5). In the diaper area, the classic presentation is beefy-red erythematous plaques with satellite papules and pustules (Fig. 161-2C). In the interdigital spaces, particularly the third webspace of the hands, a macerated whitish plaque on erythematous background (erosio interdigitalis blastomycetica) may be seen, especially in patients with chronic exposure to moisture from wet work (Fig. 161-2D).
A B
C D
24
2953
4
24
A B
C D
2954
Candida also has been implicated in chronic paronychia, which presents with erythema of the proximal nailfold area with loss of the cuticle and skin breakdown (sometimes with associated onycholysis and nail dystrophy; Fig. 161-6A). More recently, however, the Candida has been hypothesized to play a secondary role as a colonizer with either chronic wet work leading to skin barrier breakdown or chronic contact dermatitis being the primary insult.4 Candida, usually starting as paronychia, can also directly invade the nail plate and produce onychomycosis (5% to 10% of onychomycosis overall is caused by Candida; Fig. 161-6B), and is implicated in several presentations, including a distal subungual presentation and total dystrophic onychomycosis.5,6 Candida onychomycosis is more often seen in the fingernails than in the toenails, and is often associated with pain on pressure or movement of the nail plate (both of these features are in contrast to dermatophytes), and more often affects the dominant hand.6 Exposure to moisture and occupational wet work are important risk factors. Patients with chronic mucocutaneous candidiasis may present with erythematous plaques with overlying scale reminiscent of plaque psoriasis (Fig. 161-7).
A B
24
In patients with candidemia, the presence of skin lesions, most typically discrete sparse lesions ranging from erythematous papules with central pallor or necrosis to erythematous nodules to (less commonly) plaques, may be an important clue to the diagnosis (Fig. 161-8).7 The distribution favors the trunk and proximal extremities although the head and face may be involved. These classic skin lesions are reported to appear approximately 10% to 30% of the time in candidemia, and are most commonly seen in C. tropicalis infection.8
NONCUTANEOUS FINDINGS
In patients with candidemia, the classic clinical triad of fever, rash, and myalgia has been described as a
sufficient basis for initiation of empiric treatment for presumptive invasive candidiasis in a hospitalized patient.9 The myalgia is the result of hematogenous dissemination of Candida to muscle (usually in the lower extremities) causing muscle abscesses, clinically presenting with a warm, sore muscle and seen in up to 25% of patients with candidemia.10 Additionally, chorioretinitis, vitreitis, and endophthalmitis may
2955
4
24
result from hematogenous spread in roughly 4% to 7% of patients with candidemia.11,12 Although a majority of patients do complain of symptoms that include visual changes (if able to articulate symptoms), ocular Candida is also detected in asymptomatic patients.11
COMPLICATIONS
Candida may cause multiorgan failure as a manifestation of septic shock, or may hematogenously disseminate to any organ in the setting of candidemia, with the liver, spleen, kidneys, heart (and heart valves), and meninges among the more common. Retinal involvement may be painless and result in permanent visual loss.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Although typically a commensal organism, Candida does act as an opportunistic pathogen under favorable circumstances, including alteration in normal flora or immune function, a breach of skin, or a breach of mucosal integrity. A variety of virulence factors assist it in establishing infection, including, importantly, the ability to adhere to human epithelial cells.13
Candida infection elicits both innate and adaptive host immune responses largely through the interleukin-17 (IL-17) pathway, and defects in this pathway, including in genes such as STAT1, STAT3, IL17F, IL17RA, among many others, are associated with susceptibility to chronic mucocutaneous candidiasis.14,15 Recent research also has identified that mutations in caspase recruitment domain-containing protein 9 (CARD9), a molecule necessary for the induction of T-helper-17 cells, result in a specific defect in the ability of neutrophils to kill Candida, resulting in vulnerability to invasive Candida infections.16 Interestingly, the importance of the IL-17 pathway to Candida susceptibility is borne out in patients taking the increasingly prevalent IL-17–blocking medications, with early evidence suggesting an increase in Candida infections in psoriasis
and psoriatic arthritis patients taking the new anti– IL-17 medications brodalumab, secukinumab, and ixekizumab.17
RISK FACTORS
Risk factors for localized/superficial Candida infections include extremes of age; diabetes; obesity; pregnancy; HIV/AIDS (although prevalence has decreased significantly in the era of highly active antiretroviral therapy)18; and use of broad-spectrum antibiotics, corticosteroids, or immunosuppressive medications, specifically anti–IL-17-blocking medications as discussed above. Risk factors for oral candidiasis include xerostomia; wearing of dentures or other oral hardware; inhaled and systemic corticosteroids; vitamin deficiencies; radiation therapy to the head/ neck; and hypothyroidism.1 Risk factors for invasive candidiasis/candidemia include neutropenia and neutrophil dysfunction (including CARD9 mutations); hematologic malignancy; stem cell transplantation; indwelling intravascular catheters (including patients on hemodialysis); intensive care unit placement; and immunosuppressive medications.19
DIAGNOSIS
DIAGNOSIS
SUPPORTIVE STUDIES
The morphology may be distinctive and sufficient to make a clinical diagnosis in many cases of superficial Candida skin infection. Rapid confirmation may be achieved with bedside potassium hydroxide (KOH) preparation (either from a scraping from an intact pustule, or a touch preparation from a punch biopsy specimen) demonstrating pseudohyphae and budding yeast (Fig. 161-10).
Diagnostic algorithm for cutaneous candidiasis
Characteristic morphology
KOH preparation (scrape intact pustule if possible)
Swab culture (from intact pustule if possible)
Blood culture β-D-glucan and/or PCR (suspected candidemia)
Biopsy for H&E and tissue culture
2956
LABORATORY TESTING
Definitive diagnosis and speciation can be achieved via either swab culture (taken from an intact pustule if possible) or tissue culture from biopsy specimens taken from affected areas. In patients suspected of having candidemia, positive blood cultures are still considered the “gold standard” however with poor sensitivity (approximately 50%), adjunctive techniques such as β-d-glucan assay and polymerase chain reaction may be helpful.20
PATHOLOGY
Skin biopsies are of variable yield in making the diagnosis. While in localized mucocutaneous candidiasis, organisms may sometimes be readily seen in the epithelium with Grocott methenamine silver or periodic acid–Schiff staining, in patients with disseminated candidiasis, organisms (sometimes forming microabscesses) are more likely to be found in and around the dermal blood vessels, although sometimes only a mononuclear inflammatory infiltrate is seen.21
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
While most localized mucocutaneous Candida infections cause minor symptoms and respond readily to
24
For Cutaneous Candidiasis
■Seborrheic dermatitis
■Tinea corporis/dermatophytosis
■Impetigo
■Erythrasma
■Intertrigo
■Irritant contact dermatitis
■Allergic contact dermatitis
■Atopic dermatitis
■Bacterial folliculitis
■Herpes simplex or herpes zoster (localized or folliculitis)
For Oral Mucosal Candidiasis/Thrush
■Herpes simplex virus infection
■Oral hairy leukoplakia
■Morsicatio buccarum (chronic cheek chewing)
■Lichen planus white sponge nevus
For Paronychia and Onychomycosis
■Tinea unguium (dermatophyte nail infection)
■Nondermatophyte mold infections (eg, Acremonium, Alternaria)
■Acute bacterial paronychia
■Herpetic whitlow
■Squamous cell carcinoma
For Disseminated Candidiasis
For Disseminated Candidiasis
■Disseminated fungal infections: Fusarium, Aspergillus, zygomycosis
■Disseminated fungal infections: Fusarium, Aspergillus, zygomycosis
■Bacterial sepsis including meningococcemia, gonococcemia, and ecthyma gangrenosum
■Bacterial sepsis including meningococcemia, gonococcemia, and
ecthyma gangrenosum
■Disseminated herpes simplex, primary varicella, or disseminated herpes zoster
■Disseminated herpes simplex, primary varicella, or disseminated
herpes zoster
treatment, in patients with underlying risk factors (see “Risk Factors” before) infection may be recurrent and chronic, contributing to varying degrees of morbidity although not life-threatening. By contrast, mortality in patients with candidemia is significant, at 35% over 12 weeks in one larger study2; in some case series, the mortality exceeds 80%.8
MANAGEMENT
MANAGEMENT
CUTANEOUS CANDIDIASIS
First-line treatment of localized disease includes topical formulations of imidazoles (ketoconazole, clotrimazole, miconazole, econazole) in various formulations, which may include creams or powders. Nystatin
2957
4
24
FIRST LINE SECOND LINE
Cutaneous Topical imidazoles Topical nystatin Oral fluconazole
Paronychia Avoid wet work/use of gloves Topical corticosteroids Topical tacrolimus
Topical imidazole solutions Thymol 40% in ethanol Dilute acetic acid soaks
Onychomycosis Oral itraconazole Oral fluconazole Oral terbinafine
Oral (thrush) Mild:
■Clotrimazole troches
■Miconazole buccal tablets
■Disinfect dentures Severe or immunosuppressed:
■Oral fluconazole
Nystatin suspension Itraconazole, posaconazole, voriconazole, or amphotericin B solutions/suspensions
Vulvovaginitis Topical miconazole, clotrimazole, terconazole Oral fluconazole
Balanoposthitis Topical antifungal creams Low- to mid-potency topical corticosteroids (adjunctive)
Chronic mucocutaneous Oral imidazoles Oral triazoles (voriconazole and posaconazole) Long courses often required
Disseminated (candidemia) Infectious disease consul-l-l
Resistant disease:
■Echinocandins
■Liposomal amphotericin
■Flucytosine
Liposomal amphotericin
Hemodynamically stable immunocompetent patients:
Disseminated (candidemia) Infectious disease consultation is required
Liposomal amphotericin
Hemodynamically stable immunocompetent patients:
■Echinocandin (caspofungin, micafungin, or anidulafungin)
■Echinocandin (caspofungin, micafungin, or anidulafungin)
■Fluconazole Neutropenic patients:
■Fluconazole Neutropenic patients:
tation is required
■Empiric echinocandin
■Empiric echinocandin
■Switch to fluconazole once stable
■Switch to fluconazole once stable
topical is also effective. More severe cases typically require short courses of oral antifungals such as fluconazole 150 mg for several doses.
ORAL CANDIDIASIS
Clotrimazole 10-mg troches 5 times daily or miconazole 50-mg buccal tablets for 1 to 2 weeks is first-line treatment, with nystatin suspension 100,000 units/mL, 4 to 6 mL 4 times daily for 1 to 2 weeks as an alternative. Moderate and severe cases may require fluconazole 100 to 200 mg oral daily for 1 to 2 weeks. Itraconazole, posaconazole, voriconazole, and amphotericin B solutions and suspensions are alternatives for refractory or resistant disease. For denture wearers, disinfection of dentures is an important adjunctive step to prevent reinfection; the most effective methods for removal of Candida include soaking with commercially available effervescent denture tablets or a dilute bleach concentration of 1:32 or higher.23,24 For HIV-positive patients, initiation of highly active antiretroviral therapy is recommended to decrease chances of recurrence. For patients with recurrent disease, chronic suppressive dosing of fluconazole 150 mg orally 3 times weekly can be helpful.
PARONYCHIA AND ONYCHOMYCOSIS
First-line treatment of Candida onychomycosis is itraconazole given orally as pulsed dosing at 400 mg daily
2958
for 1 week monthly or 200 mg daily continuous dosing, for a total minimum duration of 4 weeks for fingernail and 12 weeks for toenail disease. Fluconazole is considered equally effective and can be given at 50 mg daily or 300 mg weekly dosing for similar durations. Although terbinafine has lower efficacy, cure rates are improved by longer courses of 250 mg daily for 4 months or longer, which makes compliance a potential concern.6
For chronic paronychia, avoidance of wet work or wearing of gloves to keep the skin dry is recommended. Given recent evidence that Candida colonization may play a secondary role, with the primary insult being skin barrier breakdown resulting from wet work and possible contact dermatitis,4 a role for topical corticosteroids has been demonstrated. In a randomized trial, topical corticosteroids were shown to yield a higher cure rate than systemic antifungals.25 Topical tacrolimus also is effective.26 Topical imidazole solutions, as well as thymol 40% compounded in ethanol or dilute acetic acid soaks, also have been used adjunctively in the treatment of chronic paronychia.
VULVOVAGINITIS AND BALANITIS
Topical antifungals such miconazole and clotrimazole are first-line treatment for Candida vulvovaginitis. Oral fluconazole (usually 150 mg in a single dose) is an alternative. Two to 3 doses 72 hours apart are recommended for more-severe cases, and even longer
courses for recurrent cases. For balanitis and balanoposthitis, topical antifungal creams, in some cases in conjunction with low- to mid-potency topical corticosteroids, are employed.
CHRONIC MUCOCUTANEOUS CANDIDIASIS
Given the high likelihood of recurrence, prolonged courses of oral imidazoles or newer triazoles (including voriconazole and posaconazole) are first-line treatment. Because of the development of resistance, echinocandins, liposomal amphotericin, or flucytosine is sometimes required.27
DISSEMINATED CANDIDIASIS
Treatment of patients with invasive candidiasis should be undertaken with the assistance of an infectious disease specialist. Either an echinocandin (caspofungin, micafungin, or anidulafungin) or fluconazole is a firstline treatment recommended in hemodynamically stable immunocompetent patients. Neutropenic patients should be started on empiric echinocandin and switched to fluconazole once stable.22 Resistance to azoles and echinocandins is a potential concern, particularly in non–Candida albicans species disease and in patients with prior exposure to these medications. Lipid formulation amphotericin B is an alternative in situations of resistance to first-line agents. Followup blood cultures and ophthalmologic examination are recommended for all patients with candidemia.
MALASSEZIA
AT-A-GLANCE
■ Malassezia species are normal flora of human skin.
■ Malassezia species can produce a variety of clinical presentations including pityriasis (tinea) versicolor, Malassezia folliculitis, seborrheic dermatitis, and neonatal cephalic pustulosis. Rarely, Malassezia species have been implicated in systemic infections, including catheter-related fungemia.
■ The diagnosis can be made via potassium hydroxide (KOH) preparation or skin biopsy. The organism is not typically cultured for this purpose as it requires special growing conditions (additional lipid).
■ Malassezia skin infections generally respond readily to topical treatments, including azole antifungals and selenium sulfide–based preparations. More extensive cases or those with folliculitis may require systemic antifungals.
■ Malassezia infections tend to have high recurrence rates and may require prophylactic treatment to prevent further episodes.
24
EPIDEMIOLOGY
EPIDEMIOLOGY
Malassezia (formerly known as Pityrosporum) are lipophilic dimorphic fungi that have been implicated in several skin conditions: pityriasis (tinea) versicolor, and Malassezia folliculitis. These organisms also have been identified at increased rates in inflammatory conditions including seborrheic dermatitis and atopic dermatitis, although their role in these conditions is less clear and thought to be more an exacerbating factor rather than a true infection.28 There are currently 14 species in the genus Malassezia, of which 11 have been detected as commensals on human skin.29 Colonization tends to occur by the age of 3 to 6 months, with earlier colonization in the neonatal phase associated with length of neonatal intensive care unit stays.30
Higher rates of Malassezia skin infections are seen in tropical climates and at the ages of peak sebum production (adolescence to young adulthood).31 In pityriasis versicolor and Malassezia folliculitis, Malassezia globosa is the most commonly isolated species,32,33 with Malassezia restricta and Malassezia sympodialis also frequently isolated from Malassezia folliculitis.34
These fungi also have been found to play a role in internal infections, with Malassezia (most frequently M. restricta and M. globosa) isolated from the sinuses of both healthy controls and patients with chronic rhinosinusitis.35 Malassezia species also are implicated in urinary tract infections, meningitis, pneumonia, and nosocomial bloodstream infections.36,37
Cather-related fungemia has been reported in neonates (most commonly by Malassezia pachydermatis, particularly preterm infants receiving parenteral lipid infusions and those with prolonged vascular catheterization.38 Malassezia fungemias also have been described in a series of immunocompromised older children and adults (with leukemias, solid tumors, diabetes, and severe combined immunodeficiency) with indwelling catheters, none of whom were receiving lipid infusions.39
CLINICAL FEATURES
CLINICAL FEATURES
CUTANEOUS FINDINGS
Pityriasis versicolor is a superficial Malassezia infection most commonly seen in adolescents and young adults. This condition is also known as tinea versicolor, but this nomenclature may be misleading as other tinea presentations are caused by dermatophytes rather than yeast. This condition manifests with asymptomatic to mildly pruritic patches and thin plaques with overlying fine scale favoring the neck, chest and back, upper arms, and, less commonly, the scalp, abdomen, and groin areas (Fig. 161-11). The name “versicolor” alludes to the spectrum of skin color changes that may be seen including hypopigmentation and hyperpigmentation, as well as erythematous to salmon-colored skin lesions (Fig. 161-12).
2959
4
24
A
B
Malassezia folliculitis presents as follicularly based erythematous monomorphic papules and pustules on the face, trunk, and upper arms (Fig. 161-13A). In contrast to acne vulgaris, comedones are a not a feature, and Malassezia folliculitis tends to spare the centrofacial areas.33 The lesions are often, but not always, pruritic. The condition is frequently diagnosed as misdiagnosed as acne vulgaris, and may even appear concurrently with acne.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Malassezia are normal flora of human skin, and rely upon hydrolysis of their human host sebum triglycerides as they lack a fatty acid synthase to allow endogenous production of C14-C16 saturated fatty acids.28,40
The free fatty acids thereby produced are believed to provoke inflammation in the skin of the host, as evidenced by the presence of a perivascular inflammatory infiltrate on histopathology.31 In pityriasis versicolor, the organism is able to transition to its pathogenic mycelial form and invade the stratum corneum. The pigmentary alterations produced in the skin are believed to be achieved via several mechanisms. The hypopigmentation seen especially in darker-skinned patients is thought to be a result of the production of azelaic acid, a dicarboxylic acid that inhibits of tyrosinase (an enzyme that catalyzes a key step in melanin synthesis) and also may be directly cytotoxic to melanocytes,41 while hyperpigmented lesions have been attributed to increased melanosomes and thickening of the stratum corneum.42
2960
RISK FACTORS
Tropical climates and heavy sweating are associated with increased rates of both pityriasis versicolor and Malassezia folliculitis. In addition, immunosuppression, oral antibiotics, and corticosteroids also are reported risk factors for Malassezia folliculitis.43 There has not been a consistent gender predilection reported.
DIAGNOSIS
DIAGNOSIS
SUPPORTIVE STUDIES
Pityriasis versicolor is often diagnosed visually based on its fairly distinctive morphology. Dermoscopy has been recommended as an ancillary tool in making the diagnosis of pityriasis versicolor as it highlights the fine scaling that may not always be readily visible to the naked eye.44 In both pityriasis versicolor and Malassezia folliculitis, illumination with a Wood lamp may reveal yellow-green fluorescence. KOH preparation can be a particularly useful in-clinic diagnostic test for pityriasis versicolor or Malassezia folliculitis and it will reveal short hyphae and yeast forms (the “ziti and meatballs” sign; Fig. 161-15). Although a superficial scraping of skin scales is adequate in pityriasis versicolor, the use of a comedone extractor or a needle to puncture an intact pustule is recommended to obtain a specimen in cases of Malassezia folliculitis where the yeast is situated
A B
C D
24
A B
2961
4
24
Diagnostic algorithm for cutaneous Malassezia infections
Additional feature for pityrasis veriscolor: fine scale (inducible or visualized by dermoscopy)
Characteristic morphology
Wood lamp (yellowgreen fluorescence)
KOH preparation Biopsy for H&E (culture not routinely performed)
deeper within the follicle.34,45 Staining with calcofluor white or May-Grunwald-Giemsa stain may improve visualization.43
LABORATORY TESTING
Culture is not generally used to confirm Malassezia infection because of the organism’s lipid requirement, which makes culture more logistically challenging— a layer of olive oil must be added or special growth media such as modified Dixon are required—and this is complicated further by slightly different growth requirements among different species.31
PATHOLOGY
Histopathology demonstrates Malassezia yeast forms; in pityriasis versicolor, they may be seen within the stratum corneum, while in Malassezia folliculitis they are found within dilated infundibula of plugged follicles in association with keratin debris (see Fig. 161-13B).46 A perivascular inflammatory infiltrate of lymphocytes, histiocytes, and neutrophils may be seen, which is typically mild unless the follicle has ruptured. A periodic acid–Schiff stain will highlight the organism.
2962
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE
AND PROGNOSIS
Superficial Malassezia infections are generally innocuous, and although most will respond readily to appropriate antifungal therapy, recurrence is common, particularly in those individuals with strong risk factors. Preterm neonates, immunosuppressed patients, and patients on
For Pityriasis Versicolor:
■Seborrheic dermatitis
■Pityriasis rosea
■Pityriasis alba
■Confluent and reticulated papillomatosis of Gougerot and Carteaud
■Tinea corporis/dermatophytosis
■Impetigo
■Secondary syphilis
■Mycosis fungoides
■Erythrasma
■Irritant contact dermatitis
■Allergic contact dermatitis
■Atopic dermatitis
■Epidermodysplasia verruciformis
For Malassezia Folliculitis:
For Malassezia Folliculitis:
■Acne vulgaris
■Acne vulgaris
■Bacterial folliculitis
■Bacterial folliculitis
■Steroid folliculitis
■Steroid folliculitis
■Eosinophilic folliculitis
■Eosinophilic folliculitis
■Rosacea
■Rosacea
■Demodex folliculitis
■Demodex folliculitis x x
FIRST LINE SECOND LINE
Pityriasis versicolor Shampoos (pyrithione zinc or selenium sulfide) Propylene glycol in aqueous solution Topical imidazoles (ketoconazole)
Oral fluconazole Oral itraconazole
Malassezia folliculitis Topical antifungal ± keratolytic (propylene glycol) Oral itraconazole
Malassezia
Topical antifungal ± keratolytic
Oral itraconazole
folliculitis
(propylene glycol)
parenteral lipid infusions are at higher risk of disseminated infection, as discussed above.
MANAGEMENT
MANAGEMENT
For Malassezia folliculitis, given the presence of the fungus deep within the hair follicle, monotherapy with topical antifungals is of less reliable efficacy. The addition of a keratolytic such as propylene glycol may improve the efficacy of topical antifungal treatment.45
Ultimately, many patients may require systemic treatment, with itraconazole being the best-studied treatment (200 mg daily for 1 to 3 weeks).45
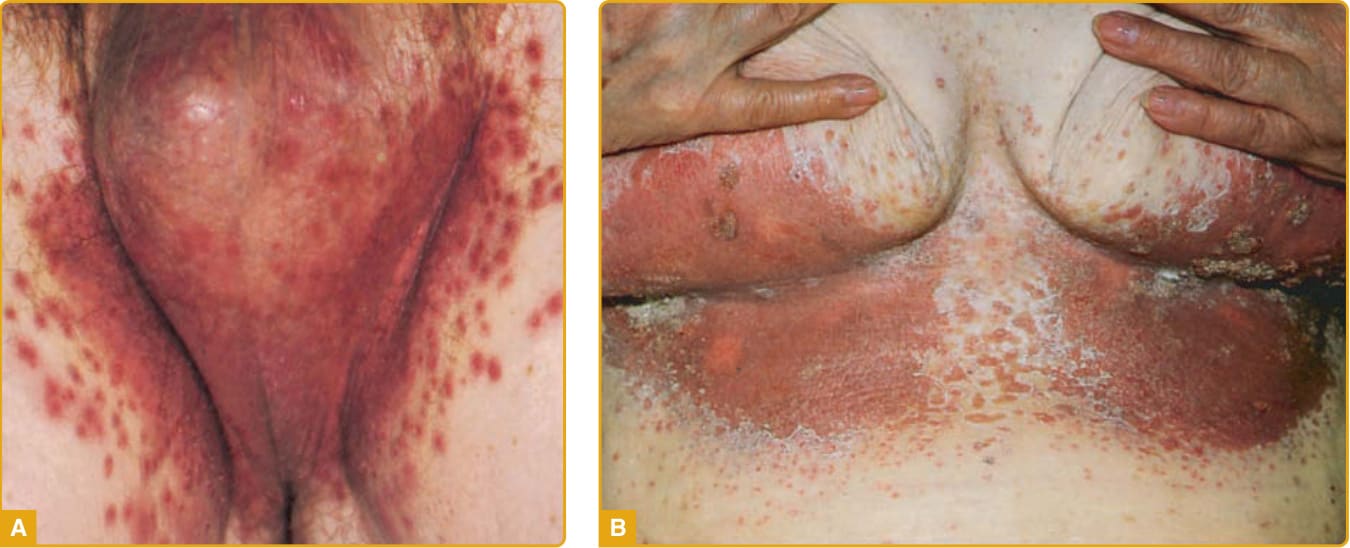
Figure 161-1 Typical morphology of cutaneous candidiasis demonstrating erythematous papules coalescing into plaques, with satellite papules and vesiculopustules.

Figure 161-2 Examples of Candida intertrigo. A, Erythematous papules becoming confluent over the inguinal area with prominent satellite papules (with scrotal involvement, in contrast to tinea cruris). B, Erythematous plaques with erosion and satellite papules. C, Diaper candidiasis demonstrated erythematous, partially eroded plaques, and satellite papules. D, Erosio interdigitalis blastomycetica demonstrating an erythematous plaque with prominent maceration in the interdigital webspace.

Figure 161-3 Miliaria caused by Candida seen on the forehead of a diabetic patient who had applied a partially occlusive dressing for headache symptoms.

Figure 161-4 A, Oral candidiasis (pseudomembranous form, thrush). Typical white palatal patches and plaques. B, Atrophic candidiasis demonstrating a shiny erythematous depapillated areas under areas in contact with dentures. C, Angular cheilitis (perleche) demonstrating fissured erythematous plaques at the bilateral oral commissures. D, Hyperplastic candidiasis on the dorsal lingual surface.

Figure 161-5 Balanoposthitis caused by Candida demonstrating pustules on the glans penis and foreskin.

Figure 161-6 A, Chronic paronychia caused by Candida albicans demonstrating erythematous, edematous proximal nailfold with onycholysis and mild dystrophy. B, Severely inflammatory candidal paronychia that has spread to the nail plate to produce onychomycosis.

Figure 161-7 Patient with chronic mucocutaneous candidiasis. Sharply marginated erythematous plaques with prominent scaling, reminiscent of plaque psoriasis.

Figure 161-8 Disseminated candidiasis with candidemia. Neutropenic febrile patient with acute myeloid leukemia demonstrating erythematous papules and nodules on the hand, some with central pustulation. Biopsy demonstrated Candida organisms and blood cultures were positive for Candida tropicalis.
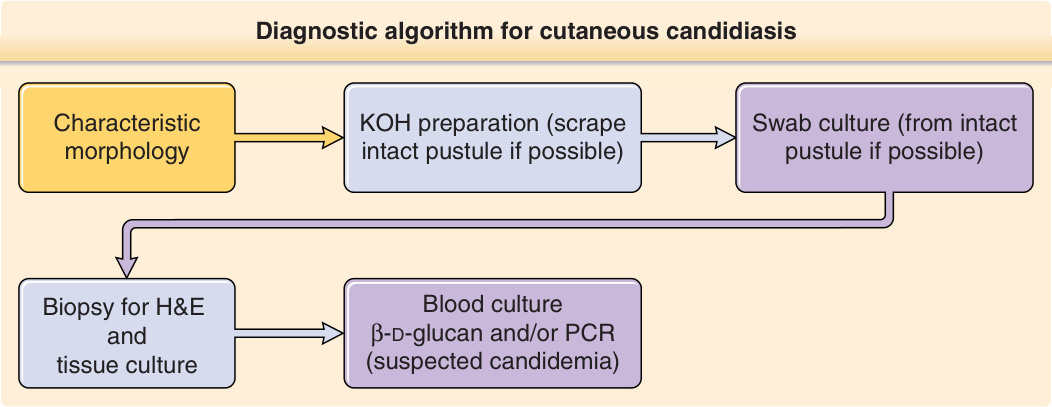
Figure 161-9 is an algorithm summarizing current recommendations for diagnosing cutaneous candidiasis.
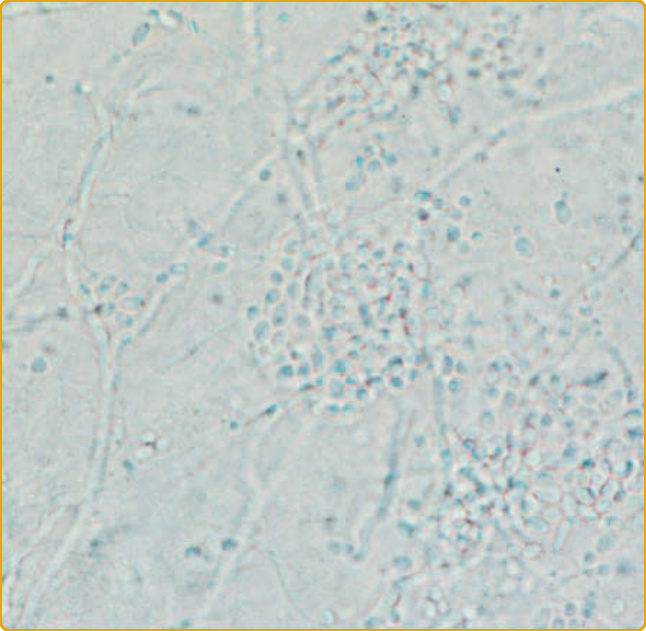
Figure 161-10 Potassium hydroxide (KOH) preparation demonstrating Candida forms including pseudohyphae and budding yeasts.
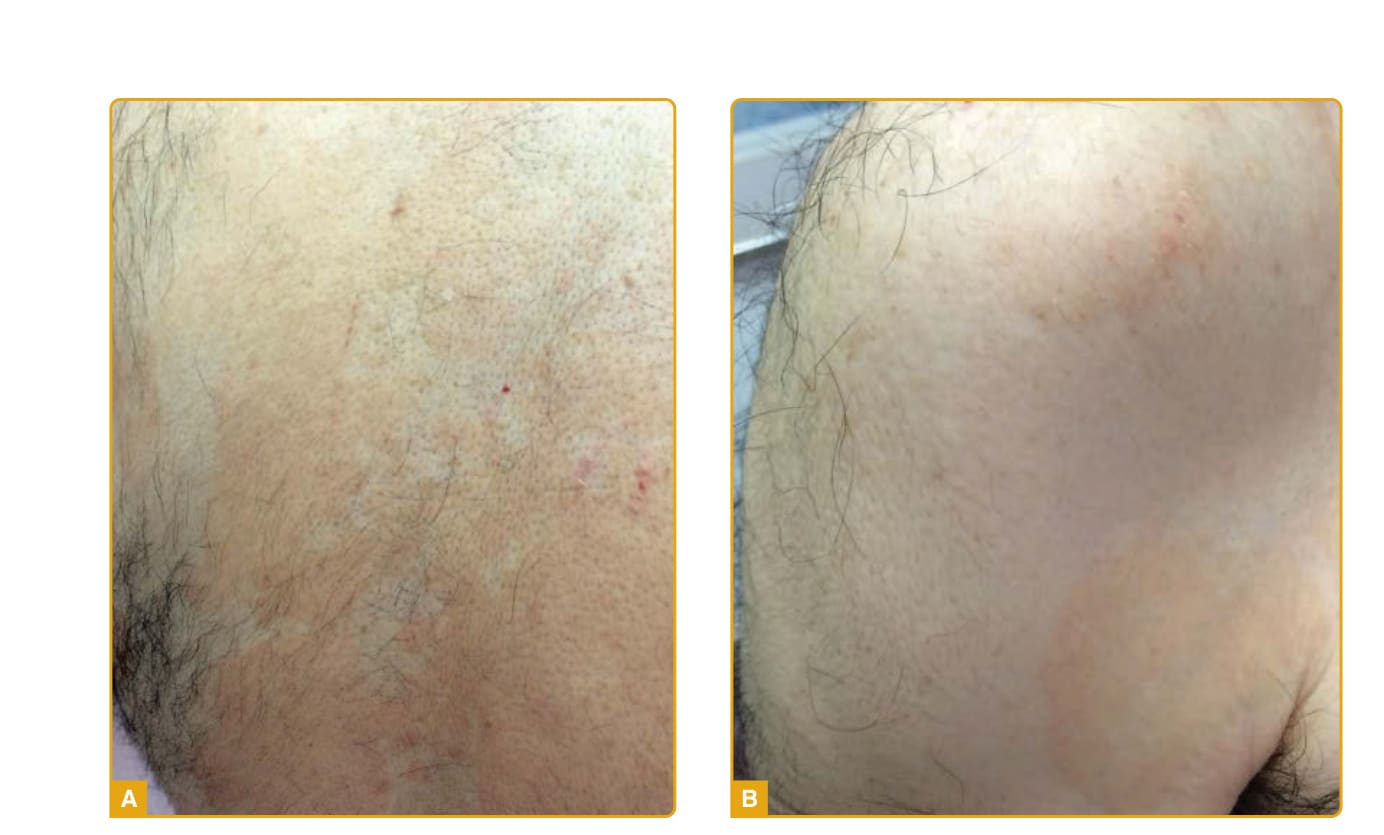
Figure 161-11 Pityriasis (tinea) versicolor. A, Multiple round to oval salmon-colored patches over the trunk. B, Salmoncolored patches and thin plaques on the shoulder and upper arm with fine overlying scale.
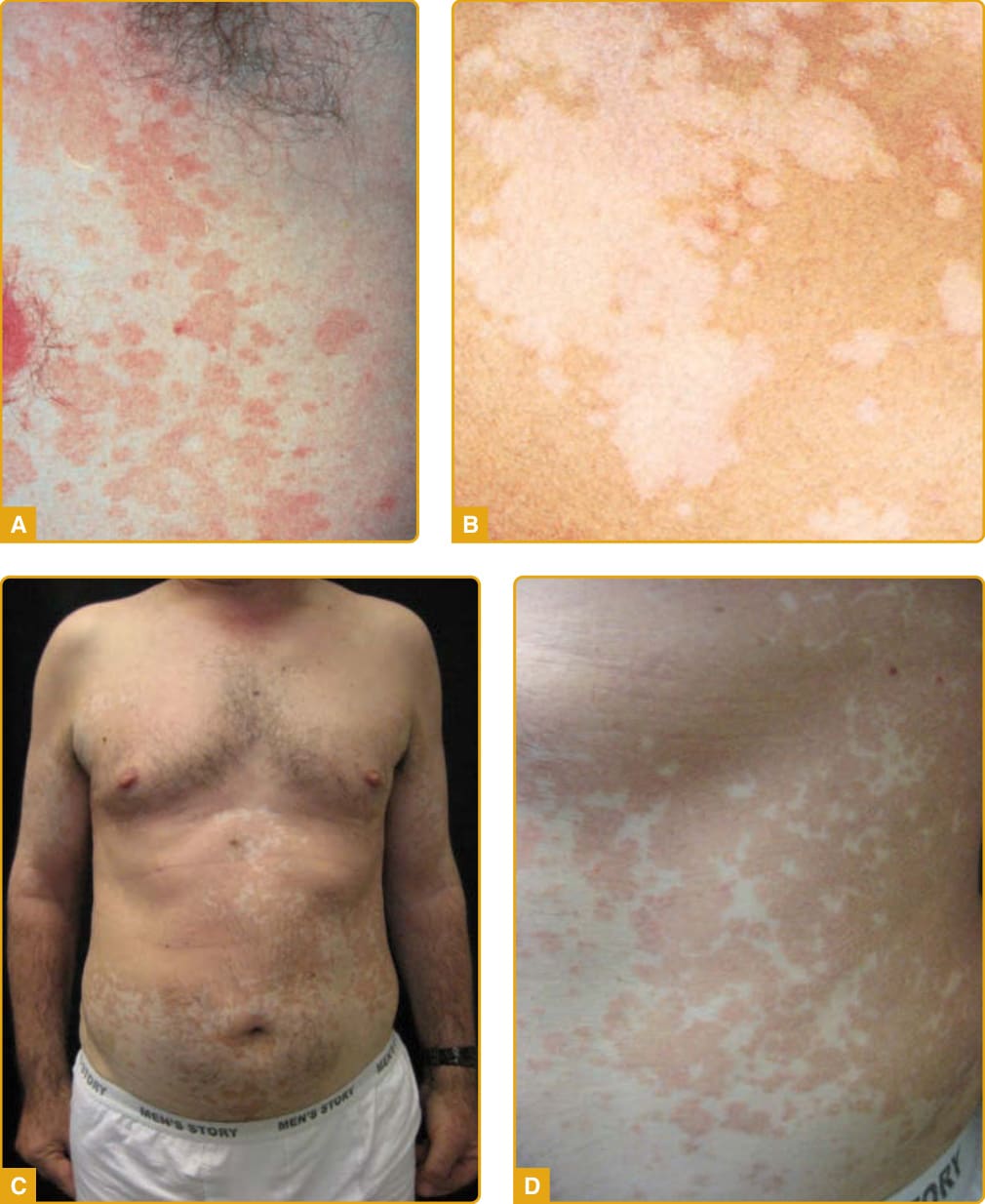
Figure 161-12 Pityriasis (tinea) versicolor. A, Erythematous macules and patches. B, Hypopigmented macules and patches that can be mistaken for vitiligo. C, Salmon-pink macules coalescing into patches. D,Characteristic fine overlying scale seen close up.

Figure 161-13 A, Malassezia folliculitis on the chest. B, Histopathology demonstrating yeast forms in the follicular infundibulum on hematoxylin-and-eosin (H&E) staining.
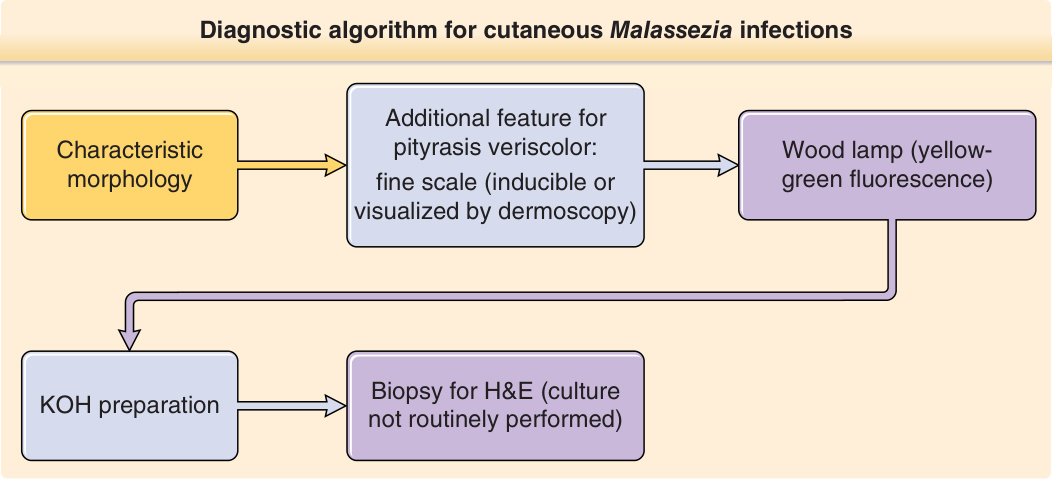
Figure 161-14 summarizes the diagnostic recommendations for cutaneous Malassezia infections.
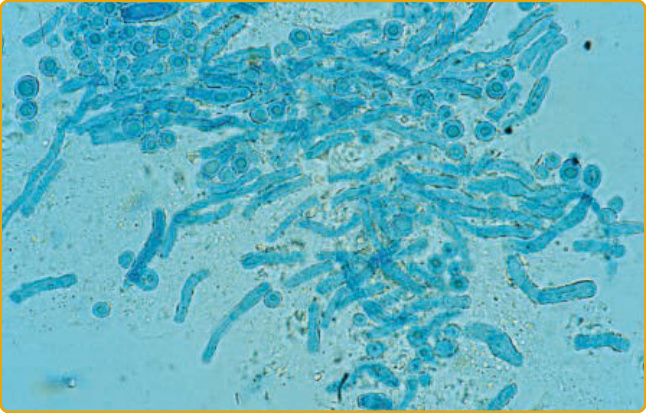
Figure 161-15 Potassium hydroxide (KOH) preparation of Malassezia demonstrating “ziti and meatballs” appearance of hyphae and yeast forms.
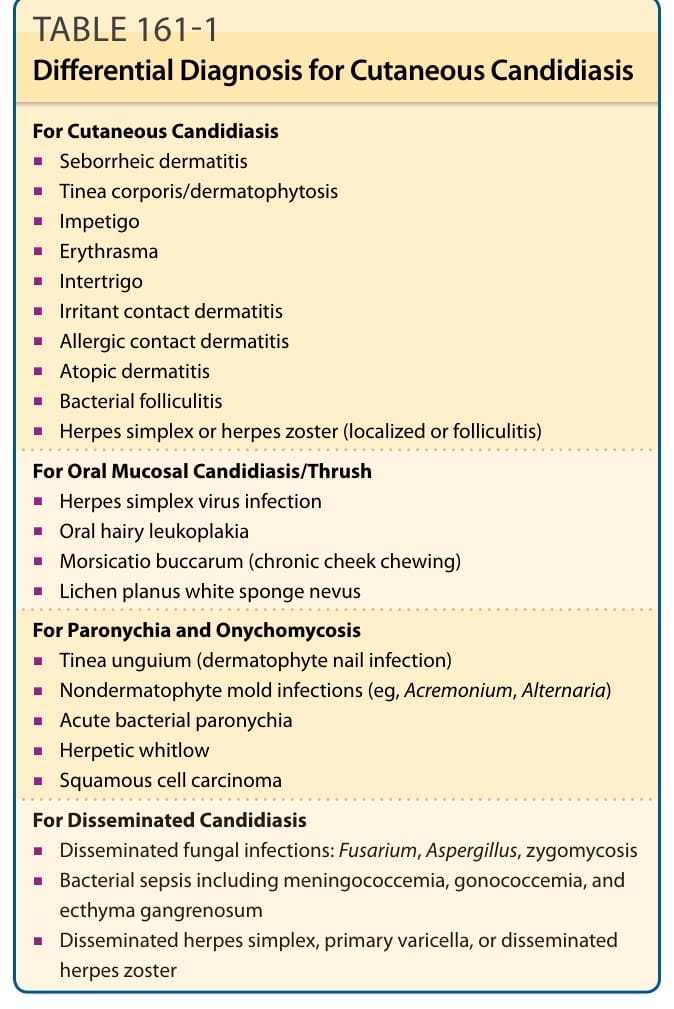
Table 161-1 summarizes the differential diagnosis for cutaneous candidiasis.
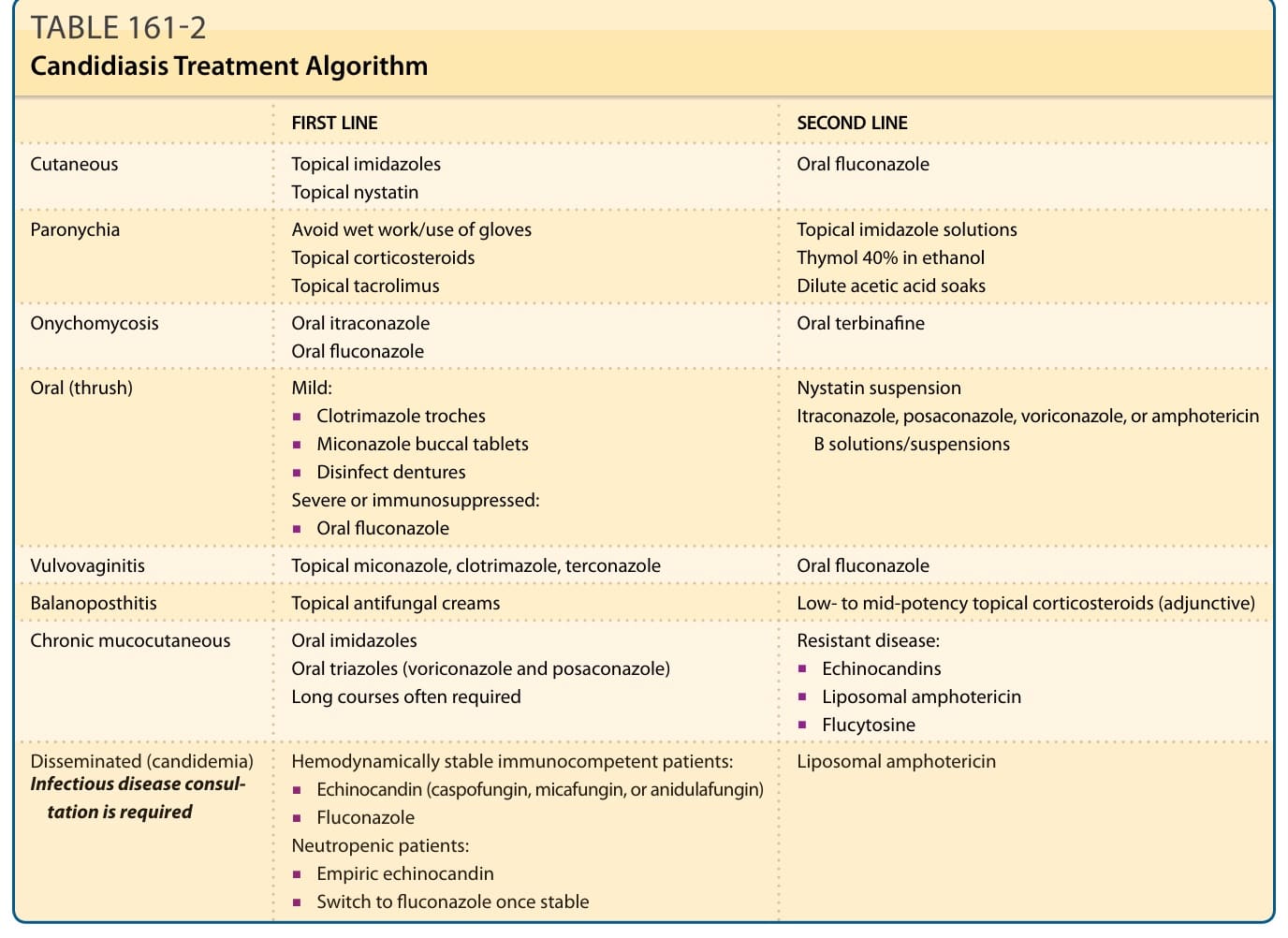
Table 161-2 summarizes the management of cutaneous candidiasis. The Infectious Diseases Society of America guidelines were most recently updated in 2016 (as of this writing) and provide clinicians with comprehensive guidance in the treatment of localized and disseminated Candida infections,22 as summarized below, and may be consulted for further detailed recommendations. Areas not covered by these guidelines include the treatment of localized cutaneous candidiasis, chronic mucocutaneous candidiasis, paronychia, and onychomycosis, for which other relevant sources are provided.
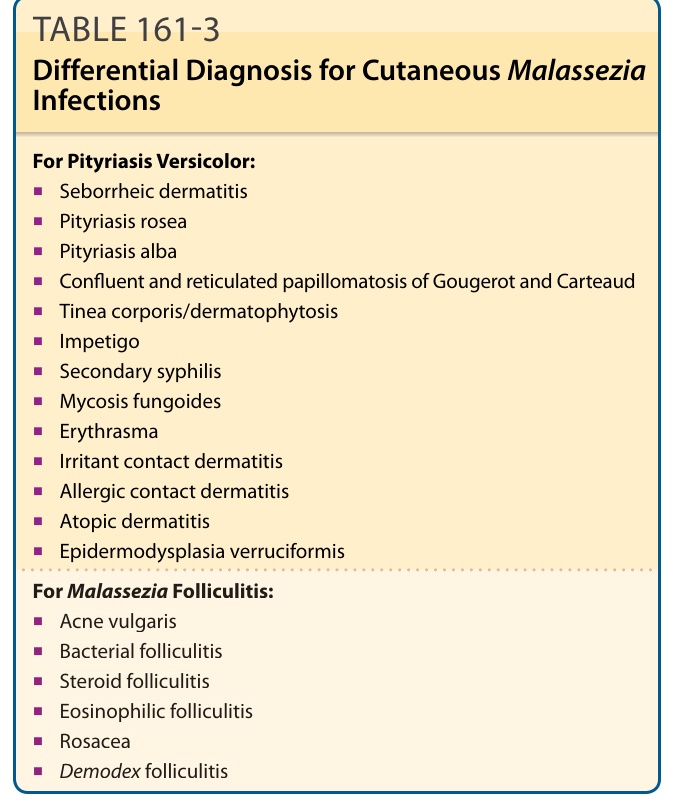
Table 161-3 summarizes the differential diagnosis for cutaneous Malassezia infections.
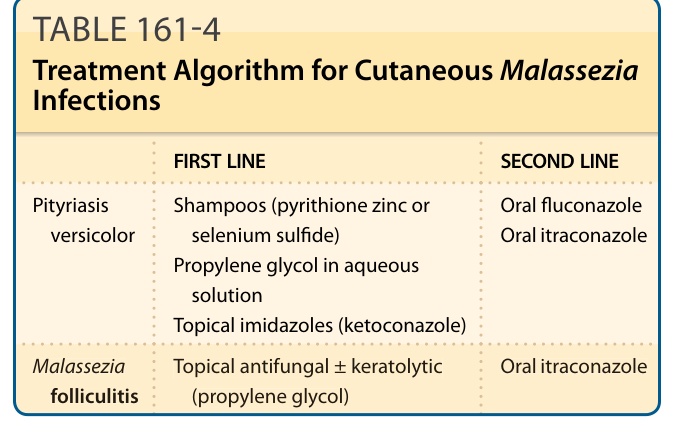
TABLE 161-4 Treatment Algorithm for Cutaneous Malassezia Infections