Superficial Fungal Infection
PART24
Fungal Diseases
AT-A-GLANCE
■ Mycoses are divided among 3 forms: superficial, subcutaneous, and deep/systemic.
■ Superficial fungal infection is defined as a dermatophyte infection of keratinized tissues including skin, hair, and nails.
■ Dermatophyte species are contained in 3 genera (Epidermophyton, Microsporum, and Trichophyton), which are further divided according to 3 natural habitats (humans, animals, and soil).
■ Trichophyton is the most common genera isolated in the United States.
■ Trichophyton rubrum is the most common cause of dermatophytosis of the skin.
■ Trichophyton tonsurans is the most common cause of tinea capitis in the United States.
■ Piedra, which consists of white and black forms, is an asymptomatic superficial fungal infection of the hair shaft.
■ Onychomycosis is the name given to dermatophytosis of the nails.
■ Microscopic examination, culture, Wood light evaluation, and histopathology may all be useful in confirming diagnosis.
■ Several topical and oral antifungals are available for effective treatment of dermatophytosis.
■ Infections involving hair bearing skin and nails typically require oral treatment.
MYCOSES
Mycoses are divided among 3 forms: (a) superficial, involving stratum corneum, hair, and nails; (b) subcutaneous, involving dermis and/or subcutaneous tissue; and (c) deep/systemic, representing hematogenous
spread of organisms including opportunistic pathogens in immunocompromised hosts. This chapter focuses on the superficial mycoses and their patterns of integumentary infections (Table 160-1). Table 160-2 is a glossary of terms used in this chapter.
DERMATOPHYTES
The kingdom of fungi comprises more than 1.5 million species worldwide. Dermatophytes (the term is derived from the Greek words for “skin plant”) are represented by approximately 40 species divided among the 3 genera Trichophyton, Microsporum, and Epidermophyton, all falling within the Arthrodermataceae family. In the United States, Trichophyton species, namely Trichophyton rubrum and Trichophyton interdigitale, represent the most common isolated species. Dermatophytes are classified further according to their natural habitats—humans, other animals, and soil. Their ability to attach to, invade, and use keratin as a source of nutrition underlies the pathogenesis of superficial fungal infection of skin, hair, and nails, and is termed dermatophytosis.1
TAXONOMY
TAXONOMY
Recent modifications to the taxonomical system of dermatophytes affecting clinical practice require mention. While classic taxonomy is governed by what is phenotypically observable, recent inclusion of data from genotypical analysis has necessitated regrouping of some taxa, as many of these genotypical differences are not reflected phenotypically, and vice versa.2 Contradictions between what is phenotypically observable and found via genomic analysis make devising such a taxonomical system for dermatophytes difficult. According to the classic, yet still current, rules
4
24
GENERA SKIN HAIR NAILS
Trichophyton × × ×
Microsporum × ×
Epidermophyton ×
×
Tinea nigra ×
Black piedra ×
White piedra ×
White piedra ×
of taxonomy governing nomenclature, a species must be identifiable in nature, with physical specimens able to be cultured and proven to be sexually isolated from others, before they may be formally named. Conversely, newer molecular ecologic studies using sequencing of variable genomic regions, such as the internal transcribed spacer regions, of pooled fungal ribosomal DNA have discovered (a) more internal transcribed spacer regions than there are in known/ observable species, (b) multiple species may have identical internal transcribed spacer regions, and (c) there may be multiple forms of internal transcribed spacer in one species’ genome.3 Current fungal taxonomy includes a synthesis of the new genomic data and classic phenotypical characterizations. In the case of dermatophytes, many species overall have very little genetic diversity and may live in the same environmental niche. Phenotypically, this is reflected by similar clinical manifestations being caused by multiple taxonomically different dermatophyte species. The additional classification of superficial fungi according to natural habitat is clinically
■Anthropophilic—preferring humans over other animals as the natural habitat.
■Anthropophilic—preferring humans over other animals as the
natural habitat.
■Arthroconidia—asexual spore produced by segmentation of hyphae.
■Arthroconidia—asexual spore produced by segmentation of
hyphae.
■Dematiaceous—melanin in the cell walls of its conidia, hyphae, or both results in a darkly colored fungus.
■Dematiaceous—melanin in the cell walls of its conidia, hyphae, or
both results in a darkly colored fungus.
■Ectothrix—dermatophyte growth pattern with spores forming a sheath on the outside of the hair shaft.
■Ectothrix—dermatophyte growth pattern with spores forming a x— x sheath on the outside of the hair shaft.
■Endothrix—dermatophyte growth pattern with spore formation within the hair shaft.
■Endothrix—dermatophyte growth pattern with spore formation x— x within the hair shaft.
■Favus—dermatophyte growth pattern with hyphae and air spaces within the hair shaft.
■Favus—dermatophyte growth pattern with hyphae and air spaces
within the hair shaft.
■Geophilic—preferring the soil over humans and animals as natural habitat.
■Geophilic—preferring the soil over humans and animals as natural
habitat.
■Hyphae—long, filamentous fungus cells forming a branching network called mycelium.
■Hyphae—long, filamentous fungus cells forming a branching net-
work called mycelium.
■Macroconidia—asexual large multinucleate spores produced by vegetative reproduction.
■Macroconidia—asexual large multinucleate spores produced by
vegetative reproduction.
■Microconidia—asexual small spores produced by vegetative reproduction.
■Microconidia—asexual small spores produced by vegetative
reproduction.
2926
■Zoophilic—preferring animals over humans as the natural habitat.
■Zoophilic—preferring animals over humans as the natural habitat.
relevant, as anthropophilic, zoophilic, and geophilic dermatophytoses provide important information about the source of infection and may demonstrate varied clinical features.
ANTHROPHILIC
Anthrophilic species are typically restricted to human hosts and are transmitted via direct contact. Infected skin or hair retained in clothing, combs, caps, socks, and towels, for example, also serve as source reservoirs. Unlike the sporadic geophilic and zoophilic infections, anthropophilic infections are often epidemic in nature. These dermatophytes have adapted to humans as hosts and elicit a mild to noninflammatory host response.
ZOOPHILIC
Zoophilic species are transmitted to humans from animals. Cats, dogs, rabbits, guinea pigs, birds, horses, cattle, and other animals are common sources of infection. Transmission may occur through direct contact with the animal itself, or indirectly via infected animal hair. Exposed areas, such as the scalp, beard, face, and arms, are favored sites of infection. Microsporum canis is often transmitted to humans from cats and dogs, whereas guinea pigs and rabbits are a frequent source of human infection with zoophilic strains of T. interdigitale. Although host adaptation by zoophilic dermatophytes may lead to relatively silent infections, these dermatophytes tend to produce acute and intense inflammatory responses in humans.1
GEOPHILIC
Geophilic fungi cause sporadic human infection upon direct contact with the soil. Microsporum gypseum is the most common geophilic dermatophyte cultured from humans. There is a potential for epidemic spread as a consequence of the higher virulence of geophilic strains, as well as an ability to form long-lived spores that may reside in blankets or grooming tools. As with zoophilic infections, geophilic dermatophytes typically result in intense inflammatory responses.4
EPIDEMIOLOGY
Superficial fungal infection is a worldwide problem that affects more than 25% of the population.5 Some species demonstrate ubiquitous distribution, whereas others are geographically limited. Accordingly,
HABITAT DERMATOPHYTE HOST
Anthropophilic Trichophyton rubrum (syn: Trichophyton megninii, Trichophyton gourvilii)
Humans
Trichophyton tonsurans
Trichophyton interdigitale (syn: Trichophyton mentagrophytes var. interdigitale)
Trichophyton schoenleinii
Trichophyton soudanense
Trichophyton violaceum (syn: Trichophyton yaoundei)
Trichophyton concentricum
Microsporum audouinii
Microsporum ferrugineum
Epidermophyton floccosum
Zoophilic Trichophyton mentagrophytes (syn: Trichophyton mentagrophytes var. quinckeanum)
Rodents
Trichophyton interdigitale (syn: Trichophyton mentagrophytes var. mentagrophytes, Trichophyton mentagrophytes var. granulosum)
Rodents
Trichophyton erinacei Hedgehogs
Trichophyton simii Primates
Trichophyton verrucosum Cattle
Microsporum canis (syn: Microsporum distortum, Microsporum equinum)
Cats, dogs, horses
Microsporum amazonicum Rodents
Microsporum gallinae Poultry
Microsporum nanum Pigs
Microsporum persicolor Rodents
Geophilic Microsporum gypseum Soil
Microsporum cookei
Microsporum persicolor
Trichophyton vanbreuseghemii
Trichophyton eboreum
Trichophyton terrestre
Trichophyton terrestre
predominant species reflect considerable geographic differences, as in the case of tinea capitis. In the United States, Trichophyton tonsurans replaced Microsporum audouinii as the most common cause of tinea capitis in the second half of the 20th century, and M. canis has now become the second most common cause.6 In Europe, M. canis remains the most common cause of tinea capitis despite a significantly increased incidence of T. tonsurans.7 The etiologic profile is quite different in Africa where M. audouinii, Trichophyton soudanense, and Trichophyton violaceum are the most prevalent pathogens.8 However, human travel and
24
migration results in dynamic patterns of infection. As an example, T. soudanense and T. violaceum, typically restricted to Africa, were isolated in U.S. cases of tinea capitis in 2007.9
Clinical presentations of dermatophytoses depend not only on the source, but also on host factors. Immunocompromised individuals are more susceptible to refractory dermatophyte infections or to deep mycoses.10,11 Interestingly, only the severity of dermatophytosis appears to be increased with HIV infection, and not the prevalence.12 Other host factors, such as age, sex, and race, appear to be additional epidemiologic factors for infection, although their relationship to dermatophyte susceptibility remains unclear. As an example, dermatophyte infections are 5 times more prevalent in males than females. Finally, local customs may also influence rates and patterns of dermatophytoses. The use of macerating occlusive footwear, for example, in industrialized nations has made tinea pedis and onychomycosis much more common in these regions.13
CLINICAL FEATURES
Clinical features of the dermatophytoses vary depending upon the causative dermatophyte (as discussed before) and the site of infection (ie, skin, hair, or nails). Skin dermatophytoses are generally named according to the following paradigm: the word tinea (Latin for “worm”) followed by a Latin term denoting location or other descriptive factor. Diagnoses within this category include tinea barbae, tinea capitis, tinea corporis, tinea cruris, tinea favosa (derivative of Latin favus, meaning “honeycomb”), tinea manuum, tinea nigra, and tinea pedis. Dermatophytosis of the hair is known as piedra, and of the nails as onychomycosis. A dermatophytid or id reaction (autoeczematization) is an acute inflammatory dermatitis at sites distant from the primary inflammatory fungal infection. (See individual diagnoses listed alphabetically under the section “Dermatophytoses” for more detail.)
PATHOGENESIS
Dermatophytes exhibit a broad armamentarium of enzymes (eg, keratinolytic proteases, lipases) and other virulence factors to allow adherence, use of keratin as a source of nutrients, invasion, and growth of mycelial elements for survival in keratinized tissues. As a consequence of keratin degradation with subsequent release of proinflammatory mediators, the host develops an inflammatory response of varying degree. The degree of inflammation is dependent upon pathogen and host factors. The classic “ringworm,” or annular, morphology of tinea corporis results from an inflammatory host response against a spreading dermatophyte, followed by a reduction or clearance of fungal elements from within the plaque, and (in many cases) spontaneous resolution of the infection.
2927
4
24
ADHERENCE
ADHERENCE
Dermatophytes overcome several lines of host defense before hyphae begin to thrive in keratinized tissues. The first step is successful adherence of arthroconidia, asexual spores formed by fragmentation of hyphae, to keratin via adhesin to result in alteration of gene expression.14,15 Dermatophytes make selective use of their proteolytic armamentarium during adherence and invasion.16,17 Following several hours of successful adherence, the spores begin to germinate in preparation for the next step in the infective chain of events, invasion.
INVASION
INVASION
Trauma and maceration facilitate penetration of dermatophytes through the skin. Invasion of germinating fungal elements is further accomplished through secretion of specific proteases, lipases, and ceramidases, the digestive products of which also serve as fungal nutrients.18 Interestingly, components of the fungal cell wall, including β-glucan, galactomannans, and chitin, show inhibitory effects on keratinocyte proliferation (to allow invasion before desquamation) and cell-mediated immunity (discussed in the following section “Host Response”).19,20 Once dermatophytes penetrate through the epidermis to the dermis, binding of adhesin to elastin again changes gene expression.14
HOST RESPONSE
HOST RESPONSE
Dermatophytes encounter a range of host responses from the nonspecific, innate to the well-tuned, adaptive immune systems. In the line of defense mechanisms, the epithelial surface, antimicrobial peptides (defensins, cathelicidins, S100 proteins, fungistatic fatty acids in sebum), and competing bacterial flora represent the first barrier against invading fungal elements.13,21,22 Besides acting as a passive physical barrier, epidermal keratinocytes play a more active role by expressing multiple pattern recognition receptors including C-type lectin receptors and multiple Tolllike receptors (TLRs) located either on the cell surface (TLR1, TLR2, TLR4, TLR5, and TLR6) or in the endosomes (TLR3 and TLR9).23 The innate immune system is able to monitor for microbes via these pattern recognition receptors, which function to bridge innate and adaptive immunity upon recognition of pathogen-associated molecular patterns to result in targeted cytokine production, recruitment, and polarization of relevant T, B, and natural killer lymphocyte subsets.21 The specific immune response generated depends upon the cell type involved.24 Monocytes, macrophages, neutrophils, epithelial, and endothelial cells phagocytize and directly kill fungi.24 Upon TLR binding of a fungal pathogen-associated molecular
2928
pattern, mannan, keratinocytes (a) increase proliferation to promote shedding, (b) increase secretion of antimicrobial peptides (such as human β defensins, ribonuclease 7, and Psoriasin) to inhibit growth of dermatophytes, and (c) increase secretion of proinflammatory cytokines (interferon-α, tumor necrosis factor-α, interleukin [IL]-1β, IL-8, IL-16, and IL-17) to further activate the immune system.23,25,26 A C-type lectin receptor called Dectin-1 binds β-1,3-glucan on fungi to activate the SYK–CARD-9 signaling pathway in neutrophils, macrophages, and dendritic cells to promote IL-23 production and subsequent T-helper (Th)-17 cell induction.21 Dendritic cells mature and promote differentiation of naïve T cells into effector Th cell subtypes after uptake of fungi.25 Once dermatophytes are able to penetrate into deeper layers of the epidermis, new nonspecific defenses emerge, such as competition for iron by unsaturated transferrin and activation of complement to inhibit fungal growth.20
The next level of defense is cell-mediated immunity resulting in a specific delayed-type hypersensitivity response against invading fungi. The degree of inflammatory reaction depends on the host’s immune status as well as the dermatophyte species involved. The inflammatory response associated with this hypersensitivity correlates with clinical resolution, while defective Th1 cell-mediated immunity, important for the activation of phagocytes at the site of infection, may result in chronic or recurrent dermatophytosis.24 In patients with chronic infection, it has been reported that T. rubrum conidia cause macrophages to increase production of tumor necrosis factor-α and IL-10 without increased IL-12 or nitric oxide, decrease costimulatory molecules, and inhibit phagocytosis; thus, when conidia are ingested, the macrophage is unable to digest the conidia, which continue growing inside until they rupture the macrophage.23 The Th2 response does not appear to be protective, as patients with elevated fungal antigen antibody titers are observed to have widespread dermatophyte infections.27 A possible role for the Th17 response to dermatophyte infections is suggested by the discovery of hyphal elements binding to Dectin-2, a C-type lectin pattern recognition receptor on dendritic cells, critical for inducing Th17 responses.28,29 Recall that many innate immune cells release proinflammatory cytokines. Some of these, such as IL-1β, transforming growth factor-β, and IL-6, promote the development of Th17 cells from naïve T cells via signal transducer and activator of transcription (STAT)-3 to induce transcription of the Th17 lineage retinoic acid-related orphan receptor gt.21 Furthermore, cell expansion and maintenance of Th17 cells is promoted by IL-23. In return, Th17 secretion of IL-17A, IL-17F, and IL-22 activates epithelial cells, granulopoiesis, neutrophil recruitment, and production of chemokines and antimicrobial factors crucial for epithelial immunity against fungi.21 Thus, a successful host response to dermatophyte infection is dependent upon well-orchestrated interaction and participation of both the innate, nonspecific, and adaptive, cellular immune systems. Some fungi have evolved to evade immune surveillance. For example, anthropophilic dermatophytes
induce secretion of a limited cytokine profile from keratinocytes in vitro compared to zoophilic species.30,31
One study found the mannans from T. rubrum are more capable of inhibiting mitogen-induced lymphoproliferation than those of M. canis.20 This difference may reflect the augmented inflammatory response generally clinically observed with zoophilic species. In the case of the most common dermatophytic pathogen, T. rubrum is first recognized by keratinocytes when fungal pathogen-associated molecular patterns are sensed by pattern recognition receptors (as discussed above) to result in increased expression and transportation of TLRs (such as TLR2) to the surface of keratinocytes, with subsequent increased recognition, and secretion of proinflammatory cytokines, including interferon-inducible protein-10 and monocyte chemotactic protein-1.32 In one study, after 24 hours of contact with T. rubrum conidia, surface expression of TLR2 was downregulated, resulting in decreased keratinocyte release of proinflammatory cytokines.32 In another study, viable intact conidia inhibited TLR2 and TLR6 expression and decreased human beta defensin-1 and human beta defensin-2 production.23 Thus, after an initial, short-lived inflammatory response resulting in clearance of active infection, T. rubrum is able to manipulate and evade surveillance by the epithelial innate immune system as inert conidia so as to survive until conditions are favorable for germination and recurrent infection.
24
GENETICS
GENETICS
Despite epidemiologic observation suggesting a genetic predisposition to dermatophyte infection, molecular insight confirming this hypothesis has been relatively lacking. Genetic mutations in the TLRs and their adaptors may result in increased susceptibility to bacterial and viral infection, but not to fungal infection.21 Polymorphisms of TLR1 and TLR4 are associated with increased risk of invasive fungal disease, and polymorphisms of TLR3 are associated with cutaneous candidiasis.21 Polymorphisms of the C-type lectin receptor Dectin-1 and mutations of CARD-9 with decreased IL-17 production are associated with chronic mucocutaneous candidiasis along with chronic dermatophyte infections.21,33 Multiple mutations are associated with increased susceptibility to other fungi, such as IL-17 receptor and cytokine genes, STAT1 and STAT3, DOCK8, Tyk2, AIRE, IL-12RB1, and MST1/ STK4, which increase mucocutaneous fungal infections; and CYBB, NCF1, NCF2, NCF4, CYBA, MAGT1, and RAG1, which increase invasive fungal infections.21
DIAGNOSIS
LABORATORY TEST METHOD FUNCTION FINDINGS
Potassium hydroxide preparation (KOH) Scales from advancing border, subungual debris, or affected hair removed and placed on a glass slide. KOH 10% dropped on specimen and covered with a cover slip. The undersurface of the glass slide may be gently heated with a low-lit flame.
KOH solution and gentle heating softens keratin and highlights the dermatophyte.
Culture Sabouraud medium (4% peptone, 1% glucose, agar, water).
Long, narrow, septated and branching hyphae.
Facilitates growth of dermatophytes. Microscopic morphology of microconidia and macroconidia, along with culture features including surface topography and pigmentation. The reader is referred to http://www .mycology.adelaide.edu.au/ for a comprehensive characterization of fungal colonies. Common colonies are characterized in Table 160-5.
Modified Sabouraud medium (addition of chloramphenicol, cycloheximide, and gentamicin).
Facilitates growth of dermatophytes and inhibits growth of non–Candida albicans, Cryptococcus, Prototheca species, Phaeoannellomyces werneckii, Scytalidium species, and Ochroconis gallopava.
Dermatophyte test medium Scales from the advancing border, subungual debris, or affected hair embedded in the medium.
Medium contains the pH indicator phenol red. Dermatophytes use proteins, which result in excess ammonium ion and an alkaline environment.
Histopathology special
Tissue may be obtained by skin
Incubation at room temperature for 5 to 14 days results in change in medium color from yellow to bright red in the presence of a dermatophyte.
Stains fungal cell wall to detect fungal
Histopathology special stains: periodic acid– Schiff (PAS) and Grocott methenamine silver (GMS)
Pink (PAS) or black (GMS) fungal
Tissue may be obtained by skin or nail biopsy techniques. Stains fungal cell wall to detect fungal elements in tissue sections. Pink (PAS) or black (GMS) fungal elements noted in the stratum corneum
stains: periodic acid– Schiff (PAS) and Grocott methenamine silver (GMS)
or nail biopsy techniques.
elements in tissue sections.
elements noted in the stratum corneum
2929
4
24
The clinical diagnosis of a dermatophyte infection can be confirmed by microscopic detection of fungal elements, by identification of the species through culture, or by histologic evidence of the presence of hyphae in the stratum corneum. In addition, fluorescence patterns under Wood light examination may support a clinical suspicion.
MICROSCOPIC EXAMINATION
MICROSCOPIC
EXAMINATION
Although microscopic evaluation of potassium hydroxide (KOH)-treated samples of scale does not allow for speciation or characterization of the susceptibility profile, it can be used as a quick and inexpensive bedside tool to provide evidence of dermatophytosis. In dermatophytosis involving the skin, hair, or nails, septate and branching hyphae without constriction (Fig. 160-1) may be visualized under microscopic examination with 10% to 20% KOH preparation. All superficial dermatophytes appear identical when visualized in this manner. Because KOH examination may yield false-negative results in up to 15% of cases, patients suspected of having dermatophytosis on clinical impression should be treated.34 Culture confirmation should be considered whenever systemic treatment is warranted, such as in the case of onychomycosis. To perform KOH examination of the skin, collect scale by scraping the involved area with a dull edge (eg, a no. 15 blade or edge of slide) outward from the advancing margins. This same technique may be used to scrape under affected nails (but diagnosis of onychomycosis is best confirmed with histopathology or culture as discussed further). Scrapings are then placed on a glass slide, covered with a coverslip, and prepared with 10% to 20% KOH. Place several drops of KOH on the slide adjacent to the coverslip edge, allowing capillary action to wick the fluid under the coverslip. A paper towel may then be used to blot excess
2930
Ectothrix and endothrix hair involvement
Ectothrix Endothrix
KOH solution from around the coverslip. Penetration of KOH into keratin may be aided by either slightly warming the slide with a low-intensity flame or by addition of dimethylsulfoxide (DMSO) in KOH solution. Some may also find the adding a drop of blue or black stain such as chlorazol black (in similar fashion as KOH solution above) helpful for better identifying fungal elements (as seen in Fig. 160-1). Hairs should be plucked (not cut), placed on a glass slide, prepared with 10% to 20% KOH, and covered with a coverslip. Slightly warming the slide with a low-intensity flame allows better penetration of the KOH solution into keratin. Low-power microscopy will reveal 3 possible patterns of infection (Fig. 160-2): (a) ectothrix—small or large arthroconidia forming a sheath around the hair shaft; (b) endothrix—arthroconidia within the hair shaft; or (c) favus—hyphae and air spaces within the hair shaft.
CULTURE
CULTURE
Speciation of superficial fungi is based on macroscopic, microscopic, and metabolic characteristics of the organism. Although some dermatophytes are readily identified on the basis of their primary isolation cultures, most require further differentiation through subcultures on specific media (identification culture) or through specific biochemical tests. Sabouraud dextrose agar (SDA) is the most commonly used isolation medium for dermatophytes and it serves as the medium on which most morphologic descriptions are based. Elimination of contaminant molds, yeast, and bacteria is achieved by the addition of cycloheximide and chloramphenicol (± gentamicin) to the medium making it highly selective for the isolation of dermatophytes. The development of colonies can take 5 to 7 days in the case of Epidermophyton floccosum and up to 4 weeks for Trichophyton verrucosum. Cultures
are incubated at room temperature (20°C to 25°C [68°F to 77°F]) for at least 4 weeks before being finalized as no growth. Dermatophyte test medium is an alternative isolation medium that contains the pH indicator phenol red. The medium turns red when dermatophyte proteolytic activity increases the pH to 8 or above, and it remains amber with the growth of most saprophytes. Nondermatophyte acidic byproducts turn the medium yellow. Although dermatophyte test medium serves as a good alternative for isolation of dermatophytes, it may not allow for their direct identification because of altered growth, and thus morphology, of dermatophytes in dermatophyte test medium. Table 160-5 describes general microscopic features of microconidia and macroconidia of the 3 genera of dermatophytes, and Table 160-6 describes colony and microscopic features of the most common dermatophyte species. Identification of isolated fungi is facilitated by subculture on specific media such as potato dextrose agar or Borelli lactritmel agar that stimulate sporulation,
24
GENERA MICROCONIDIA MACROCONIDIA
Trichophyton Smooth walled; used for identification Absent or nondiagnostic
Microsporum Absent or nondiagnostic Rough walled; used for identification
Epidermophyton Absent Smooth walled; used for identification
Epidermophyton Absent Smooth walled; used for
identification
production of pigment and development of typical morphology. Finally, dermatophytes may be differentiated further by their ability to grow on autoclaved polished rice, perforate short strands of hair in vitro, hydrolyze urea (urease test), or require nutritional supplementation for growth (Table 160-7).
ORGANISM COLONY MORPHOLOGY
MICROSCOPIC APPEARANCE
Epidermophyton floccosum
Flat feathery colonies with a central fold and yellow to dull gray-green pigment. Yellow to brown reverse pigment.
Microsporum audouinii
Flat and white to gray with widely spaced radial grooves. Tan to salmon reverse pigment. Salmon-pink pigment on PDA. No growth on polished rice.
Microsporum canis
Flat, white to light yellow, coarsely hairy, with closely spaced radial grooves. Yellow to orange reverse pigment. Yellow on PDA. Growth on polished rice.
Microsporum gypseum
Flat and granular with tan to buff pigment, no reverse pigment.
Numerous thin and thick-walled, clubshaped macroconidia.
Terminal chlamydoconidia and pectinate (comb-like) hyphae.
Numerous thick walled and echinulate spindle shaped macroconidia with terminal knobs and more than 6 cells.
Numerous thin-walled pickle-shaped macroconidia without knobs and less than 6 cells.
2931
(Continued)
4
24
(Continued)
ORGANISM COLONY MORPHOLOGY
MICROSCOPIC APPEARANCE
Trichophyton interdigitale
White to creamy with a cottony, mounded surface. None to light brown reverse pigment. No pigment on PDA. Urease positive, which helps to distinguish it from Trichophyton rubrum.
Mounded white center with maroon periphery. Maroon reverse pigment. Cherry red on PDA. Urease negative.
Trichophyton rubrum
Trichophyton schoenleinii
Heaped or folded and whitish. Colorless to yellow-tan reverse pigment.
Suede-like center with feathery periphery, white to yellow or maroon color. Reverse pigment usually dark maroon, sometimes none to yellow. Partial thiamine requirement.
Trichophyton tonsurans
Trichophyton verrucosum
Small and heaped, although sometimes flat, white to yellow-gray. Reverse pigment none to yellow. Requires thiamine and usually inositol for growth.
Trichophyton violaceum
Trichophyton violaceum Waxy and heaped, deep purplish-red. Purple reverse pigment. Partial thiamine requirement.
Waxy and heaped, deep purplish-red.
Purple reverse pigment. Partial thiamine requirement.
PDA, potato dextrose agar; SDA, Sabouraud’s dextrose agar. Used with permission from David Ellis, PhD.
2932
Grape-like clusters of round microconidia, rare cigar-shaped macroconidia, occasional spiral hyphae. Hair perforation positive, which helps to distinguish it from T. rubrum.
Few tear-shaped microconidia, rare pencil-shaped macroconidia. Hair perforation negative.
Knobby antler-like hyphae (favic chandeliers), numerous chlamydoconidia.
Numerous multiform microconidia and rare cigar-shaped macroconidia.
Chains of chlamydoconidia on SDA. Long and thin “rat-tail” macroconidia with thiamine.
Irregular hyphae with intercalary
Irregular hyphae with intercalary chlamydoconidia. No micro- or macroconidia on SDA, rare micro- and macroconidia with thiamine.
chlamydoconidia. No micro- or macroconidia on SDA, rare microand macroconidia with thiamine.
Urease test Differentiates Trichophyton interdigitale (positive) from Trichophyton rubrum (negative)
Hair perforation test Differentiates T. interdigitale (positive) from T. rubrum (negative)
Nutritional requirement Differentiates Trichophyton species
Thiamine Trichophyton tonsurans
Trichophyton concentricum
Trichophyton violaceum
Thiamine + inositol Trichophyton verrucosum
Nicotinic acid Trichophyton equinum
Histidine Trichophyton megninii
Growth on polished rice Differentiates Microsporum species
Good growth Microsporum canis
Poor growth Microsporum audouinii
Microsporum distortum
Microsporum distortum
HISTOPATHOLOGY
HISTOPATHOLOGY
Skin biopsy is not often employed in the workup of typical dermatophytoses. Localized cutaneous eruptions suspected to represent dermatophytosis with equivocal KOH examination are often treated despite the lack of confirmation. Biopsy may confirm the diagnosis when a systemic agent is being considered for treatment of a recalcitrant or more widespread eruption. Biopsy may be used to aid in the diagnosis of Majocchi granuloma in which KOH examination of scale on the surface more often may be negative. Biopsy is also sometimes useful in confirming the presence of hyphae involving hair shafts on the scalp in tinea capitis, although culture is necessary to allow speciation of the pathogen. When present, hyphae may be appreciated in the stratum corneum on hematoxylin-and-eosin (H&E) staining. However special stains, most commonly periodic acid–Schiff (PAS) and methenamine silver stains, highlight hyphae that may otherwise be subtle in appearance on routine staining. Whereas culture is the most specific test for onychomycosis, PAS examination of nail clippings is the most sensitive and obviates the need to wait weeks for a result.35 Full-thickness nail clippings for H&E or culture should involve the dystrophic portion, as proximal from the distal edge as possible without causing injury.
WOOD LIGHT FLUORESCENCE
WOOD LIGHT
FLUORESCENCE
Examination of involved hair bearing areas, such as the scalp or beard, with a Wood lamp (365 nm) may
24
PATTERN DERMATOPHYTE FLUORESCENCE
Endothrix Trichophyton soudanense Trichophyton violaceum Trichophyton tonsurans Trichophyton gourvilii Trichophyton yaoundei
None
Ectothrix Microsporum canis Microsporum audouinii Microsporum distortum Microsporum ferrugineum
Yellow-green
Microsporum fulvum Microsporum gypseum None
Trichophyton megninii Trichophyton interdigitale Trichophyton rubrum Trichophyton verrucosum
None
Favus Trichophyton schoenleinii Blue-gray, occasional
Favus Trichophyton schoenleinii Blue-gray, occasional
reveal pteridine fluorescence of hair infected with particular fungal pathogens. Hairs that fluoresce should be selected for further examination, including culture. Although ectothrix organisms M. canis and M. audouinii will fluoresce on Wood light examination, the endothrix organism T. tonsurans will not fluoresce. T. tonsurans, which is now the most common cause of tinea capitis in the United States, thus limits the use of Wood light examination. Table 160-8 lists common patterns of dermatophyte hair involvement and fluorescence.
MANAGEMENT
CLINICAL COURSE AND PROGNOSIS
The clinical course of dermatophytosis varies according to pathogen and host factors. As discussed before, some dermatophytes are able to evade or suppress host immune function, and some hosts are unable to mount an effective immune response to clear infection. As such, the severity of each infection is variable according to the combination of these factors.
2933
4
24
DISEASE TOPICAL TREATMENT SYSTEMIC TREATMENT
Tinea capitis (requires systemic treatment)
Only as adjuvant Selenium sulfide 1% or 2.5% Zinc pyrithione 1% or 2% Povidone-iodine 2.5% Ketoconazole 2%
Tinea barbae (requires systemic treatment) Only as adjuvant Zinc pyrithione 1% or 2% Povidone-iodine 2.5%
Tinea corporis/cruris
Allylamines Imidazoles Tolnaftate Butenafine Ciclopirox Gentian violet
Tinea pedis/manuum
Allylamine Imidazoles Ciclopirox Benzylamine Tolnaftate Undecenoic acid
Onychomycosis Ciclopirox Amorolfine Tioconazole Efinaconazole
Onychomycosis
Ciclopirox Amorolfine Tioconazole Efinaconazole
2934
Adults
■Griseofulvin, 20 to 25 mg/kg/day × 6 to 8 weeks
■Terbinafine, 250 mg/day × 2 to 8 weeks
■Itraconazole, 5 mg/kg/day × 2 to 4 weeks
■Fluconazole, 6 mg/kg/day × 3 to 6 weeks Children
■Griseofulvin, daily × 6 to 8 weeks
■Age 1 month to 2 years: 10 mg/kg/day
■Age ≥2 years: 20 to 25 mg/kg/day (micro)
■Age ≥2 years: 10 to 15 mg/kg/day (ultramicro)
■Terbinafine daily × 2 to 4 weeks
■Weight <20 kg: 62.5 mg/day
■Weight 20 to 40 kg: 125 mg/day
■Weight >40 kg: 250 mg/day
■Itraconazole
■3 to 5 mg/kg/day × 2 to 4 weeks
■5 mg/kg/day × 1 week/month × 2 to 3 months
■Fluconazole (not standard therapy)
■6 mg/kg/day × 3 to 6 weeks
■6 mg/kg once weekly × 8 to 12 weeks
■Griseofulvin 1 g/day × 6 weeks
■Terbinafine 250 mg/day × 2 to 4 weeks
■Itraconazole 200 mg/day × 2 to 4 weeks
■Fluconazole 200 mg/day × 4 to 6 weeks
Adults
■Terbinafine 250 mg/day × 2 to 4 weeks
■Itraconazole 100 mg/day × 1 week
■Fluconazole 150 to 300 mg/day × 4 to 6 weeks
■Griseofulvin 500 mg/day × 2 to 4 weeks Children
■Terbinafine 3 to 6 mg/kg/day × 2 weeks
■Itraconazole 5 mg/kg/day × 1 week
■Griseofulvin 10 to 20 mg/kg/day × 2 to 4 weeks
Adults
■Terbinafine 250 mg/day × 2 weeks
■Itraconazole 200 mg twice daily × 1 week
■Fluconazole 150 mg/week × 3 to 4 weeks Children
■Terbinafine 3 to 6 mg/kg/day × 2 weeks
■Itraconazole 5 mg/kg/day × 2 weeks
Adults
Adults
■Terbinafine 250 mg/day × 6 to 12 weeks
■Terbinafine 250 mg/day × 6 to 12 weeks
■Itraconazole 200 mg/day × 2 to 3 months, or
■Itraconazole 200 mg/day × 2 to 3 months, or
■Pulse 400 mg daily × 1 week/month × 2 to 3 months
■Pulse 400 mg daily × 1 week/month × 2 to 3 months
■Fluconazole 150 to 300 mg/week × 3 to 12 months Children
■Fluconazole 150 to 300 mg/week × 3 to 12 months Children
■Terbinafine daily × 6 to 12 weeks
■Terbinafine daily × 6 to 12 weeks
■Weight 10 to 20 kg: 62.5 mg/day
■Weight 10 to 20 kg: 62.5 mg/day
■Weight 20 to 40 kg: 125 mg/day
■Weight 20 to 40 kg: 125 mg/day
■Weight >40 kg: 250 mg/day
■Weight >40 kg: 250 mg/day
■Itraconazole 1 week/month × 2 to 3 months
■Itraconazole 1 week/month × 2 to 3 months
■Weight <20 kg: 5 mg/kg/day
■Weight <20 kg: 5 mg/kg/day
■Weight 20 to 40 kg: 100 mg/day
■Weight 20 to 40 kg: 100 mg/day
■Weight 40 to 50 kg: 200 mg/day
■Weight 40 to 50 kg: 200 mg/day
■Weight >50 kg: 200 mg twice daily
■Weight >50 kg: 200 mg twice daily
■Fluconazole 3 to 6 mg/kg/week × 3 to 6 months
■Fluconazole 3 to 6 mg/kg/week × 3 to 6 months
24
MEDICATION DRUG CLASS INDICATIONS WARNINGS/MONITORING
Fluconazole Triazole Onychomycosis Tinea barbae Tinea capitis Tinea corporis/cruris Tinea pedis/manuum
Adverse effects: headache, GI upset Caution: liver and/or renal impairment Contraindications: pregnancy, concurrent QT-prolonging medications Monitor liver function tests, basic metabolic panel, complete blood cell count; pregnancy test prior to start in females Pregnancy category D
Griseofulvin Inhibits fungal mitosis Tinea barbae Tinea capitis (first-line Microsporum) Tinea corporis/cruris Tinea pedis/manuum
Adverse effects: headache, GI upset Caution: liver impairment Contraindications: porphyria, pregnancy, hepatic failure Check pregnancy test prior to start in females Pregnancy category X
Itraconazole Triazole Onychomycosis Tinea barbae Tinea capitis Tinea corporis/cruris Tinea pedis/manuum
Adverse effects: headache, GI upset Caution/contraindication: cardiac failure, hepatotoxicity Monitor liver function tests, basic metabolic panel, complete blood cell count baseline and at 1 month Check pregnancy test prior to start in females Pregnancy category C
Adverse effects: GI upset, taste disturbance, elevation of liver enzymes Risk of hepatotoxicity Monitor liver function tests baseline and at 1 month Pregnancy category B
Terbinafine Allylamine Onychomycosis (first-line) Tinea barbae Tinea capitis Tinea corporis/cruris Tinea pedis/manuum
Terbinafine Allylamine Onychomycosis (first-line) Tinea barbae Tinea capitis Tinea corporis/cruris Tinea pedis/manuum
Adverse effects: GI upset, taste disturbance, elevation of liver enzymes Risk of hepatotoxicity Monitor liver function tests baseline and at 1 month Pregnancy category B
MEDICATION CLASS/MECHANISM FORMULATION USE ADMINISTRATION WARNING/PRECAUTIONS
Amorolfine Morpholine Liquid, 250 mg/ 5 mL
Onychomycosis (dermatophyte or Candida) treatment and/or relapse prophylaxis
Apply 1 to 2 times/week after gentle nail filing × 6 to 12 months
Not available in the United States
Butenafine Synthetic allylamine Cream, 1% Tinea corporis, cruris, pedis, versicolor Apply 1 to 2 times daily for 1 to 4 weeks Pregnancy category C Children ≥12 years of age
Ciclopirox Inhibits DNA, RNA, and protein synthesis
Cream, 0.77% Suspension, 0.77% Gel, 0.77%
Tinea corporis, cruris, pedis, versicolor; cutaneous Candida; seborrheic dermatitis
Apply twice daily Pregnancy category B Cream and suspension, children >10 years of age Gel and shampoo, children >16 years of age Solution, children ≥12 years of age
Shampoo, 0.1% Seborrheic dermatitis Apply, wait 5 to 10 minutes prior to rinsing; use 2 to 3 times/week to treat, 1 to 2 times/week to maintain
Solution, 8% Onychomycosis Apply to nail and surrounding skin at bedtime × 7 days, then remove with rubbing alcohol and repeat
Clotrimazole Imidazole Cream, 1% Ointment, 1% Solution, 1%
Tinea corporis, cruris, pedis, versicolor Apply twice daily × 1 to 4 weeks Pregnancy category B
Econazole Imidazole Cream, 1% Foam, 1% Tinea corporis, cruris, pedis, versicolor Apply 1 to 2 times daily × 2 to 4 weeks Pregnancy category C Children ≥12 years of age
(Continued)
2935
4
24
(Continued)
MEDICATION CLASS/MECHANISM FORMULATION USE ADMINISTRATION WARNING/PRECAUTIONS
Efinaconazole Triazole Solution, 10% Onychomycosis Apply daily × 48 weeks Pregnancy category C
Gentian violet Antifungal Antibiotic Solution, 1% and 2% Superficial cutaneous infections, effective against some Gram+ bacteria (Staphyloccocus sp.), fungi, some yeasts
Ketoconazole Imidazole Cream, 2% Foam, 2% Gel, 2%
Apply 1 to 2 times daily Pregnancy category not classified Stains skin and clothing May tattoo open wounds
Tinea corporis, cruris, pedis, versicolor; cutaneous Candida; seborrheic dermatitis
Apply 1 to 2 times daily Pregnancy category C Children ≥12 years of age
Shampoo, 1% and 2% Tinea capitis adjuvant, tinea versicolor, seborrheic dermatitis
Miconazole Imidazole Aerosol, 2% Cream, 2% Lotion, 2% Ointment, 2% Powder, 2% Solution, 2%
Apply, wait 5 to 10 mins prior to rinsing; use 2 to 3 times/ week to treat, 1 to 2 times/ week as prophylaxis
Tinea corporis, cruris, pedis Apply twice daily × 4 weeks Pregnancy category not classified Children ≥2 years of age May increase serum concentration of vitamin K agonist
Povidineiodine Broad-spectrum germicidal agent Wash, 7.5% Shampoo, 7.5% Tinea capitis and barbae adjuvant, seborrheic dermatitis
Selenium sulfide Cytostatic effects on keratinocytes Foam, 2.25% Lotion, 2.25% Shampoo, 1% and 2.3%
Use twice weekly until controlled, then once weekly Pregnancy category C Use with caution in children Hypersensitivity to iodine contraindication
Tinea capitis adjuvant, tinea versicolor, seborrheic dermatitis
Terbinafine Allylamine Cream, 1% Gel, 1% Solution, 1%
Foam: twice daily Lotion: Apply, rinse after 10 minutes once daily × 1 week, then once monthly × 3 months
Pregnancy category C Children ≥2 years of age
Shampoo: Apply, wait 5 to 10 mins prior to rinsing; use 2 to 3 times/week to treat, 1 to 2 times/week as prophylaxis
Tinea corporis, cruris, pedis, versicolor; cutaneous candidiasis
Apply 1 to 2 times daily × 1 to 2 weeks Pregnancy category not classified Children ≥12 years of age
Tioconazole Imidazole Solution, 28% Onychomycosis Apply twice daily × 6 to 12 months Not available in the United States Possible allergic contact dermatitis
Tolnaftate Distorts hyphae and mycelial growth Aerosol, 1% Cream, 1% Lotion, 1% Powder, 1% Solution, 1%
Tinea corporis, cruris, pedis Apply twice daily × 2 to 4 weeks Pregnancy category not classified Children ≥2 years of age
Zinc
Keratolytic Bar, 2% Liquid/wash,
Tinea capitis and bar-
Zinc pyrithione Keratolytic Bar, 2% Liquid/wash, 0.5% Shampoo, 2%
Use at least 2 times/week Pregnancy category C
Tinea capitis and barbae adjuvant; seborrheic dermatitis
pyrithione
Use at least 2 times/week Pregnancy category C
bae adjuvant; seborrheic dermatitis
0.5% Shampoo, 2%
2936
DERMATOPHYTOSES
DERMATOPHYTID (ID) REACTION
DERMATOPHYTID (ID)
REACTION
A dermatophytid (or id) reaction is an inflammatory dermatitis occurring at sites distant from the primary dermatophytosis (such as tinea pedis or kerion) in 4% to 5% of patients.39 Although the precise mechanism is unknown, the id reaction is associated with a delayedtype hypersensitivity response to the Trichophyton test, and so may involve a local delayed-type hypersensitivity response to systemically absorbed fungal antigen.40 Id reactions appear polymorphic, ranging in morphology from follicular or nonfollicular papules and vesicles of the hands and feet to reactive erythemas including erythema nodosum, erythema annulare centrifugum, or urticaria.41-44 Unlike the primary eruption, the id eruption is both KOH examination negative and culture negative. The 3 criteria for establishing the presence of an id eruption are (a) dermatophytosis on another part of body, (b) absence of fungal elements from the id eruption, and (c) resolution of the id eruption with clearing of the primary dermatophyte infection.
ONYCHOMYCOSIS
ONYCHOMYCOSIS
Onychomycosis describes fungal infection of the nail caused by dermatophytes, nondermatophyte molds, or yeasts. Tinea unguium refers strictly to dermatophyte infection of the nail. Clinically, 3 types of onychomycosis are distinguished: (a) distolateral subungual onychomycosis (DLSO), (b) proximal subungual onychomycosis (PSO), and (c) white superficial onychomycosis (WSO).
EPIDEMIOLOGY
Onychomycosis is the most prevalent nail disease and accounts for approximately 50% of all causes of onychodystrophy. It affects up to 14% of the population, with both an increasing prevalence45 and an overall increasing incidence among older individuals.46 Onychomycosis is also increasing in incidence among children and adolescents, and accounts for up to 20% of dermatophyte infections diagnosed in children.47 Risk factors for nail infection include age, male sex, nail trauma, immunosuppression (including HIV infection and diabetes mellitus), and peripheral vascular insufficiency.48 Patients with HIV and with a CD4 T-lymphocyte count of less than 400 cells/µL (reference range: 1200 to 1400 cells/µL) and who are on immunosuppressants or have defective polymorphonuclear chemotaxis have an increased risk of onychomycosis, which tends to be more widespread and involve all 20 nails.36
The increasing prevalence of onychomycosis may be secondary to wearing of tight shoes, increasing
24
numbers of individuals on immunosuppressive drugs and with diabetes mellitus, and an increased use of communal locker rooms. The dermatophytosis commonly begins as tinea pedis before extending to the nail bed, where eradication is more difficult. This site serves as a reservoir for local recurrence or for infections spreading to other areas. Up to 40% of patients with toenail onychomycosis show concomitant skin infections, most commonly tinea pedis (30%).49
CLINICAL FEATURES
Distolateral Subungual Type: DLSO is the most common form of onychomycosis. It begins with invasion of the stratum corneum of the hyponychium and distal nail bed, forming a whitish to brownish–yellow opacification at the distal edge of the nail (Fig. 160-3A). The infection then spreads proximally up the nail bed to the ventral nail plate. Hyperproliferation (or altered differentiation) of the nail bed in response to the infection results in subungual hyperkeratosis, while progressive invasion of the nail plate results in an increasingly dystrophic nail.
Proximal Subungual Type: PSO (see Fig. 160-3B) results from infection of the proximal nailfold primarily with T. rubrum and Trichophyton megninii and is apparent as a white-to-beige opacity on the proximal nail plate. This opacity gradually enlarges to affect the entire nail and eventuates in subungual hyperkeratosis, leukonychia, proximal onycholysis, and/or destruction of the entire nail. Patients with PSO should be screened for HIV, as it has been identified as an a marker for this disease.6,50
White Superficial Type: WSO (see Fig. 160-3C) results from direct invasion of the dorsal nail plate resulting in white to dull yellow, sharply bordered patches anywhere on the surface of the toenail. It is usually caused by T. interdigitale, although nondermatophyte molds such as Aspergillus, Scopulariopsis, and Fusarium are also known pathogens. Candida species may invade the hyponychial epithelium to eventually affect the entire thickness of the nail plate.51
Other Clinical Presentations: Total dystrophy of the nail may result from almost complete destruction of the nail plate secondary to any of the foregoing varieties of onychomycosis; this is known as total dystrophic onychomycosis.36 Primary total dystrophic onychomycosis is rare, usually caused by Candida, and typically affects immunocompromised patients.36 Multiple patterns of onychomycosis may present in the same individual, most commonly with the combination of PSO with WSO or DLSO with WSO.36 Secondary bacterial infection of the nail is possible. Infection with Pseudomonas aeruginosa presents as a green or black discoloration under the nail. It is also possible to have mixed infections with both a dermatophyte and yeast form, such as Candida.
2937
4
24
Onychomycosis
Distolateral subungual type Trichophyton rubrum,a Trichophyton interdigitale
Proximal subungual type Trichophyton rubrum, Trichophyton megninii
White superficial type Trichophyton interdigitale (also the following nondermatophytes: Aspergillus, Scopulariopsis, Fusarium, Candida sp.)
Total dystrophic onychomycosis Candida sp.
Tinea Barbae
Superficial type Trichophyton violaceum
Inflammatory type Trichophyton interdigitale
Tinea Capitis
Inflammatory Microsporum audouinii, Microsporum canis, Microsporum gypseum, Microsporum nanum, Trichophyton interdigitale, Trichophyton schoenleinii, Trichophyton tonsurans, Trichophyton verrucosum
Noninflammatory Microsporum audouinii, Microsporum canis, Microsporum ferrugineum, Trichophyton tonsurans
Black dot Trichophyton tonsurans, Trichophyton violaceum
Favus Trichophyton schoenleinii, Trichophyton violaceum, Trichophyton mentagrophytes
Tinea Corporis
Tinea Corporis Adults: Trichophyton rubrum Children: Microsporum canis
Tinea incognito Trichophyton rubrum
Majocchi’s granuloma Trichophyton rubrum, Trichophyton interdigitale, Microsporum canis
Tinea imbricata Trichophyton concentricum
Tinea cruris Trichophyton rubrum, Epidermophyton floccosum, Trichophyton interdigitale, Trichophyton verrucosum
Tinea nigra Hortaea werneckii
Tinea Pedis
Interdigital type Trichophyton rubrum, Trichophyton interdigitale, Epidermophyton floccosum
Chronic hyperkeratotic (moccasin) type Trichophyton rubrum, Epidermophyton floccosum
Vesicobullous type Trichophyton interdigitale (usually zoophilic strains)
Adult ulcerative type Trichophyton interdigitale (zoophilic strains) with combined Gram-negative bacterial superinfection
Tinea Manuum
Tinea manuum Trichophyton rubrum, Trichophyton interdigi-
Tinea manuum Trichophyton rubrum, Trichophyton interdigitale, Epidermophyton floccosum
tale, Epidermophyton floccosum
aA single dermatophyte may have more than one presentation.
2938
A
B
C
ETIOLOGY AND PATHOGENESIS
In the majority of cases, onychomycosis is caused by dermatophytes, with T. rubrum and T. interdigitale responsible for approximately 90% of all cases. T. tonsurans and E. floccosum are also well-documented causative agents.52 Yeast and nondermatophyte molds such as Acremonium, Aspergillus, Fusarium, Scopulariopsis brevicaulis, and Scytalidium are the source of approximately 10% of toenail onychomycosis. Interestingly, Candida species are responsible for up to 30% of fingernail cases, whereas nondermatophyte molds were not
detected in diseased fingernails.53 Candida (and irritant dermatitis) may also cause chronic paronychia. Risk factors for onychomycosis include increasing age, male sex, peripheral vascular disease, trauma, hyperhidrosis, and immunosuppressed states, including HIV, diabetes mellitus, and medication-induced immunosuppression.36 In children, onychomycosis may be responsible for up to 15% of onychodystrophies.36 As in adults, prevalence increases with age and may be associated with occlusive footwear.
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
24
Most Likely
■Psoriasis, lichen planus, chronic trauma, onychogryphosis
Consider
■Pachyonychia congenita, acquired and congenital leukonychias, Darier-White disease, yellow nail syndrome
Rule Out
Rule Out
■Melanoma
■Melanoma
MANAGEMENT
Systemic Therapy: An oral antifungal (see Table 160-10) is required for onychomycosis involving the matrix area, or when a shorter treatment regimen or higher chance for clearance/cure is desired. Selection of the antifungal agent should be based on the causative organism, potential adverse effects, risk of drug interactions, and comorbidities in each patient. Of note, griseofulvin is no longer considered standard treatment for onychomycosis because of its prolonged treatment course, potential for adverse effects and drug interactions, and its relatively low cure rates.
Topical Therapy: In patients with distal nail involvement, WSO, and/or contraindication for systemic treatment, topical therapy (see Table 160-11) should be considered. Combination therapy regimens may have a higher clearance rate than either oral or topical treatments alone. Studies have been performed using combination therapy regimens with topical tioconazole, ciclopirox, and amorolfine with mixed results.36,56,57 In vitro fungicidal activity demonstrated by thymol, camphor, menthol, and oil of Eucalyptus citriodora offers the potential for additional therapeutic strategies to treat onychomycosis.58,59 Thymol 4% prepared in ethanol may be used as drops applied to the nail plate and hyponychium. The application to nails of commercially available topical preparations with thymol, such as Vicks VapoRub, has anecdotally led to success. Topical therapy may be useful as a means to prevent recurrence.
Mechanical Intervention: Trimming, debridement, nail bed curettage, and nail abrasion may speed delivery of medications to the site of action. Other options for refractory cases include laser, surgical avulsion, or chemical removal of the nail with 40%
2939
4
24
urea compounds in combination with topical or oral antifungals.
PIEDRA
PIEDRA
Piedra is an asymptomatic superficial fungal infection of the hair shaft also known as trichomycosis nodularis. Black piedra is caused by Piedraia hortae, whereas white piedra is caused by pathogenic species of the Trichosporon genus, namely Trichosporon asahii, Trichosporon ovoides, Trichosporon inkin, Trichosporon mucoides, Trichosporon asteroides, and Trichosporon cutaneum.60
EPIDEMIOLOGY
Black piedra is seen commonly in humans and primates of tropical areas of South America, the Pacific Islands, and the Far East, and less commonly in Africa and Asia. P. hortae is present in the soil, stagnant water, and crops. Scalp hair is most often affected. In fact, infection is encouraged for religious and esthetic reasons by some indigenous cultures.61
White piedra is most common in temperate and semitropical climates of South America and Asia, the Middle East, India, Africa, and Japan. It occurs infrequently in the United States and Europe. White piedra affects facial, axillary, and genital hair more commonly than scalp hair. T. ovoides is found more commonly on scalp hair, T. inkin on pubic hair, and T. asahii on other body surfaces. Person-to-person transmission is rare, and infection is not associated with travel to endemic areas.62
CLINICAL FINDINGS
Black piedra is characterized by firmly attached, hard or gritty, brown-black–colored concretions on the hair shaft that vary in size from the microscopic range to a few millimeters in size. Concretions are most commonly noted on frontal portions of the scalp. Black piedra weakens the hair shaft and results in hair breakage. White piedra consists of softer and less-adherent whitish to beige–colored concretions that are discrete or may coalesce into sleeve-like structures along the hair shaft. These concretions affect the outer layers of the hair shaft and may be easily detached. Broken hairs, although sometimes present, are less common than in black piedra.60
DIAGNOSIS
Nodules of black piedra examined by KOH preparation display a periphery of aligned hyphae and a wellorganized center of thick-walled cells packed closely together, sometimes termed pseudoparenchyma. These nodules are mostly outside of the hair shaft. P. hortae grows well, albeit slowly, on most laboratory media and is uninhibited by cycloheximide. The nodules of white piedra have a less organized and more intrapilar
2940
Most Likely
■Pediculosis, trichomycosis axillaris, tinea capitis
Consider
Consider
■Monilethrix
■Monilethrix
appearance than do nodules of black piedra. Hyphae are arranged perpendicularly to the hair shaft. T. asahii thrives on SDA and it is inhibited by cycloheximide. Microscopy readily differentiates piedra from nits, hair casts, developmental hair shaft defects, and trichomycosis axillaris. In addition, the nodules of trichomycosis axillaris are usually smaller and may fluoresce under a Wood lamp.
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
Shaving the infected hair is curative and represents the best treatment of both black and white piedra, although this approach should be supplemented with a topical azole preparation (see Table 160-11). Because of high relapse rates, as well as evidence for intrafollicular organisms in white piedra, some advocate the use of a systemic antifungal agent such as itraconazole.62
TINEA BARBAE
TINEA BARBAE
EPIDEMIOLOGY
Tinea barbae, as its name would imply, occurs predominantly in the beard area of males. The incidence of tinea barbae has decreased as improved sanitation has reduced transmission by contaminated barbers’ razors. Direct exposure to cattle, horses, or dogs is now the more common mode of acquisition, and thus accounts for a shift in prevalence toward farmers or ranchers in rural settings.
CLINICAL FINDINGS
Superficial Type: Caused by anthropophilics such as T. violaceum, this form of tinea barbae is less
24
A B
inflammatory and resembles tinea corporis or bacterial folliculitis. The active border shows perifollicular papules and pustules accompanied by mild erythema (Fig. 160-4A). Alopecia, if present, is reversible.
Inflammatory Type: Usually caused by T. interdigitale (zoophilic strains) or T. verrucosum, inflammatory tinea barbae is the most common clinical presentation. It presents analogously to kerion formation in tinea capitis with boggy-crusted plaques and a seropurulent discharge (see Fig. 160-4B). Hairs are lusterless, brittle, and easily epilated to demonstrate a purulent mass around the root. Perifollicular pustules may coalesce and eventuate in abscess-like collections of pus, sinus tracts, and scarring alopecia.
ETIOLOGY AND PATHOGENESIS
Tinea barbae is most commonly caused by the zoophilic strains of T. interdigitale (formerly named Trichophyton mentagrophytes var. mentagrophytes), T. verrucosum, and, less commonly, M. canis. Among the anthropophilic organisms, Trichophyton schoenleinii, T. violaceum, and certain strains of T. rubrum (formerly named T. megninii) cause tinea barbae in endemic areas.63
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
TINEA CAPITIS
TINEA CAPITIS
Tinea capitis describes a dermatophyte infection of hair and scalp typically caused by Trichophyton and Microsporum species, with the exception of Trichophyton concentricum.
EPIDEMIOLOGY
Tinea capitis is most commonly observed in children between the ages of 3 and 14 years.37 The fungistatic effect of fatty acids in sebum may help to explain the sharp decrease in incidence after puberty.64 Overall prevalence of the carrier state is approximately 4% in the United States, with a peak prevalence of approximately 13% in girls of sub-Saharan African American descent.65
Most Likely
■Bacterial folliculitis (sycosis vulgaris), pseudofolliculitis barbae, acne vulgaris, rosacea, contact dermatitis, perioral dermatitis, candidal folliculitis
Rule Out
Rule Out
2941
■Herpes simplex, halogenoderma
■Herpes simplex, halogenoderma
4
24
For unknown reasons, tinea capitis is generally more common among children of African descent. Transmission is increased with decreased personal hygiene, overcrowding, and low socioeconomic status. The anthropophilic dermatophyte T. tonsurans is the most prevalent species found in the United States and United Kingdom, while M. canis remains the most common cause of tinea capitis in Europe.37,66 Organisms responsible for tinea capitis have been cultured from fomites such as combs, caps, pillowcases, toys, and theater seats. Even after shedding, hairs may harbor infectious organisms for more than 1 year.67 The high prevalence of asymptomatic carriers thwarts eradication of the disease.
CLINICAL FINDINGS
Noninflammatory Type: Also called the seborrheic form of tinea capitis (because scale is the predominant feature),68 noninflammatory tinea capitis is seen most commonly with anthropophilic organisms such as M. audouinii or Microsporum ferrugineum. Arthroconidia may form a sheath around affected hairs, turning them gray and causing them to break off just above the level of the scalp. Alopecia may be imperceptible or, in more inflammatory cases, may have circumscribed erythematous scaly patches of nonscarring alopecia with breakage of hairs (“gray patch” type; Fig. 160-5). Patches often occur on the occiput.67 When involving an ectothrix pattern, infected hairs may exhibit green fluorescence under Wood light (see Table 160-8).
“Black Dot” Tinea Capitis: The “black dot” form of tinea capitis (Fig. 160-6) is typically caused by the anthropophilic endothrix organisms T. tonsurans and T. violaceum. Hairs broken off at the level of the scalp leave behind grouped black dots within patches of polygonal-shaped alopecia with finger-like margins. Normal hairs also remain within patches of broken hairs. Diffuse scaling is also often present. Even though “black dot” tinea capitis tends to be minimally inflammatory, some patients may develop follicular pustules, furuncle-like nodules, or, in rare cases, kerion—a boggy, inflammatory mass studded with broken hairs and follicular orifices oozing with pus.69
Inflammatory Type: Zoophilic or geophilic pathogens, such as M. canis, M. gypseum, and T. verrucosum, are more likely to cause an inflammatory type of tinea capitis via a hypersensitivity reaction. Resultant inflammation ranges from follicular pustules to furunculosis (Fig. 160-7) or kerion (Fig. 160-8). Intense inflammation may also result in scarring alopecia. The scalp is usually pruritic or tender. Posterior cervical lymphadenopathy is often present, and may serve as a
2942
clinical pearl in differentiating tinea capitis from other inflammatory disorders involving the scalp.
DIAGNOSIS
mid- to late-anagen hairs before descending into the follicle to penetrate the cortex. With hair growth, the infected part of the hair rises above the surface of the scalp where it may break because of its increased fragility. In ectothrix infections (see Fig. 160-2), although hyphae are also present within the hair shaft, only the arthroconidia on the surface of the hair shaft may be visualized and the cuticle is destroyed. On Wood lamp examination, a yellow-green fluorescence may be detected, depending on the causative organism. In endothrix infections (see Fig. 160-2), arthroconidia and hyphae remain within the hair shaft and leave the cortex and
24
cuticle intact. This pattern of tinea capitis is associated with the appearance of “black dots,” which represent broken hairs at the surface of the scalp. Endothrix organisms do not show fluorescence on Wood lamp examination. Favus is characterized by longitudinally arranged hyphae and air spaces within the hair shaft. Arthroconidia are not usually noted in infected hairs of favus. On histopathology of tinea capitis, PAS and methenamine silver stains readily reveal hyphae around and within hair shafts. The dermis demonstrates a perifollicular mixed cell infiltrate with lymphocytes, histiocytes, plasma cells, and eosinophils. Follicular disruption leads to an adjacent foreign-body giant cell reaction. Markedly inflammatory lesions, such as a kerion, demonstrate an acute infiltrate of polymorphonuclear leukocytes within the dermis and follicle.70 Organisms may not be visualized in kerion because the intense host response destroys many of the fungal organisms. However, fungal antigens may be detectable with immunofluorescent techniques.71
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
Adjuvant Therapy: Selenium sulfide (1% and 2.5%), zinc pyrithione (1% and 2%), povidone-iodine (2.5%), and ketoconazole (2%) are shampoo preparations that help eradicate dermatophytes from the scalp. Adjunctive use of these shampoos is recommended 2 to 4 times weekly for 2 to 4 weeks.72 The thrice weekly use
Most Likely
■Seborrheic dermatitis, contact dermatitis, pustular or plaque psoriasis, atopic dermatitis, bacterial pyodermas, folliculitis decalvans, lichen planopilaris, and dissecting cellulitis of the scalp
Consider
■Alopecia areata, trichotillomania, pseudopelade, psoriasiform reaction to tumor necrosis factor-α inhibitor
Rule Out
Rule Out
2943
■Discoid lupus erythematosus, syphilis
■Discoid lupus erythematosus, syphilis
4
24
of ketoconazole 2% shampoo or selenium sulfide 2.5% by all household members also reduces transmission by decreasing the shedding of spores.73 Oral glucocorticoids may reduce the incidence of scarring associated with markedly inflammatory varieties of tinea capitis. Although there is no consistent evidence for improved cure rates with use of oral glucocorticoids, they appear to relieve pain and swelling associated with infections. The usual regimen is prednisone 1 to 2 mg/kg each morning during the first week of therapy.
TINEA CORPORIS
TINEA CORPORIS
Tinea corporis refers to any dermatophytosis of glabrous skin except palms, soles, and the groin.
EPIDEMIOLOGY
Tinea corporis may be transmitted directly from infected humans or animals, via fomites, or it may occur via autoinoculation from reservoirs of dermatophyte colonization on the feet.74 Children are more likely to contract zoophilic pathogens, especially M. canis, from dogs or cats. Occlusive clothing and a humid climate are associated with more frequent and severe eruptions.75 Wearing of occlusive clothing, frequent skin-to-skin contact, and minor traumas, such as the mat burns in competitive wrestling, create an environment in which dermatophytes flourish. “Tinea corporis gladiatorum” is caused most commonly by T. tonsurans, and it occurs most frequently on the head, neck, and arms.76
CLINICAL FINDINGS
2944
A
B
C
ETIOLOGY AND PATHOGENESIS
Although any dermatophyte can cause tinea corporis, it is caused most commonly caused by T. rubrum, which is also the most likely candidate in cases with
concomitant follicular involvement.69 E. floccosum, T. interdigitale (anthropophilic and zoophilic strains), M. canis, and T. tonsurans are also common pathogens.1
Tinea imbricata, caused by T. concentricum, is limited geographically to areas of the Far East, South Pacific, and South and Central America.
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
Most Likely
■Erythema annulare centrifugum, nummular eczema, psoriasis, tinea versicolor, subacute cutaneous lupus erythematosus, cutaneous candidiasis
Consider
■Contact dermatitis, atopic dermatitis, pityriasis rosea, seborrheic dermatitis
Rule Out
Rule Out
■Mycosis fungoides, parapsoriasis, secondary syphilis
■Mycosis fungoides, parapsoriasis, secondary syphilis
24
tolnaftate, butenafine, and ciclopirox are effective. Most are applied twice daily for 2 to 4 weeks. Oral antifungal agents are reserved for widespread or more inflammatory eruptions.
TINEA CRURIS
TINEA CRURIS
Tinea cruris is a dermatophytosis of the groin, genitalia, pubic area, and perineal and perianal skin. The designation is a misnomer, because in Latin, “cruris” means “of the leg.” It is the second-most common type of dermatophytosis worldwide.
EPIDEMIOLOGY
Much like tinea corporis, tinea cruris spreads via direct contact or fomites, and is exacerbated by occlusion and humidity. Autoinfection from distant reservoirs of T. rubrum or T. interdigitale on the feet, for example, is common.74 Tinea cruris is 3 times more common in men, and adults are affected more often than children.
CLINICAL FINDINGS
Tinea cruris presents classically as a well-marginated annular plaque with a scaly raised border that extends from the inguinal fold to the inner thigh, often bilaterally. Presentation with erythematous, scaly patches with papules and vesicles involving the inner thighs is also common but perhaps less obvious. Pruritus is common, as is pain when plaques are macerated or secondarily infected. Plaques in tinea cruris caused by E. floccosum are more likely to demonstrate central clearing with involvement of the genitocrural crease and medial upper thigh. In contrast, plaques in tinea cruris caused by T. rubrum coalesce with extension to the pubic, perianal, buttock, and lower abdominal areas (Fig. 160-11). Genitalia (including the scrotum)
2945
4
24
Most Likely
■Erythrasma, cutaneous candidiasis, intertrigo, contact dermatitis, inverse psoriasis, seborrheic dermatitis, lichen simplex chronicus, folliculitis
Consider
Consider
■Familial benign pemphigus, Darier-White disease, histiocytosis
■Familial benign pemphigus, Darier-White disease, histiocytosis
are infrequently affected and may be useful to distinguish from other conditions such as inverse psoriasis.63
ETIOLOGY AND PATHOGENESIS
Most tinea cruris is caused by T. rubrum and E. floccosum, the latter being most often responsible for epidemics.63 T. interdigitale and T. verrucosum are implicated less often.
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
Medical treatment of tinea cruris is the same as that for tinea corporis, which is discussed earlier. In addition to medical treatment, it also may be helpful to correct any underlying moisture issues in the affected area (with use of loose-fitted clothing and regular application of barrier-protective zinc-containing cream) or other areas of infection (eg, tinea pedis). If tinea pedis is present, in addition to medical treatment targeting the feet, one might also recommend the patient apply socks before underwear so as to prevent autoinoculation of the area.
TINEA FAVOSA
TINEA FAVOSA
Tinea favosa or favus (Latin for “honeycomb”) is a chronic dermatophyte infection of the scalp that rarely involves glabrous skin and/or nails, and is characterized by thick yellow crusts (scutula) within the hair follicles that lead to scarring alopecia.
EPIDEMIOLOGY
Favus is usually acquired before adolescence, but may extend into adulthood.78 It is associated with
2946
malnutrition and poor hygiene. Over the last century, favus has become geographically limited and is now seen almost exclusively in Africa, the Middle East, and parts of South America. Even these regions have had a dramatic decrease in incidence with studies from South Africa, Libya, and Arabia suggesting disappearance of favus over the last few decades.79-81
CLINICAL FINDINGS
During the first 3 weeks of infection, early favus is characterized by patchy perifollicular erythema with slight scaling and matting of the hair. Progressive hyphal invasion distends the follicle, first producing a yellow-red follicular papule, then a yellow concave crust (scutulum) around a single dry hair (Fig. 160-12) that is less brittle than hair of endothrix infections. The scutulum may reach 1 cm in diameter, engulfing surrounding hairs, and coalescing with other scutula to form large, adherent mats with an unpleasant cheeselike or musky odor. Over several years, the plaques advance peripherally leaving behind central, atrophic areas of alopecia.63
ETIOLOGY AND PATHOGENESIS
T. schoenleinii is the most common cause of human favus, with T. violaceum and M. gypseum also as rare isolates.63 Although favus occurs in animals including domesticated birds (Microsporum gallinae) and mice (T. mentagrophytes formerly named T. mentagrophytes var. quinckeanum), there exist only a few reports of human infection by the same pathogens responsible for animal favus.82
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
Treatment is the same as for tinea capitis.
TINEA MANUUM
TINEA MANUUM
Tinea manuum is discussed with tinea pedis under the section “Tinea Pedis and Tinea Manuum.”
TINEA NIGRA
TINEA NIGRA
Tinea nigra is a superficial dermatomycosis caused by dematiaceous, darkly pigmented, Hortaea werneckii (formerly named Phaeoannellomyces werneckii and Exophiala werneckii).83
EPIDEMIOLOGY
Tinea nigra occurs in tropical or subtropical areas, including Central and South America, Africa, and Asia. Its incidence is low in the United States and Europe. Although the majority of the approximately 150 North American cases reported since 1950 were associated with tropical travel,63 endemic foci exist in the coastal southeastern United States and in Texas. Person-toperson transmission is rare.84 Tinea nigra has a femaleto-male predilection of 3:1.
CLINICAL FINDINGS
Tinea nigra is found on otherwise healthy people and presents typically as an asymptomatic, mottled brown to greenish-black macule or patch with minimal to no scale on the palms or soles (Fig. 160-13). The macule is often darkest at the advancing border. Because of its coloration and location on palms and soles, tinea nigra is frequently misdiagnosed as acral lentiginous melanoma.
24
ETIOLOGY AND PATHOGENESIS
Tinea nigra is almost always caused by H. werneckii, although other dematiaceous fungi such as Stenella araguata may produce the same clinical picture. Dematiaceous fungi are commonly found in soil, sewage, and decaying vegetation.84 Tinea nigra arises after trauma to the skin with subsequent inoculation, and a typical incubation period of 2 to 7 weeks.
DIAGNOSIS
KOH examination of scrapings from the macule reveals brown to olive-colored, thick branching hyphae, along with oval to spindle-shaped yeast cells that occur singly or in pairs with a central transverse septum. Cultures performed on SDA with cycloheximide and chloramphenicol grow within 1 week. The colony is initially yeast-like with a brown to shiny black color and appears as typical 2-celled yeast forms under microscopic examination. With time, mycelial growth predominates creating a fuzzy grayish-black colony.
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
2947
4
24
Most Likely
■Junctional nevus, dysplastic nevus, melanoma
Consider
■Chemical exposure
Rule Out
Rule Out
■Addison disease, syphilis, yaws
■Addison disease, syphilis, yaws
resolution to prevent relapse. Although oral ketoconazole, itraconazole, and terbinafine are also effective, systemic therapies are rarely indicated.83
TINEA PEDIS AND TINEA MANUUM
TINEA PEDIS AND
TINEA MANUUM
Tinea pedis denotes dermatophytosis of the feet, whereas tinea manuum involves the palmar and interdigital areas of the hands. Infection of the dorsal aspects of feet and hands is considered to be tinea corporis.
EPIDEMIOLOGY
Occurring worldwide, tinea pedis and tinea manuum are the most common dermatophytoses. Estimated to be approximately 10%, the high prevalence is attributed primarily to modern occlusive footwear, although increased worldwide travel also has been implicated.63
Incidence of tinea pedis is higher among those using communal baths, showers, or pools. With the ubiquitous presence of dermatophytes in the environment, however, it may be that host factors, such as an individual’s immune response to dermatophytes, play a determining role in the development of tinea pedis. Tinea manuum is acquired through direct contact with an infected person or animal, the soil, or via autoinoculation. Most commonly only 1 hand (singular: tinea manus) is involved, concomitant with infection of feet and toenails for which the term two feet–one hand
syndrome has been coined. This classic presentation of tinea manus represents a secondary infection of the hand acquired from excoriating and picking infected feet and toenails.87 Tinea manuum should be suspected in individuals who have fine dry scaling of the palm or palms, often accentuated in the creases.
CLINICAL FINDINGS
Interdigital Type: The interdigital type, the most common presentation of tinea pedis, begins as scaling, erythema, and maceration of the interdigital and subdigital skin of the feet, particularly between the lateral third and fourth and fourth and fifth toes (Fig. 160-14A). Under appropriate conditions, the infection will spread to the adjacent sole or instep, but it rarely involves the dorsum. Occlusion and bacterial coinfection (Pseudomonas, Proteus, and Staphylococcus aureus) soon produce the interdigital erosions with pruritus and malodor that are characteristic of the dermatophytosis complex, or “athlete’s foot.”
Chronic Hyperkeratotic (Moccasin) Type: Chronic hyperkeratotic (moccasin) type tinea pedis, is characterized by patchy or diffuse scaling on the soles and the lateral and medial aspects of the feet, in a distribution similar to a moccasin on a foot (see Fig. 160-14B). The degree of erythema is variable, and there may also exist a few minute vesicles that heal with collarets of scale less than 2 mm in diameter. The most common pathogen is T. rubrum followed by E. floccosum and anthropophilic strains of T. interdigitale.
Vesiculobullous Type: Vesiculobullous type of tinea pedis, typically caused by zoophilic strains of T. interdigitale (formerly named T. mentagrophytes var. mentagrophytes), features tense vesicles larger than 3 mm in diameter, vesiculopustules, or bullae on the soles and periplantar areas (see Fig. 160-14C). This type
A B C
2948
of tinea pedis is uncommon in childhood but has been caused by T. rubrum.88
Acute Ulcerative Type: Acute ulcerative type tinea pedis caused by zoophilic T. interdigitale in combination with Gram-negative bacterial superinfection produces vesicles, pustules, and purulent ulcers on the plantar surface. Cellulitis, lymphangitis, lymphadenopathy, and fever are frequently associated.
Vesicular Id Reaction: Vesiculobullous and acute ulcerative types commonly produce a vesicular id reaction, either on the lateral foot or toes, or on the lateral aspects of the fingers.
Tinea Manuum: Dermatophyte infection of the hand usually has a noninflammatory presentation with diffuse dry scaling and accentuation in the creases (Fig. 160-15). However, vesicles, pustules, and exfoliation may be present, especially when zoophilic dermatophytes are involved. Tinea manuum commonly occurs in association with moccasin-type tinea pedis and onychomycosis, all of which should be treated to minimize relapse.89
ETIOLOGY AND PATHOGENESIS
Tinea pedis and tinea manuum are caused predominantly by T. rubrum (most common), T. interdigitale, and E. floccosum.
DIAGNOSIS
24
Most Likely
■Interdigital: erosio interdigitalis blastomycetica, erythrasma, bacterial coinfection
■Hyperkeratotic: dyshidrosis, psoriasis, contact dermatitis, atopic dermatitis, hereditary or acquired keratodermas
■Vesiculobullous: dyshidrosis, contact dermatitis, pustular psoriasis, bacterid or other autoeczematization, palmoplantar pustulosis, bacterial pyodermas, scabies
Consider
■Pityriasis rubra pilaris
Rule Out
Rule Out
■Reactive arthritis
■Reactive arthritis
chronic, superficial perivascular infiltrate in the dermis. Subcorneal or spongiotic intraepithelial vesiculation may be seen in the vesiculobullous type of tinea pedis.
DIFFERENTIAL DIAGNOSIS
MANAGEMENT
ACKNOWLEDGMENTS
Many thanks, to Dr. Amit Garg who served as senior author of previous editions and provided the great majority of clinical images in this chapter.
2949
4
24
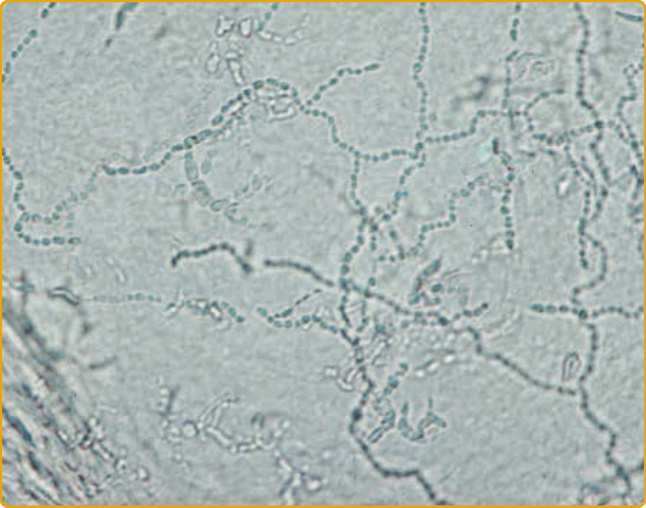
Figure 160-1 Microscopic examination of skin scrapings (scales) revealing septate, branching hyphae.
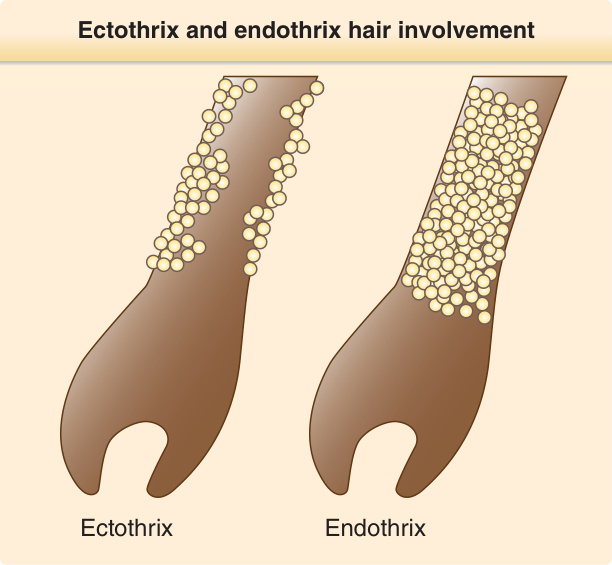
Figure 160-2 Graphic demonstration of ectothrix and endothrix hair involvement.

Figure 160-3 Tinea unguium. A, Distal subungual type. Discoloration, thickening and subungual debris of the distal aspect of the toenails. B, Proximal subungual type. Discoloration and thickening of the proximal nail in a patient with AIDS; Kaposi sarcoma is also seen on the fourth toe. C, White superficial type. Irregular opaque white patches on various parts of the nail plates.

Figure 160-4 Tinea barbae. A, Superficial type. Scattered follicular papules, pustules, and small nodules, which may be easily mistaken for Staphylococcus aureus folliculitis. B, Kerion type. Sharply demarcated red edematous nodule studded with multiple yellowish weeping pustules. Note hairs have been lost from this nodule.

Figure 160-5 Tinea capitis “gray patch” type. A large, round, hyperkeratotic plaque of alopecia, a result of breaking off of hair shafts close to the surface, gives the appearance of a mowed wheat field on the scalp of a child. Remaining hair shafts and scales exhibit a green fluorescence when examined with a Wood lamp. Microsporum canis was isolated on culture.

Figure 160-6 “Black dot” tinea capitis caused by Trichophyton tonsurans.

Figure 160-7 Inflammatory tinea capitis caused by Microsporum canis. Along with alopecia, there are inflammatory papules, pustules, and nodules. This patient also had posterior cervical lymphadenopathy.

Figure 160-8 Kerion of the scalp.

Figure 160-9 Tinea corporis. A, Annular. Tinea corporis demonstrating the classic annular or “ringworm”-like configuration and advancing raised erythematous and scaly border. Note that because the dorsum of the foot is predominantly involved, this eruption is considered tinea corporis and not tinea pedis. B, Polycyclic. Tinea corporis demonstrating multiple polycyclic red erythematous plaques with a raised scaly border. C, Psoriasiform. Tinea corporis resembling psoriasis.

Figure 160-10 Majocchi granuloma. Follicular papules and nodules with scale coalescing to form an annular-shaped plaque on the leg of a woman applying topical corticosteroids to the area.

Figure 160-11 Tinea cruris. Annular erythematous plaques with a raised scaling border expanding from the inguinal on the inner thighs and pubic region.

Figure 160-12 Favus caused by Trichophyton schoenleinii. Note the numerous yellow scutula.

Figure 160-13 Tinea nigra palmaris. An irregular, brownish-black patch on the palm caused by Hortaea werneckii.

Figure 160-14 Tinea pedis. A, Interdigital type. The interdigital space is macerated with opaque white scales and has erosions. B, Moccasin type. Patchy erythema and scaling in a moccasin distribution on the foot. The arciform pattern of scales is characteristic. C, Bullous type. Ruptured bullae, erosions and erythema on the plantar aspect of the great toe. Hyphae were detected on KOH 10% preparation obtained from epithelial cell on the roof of the inner aspect of the bulla.

Figure 160-15 Tinea pedis and manus. “Two feet–one hand” presentation of Trichophyton rubrum. Scaling in the involved (right) hand is accentuated in the creases.
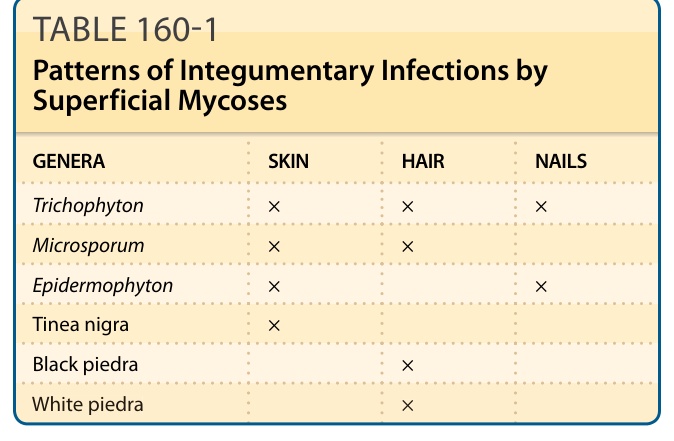
TABLE 160-1 Patterns of Integumentary Infections by Superficial Mycoses
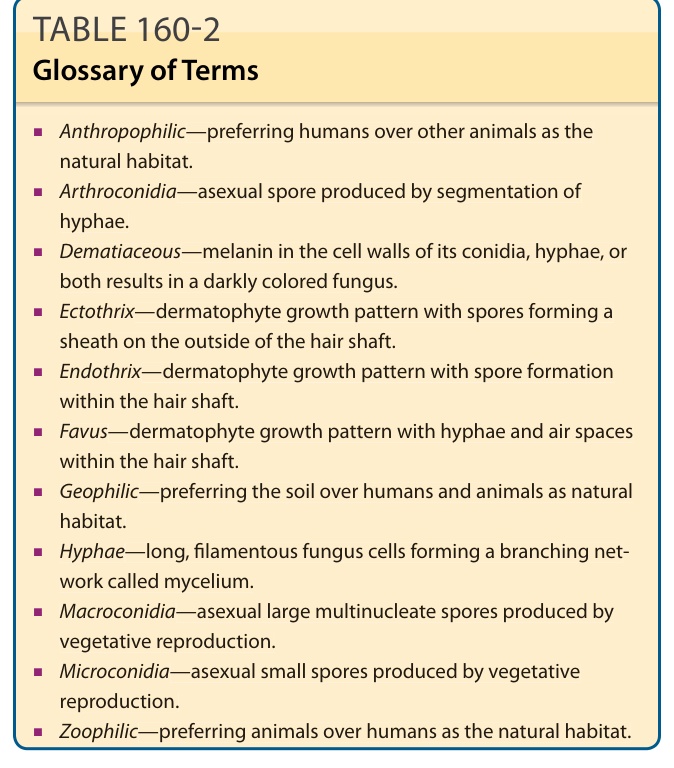
TABLE 160-2 Glossary of Terms
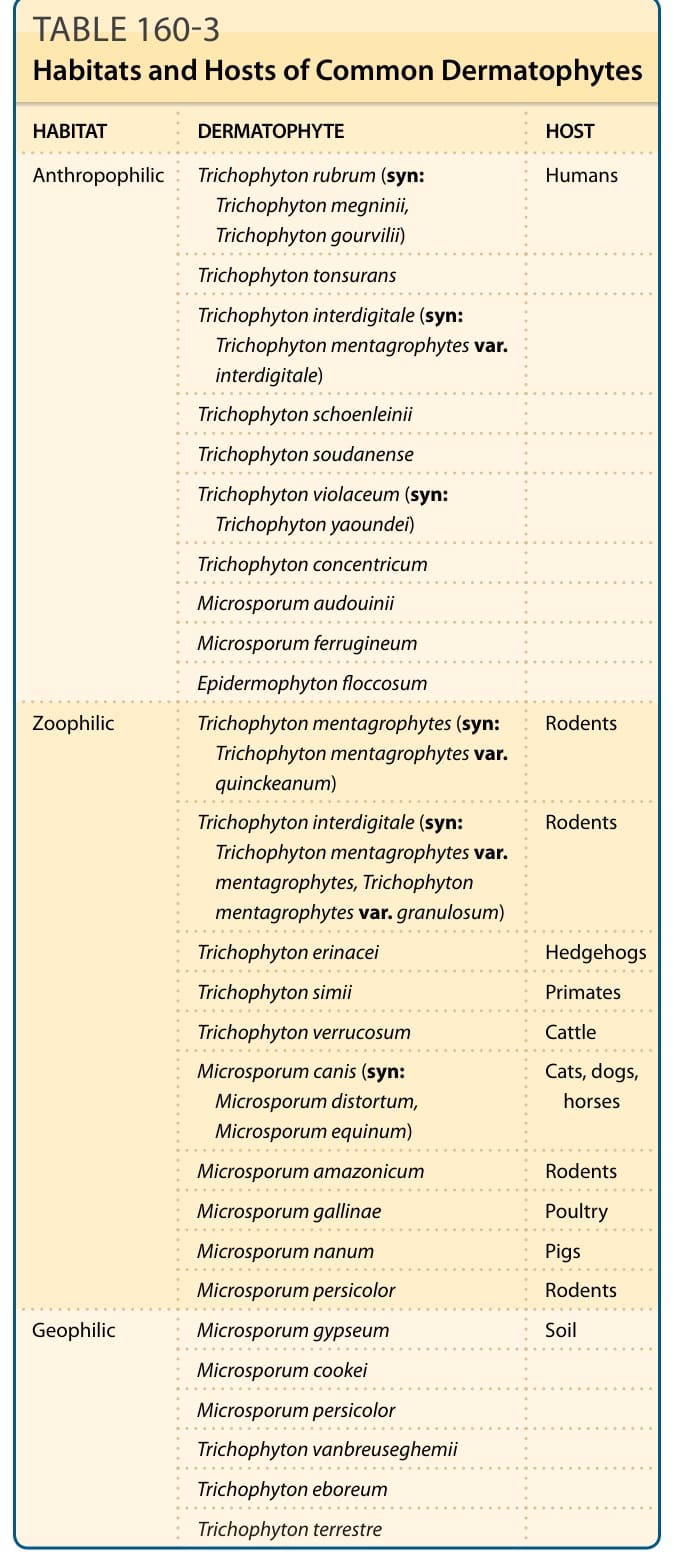
Table 160-3 lists the most commonly encountered dermatophyte pathogens according to their natural habitats and reservoirs. As there are still texts that use the classical names, to avoid confusion and to remain broadly reflective of the literature, this chapter uses both old and current nomenclatures.
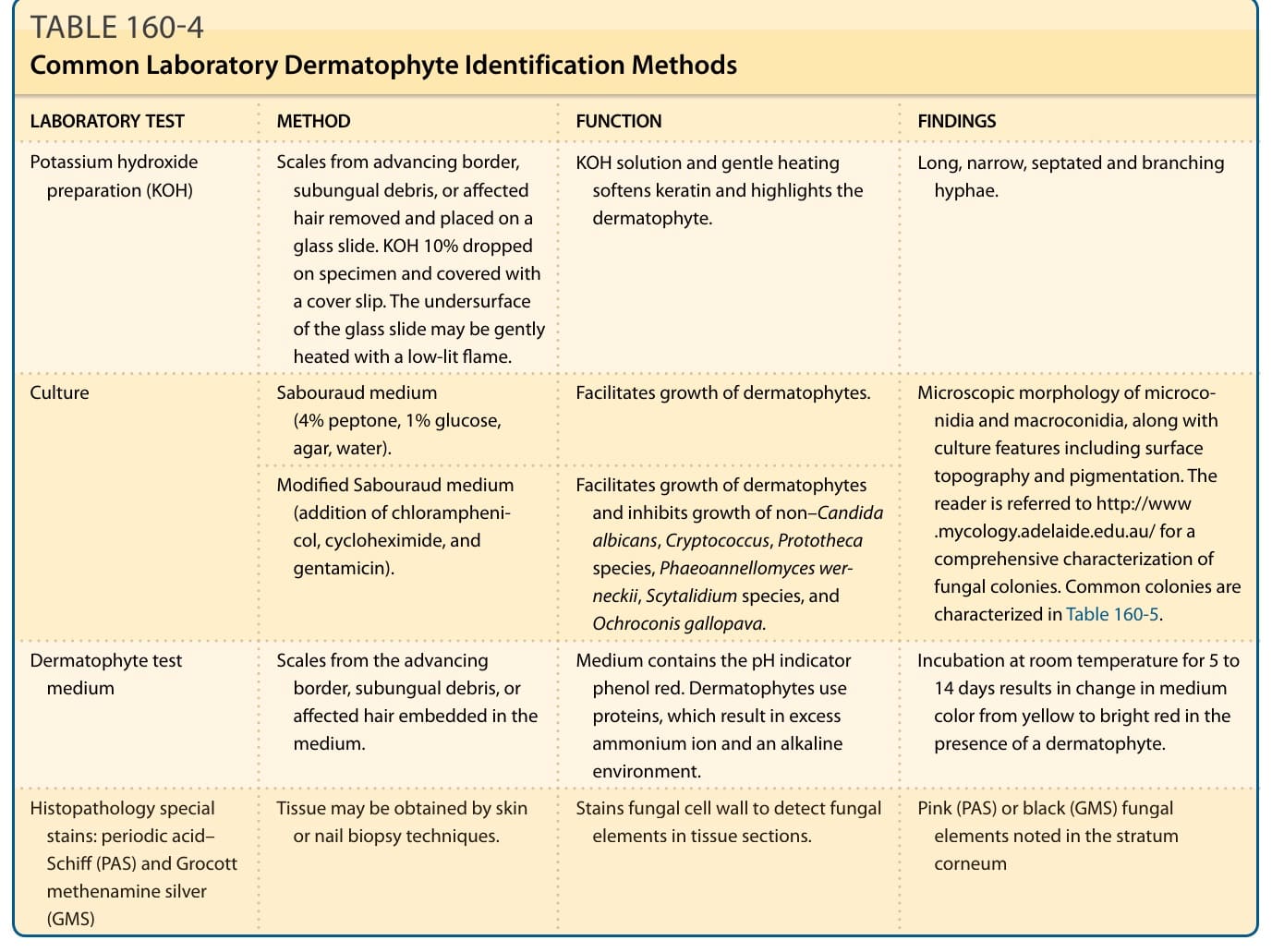
Table 160-4 outlines common laboratory dermatophyte identification methods.
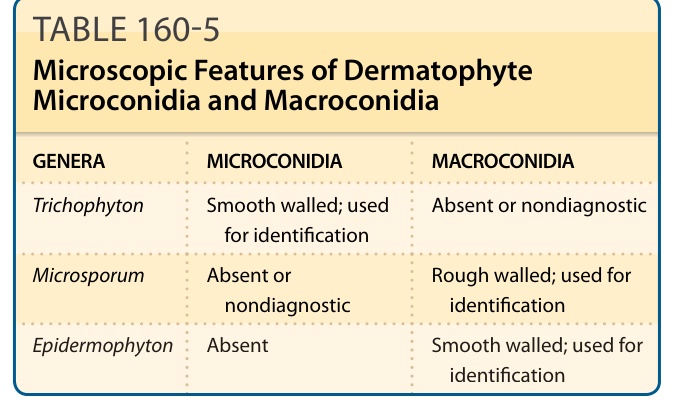
TABLE 160-5 Microscopic Features of Dermatophyte Microconidia and Macroconidia
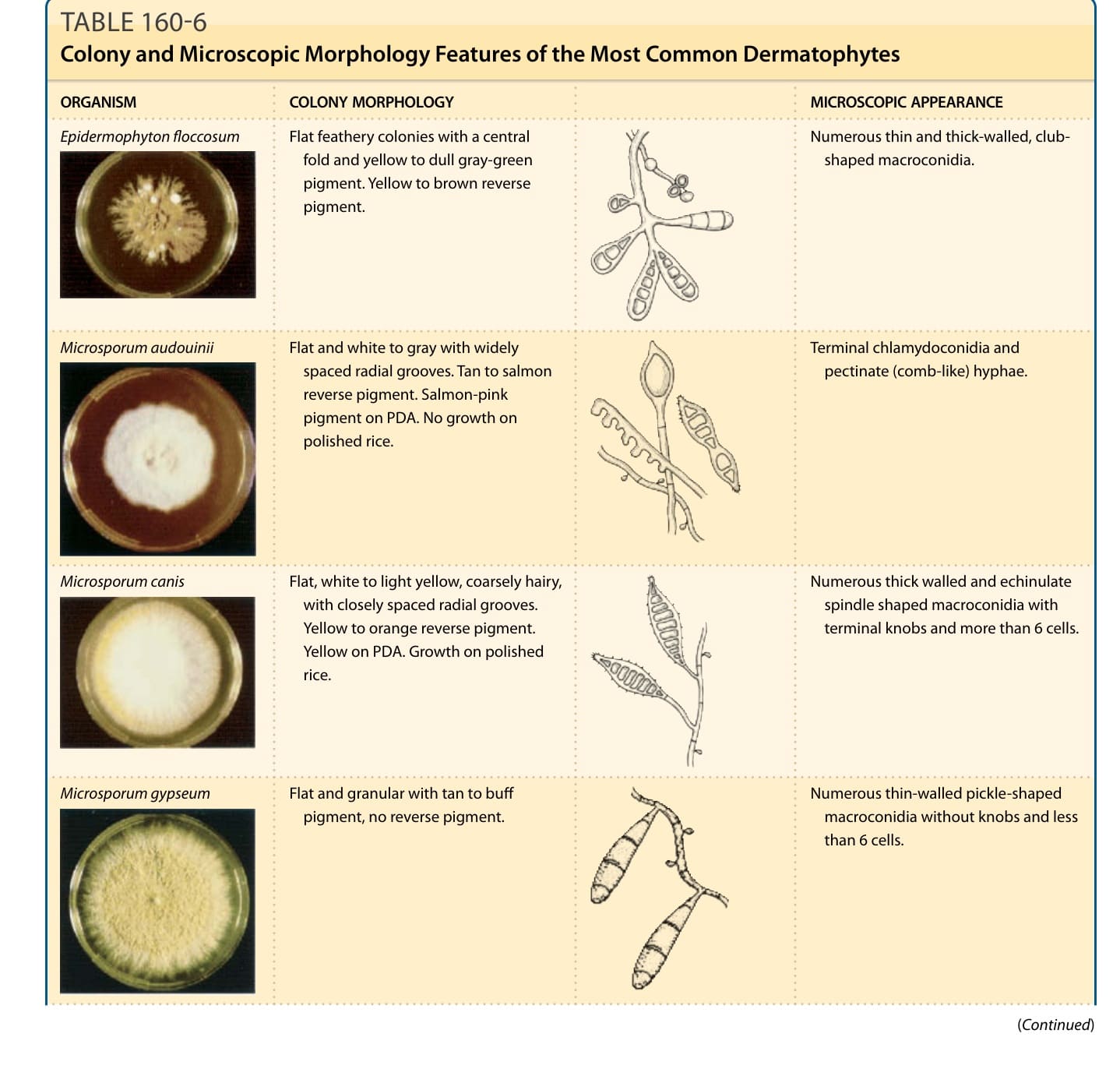
TABLE 160-6 Colony and Microscopic Morphology Features of the Most Common Dermatophytes
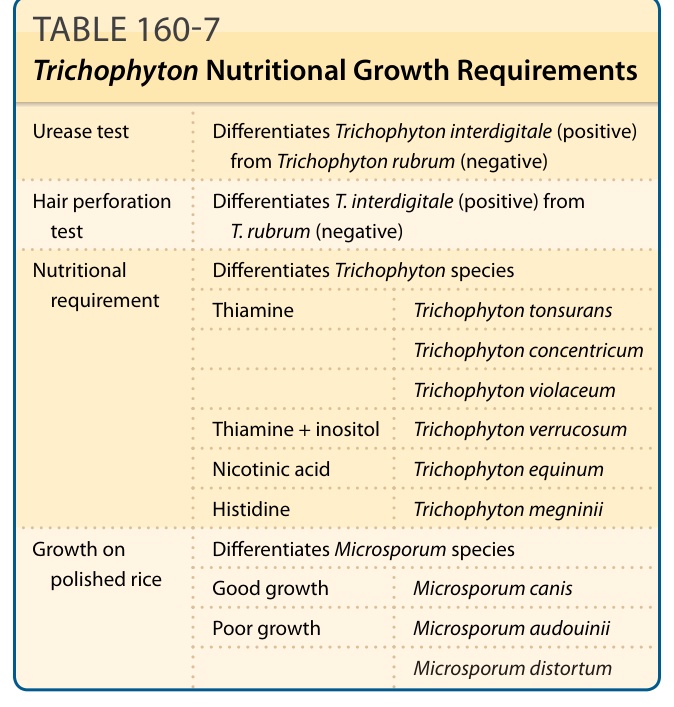
TABLE 160-7 Trichophyton Nutritional Growth Requirements
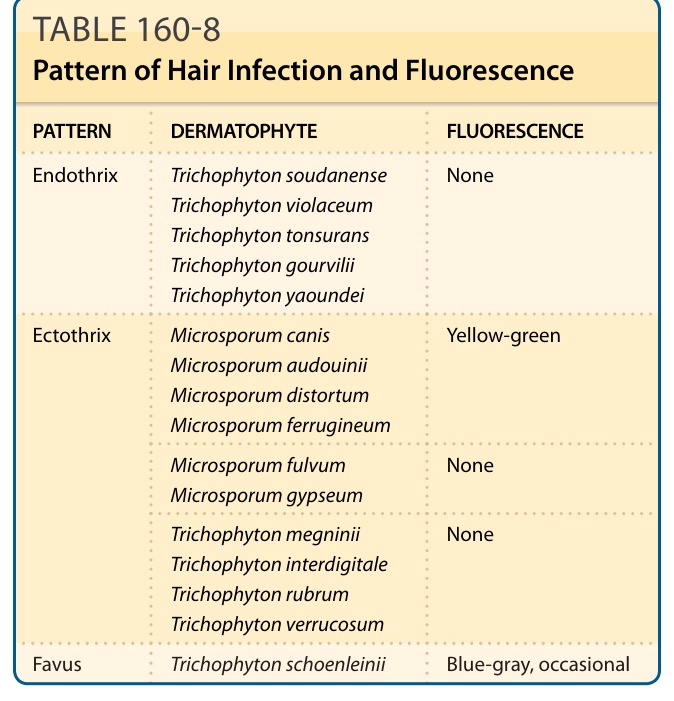
TABLE 160-8 Pattern of Hair Infection and Fluorescence
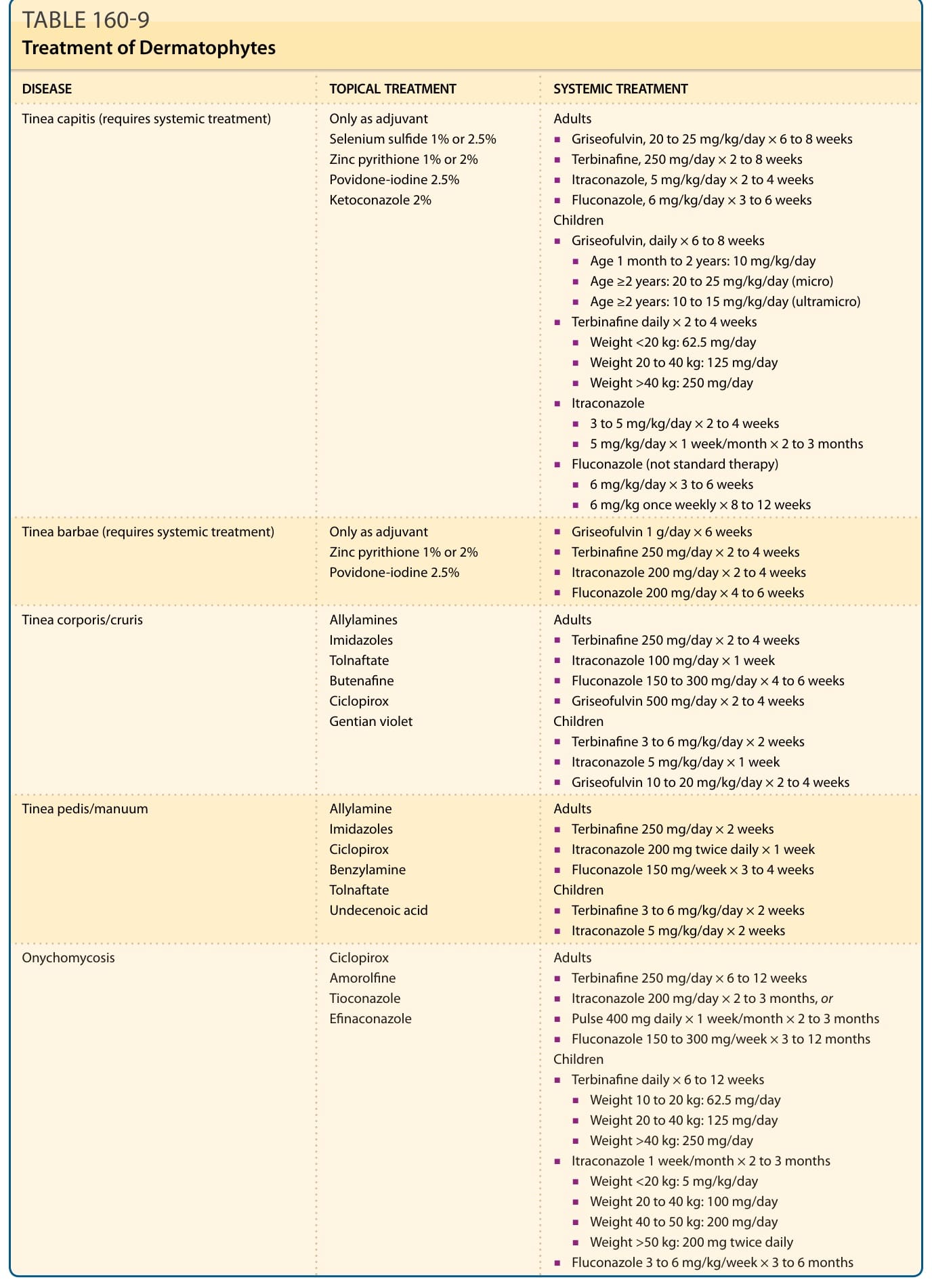
Table 160-9 outlines the treatment of dermatophytes, Table 160-10 lists oral antifungal agents, and Table 160-11 lists topical antifungal agents. Multiple systemic and topical antifungal agents are available to treat dermatophytoses of skin, hair and nails.36-38 Of note, dermatoses involving hair-bearing skin and nails typically require oral treatment. See individual diagnoses in the section “Dermatophytoses” for more information.
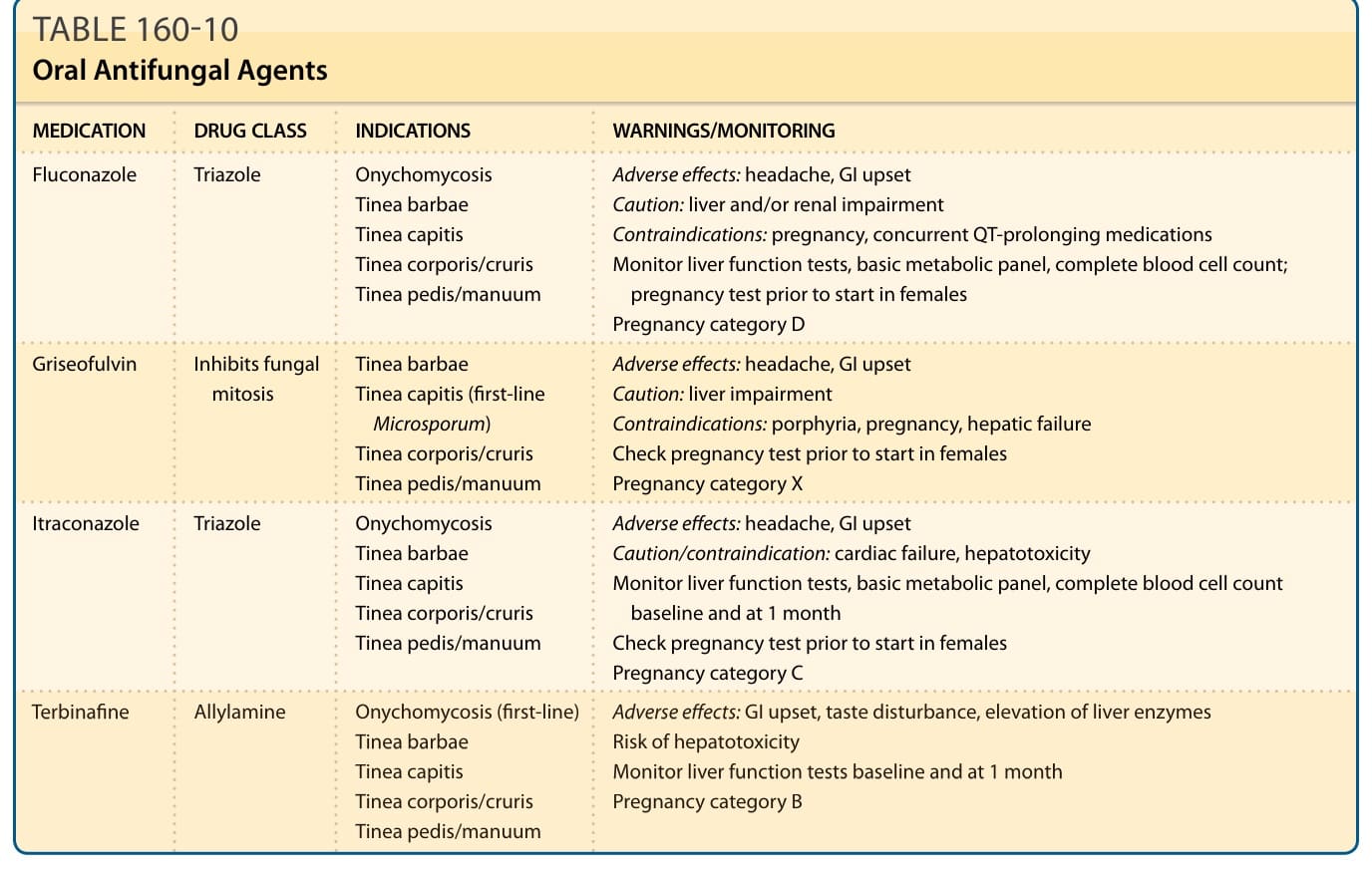
TABLE 160-10 Oral Antifungal Agents
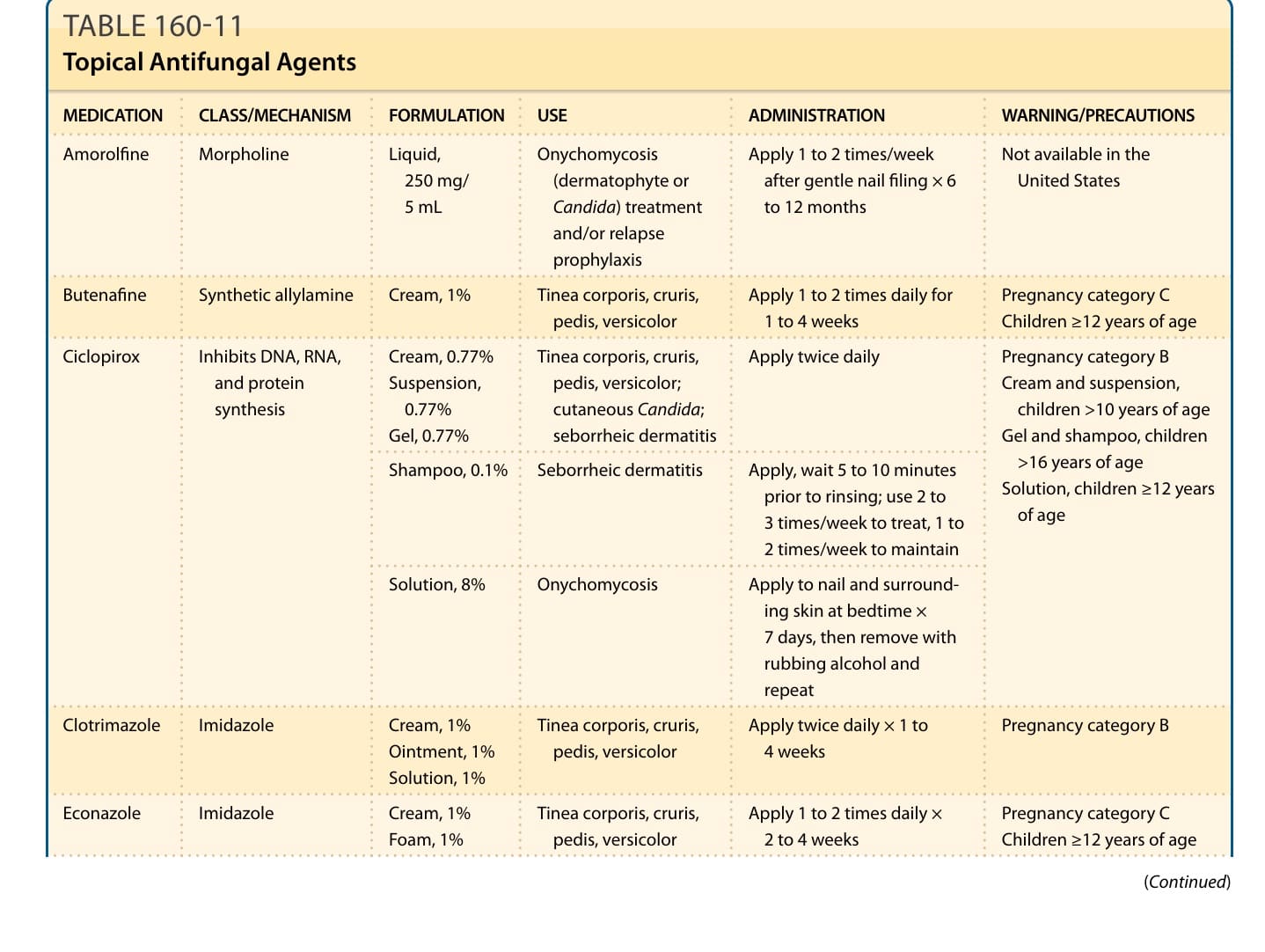
TABLE 160-11 Topical Antifungal Agents
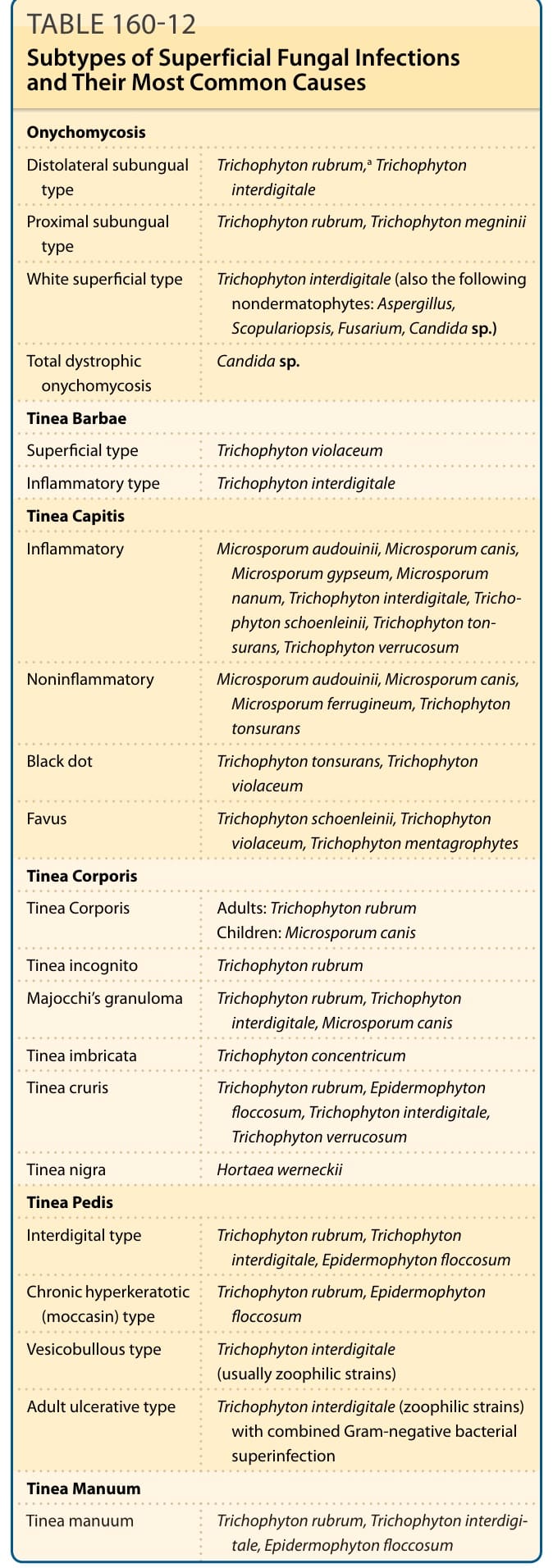
Table 160-12 summarizes the subtypes and most common causes of onychomycosis.
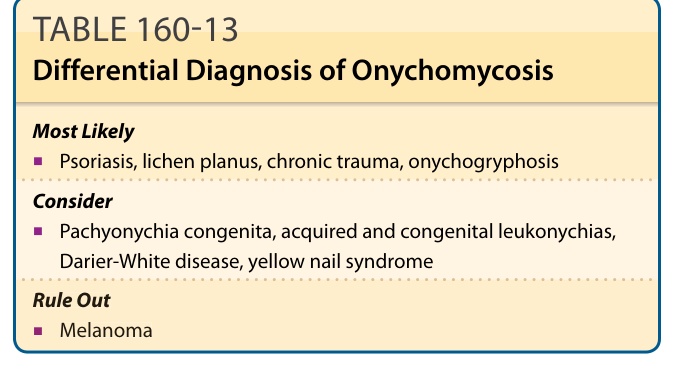
Table 160-13 outlines the differential diagnosis of onychomycosis.
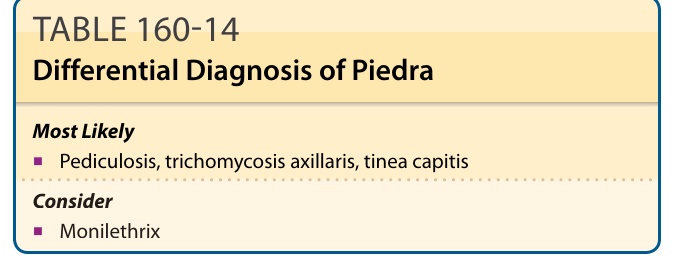
TABLE 160-14 Differential Diagnosis of Piedra
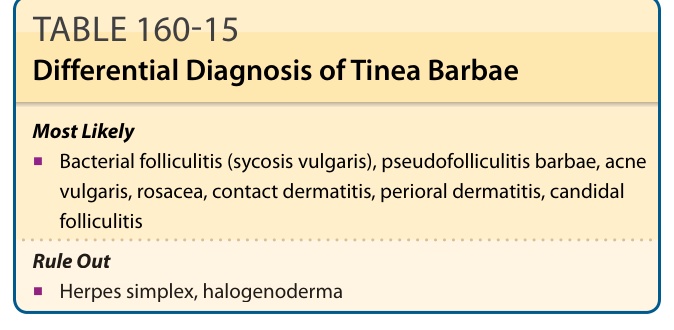
Table 160-15 summarizes the differential diagnosis of tinea barbae.
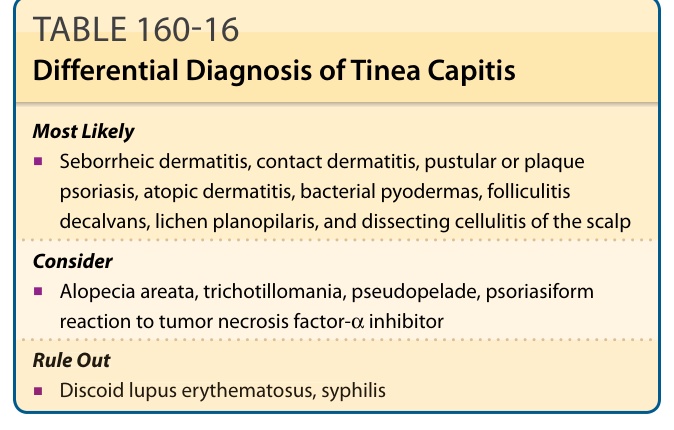
Table 160-16 summarizes the differential diagnosis of tinea capitis.
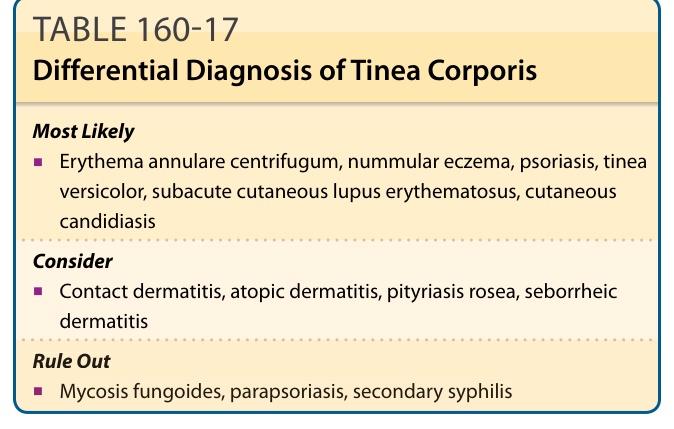
Table 160-17 summarizes the differential diagnosis of tinea corporis.
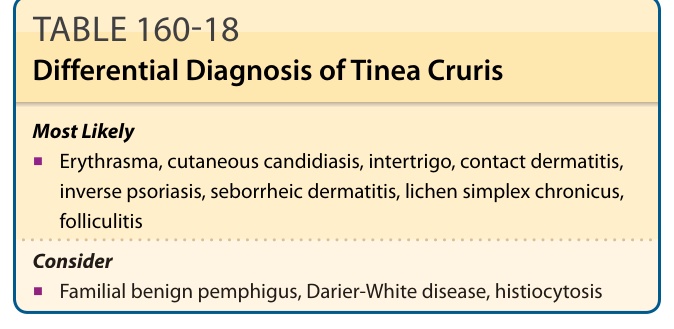
TABLE 160-18 Differential Diagnosis of Tinea Cruris
Table 160-19 outlines the differential diagnosis of tinea nigra.
TABLE 160-20 Differential Diagnosis of Tinea Pedis