Leprosy
23
AT A GLANCE
■ Definition: A chronic granulomatous disease affecting mainly the skin and nerves caused by the obligate intracellular pathogen Mycobacterium leprae.
■ Involvement: Primarily the skin and nerves, but causing sequelae to a wide range of tissues and systems including eyes, upper respiratory tract, lymphoid tissue, testicles, muscles, and bones.
■ Diagnosis: Based on clinical signs and symptoms, hallmarks include loss of sensation within skin lesions, nerve swelling or pain, or demonstration of acid-fast bacilli in skin smears or biopsies.
■ Incidence: 214,783 new cases detected worldwide in 2016, essentially unchanged for the last 4 years. More than 80% of all new cases are detected in only 3 countries—India, Brazil, and Indonesia.
■ Long-term morbidity: Despite the global use of multidrug therapy in use since the mid-1980s, up to 30% to 50% of all leprosy patients will experience some type of reactional episode that may result in a permanent neurologic deficit or disability.
■ A clinical challenge: The long incubation time prior to the slow development of diverse symptoms (3-7 years postinfection), the very low rate of disease progression in infected individuals, and issues with misdiagnosis all create challenges to the development of ways to interrupt transmission.
■ An immunologic spectrum of disease: Understanding what genetic factors and the interplay of innate and adaptive immune responses of the host that leads to resistance or susceptibility to disease are critical in developing novel treatment approaches.
INTRODUCTION
DEFINITION
DEFINITION
Leprosy is a chronic granulomatous infection caused by Mycobacterium leprae, that infects mucous cutaneous tissues and peripheral nerves, leading to loss of
sensation on the skin—with or without dermatologic lesions—and the development of incapacities during the progression of the disease. WHO states that any individual in endemic countries presenting skin lesions with definite sensory loss or positive skin smears may be diagnosed with leprosy.1
HISTORICAL PERSPECTIVE
HISTORICAL PERSPECTIVE
Leprosy is one of the oldest diseases known to afflict mankind. Gerhard Armauer Hansen, a Norwegian physician, was the first to describe the M. leprae bacillus in 1873, identifying the first bacterial pathogen associated with human disease. The name Hansen disease is used in some countries, like Brazil, to lessen the stigma associated with the common name. The characteristic destructive changes that lead to disfigurement, deformity, and disability were among the hallmarks of the disease that allowed it to become stigmatized in ancient times.2 Speculations about the existence of leprosy in ancient India, Egypt, and China have been proposed, with the earliest paleopathological evidence found in 4000-year-old bones from the Balathal burial site in Rajasthan, western India.3 The first use of molecular techniques using polymerase chain reaction (PCR) to detect M. leprae DNA specific sequences in ancient bones dated to ad 600 was described in 1994.4 PCR was used to identify M. leprae DNA in 1st century ce bones from the Tomb of the Shroud burial site in Israel, the earliest known date of existence of leprosy in this region.5
Using paleopathological and molecular methods to analyze ancient bones from archeological sites, burial grounds, and cemeteries, evidence of the spread of leprosy has emerged, indicating the spread of the disease from Western and Central Asia from the 4th century ad into Eastern and Central Europe occurred mainly due to human migrations associated with military campaigns, expansion of territories, or migrations to effect colonization.6 Houses were established to quarantine those with leprosy and other communicable diseases, called lazarets, in 7th-century France, but it was not until the return of the Crusaders from ad 1100 coming back from countries of the Ottoman Empire where leprosy was endemic that the disease became an increasing problem. Leprosy in Europe and the United Kingdom peaked in the 13th and 14th centuries and then began a slow decline. Comparison of the M. leprae whole genome
obtained from ancient European, UK, and Scandinavian gravesites show only a few dozen single nucleotide polymorphism (SNP) changes over the last 1000 years, with no mutations in any genes related to increased virulence or pathogenesis.7 The essentially clonal nature of M. leprae from the ancient to modern times suggests that the precipitous decrease in leprosy prevalence was independent of features of the pathogen and were more likely related to changes in host resistance or environment. Since people with lepromatous leprosy likely had a weakened immune status, they were more likely to succumb to other infections. Events thought to have contributed to a higher death rate in those with leprosy included a serious famine in 1325, followed by the outbreak of plague, or Black Death, in 1349 that killed between one-third and two-thirds of the population in Europe and the United Kingdom. Such massive death would have severely curtailed the support networks of hospices and leprosaria whose religious clergy, patrons and physicians had cared for patients, but were likely decimated. There is also suggestive evidence that increases in population density, overcrowded living conditions, and the rise of tuberculosis after the 15th century contributed to death by coinfections with multiple diseases.8 As those susceptible individuals succumbed to disease, the innate resistance of the surviving population to mycobacterial infection and other diseases common during that period likely improved, and coupled with improved socioeconomic conditions, sanitation, and hygiene, the lines of transmission of infection were broken. Currently, endemic cases of leprosy in Europe and the United Kingdom are extremely rare. Comparative genomic studies of M. leprae isolates all over the world revealed a remarkable conservation of the genome (99.995% identity among all strain types), showing the existence of 215 polymorphic sites consisting mainly of SNPs. Four of these SNPs represented 4 main strain types that showed very strong geographical associations that were used to trace the evolution and distribution of M. leprae based on human migration patterns throughout history.9 SNP Type 1 was found primarily in Southeast Asia; SNP Type 2 was found mainly in East Africa; SNP Type 3 was associated with the European/North African region, whereas SNP Type 4 was found mainly in West Africa. Leprosy did not exist in North or South America until its introduction via colonialism from Europe (SNP Type 3) and from the importation of slaves from Africa (SNP Type 4). These four main types were subdivided into 16 subtypes based on further characterization of SNPs and insertion/deletion events from modern and ancient M. leprae genomes from a total of 400 samples from 28 different regions of the world, namely SNP Type 1 (A-D), Type 2 (E-H), Type 3 (I-M), and Type 4 (N-P).10
Besides humans, M. leprae is also found as a zoonotic infection in armadillos in the Southern United States,11 and recently in red squirrels in the British Isles.12 Interestingly, both armadillo and squirrel M. leprae have the same SNP subtype, 3I, indicating a common European ancestry.
23
EPIDEMIOLOGY
Leprosy is still a serious neglected disease. WHO refers the number of new cases is gradually decreasing in the last 10 years, from 265,661 in 2006 to 210,758 in 2015,13
but different groups of researchers have demonstrated that the hidden endemics may be high,14,15 the number of cases in children is increasing16 or stable,17 whereas the proportion of multibacillary patients is increasing18
and cases with grade 2 disability seem to be stable,19
but high,20 indicating late diagnosis. Altogether, these factors demonstrate that instead of a true decline of new cases, delay21 and absence of diagnosis seem to be the main problems.15,22,23 In fact, mathematical modeling shows that in 2020 we may have 4 million cases of undiagnosed leprosy worldwide, that is, almost 20 times more than the present number of cases diagnosed annually.24
The definition of leprosy has changed with time. There is currently no laboratory test to diagnose leprosy. Once a patient completes multidrug therapy, the individual is usually removed from the registry and is no longer considered a case, even if disability and reactional episodes continue long after treatment. For decades, treatment of leprosy was done continuously with dapsone alone (monotherapy), and all cases that received dapsone monotherapy were registered in the system. Because of this practice, the prevalence of leprosy remained high, with more than 10 million patients on the registry during the 1980s. With the implementation of multidrug therapy in 1982, treatment was shortened to, at most, 2 years. The active registry then changed to only those being treated, while those who completed their therapy were subsequently “cleared.” Thus, over the course of a decade, millions of patients who completed multidrug therapy and did not have symptoms were purged from registries.25 The net effect was that within 20 years after the introduction of multidrug therapy, leprosy prevalence was markedly reduced by more than 85%13 although the new case detection rate has remained relatively stable at more than 200,000 worldwide for almost 10 years (Fig. 159-1). Currently, the most important epidemiologic indicators of leprosy burden are the new case detection rate by country, and the proportion of cases in children, those with multibacillary disease and those with grade 2 disability, indicating a late diagnosis.13 Although India has the highest number of leprosy cases in the world, Brazil has the highest new case detection rate among all countries (Fig. 159-2). However, when we look at the other 2 most significant parameters, the percentage of cases in children (Fig. 159-3) and those with grade 2 disability (Fig. 159-4), there is a clear shift, with most of the reporting countries considered as high or very high, whereas Brazil, India, and Indonesia have medium or low percentages. Although these 3 countries collectively account for >80% of the global leprosy burden, the large number of cases reported dilutes the percentage of both children with leprosy and those with grade 2 disability, while countries who report
2893
23
Global prevalence and new case detection of leprosy
12
11
10
9
8
Prevalence (millions)
7
6
5
4
3
2
1
0
12
11
10
9
8
NCD (millions)
7
Prevalence
6
New cases detection
5
4
3
2
1
0 1966 1970 1975 1980 1985 1990
1995 2000 2005 2010 2015
Year
Leprosy new case detection rate, world 2015
2894
23
Proportion of cases among children
Proportion of new cases with grade-2 disability, world 2015
Arctic Ocean
2895
23
less than 1000 new cases per year generally have much higher rates in both categories. A high or very high percentage of these 2 parameters likely means that children and adults are diagnosed only when presenting classical pathognomonic lesions of leprosy and/or disabilities, indicating late diagnosis.15,21
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
During the IV International Leprosy Congress in Madrid, 1953, leprosy was classified in 2 stable forms, tuberculoid leprosy and lepromatous leprosy, and a borderline group between these 2 polar forms. In 1966, Ridley and Jopling proposed a 5-group classification system based on clinical, histopathologic, and immunologic criteria26 that is still in use for classifying leprosy. The colonization of skin and invasion of peripheral nerves by the bacilli, followed by innate and adaptive immune responses by the host, results in the clinical spectrum of leprosy (Fig. 159-5). There is an overall genetic resistance toward developing leprosy,
with more than 90% of people having a natural immunity, with cell-mediated immunity being most important in preventing disease progression. All patients, except those with primary neural leprosy,27 first present 1 or a few hypopigmented macules on the skin. Indeterminate leprosy (Fig. 159-6) may last for months or years before moving to spontaneous cure or toward one of the poles or borderline forms of the clinical spectrum, depending mainly on the cellmediated immunity of the host against the bacilli. At one end of the spectrum with a better cellmediated immunity, there is polar tuberculoid leprosy, where well-defined plaques, usually a few in just one segment of the body, hypochromic and/or erythematous, sometimes atrophic, present with papules or tubercles that are mainly circinate on the periphery of the lesions (Fig. 159-7). A special self-healing type of tuberculoid leprosy, infantile nodular leprosy, can be found as a single nodular lesion, but also as papules or plaques, usually on the face of the child (Fig. 159-8).28
At the other end of the spectrum lies polar lepromatous leprosy, which is established by a complete lack of cell-mediated immunity, usually presenting with plentiful nodular lesions disseminated throughout the body, associated with diffuse infiltration (Fig. 159-9),
Leprosy clinical spectrum
M. leprae
Person Cure
Indeterminate leprosy
Primary Neural leprosy
BT BB
TT
Borderline
Cell-, mediated immune response
BL LL
Antibody-, mediated immune response
unstable forms
IL-2 IFN- γ
IL-4 IL-10
AFB anti-PGL- I IgM
Reversal Reaction
ENL
Chronic Neuritis/Neuropathy
2896
including the ears (Fig. 159-10) and face, that may have facial features so marked that it gives the appearance of a lion’s face, known as leonine facies (Fig. 159-11).29 A special type of lepromatous leprosy is histoid leprosy, that has an even higher bacillary load than the usual lepromatous leprosy, with rafts of bacilli called globi, presenting diffuse shiny nodules and papules, and a variable degree of skin infiltration (Fig. 159-12).30 Some cases of lepromatous leprosy are a challenge for less experienced health professionals to diagnose when the main skin manifestation is infiltration (Fig. 159-13). This special type is called Lucio leprosy, first described by Lucio and Alvarado in Mexico in 1852.31 Isolation and characterization of this new species from Lucio patients, called Mycobacterium lepromatosis,32 and whole genome sequencing33 have now firmly established that this closely related mycobacterium causes this form of leprosy found mainly in Mexico and the Caribbean. The 3 borderline forms (borderline-tuberculoid, borderline-borderline, and borderline-lepromatous)
23
in between are all immunologically unstable. All borderline patients have skin infiltration, varying from a few to many lesions, in one or many areas of the body. Although tuberculoid leprosy patients have just papules or tubercles with no infiltration, borderlinetuberculoid leprosy presents a clear infiltrative band around the periphery of the lesions, changing from a very sharp border in tuberculoid leprosy to a more diffuse infiltrated outer layer in borderline-tuberculoid leprosy (Fig. 159-14). As the forms progress toward the
2897
23
lepromatous end in borderline-borderline (Fig. 159-15) with its classical foveolar lesions, and borderlinelepromatous leprosy (Fig. 159-16), effective cellmediated immunity decreases, allowing a progressive spread and increase in the number of bacilli, an increase in infiltration of the lesions, with the evolution to form more nodular lesions, often involving the face and ears. The diagnosis of leprosy is based on the detection of hypo- or total anesthesia in the lesions that may be associated with hypohidrosis and alopecia. Tuberculoid leprosy patients can present both dryness of the skin and alopecia restricted to the territory of the lesions. In contrast, lepromatous leprosy patients may show extensive areas of dryness, especially on the legs, and in advanced cases may result in madarosis and hair loss in different parts of the skin. Borderline patients follow the same pattern, with more restricted features in borderline-tuberculoid leprosy and more diffuse in borderline-lepromatous leprosy. Paresthesia is a frequent symptom associated with leprosy cases. Burning, numbness, tickling, and other
2898
sensations may be present within the lesions or following the territory innervated by the nerve trunks in the affected area. Patients may feel these sensations in acute crisis, especially at night in cold weather, that may recur frequently, becoming increasingly common with the progression of the disease. All types of leprosy lesions must be submitted to a thorough sensitivity evaluation, including vasomotor reflex, sweating function, thermal, pain, and tactile sensitivity. Dilation of blood capillaries as a secondary axon reflex erythema, which is dependent on nerve integrity, may be tested using a 1:1000 histamine solution, injected intradermally in normal and lesional skin. Within 5 to 10 seconds, erythema will result from the direct action of histamine on the capillaries, causing vasodilation in both areas, normal and lesional. Two minutes after this a secondary erythema caused by capillary dilation will occur only on normal skin. The last phase of triple Lewis response is exudation of liquid to the dermis, resulting in wheal formation in both areas. Therefore, the triple Lewis response is incomplete only on lesional skin, with the absence of secondary erythema.
23
Iodine-starch or alizarin red34 may be used to assess sweating function of leprosy lesions. After iodine painting followed by starch, or after alizarin red, exercise may be required to induce sweating. When autonomic nerve function is affected sweating is impaired or completely absent and the skin remains dry. On normal skin, a bluish or dark brown (iodine-starch) or violet (alizarin red) color will appear, while there will be no reaction (anhidrosis) or irregular sweating (hypohidrosis) on leprosy lesions. Thermal, pain and tactile, and Semmes-Weinstein Monofilaments tests are all directly dependent on correct verbal responses from the patient. Therefore, it is crucial to explain what each test is for, how to give proper feedback for the sensation elicited, and to perform the test on normal non-lesional skin sites to familiarize the individual with the sensation before testing lesion areas to measure any changes. The thermal test is based on the capacity to discriminate between hot and cold sensitivity on touching the skin with 2 tubes containing hot (±45°C [113°F]) or cold water. The tube surface is touched on lesional and normal skin randomly, followed by recording the patients’ answers. The professional must be careful to avoid touching lesional and normal skin at the same time, especially for smaller lesions. Pain sensitivity is based on the ability to distinguish between the tip or the base of a needle, since one produces pain whereas the other does not. Also, randomly, lesional and nonlesional skin must be touched with the tip or the base of the needle, followed by recording the answers. A clear limitation of this method is the use of a perforating instrument, that may cause fear to some patients, especially children. Tactile sensitivity is tested using a cotton wad, and the patient should answer if he/she senses the light touch of the cotton touching the skin, both normal or lesional. Semmes-Weinstein Monofilaments or esthesiometer kits are monofilament lines graded in thickness with different colors that are attached to plastic posts to apply different amounts of target pressure to the skin. The color and range of target force varies from green (range 0.008-0.07 g, normal skin sensation), the thinnest of which is like the sensation of a mosquito landing on skin, to the thickest, red (up to 300 g).35 These devices are simple and cheap and can easily measure diminished or loss of protective sensation cause by diabetic neuropathy or neuropathy cause by leprosy nerve damage. Loss of sensation using the blue Semmes-Weinstein monofilaments indicates diminished sensation of light touch (0.16-0.4 g), purple indicates diminished protective sensation (0.6-2 g), and red indicates more profound loss of protective sensation (4-300 g). More recently, the simplicity and ease of use of Semmes-Weinstein monofilaments have supplanted all of the other tactile, thermal, and pain tests.36 After showing the patient how the monofilament works and getting a “yes” response if he or she feels the touch, various thicknesses of Semmes-Weinstein monofilaments can test areas of skin randomly inside and outside the suspect lesion, as depicted in Video 159-1 at mhprofessional.com/fitzderm9evideos. Even children
2899
23
as young as 6 to 7 years old can respond very well to this kind of test, and those children who are not able to communicate well can still point to the place on the skin if they feel the device touching it (see Video 159-1 at mhprofessional.com/fitzderm9evideos). In conclusion, the “classic” cases as defined by Ridley-Jopling classification have well-defined lesions, associated with a range of signs and symptoms, which facilitate the diagnosis of leprosy. After 35 years of multidrug therapy, the challenge now is to diagnose cases early, with the goal to eliminate disabilities.
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
Although leprosy diagnosis is based primarily on the presence of skin lesions, usually when dermatologic signs are detected, at this point the peripheral nerves have been already invaded and damaged by M. leprae itself and/or by the response of our immune system. In fact, nerves may be the first target of M. leprae, and the infection itself together with immune cell infiltration and inflammation that can be clinically detected by palpation. Palpation of the peripheral nerve trunks can establish nerve thickness and tenderness. However, even for highly trained health professionals, it is not a simple task to detect differences in thickness from one side to the other, or to decide if the nerve is soft, and therefore normal, or fibrotic. Furthermore, those differences should be considered only when it is associated to some functional harm, as (1) loss of sensation defined by hypo- or total anesthesia on the territory of the nerve; (2) motor dysfunction, as in the case of interosseous muscle hypotrophy; or (3) autonomic alteration, as with skin sweating deficit. Although tuberculoid leprosy patients may have conspicuous alterations in just one specific peripheral nerve trunk, usually in the same segment of the skin lesion, lepromatous leprosy patients often present thickness and tenderness variations in many nerves, accompanied or not with functional alterations in different segments of the body. Borderline-tuberculoid, borderline-borderline, and borderline-lepromatous leprosy patients usually present nerve changes, varying from a few nerve trunks affected in borderlinetuberculoid leprosy to many in borderline-lepromatous leprosy. In many cases, there is some degree of pain, spontaneously reported by the patient, or mentioned during palpation. Besides upper and lower limbs, the face also may be affected when facial or trigeminal nerves are damaged, which can result in hypo- or anesthesia, including on the cornea, and muscle hypotrophy, especially when palpebral muscles are involved, resulting in lagophthalmos (Fig. 159-17). The presence of any of these changes in peripheral nerve trunks detected by palpation or functional loss eliminates the diagnosis of indeterminate leprosy. On the other hand, between 5% and 17% of all leprosy patients only have signs of nerve inflammation or
2900
functional deficit without any skin lesions, in which case the diagnosis may be pure neuritic, or the more common term primary neural leprosy,37 because up to 35% of such cases may develop skin lesions after the diagnosis of primary neural leprosy.38
Primary neural leprosy accounts for about 4% to 8% of all leprosy cases, although in India it may be as high as 17%.37 A positive acid-fast bacilli result on slit-skin smear eliminates primary neural leprosy, but a nerve biopsy can demonstrate the presence of acidfast bacilli in 16% of these cases, whereas PCR is positive in almost half of them.39 Definitive diagnosis of primary neural leprosy is not a simple task and may require clinical signs, nerve histopathology, electrophysiology, and ultrasonography,37 although most of those techniques are not available in highly endemic countries. Endocrine dysfunctions, after nerve and skin lesions, are most prominent in patients, but are not readily detected, reaching up to 25% of cases40 leading to, among other problems, hypothyroidism, euthyroid sick syndrome, hypogonadism, sterility and osteoporosis.41 Levels of testosterone were inversely correlated with the number of skin lesions,40 and the level of adrenal androgen dehydroepiandrosterone sulphate had an inverse correlation with interleukin (IL)-6 and tumor necrosis factor (TNF)-α, whereas gonadotropins—luteinizing hormone and folliclestimulating hormone—were positively correlated with proinflammatory cytokines,42 suggesting a possible neuro-immune-endocrine correlation in leprosy.
COMPLICATIONS
COMPLICATIONS
The natural history of leprosy is the evolution to impairment, especially with the eyes, hands, and feet, in both soft tissues and bones, leading to disfigurement and deformity, the origin of all leprosy-related stigma. Even with bacteriological cure after multidrug therapy implementation, and assistance from social networks involved in education, training, and reintegration of those with disabilities into society, estimates
of the numbers of people living with varying levels of disability, including Grade 1 (partially disabled) to Grade 2 (can be completely disabled and unable to work) caused by M. leprae are likely between 1 and 4 million worldwide.43
With the eyes, loss of corneal sensation can result in wounds, followed by infection and blindness, whereas hypotrophy of palpebral muscles may result in lagophthalmos, which can also contribute to corneal infection. Advanced cases, especially in multibacillary leprosy, mostly toward the lepromatous leprosy pole, may present characteristic facial bone malformations, resorption, and pitting, particularly involving destruction of the anterior nasal spine, resorption of the alveolar process of the maxilla, sometimes with loss of teeth, collectively characterized as rhinomaxillary syndrome.44
For hands and feet, complications start with a loss of sensation that may lead to wound formation (Fig. 159-18) after burns, trauma, or repetitive moderate pressure–induced skin disruption not detected by the patient, with possible evolution to fissures and ulcers, soft tissue inflammatory autolysis, muscle atrophy, bone decalcification, osteitis and resorption (Fig. 159-19), fusion and joint dislocation, osteoarthritis, and destruction.45 At the same time, interosseous hypotrophy or amyotrophy may result in paresis or paralysis, leading to formation of claw and/or drop hand or foot (see Video 159-2 at mhprofessional.com/ fitzderm9evideos), that may be mobile at first, and constitute severe impairments to leprosy patients,46
like walking (see Video 159-3 at mhprofessional.com/ fitzderm9evideos).
23
ETIOLOGY AND PATHOGENESIS
RISK FACTORS
RISK FACTORS
Mycobacterium leprae, a noncultivable obligate intracellular pathogen that mainly damages skin and peripheral nerves, is the causative agent of leprosy, resulting in a broad range of skin lesions with anesthesia, peripheral neuropathy through nerve damage, and muscle weakness and atrophy leading to bone loss by resorption, with related deformity, disfigurement, and disability along with the social stigmatization associated with this disease afflicting mankind for thousands of years. Although M. leprae shares roughly 1,439 gene orthologs and homologs with M. tuberculosis, a reductive evolutionary event that occurred between 10 and 20 million years ago resulted in massive gene deletion and decay, resulting in the transformation of nearly half of all coding genes into nonfunctional truncated gene remnants or pseudogenes.47 This process of reductive evolution has occurred in several obligate intracellular pathogens, including Rickettsia and Chlamydia, and is thought to be a survival response to dramatic changes in ecological niche or lifestyle. The streamlining and elimination of many genes and pathways once required for survival as a free-living species would be superfluous in an intracellular habitat, resulting in deletion or inactivation of large parts of the genome. Thus, M. tuberculosis has 4.41 Mb, where >90% of the genome encodes 3,998 protein coding sequences, whereas M. leprae has 3.27 Mb, where just under 50% of the genome codes for 1614 functional genes, with the remainder coding for 1306 pseudogenes and gene remnants whose complete counterparts can be found in M. tuberculosis. The combined effect of gene reduction has created a minimal gene set, reducing the number of genes involved in all functional metabolic pathways, including critical pathways involved in gene regulation, detoxification, DNA repair, transport
2901
23
or efflux of metabolites and small molecules, while generally decreasing the frequency of genes in degradative pathways versus synthetic ones and a paucity of respiratory enzymes. Because of these deficiencies, M. leprae has one of the longest doubling times of any bacteria, around 13 days, possibly explaining the exceptionally long incubation time between infection and development of clinical disease, usually between 3 and 7 years, although in some cases up to 20 years. The failure to grow M. leprae in axenic medium despite decades of attempts is probably the result of the combined effects of gene reduction and mutations in key metabolic pathways. One of the hallmarks of the leprosy bacillus is the ability to attach and invade Schwann cells associated with the peripheral nervous system, which leads to colonization and inflammation within nerves, causing nerve damage, demyelination, and neuropathy. Binding to the laminin-2 molecule in the basal lamina of Schwann cells is mediated by 2 bacterial cell wall components, the laminin-binding protein (encoded by ML1683c) and the terminal trisaccharide of the M. leprae–specific phenolic glycolipid I (PGL-I).48 Transmission is thought to occur through the aerosol route, with the bacillus gaining entry and colonizing resident macrophages within the nasal mucosa and turbinate,49 then disseminating to tissues and nerves through the bloodstream. Early events involved in host–pathogen interaction at the cellular level is likely mediated by host genes involved in pattern recognition receptors and mycobacterial uptake (Toll-like receptors [TLR], nucleotide-binding oligomerization domain containing 2 [NOD2], and mannose receptor C-Type 1 lectin [MRC1]), which modulate autophagy. For example, bacterial cell wall lipoproteins that recognize and bind TLR 1/2 heterodimer ligands on the host cell surface trigger an innate immune response, the outcome of which will determine whether the bacillus is contained or killed within a granuloma or grows uncontrollably. There is an overall genetic resistance toward developing leprosy, with more than 90% of people worldwide having a natural immunity.50 Early innate immune responses to mycobacteria binding to these pattern recognition receptors and entry into the cell regulates cellular metabolism to activate NF-κB and vitamin D receptor pathways to upregulate cytokine production and genes that are critical to form and maintain granulomas required to contain the bacilli, including TNF, interferon gamma (IFN-γ) and lymphotoxin alpha. What occurs next is likely determined by the complex interplay of the adaptive immune response involving cell-mediated and humoral immune responses, with T helper 1 (Th1) cytokines and a pro-inflammatory response leading to heightened cell-mediated responses controlling bacterial growth and preventing dissemination, and a shift to T helper 2 (Th2) cytokine production downregulating the inflammatory response and leading to uncontrolled growth, high levels of ineffective antibody responses to bacterial antigens, and progressively worsening disease symptoms.
2902
Epidemiologic studies, including twin studies, complex segregation analyses, and genomewide analyses in various genetically diverse populations from different leprosy endemic countries have indicated the probable importance of host genetics in the susceptibility or resistance to this disease. Twin studies conducted in India in the 1960s and 1970s showed that there was an overwhelming concordance (60%-80%) for monozygotic twin pairs to develop leprosy.51,52 Genomewide analysis studies examining linkage and association of multiple gene candidates suggest that there is genetic control involved in the susceptibility of developing leprosy and a predilection to develop a particular form of disease. Evidence for the latter is seen in Mexico and the Philippines, where 90% of cases develop the lepromatous form of the disease, whereas about equal numbers of patients develop tuberculoid or lepromatous disease in many African countries and in Brazil. Extensive studies have implicated associations with human leukocyte antigen (HLA) complex genes (class I and class II) because of their primary role in the adaptive host immune response, and a number of alleles are overrepresented for leprosy susceptibility or the development of either the tuberculoid or lepromatous subtype when particular ethnic populations in different countries were examined. There is also a shared genetic background between leprosy and a number of inflammatory diseases, including Crohn disease (nucleotide-binding oligomerization domain containing 2 [NOD2]), myocardial infarction (lymphotoxin α [LTA]), Type 1 diabetes and psoriasis (vitamin D receptor [VDR]), and Parkinson disease (E3 ubiquitinprotein ligase [PARK2]).50 More recently, genomewide association studies examining SNP differences between leprosy cases and controls in China have increased the list of genes that may be involved in regulating innate and adaptive immune response pathways associated with susceptibility or resistance to leprosy.53 Fifteen SNPs detected among 6 genes were associated with leprosy (HLA-DR-DQ, RIPK2, TNFSF15, CCDC122, C13orf31, and NOD2), whereas pathway analysis identified a total of 35 genes involved in a single network involved in leprosy susceptibility or resistance. Besides genetic risk factors, many studies have shown that there are a number of other factors, operational or socioeconomic, that increase the risk or predispose individuals toward developing disease. Household contacts living within a dwelling with an untreated multibacillary leprosy index case have the highest risk of eventually coming down with disease, particularly if the household contact is a blood relative to the index case.54 Individuals who have a positive anti-PGL-I titer have up to an 8-fold higher risk of developing leprosy. Other risk factors include living in an endemic or hyperendemic area for leprosy, poverty, living in high-density households with >2 persons sleeping together in a room, poor nutritional status, poor sanitation or lack of clean water, and lack of health care availability.55 Improving these underlying problems would greatly decrease the likelihood of those at risk of leprosy from ever developing this disease.
DIAGNOSIS
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
PATHOLOGY Physiopathology of Leprosy: The routes used by M. leprae to gain access to the target cells, mainly Schwann cells, have always been a matter of discussion. Basically, 4 different pathways have been proposed: (1) naked nerve filaments in the epidermis; (2) entrance of M. leprae in the epidermis, and from there to other Schwann cells; (3) phagocytosis of M. leprae by dermal macrophages, which then invade the perineurium, liberating bacilli to enter Schwann cells; and (4) through the blood, that is, M. leprae could gain access to the nerve by intraneural capillaries. Enlarged endothelial cells could facilitate bacilli entrance to the nerve system, and finally to Schwann cells.56
M. leprae interaction with and engulfment by endothelial cells was identified long ago.57 Armadillo studies showed epineural thickening following M. leprae infection of macrophages of lymphatic and vascular endothelial cells.58 Although this model of infection is well known, it is still not clear how M. leprae is then transferred from those cells to Schwann cells. Once M. leprae reaches the extracellular matrix, PGL-I48
or a histonelike 21-kDa laminin-binding protein59
binds to the laminin α2 chain to invade Schwann cells. The presence of the G domain of α-dystroglycan
23
(α-DG) might be necessary for the adherence of M. leprae to Schwann cells.60 The matrix cytoskeleton link (α-DG, α2-laminin, β-DG) may be the route used by M. leprae to enter the host cell (Fig. 159-20). M. leprae bypass neuregulin receptor (an epidermal growth factor family component) and does a direct bacterial ligation to ErbB2, signaling with no ErbB3 heterodimerization and amplifying Erk1/2 signaling that may induce myelin sheath degradation.61 In addition, using a nonclassical pathway and MEK-independent signaling, M. leprae can activate Erk1/2 directly by lymphoid cell kinase (p56LcK), inducing cell proliferation and maintaining its niche of proliferation.62 On infection, there is an increased expression of 9-O-acetyl GD3 ganglioside, a molecule involved in anti-apoptotic signaling and nerve regeneration (Fig. 159-20). Immunoblocking of 9-O-acetyl GD3 ganglioside on Schwann cells reduces Erk1/2 and cell proliferation.63
M. leprae can dedifferentiate and reprogram adult Schwann cells to stem cell–like cells, possibly using this to promote dissemination of infection.64 Bacilli survival may be maintained by different mechanisms. After invasion (Fig. 159-20), M. leprae interferes with (1) endocytic maturation inhibiting vesicle acidification of phagosomes65; (2) host-cell lipid homeostasis, inducing and accumulating lipid droplets through cytoskeleton reorganization and PI3K signaling, independently of TLR-266; and (3) oxidative pathways, by an intensification of glucose uptake and augmentation of glucose- 6-phosphate dehydrogenase, that once inhibited can decrease M. leprae viability by up to 70%.67
Mechanisms of adhesion, survival, and growth of Mycobacterium leprae cell on interaction
PGL-I Extracellular matrix
Schwann cell
Glucose uptake
9-o-acetyl GD3 ganglioside α2-Laminin α-DG
Antiapoptotic pathway and nerve regeneration
PI3K
Inhibiting of vesicle acidification of phagosome
Accumulation of lipid droplets
Myelin sheath degradation
Myelin
β-DG
MEK-independent signaling (p56LcL)
ERBB2
ERK1/2
Phagosome
Neuregulin receptor ErbB3 heterodimerization
Axon
2903
23
The immune response may initiate at any phase of the host–bacteria interaction. Epidemiologic surveys in hyperendemic areas in Brazil show a high percentage (up to 50% or more) of anti-PGL-I IgM antibodies circulating among schoolchildren, indicating infection with M. leprae followed by an early antibody response against the bacilli.68 Although nerve demyelination may occur in T and B lymphocyte–depleted mice,69
diverse immune reactions occur during infection. There is a well-characterized dichotomy in the human immune response in leprosy, with those at the tuberculoid end of the spectrum having a strong Th1 cell–mediated response whereas those at the lepromatous end have a skewed Th2 response with T-cell anergy present. Tuberculoid leprosy cases have a strong Th1 response, with IL-2, TNF-α, IFN-γ, and IL-12 cytokine production, whereas lepromatous leprosy patients have a Th2 response, with IL-4, IL-5, IL-10 and high levels of antibody production. Those characteristics are found also in the skin, where generally the 2 situations may appear as demonstrated by the progressive disorganization of the immune cells that infiltrate the skin70 in histochemical stained tissue sections of lesions. Tuberculoid leprosy patients present a well-organized granuloma containing epithelioid cells, CD4+ T cells, a good cell–mediated immunity, almost no antibody production, and no bacilli found by slit-skin smear bacilloscopy. On the other hand, lepromatous leprosy patients demonstrate a massive infiltration of foamy macrophages filled with large numbers of bacilli, with few lymphocytes, mostly CD8+ T cells, and a defective cell-mediated immunity with high titers of antibodies to M. leprae antigens, including to PGL-I.71
Toll-like receptors, such as TLR-1, TLR-2, and TLR-4, along with DC-SIGN (CD209) and CD163 may be involved in macrophage/dendritic cell interactions with M. leprae. TLR-1 and TLR-2 have a higher expression in tuberculoid leprosy in comparison with lepromatous leprosy lesions, and TLR-1/TLR-2 heterodimers mediate monocyte and dendritic cell activation, stimulating TNF-α and IL-12 production72 (Fig. 159-19). M. leprae can also stimulate TNF-α, IL-6, and CXCL10 (IP-10) production through TLR-4 signaling in macrophages.73 On the other hand, TLR-2 signaling in Schwann cells is related to apoptosis.74
M. leprae increases IL-10 expression in dendritic cells through DC-SIGN signaling, activating Raf-1, resulting in acetylation of the NFκB p65 subunit after TLR-induced activation of NFκB.75 IL-10 induces phagocytosis by macrophages through DC-SIGN and differentiates monocytes into foamy macrophages by upregulation of oxidized low-density lipoprotein uptake, whereas IL-15 induces the vitamin D antimicrobial pathway, exhibiting less phagocytosis.76 Together with upregulation of DC-SIGN and indoleamine 2,3-dioxygenase, CD163 is also increased and contributes to iron uptake and to the creation of an advantageous environment for M. leprae entry and survival in lepromatous leprosy macrophages77 (Fig. 159-20). M. leprae can modulate NFκB activation in Schwann cells, a function that can be inhibited by
2904
thalidomide.78 Moreover, metalloproteinases 2 and 9 and TNF-α are upregulated in Schwann cells, macrophages and endothelial cells in primary neural leprosy nerves,79 that result in a prominent endoneurial infiltrate, with perineurial fibrosis and enlargement in comparison to non-leprosy peripheral neuropathy.80
Besides the Th1/Th2 cytokine profile, other factors, such as IL-17, cathelicidin LL-37, and insulinlike growth factor I also seem to be important in leprosy physiopathology. VCAM-1 is augmented in the serum of leprosy patients,81 whereas vascular endothelial growth factor and thromboplastin expression is increased by endothelial cells of leprosy patients.82
IL-17 is low in all leprosy patients in comparison to nonleprosy controls, but even lower in lepromatous leprosy.83 Although IL-17-producing CD4+CD45RO+
Th17 cells were increased in peripheral blood mononuclear cells of tuberculoid leprosy patients, IL- 10-producing Foxp3+ Treg cells were 5 times more prevalent in lepromatous leprosy than in tuberculoid leprosy patients, indicating a role for Tregs in multibacillary leprosy development.84 Cathelicidin LL-37, a unique cathelicidin family member of host defense peptides found in humans that is known to modulate the immune response against M. tuberculosis, is low in all leprosy patients85 (Fig. 159-21). Insulinlike growth factor I, known to decrease macrophage antimicrobial capacity, inhibiting M. leprae killing,86 was also found to be low in lepromatous leprosy patients, mostly among those who did not develop Type 2 reaction or erythema nodosum leprosum (ENL).87
ENL, an immunologic Type III hypersensitivity response, occurs with immune complex deposition88
with anti-PGL-I and anti-monocyte chemoattractant protein-I antibodies,89 upregulation of Th17, IL-6, IL-1β, sIL2R, and sIL6R; a decrease of the Treg response; and an influx of neutrophils in the lesions90 (Fig. 159-21). In addition, ENL can be initiated on IFN-γ intradermal injection in lepromatous leprosy patients,91 there is an increase in the CD4+/CD8+ ratio, high serum levels of TNF-α are found,92 and the use of TLR-9 agonists augments TNF-α, IL-6, and IL-1β.93 E-selectin is expressed in a vascular pattern, higher in ENL than in nonreactional lepromatous leprosy patients,94 and FcγRI increases in circulating neutrophils of ENL patients95
(Fig. 159-21). Gene expression analysis showed an increased expression of a “cell movement” biologic group, including P-selectin, E-selectin, and neutrophil adhesion to endothelial cells, with migration and inflammation. In vitro stimulation of TLR-2 induced IL-1β and FcR expression, that together with IFN-γ and granulocyte macrophage colony–stimulating factor, augmented E-selectin expression, and increased neutrophil adhesion to endothelial cells.94 Thalidomide inhibited this neutrophil recruitment pathway, decreases neutrophil influx, FcγRI expression, and TNF-α production. C1qA, B, and C components of the classical complement pathway, and the receptors C3AR1 and C5AR1, were also increased in lepromatous leprosy patients.59
23
Immunology highlights on PB and MB sides of the leprosy spectrum
TT LL
T
T
T
TT
T
T
T
T
T
T
T
T
T
DC
TLR-2 TLR-1
IL-12
Monocyte
TNF-α
IL-2
INF-γ Th1
CD4+ Reversal Reaction
VEGF IL-1β IL-10 IL-17
IL-17 IGF-I IL-2 CXCL-9 TNF-α IL-17A IFN-γ G-CSF IL-10 Treg
Well-organized granuloma
LL
LL
TLR-4
CD163 DC
Fe+
P65/NFκB
IDO
Raf-1
IL-10
oxLDL
DC-SIGN
IL-5 IL-4
LB
Th2
Ab
Erythema Nodosum Leprosum
IL-1β IL-6 sIL2r sIL6R Neutrophils TNF-α FcγRi E-selectin CD4+/CD8+
Th17
Massive infiltration of foamy macrophages
Increase of VCAM-1, VEGF, and tromboplastine Decrease of cathelicidin LL-37
Treg
Type 1 reaction or reversal reaction, a Type IV hypersensitivity immune response, is caused by a specific increase in cell-mediated immunity against M. leprae, and may rapidly evolve to nerve damage. Together with an increase of CD4+ T cell infiltration associated with IL-1β, IL-2, TNF-α, and IFN-γ upregulation96 (Fig. 159-21), an augmentation of CC chemokines monocyte chemoattractant protein-I and RANTES97 is observed. Also, vascular endothelial growth factor, IL-10, CXCL-9, and IL-17A were demonstrated to be upregulated on the reversal reaction onset, together with downregulation of IL-10 and granulocyte colonystimulating factor. This profile was related to a decrease of CD39+CCL4+CD25++ regulatory T-cell subsets and an increase of GNLY, GZMA/B, and PRF1 genes associated with cytotoxic T cell.98
LABORATORY TESTING
Further reduction in leprosy would require the diagnosis of those in the early stages of disease to allow treatment to prevent nerve damage and impairment, but it is estimated that most patients experience up to 2 years delay in diagnosis.99 Reasons for this are complicated, but include a reduction in the numbers of trained leprosy clinicians and laboratory technicians worldwide and the incorporation of leprosy diagnosis into the general family health delivery system, resulting in increased levels of misdiagnosis or delays in
beginning treatment. When there are doubts about the clinical diagnosis, laboratory tests can be used to assist or confirm a presumptive case of leprosy. The clinical spectrum of leprosy shows a range of pathologic manifestations in skin lesions and nerve damage that is aligned with the competence of the host’s immune response, and is dependent on the strength and interaction of both cell-mediated and antibody responses.100 The standard for laboratory diagnosis in a skin biopsy is the detection of acid-fast bacilli by the Fite-Faraco modification of the carbol fuchsin technique and characteristic cellular histologic patterns that make up the immunopathologic types of leprosy as detected by hematoxylin–eosin staining. The widely used Ridley-Jopling classification system26 divides the disease into 5 forms based on the number of acid-fast bacilli and the degree of lymphocytic infiltration and organization, as described in pathology (above). Bacilloscopy of multiple skin biopsies or slit-skin smear can establish the bacillary index on a logarithmic scale, which can range from 0 (no acid-fast bacilli detected in tuberculoid leprosy lesions) to 6+ (>1000 acid-fast bacilli per field in lepromatous leprosy) (Fig. 159-22). For treatment purposes, detection of acid-fast bacilli in skin lesions or slit-skin smear automatically places the patient in the multibacillary category to receive 12 months of multidrug therapy. There is currently no laboratory test capable of diagnosing leprosy or identifying asymptomatic individuals who are progressing toward developing
2905
23
early symptoms, so the development of a simple and cheap test that could assist health professionals to correctly diagnose the disease based on immunologic or metabolomic biomarkers of infection is desirable. A number of research groups have developed a variety of tests that partially achieve this goal, measuring antibody titers to mycobacterial antigens by rapid lateral flow devices; cell-mediated cytokine release assays (such as the detection of IFN-γ, similar to commercial whole blood assays used to detect infection by M. tuberculosis); amplification of mycobacterial DNA by PCR; or the use of metabolomics to detect molecular features specific to M. leprae infection in the blood or urine. Laboratory assays adapted to assess leprosy patient antibody titers to the M. leprae– specific antigen, PGL-I, have been in use for more than 30 years101,102 and include enzyme-linked immunosorbent assays and lateral flow devices that use the soluble synthetic disaccharide of PGL-I coupled to either bovine or human albumin, called ND-O-BSA or ND- O-HSA, respectively. Another is the protein antigen LID-1, composed of the fusion of 2 well-recognized M. leprae proteins, ML0405 and ML2331, that is recognized by >95% of lepromatous patients.103 Coupling the synthetic disaccharide of PGL-I to LID-1 and incorporating this NDO-LID glycoprotein in a lateral flow test resulted in enhanced sensitivity to detect leprosy patients, even those at the paucibacillary end of the spectrum.104 Another group has combined lateral flow assays with up-converting phosphor reporter technology to assess both anti-PGL-I titers along with T cell–mediated cytokine responses (IFN-γ, IL-10, and others) in a single sample. The ability to quantitate the ratio of inflammatory Th1 cytokines versus downregulating Th2 responses provides more information about the complex interplay of cellular and humoral immunity within individuals that can be used to better predict those with asymptomatic infection or who are progressing to disease.105,106 Another method that has been used to diagnose difficult cases is the molecular detection of the M. leprae–specific repetitive RLEP sequence by PCR. Because there are 37 copies
2906
of the RLEP sequence in the genome, this enables the detection of as few as 3 bacterial genomes in a sample. Recent evidence indicates that individuals who are RLEP PCR positive in biopsies of skin lesion sites, earlobe slit-skin smear, or the nasal turbinate as well as having a positive anti-PGL-I titer likely have asymptomatic infection and are at the highest risk of developing disease.49 Our own household contact studies in hyperendemic areas in Pará, Brazil, support these findings. Initial results of multiple families living in “hot zones” indicated that in many instances >80% of household contacts had a positive anti-PGL-I titer, >70% were positive for RLEP by PCR in slit-skin smear, with up to 65% being positive for both biomarkers, demonstrating extreme rates of infection, with 1 or more individuals in each household diagnosed with leprosy based on clinical signs (Salgado et al, unpublished observations). Finally, metabolomics has been used to identify molecular features found in the serum of leprosy patients, indicating that there was an increase of circulating polyunsaturated fatty acids and phospholipids in individuals with lepromatous disease.107 A recent report has even shown that molecular features of infection can be identified by mass spectrometry simply by pressing silica plates against patient skin lesions.108 Moreover, the leprosy miRNome sequencing has been recently published, and revealed new markers involved on leprosy physiopathology109
Although advances have been made in identifying biomarkers of infection by many research groups, translating this to a rapid, cheap, point-of-care test that will aid in diagnosing all patients throughout the leprosy clinical spectrum, including asymptomatic individuals, has a long way to go. Currently, leprosy diagnosis must remain in the competent hands of welltrained leprosy clinicians and health care workers. We have shown the importance of targeting schoolchildren in school-based surveillance and followup of household contacts of those diagnosed children to detect cases early in the disease process. The use of a Geographic Information System, spatial analysis tools, and laboratory tests (anti-PGL-I enzyme-linked immunosorbent assay and RLEP PCR) has enhanced the ability to identify “hot zones” within hyperendemic cities,110,111 which can then allow focused targeting of foci of infection by community health care agents working in local areas. Nevertheless, given the complexities of examining, diagnosing, and ensuring treatment to individuals living in hyperendemic areas,15 developing a simple laboratory test to diagnose leprosy early is highly desirable and would facilitate breaking the lines of transmission to eventually reach the goal of leprosy elimination.
HISTOPATHOLOGY
Skin biopsies should include the dermis and, if possible, subcutis of a lesion. Hematoxylin–eosin staining is complemented using the Fite-Faraco staining method or another method to detect acid-fast bacilli.
A
23
B
C
Histopathologic findings are graded according to the Ridley and Jopling scale.26 The tissue response in Indeterminate leprosy is nonspecific. The normal epidermis or basal layer of the skin show melanin reduction. Perivascular or perineural, superficial and deep dermal infiltration by few macrophages and lymphocytes are common findings. Sometimes the infiltrate surrounds skin appendages and rarely there are bacilli in nerves (Fig. 159-23). Tuberculoid leprosy shows an epidermis that is usually normal and the subepidermal clear zone is absent. There is a noncaseating dermal granulomatous process composed chiefly of activated macrophages (epithelioid cells) with CD4+ T cells in the center of the epithelioid cells, CD8+ T cells in the mantle surrounding the granuloma, and giant cells of the Langhans type. Granulomas may contact the epidermis and are often arranged around nerves and vessels. Peripheral nerve involvement, cellular infiltration of sweat glands, and invasion of the arrectores pilorum muscle by a granulomatous infiltrate is common. There are no acid-fast bacilli or when they are present are found more frequently within peripheral nerves, arrectores pilorum muscle, or even granulomas112,113 (Fig. 159-24). The histopathology of the borderline-tuberculoid form can be distinguished from tuberculoid leprosy by the presence of a subepidermal grenz zone. In general, there is no well-defined granuloma with organized collections of epithelioid cells, and there is a reduction in the frequency of lymphocytes and scarce Langhans cells with rare acid-fast bacilli (Fig. 159-25).
In borderline-borderline, there are aggregates of epithelioid cells, scarce dispersed lymphocytes, no Langhans multinucleated giant cells, and increasing numbers of acid-fast bacilli (Fig. 159-26). Borderline-lepromatous leprosy shows a subepidermal grenz zone, aggregates of macrophages, occasional epithelioid cells with abundant cytoplasm, and some foamy cells, with few lymphocytes. A great number of bacilli and some globi can be found (Fig. 159-27).114
In lepromatous leprosy there is a normal to flattened epidermis, subepidermal grenz zone, aggregates and sheets of foamy macrophages admixed with predominantly CD8+ lymphocytes and plasma cells throughout the dermis and into the subcutaneous fat. Huge numbers of acid-fast bacilli and globi are found within foamy macrophages (Virchow cells), nerves, arrectores pilorum muscle, follicular epithelium, and sweat glands (Fig. 159-28). Histoid leprosy is characterized by epidermal atrophy, a subepidermal grenz zone, and a dermis showing sheets of predominantly spindle-shaped cells with nuclear pyknosis and foamy cytoplasm, vacuolated, and arranged in a storiform pattern. Some polygonalshaped cells, macrophages, and inflammatory cells are present. Some cases may show a pseudocapsule. The lesion resembles a fibrohistiocytic tumor (Fig. 159-29). The Fite-Faraco stain reveals a large number of acidfast bacilli, mostly as rafts or globi (Fig. 159-30). Bacilli can be located in nerves, Schwann cells, eccrine glands, and in the vascular endothelium. CD68-positive macrophages and spindle cells are present in histoid leprosy.115
2907
23
A
B
C
In leprosy reversal reaction, the histopathologic features are edema both extracellular as in epithelioid cell granulomas, increased number of lymphocytes and Langhans giant cells in the infiltrate, small collections of epithelioid cells, as well as a poorly organized
B
A
granuloma. Fibrinoid necrosis is present in severe cases of reversal reaction. Bacilli are found in macrophages and nerves (Fig. 159-31). The downgrading reaction reveals aggregates of foamy macrophages, a remarkable reduction or complete absence in the
C D
2908
A
23
B
C
number of lymphocytes, and acid-fast bacilli in greater numbers.116,117
ENL or Type 2 reaction. The characteristic histologic features are edema and a mixed inflammatory infiltrate
A
in the dermis and in the subcutis, predominantly neutrophils with eosinophils, lymphocytes, aggregates of foamy macrophages, plasma cells, and mast cells. Vasculitis and a mixed lobular and septal panniculitis
B
C
2909
23
A
B
C
are present in most cases (Fig. 159-32). Bacilli in large numbers, usually granular in appearance, are easily found. The predominant lymphocyte present in ENL is the T-helper cell, whereas T-suppressor cells predominate in the lepromatous leprosy.117,118
A
Lucio phenomenon or erythema necrotisans. The main microscopic features are that of a cutaneous or subcutis necrotizing vasculitis. There is fibrinoid necrosis of small and medium-sized vessels. The other histologic picture reported in Lucio phenomenon are necrosis of
B
C
2910
A
23
B
epidermis and superficial dermis, micro-abscess formation, angiogenesis, endothelial swelling, vascular occlusion caused by luminal thrombi, and deposits of fibrin in small blood vessel walls of the dermis and the subcutis. There is a mixed dermal and/or subcutis
A
infiltrate of neutrophils, eosinophils, lymphocytes, and nuclear dust. Bacilli are found in endothelial cells, in blood vessels, nerves, arrectores pilorum muscle, follicular epithelium, sebaceous glands, and sweat glands.119-122
B
C
2911
23
A
B C
NERVE CONDUCTION STUDY— ELECTRONEUROMYOGRAPHY
Leprosy neuropathy manifests as asymmetric focal or multifocal lesions, mononeuropathy or mononeuritis multiplex, caused by the direct damage of nerves by M. leprae and by an inflammatory immune response of the host. There is chronic neuropathy, with acute exacerbations resulting from reversal reaction or ENL. Besides focal lesions, entrapment of the enlarged nerves is also a concern, that may require surgical intervention to decompress the nerve. Evaluation includes nerve palpation, pain evaluation, sensory assessment, muscle power measurement and autonomic examination. Electroneuromyography is a refined tool for nerve function assessment at diagnosis, and for patient followup to detect and characterize new lesions, especially during reversal reaction or ENL, or to evaluate entrapment syndromes and neuropathic pain. Leprosy neuropathy starts with Schwann cell demyelination that may evolve to axon loss. Commonly affected sites include the elbow for the ulnar nerve, the carpal tunnel for the median nerve, the fibula head for the fibular nerve, and the tarsal tunnel for the posterior tibial nerve, all which are key areas for evaluating neuropathy.123
IMAGING
High-resolution ultrasound use for peripheral nerve evaluation is an established procedure. However, only
2912
recently has it seen more use in the evaluation of nerve function impairment in leprosy neuropathy. Clinical examination of nerve enlargement may be difficult to measure, even for experienced leprologists, and there are no robust parameters to be recorded to followup the leprosy patient during and after multidrug therapy. High-resolution ultrasound can be used for evaluation of echogenicity, vascularity, and nerve thickening, using objective parameters and values for several neuropathies, including leprosy.124 In addition, nerve abscesses and entrapment also can be detected early and evaluated.123 Its utilization for leprosy neuropathy evaluation is still evolving, but very promising. Echogenicity abnormalities, intraneural Doppler and post-multidrug therapy cross-sectional areas above normal limits, with less than 30% reduction, have been linked to poor outcomes. Worsening of nerve abnormalities after multidrug therapy were found independent of leprosy classification or presence of reactions.125
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
See Fig. 159-33.
DIFFERENTIAL DIAGNOSIS
See Table 159-1.
Thickened nerves with sensitivity or motor function impairment?
Ask patient to remove clothes, examine all skin surface and palpate nerve trunks
Skin lesions with altered sensitivity? Only thickened nerves? Yes
Autonomic alterations?
Leprosy diagnosis algorithm
or
or
No Not leprosy
-
Test sensitivity on the nerve territory
-
Test motor function
Normal
Altered 1 or 2
23
Diffuse infiltration, nodules and autonomic dysfunctions
Many thickened nerves
Leprosy
LL
Many infiltrated lesions, associated or not to nodules
Many thickened nerves
Leprosy
BL
One or many infiltrated lesions, that may be foveolar
Usually, more than one thickened nerve
Leprosy
BB
One or a few infiltrated lesions
Leprosy
BT
One or a few tuberculoid lesions
No more than one thickened nerve
Leprosy
TT
No thickened nerves
One or a few hypochromic lesions
No autonomic alteration
Indeterminate
Leprosy
23
Primary Lesions
■Macules and patches. The hypopigmentation of pityriasis alba and indeterminate leprosy mimic each other. If the patient was born in, or had resided in, an endemic area, then the distinction between the two may be made by neurologic or histologic examination. Hypopigmented BL plaques can be so faintly indurated as to mimic patches. Telangiectasias may be eruptive or present as mats on the face and upper trunk.
■Papular to nodular lesions. In the dermis, leprosy may mimic, or be mimicked, by dermatofibromas, histiocytomas, lymphomas, sarcoidosis, neurofibromatosis, syphilis, anergic leishmaniasis, paracoccidioidomycosis, chromoblastomycosis, sporotrichosis, lobomycosis, tuberculosis, and other granulomas. Eruptive and recurrent inflammatory subcutaneous nodules may be ENL, erythema nodosum, erythema induratum, and vasculitis. Palpable, but not visible, subcutaneous nodules in Lucio leprosy may mimic lipomas.
■Plaques. Erythematous plaques may mimic mycosis fungoides. Plaques without pigmentary change may be wheal like in appearance, causing confusion with urticaria. Hypopigmented plaques may mimic papulosquamous eruptions. Islands of normal skin within a plaque may suggest psoriasis.
■Polymorphous vesiculobullous eruption/Dermoepidermal separation. They may occur in ENL. IgM is deposited not uncommonly at the epidermal basement membrane in LL. These antibodies are not necessarily pathogenic but may confuse diagnosis.
■Annular lesions. Leprosy may mimic, or be mimicked by, annular erythemas, sarcoidosis, syphilis, or tinea.
Secondary Lesions
■Infarcts. Lucio phenomenon lesions and necrotic ENL mimic septic infarcts.
■Ulcers. Ulcers occur in Lucio phenomenon and ENL secondary to vascular occlusion. In patients with nerve destruction, neurotrophic ulcers occur on the plantar surface, patients with Leg ulcers secondary to venous insufficiency are seen in Lucio leprosy.
Clinical Constellations
Clinical Constellations
■Systemic lupus erythematosus–like changes. Fusiform fingers, swan neck deformity, false positive syphilis tests, antiphospholipid antibodies, lupus anticoagulant, hyperglobulinemia, and anemia.
■Systemic lupus erythematosus–like changes. Fusiform fingers,
swan neck deformity, false positive s y,y yphilis tests, antiphospholipid antibodies, lupus anticoagulant, hyperglobulinemia, and anemia.
■Vasculitis. A true vasculitis may occur in ENL, Lucio phenomenon, and Lucio leprosy. Clinically, leprosy lesions of a nodular character may be misdiagnosed as “vasculitis.”
■Vasculitis. A true vasculitis may occur in ENL, Lucio phenomenon,
and Lucio leprosy. Clinically, lepros y,y y lesions of a nodular character may be misdiagnosed as “vasculitis.”
CLINICAL COURSE AND PROGNOSIS
One of the most important problems during the leprosy clinical course is the appearance of acute or subacute episodes of inflammation, defined as reactions. Leprosy reactions, caused by immune response against M. leprae antigens, are divided into Type 1 or reversal reaction, involving mainly peripheral nerves and skin, and Type 2 or ENL, that may have localized or systemic symptoms. Acute neuritis also may be considered as a type of reaction. Reactions never occur in Indeterminate patients. Up to 50% of all patients on multidrug therapy may present reactions during treatment, but these reactions can also occur before and after therapy. Neuropathy present at the time of diagnosis, multibacillary leprosy,
2914
extent of the disease, and the presence of lesions overlying peripheral nerve trunks are factors that increase the risk of reactions and nerve function impairment.126
Reversal reaction and ENL may happen together in some patients (Table 159-2). Reversal reaction can occur in up to 30% of patients, whereas tuberculoid leprosy cases are seldom affected,127 the majority of the reactional episodes occur in borderline forms, mainly borderlinelepromatous and borderline-borderline, followed by lepromatous leprosy.128 It starts as a sudden worsening of skin lesions and nerve function impairment, with no apparent systemic involvement. Besides prereactional lesions presenting more infiltration and desquamation, previous and newly developing lesions may be bright red, hot, and sensitive to the touch (Fig. 159-34), sometimes ulcerated, frequently associated with peripheral nerve enlargement, and usually accompanied by pain. Reversal reaction requires immediate intervention, because it can result in nerve impairment and permanent disabilities. ENL is an aggressive vasculitis with immune complex deposition affecting different organs, resulting in, among other sequelae, neuritis, panniculitis, glomerulonephritis, arthralgia, epididymitis, orchitis, eye inflammation, osteitis and lymphadenitis with systemic symptoms such as fever, edema and malaise.129
REVERSAL REACTION (TYPE I) ERYTHEMA NODOSUM LEPROSUM (TYPE II)
Predominant leprosy subtype
Borderline-tuberculoid Borderline-borderline Borderline lepromatous Lepromatous leprosy
Lepromatous leprosy
Signs and symptoms Acute worsening of skin lesions Acute worsening of nerve function impairment No apparent systemic symptoms
Erythema nodosum Erythema polymorphous Severe cutaneous necrotizing vasculitis Fever, edema, malaise
Extracutaneous involvement Neuritis Neuritis Panniculitis Glomerulonephritis Arthralgia Epididymitis Orchitis Eye inflammation Osteitis Lymphadenitis
Treatment Prednisone (1-2 mg/
Thalidomide
Treatment Prednisone (1-2 mg/ kg/d with slow taper ∼3 mo)
Thalidomide 100-400 mg/d AND prednisone (1-2 mg/kg/d) OR Pentoxifylline 400 mg thrice a day
kg/d with slow taper ∼3 mo)
100-400 mg/d AND prednisone
(1-2 mg/kg/d) OR Pentoxifyfyf lline 400 mg
thrice a day
A
23
B
C
A high bacillary index and diffuse skin infiltration are important risk factors130 and 65% of the cases have more than one episode of ENL.131 The main skin manifestation is erythema nodosum, more palpable than visible (Fig. 159-35), and may be accompanied by erythema polymorphous or severe cutaneous necrotizing vasculitis (Lucio phenomenon) (Fig. 159-36). Immunologic disorders, like HIV and HTLV infections, immunosuppressive drugs, or immunobiological medications can interfere with the resolution of leprosy. The first case of leprosy occurring as a result of immune reconstitution inflammatory syndrome (IRIS) in an HIV-infected individual was described in 2003.132 The upgrading of the cell-mediated immune response due
to antiviral therapy in AIDS patients is now well recognized in IRIS,133 and the percentage of HIV and other viral infections in leprosy patients is high, indicating that all leprosy patients should be tested for HIV, HBV, HCV and HTLV-1.134 Viral coinfection decreases the
2915
23
survival of leprosy patients,135 whereas increasing rates of neuritis, nerve function impairment, and leprosy relapses.134 Anti-TNF therapy can result in the development of clinical leprosy in infected individuals following cessation of the immunobiological medication136-138 regardless of whether reactional episodes are involved. It is important to distinguish reactions from relapses. Reactions may occur before, during, and a few years after multidrug therapy. Usually, they are acute, with a rapid appearance of new lesions and infiltration of the old ones, deterioration of neural function, and/or systemic involvement, responding well to treatment with antiinflammatory drugs. On the other hand, relapses in general are slowly progressing, almost always with resurgence of primary lesions followed by the gradual appearance of new lesions, together with nerve involvement, and, in contrast, there is no response to antiinflammatory drugs. A true relapse must be defined after confirmation of completion of the first treatment by the patient. If the full course of treatment is confirmed, it becomes necessary to test for drug resistance, although reinfection cannot be ruled out. If the patient was wrongly classified, then an insufficient length of therapy may be the case. Histopathology can be useful to distinguish a reaction from a case of relapse.139
Although leprosy is well known for loss of skin sensation, neuropathic pain may arise during or after multidrug therapy, due to tissue inflammation or dysfunction of the nervous system.140 Nerve trunk pain onset may be spontaneous or appear after palpation, either abrupt or insidious, but many patients experience recurrent episodes. More than half of the patients have some pain episode during or after multidrug therapy, with a higher prevalence in lepromatous leprosy, decreasing toward the borderline and tuberculoid forms. The most affected nerves are ulnar and tibial.140
If the pain persists during treatment, or becomes longlasting after completing multidrug therapy, it may be defined as chronic neuritis or neuropathy.141
MANAGEMENT
INTERVENTIONS
INTERVENTIONS
MEDICATIONS
There are, basically, 3 groups of medications used for treating leprosy: antibiotics, antiinflammatory or immunosuppressants and analgesic drugs. The first group, antibiotics, has a well-defined standard for treatment, the WHO Multidrug Therapy drug regimen, that contains rifampicin and dapsone, with or without clofazimine, in monthly blister packs. Antiinflammatory drugs, usually prednisone and thalidomide, are prescribed to control leprosy reactions by reducing inflammation, whereas analgesics are used to control neuropathic pain. Before the discovery of sulfones’ power to improve leprosy signs by Guy Faget in 1941,142 chaulmoogra oil, drug used in India for decades, was the only commonly
2916
used treatment for leprosy, although its efficacy was questionable, as it generally induced only a localized inflammatory response in the skin. Dapsone is a simple, low-cost, highly effective drug for leprosy, used in a daily dose of 100 mg or 1 to 2 mg/kg. The drug is absorbed by the GI tract and eliminated through the kidneys. It is usually well tolerated, although it is dependent on the presence of the enzyme glucose 6-phosphate dehydrogenase (G6PD), an X-chromosomally transmitted enzyme, that is lacking in 400 million people worldwide, mostly in tropical areas where malaria is present143 and also where leprosy is prevalent. G6PD deficiency leads to serious hemolytic events by oxidative stress, including the formation of methemoglobin that is clinically detected as a violet color on sclera, lips, and the extremities of fingers together with malaise, headache, and dyspnea. In addition to a high level of hemolysis, G6PD-deficient patients using dapsone are at a greater risk of developing severe life-threatening hemolytic anemia, and must change their medication.144 Dapsone hypersensitivity syndrome, a rare but potentially fatal event, presents with fever and cutaneous rash, eventually involving internal organs, especially the lungs, with eosinophilic infiltrates and pneumonitis. It may occur at any time during treatment, and it may be related to drug rash with eosinophilia and systemic symptoms (DRESS syndrome).145
Clofazimine is a pigment that, in addition to its unknown antibiotic mechanism, also has antiinflammatory properties. The main objection as far as patients are concerned is its affinity to fat tissue and macrophage deposits leading to skin hyperpigmentation, especially in the lesions. An additional side effect is skin dryness that together with pigmentation, gives the skin a highly xerodermic appearance (Fig. 159-37). It is used in a dose of 300 mg once a month, and 50 mg per day, only in multibacillary patients. Clofazimine is well-tolerated by leprosy patients.146
Rifampicin is highly bactericidal, and unlike the daily administration of dapsone and clofazimine, it is
only administered once per month with supervision, 450 mg to children and 600 mg to adults. Adverse effects include face and neck redness, pruritus and cutaneous rash, loss of appetite, nausea, vomiting, and diarrhea, malaise (which may require cessation of the drug), purpura, and epistaxis. Flulike syndrome, a not well-understood immunologic side effect occurring with the use of intermittent doses of rifampicin, is characterized by fever, asthenia, myalgia, and headache, sometimes accompanied by bone pain. Eosinophilia, nephritis, thrombocytopenia, and shock may eventually develop. Although considered rare, it was the major side effect reported in a Brazilian study with 20,667 leprosy patients on multidrug therapy.147
Multidrug therapy schemes used today are the same as 1982 when they were first implemented (Table 159-3), with dapsone, clofazimine, and rifampicin prescribed for multibacillary cases for up to 24 months, or dapsone and rifampicin for 6 months for paucibacillary patients. Pregnancy and breastfeeding do not contraindicate the use of multidrug therapy.144
In the 1960s, together with the confirmation of clofazimine and rifampicin148 efficacy against M. leprae, the first cases of dapsone-resistant leprosy appeared.149 In the 1970s, WHO decided to replace dapsone monotherapy in favor of a 3-drug strategy with dapsone, rifampicin, and clofazimine combined in a new drug regimen to treat leprosy called multidrug therapy. Although drug resistance in leprosy appears to remain low,150 reports of MDR-leprosy are increasing in the literature,151-153 and it may be a concern for leprosy treatment in the near future.154 The substitute drugs available, either to resistant strains or to patients with side effects on multidrug therapy, ofloxacin, minocycline, or clarithromycin (Table 159-3), appear to be safe and effective for leprosy treatment,146 but new alternative drugs are necessary. Although there are a few well-structured clinical trials for treating nerve damage in leprosy, with moderate-quality evidence, including one with intravenous
23
methylprednisolone pulse therapy,155 WHO recommends leprosy reactions must be immediately treated with antiinflammatory or immunosuppressant drugs.144 The most widely used are corticosteroids and thalidomide. Reversal reaction can be treated with prednisone at doses of 1 to 2 mg/kg/d in a regressive scheme, diminishing 10% to 15% of the dose every 15 days, with a complete cycle of treatment lasting up to 3 months. If there is a worsening of the clinical situation, it may be necessary to go back to the previous higher dose, extending this level of corticosteroid treatment for 30 to 45 days, followed by tapering off again. Glucose levels and blood pressure must be controlled during the use of corticosteroids. Glaucoma, cataracts, moon face, striae, adrenal gland atrophy, and osteoporosis may occur with long term usage, and as with other immunosuppressive agents, other infectious diseases, such as systemic fungal infections and tuberculosis may arise. In addition, Strongiloydes stercoralis hyperinfection is a concern. Ivermectin 200 µg/ kg/d for 2 days, repeated after 2 weeks, can be used in prevention.156 After an equivalence conversion calculation, prednisone may be replaced by other steroids, including its metabolite prednisolone, dexamethasone, or deflazacort. Calcium intake of 1200 to 1500 mg/d and vitamin D supplements are recommended for any patient using glucocorticoids, independent of dose and duration of therapy.157
ENL may be treated with 100 to 400 mg/d of thalidomide. As thalidomide is a teratogenic drug, it is mandatory to test for pregnancy and prescribe 2 contraceptive methods before starting therapy in women of childbearing age. Usually, ENL appears with nerve damage, and concomitant treatment with steroids is required. Higher doses of prednisone, up to 2 mg/kg/d, are linked to improved nerve function outcome, but if therapy is initiated immediately after the first signs of reaction, lower doses of 1 mg/kg/d may have the same effect.158 If ENL is associated with any other tissue inflammation, like orchitis or iritis, or
RECOMMENDING ORGANIZATION DISEASE TYPE RIFAMPICIN DAPSONE CLOFAZIMINE DURATION FOLLOWUP
World Health Organization
PB 600 mg/mo 100 mg/d — 6 mo No mandated followup. To return as needed
MB 600 mg/mo 100 mg/d 50 mg/d 1 y No mandated followup
300 mg/mo
To return as needed
US Public Health Service
PB 600 mg/d 100 mg/d — 1 y At 6-mo intervals for 5 y
MB 600 mg/d 100 mg/d 50 mg/d 2 y At 6-mo intervals for 10 y
Other Microbicidal Agents Dose
Clarithromycin 500 mg/d
Minocycline (substitute for dapsone or clofazimine) 100 mg/d
Ofloxacin 400 mg/d
Ofloxacin 400 mg/d
PB, paucibacillary; MB, multibacillary.
2917
23
with reactions of the hands and feet, as with osteoarthritis and soft tissue inflammation, steroids are also necessary. In cases where the use of thalidomide must be avoided, pentoxifylline 400 mg, 3 times a day, is an alternative drug, quite useful for controlling limb edema and systemic symptoms.159
Steroids and thalidomide may help patients with neuropathic pain by reducing edema and immunologic reactions targeting the nerve, especially in acute episodes. However, its treatment continues to be a challenge, especially for those with chronic neuritis/ neuropathy. Central nerve system drugs, such as the tricyclic antidepressants amitriptyline and imipramine or the anticonvulsants carbamazepine and gabapentin have been used in an attempt to control chronic neuritis/neuropathy in those patients, but these drugs do not interfere with the nerve damage process, and therefore do not protect leprosy patients from nerve deterioration. Although some anecdotal reports show that immunosuppressive agents, like cyclosporine and azathioprine, may be useful for treating chronic neuritis/ neuropathy patients, a recent trial with azathioprine did not show improvement in patients with reversal reaction.160 More research is necessary in physiopathology and with new drugs for treating neuropathic pain.
PROCEDURES
Simple preventive techniques may be used by patients to prevent the progression of damage. Massage and hydration of the skin of hands and feet are necessary to avoid fissures, ulcers, and fixed claw formation. In addition to the use of special boot soles or customized shoes for feet with loss of sensation and with disabilities, self-examination is mandatory for early detection and immediate treatment of trauma. For hands, adduction, abduction, and opposition movements are necessary to keep trophic muscles and healthy joints. Adaptation of working instruments and household items help to prevent trauma and burns. For eyes, the use of lubricating eye drops may prevent keratitis in cases of lagophthalmos. In more complex cases, the patients may be referred to specialized centers for more complex treatments with a multiprofessional team for physical, psychological, and social rehabilitation. In different stages of leprosy, surgery may be necessary. Nerve abscess is infrequent, appearing more in primary neural leprosy and tuberculoid leprosy and less toward the lepromatous leprosy pole, but it may be the first clinical manifestation161 of disease. In such cases, abscess drainage is mandatory, and the content must be sent to the laboratory for investigation. Nerve decompression may be used to improve leprosy neuropathy and muscular function, albeit there are no reliable clinical trials to definitely prove its usefulness.162
Finally, reconstructive surgery may recover some functional aspects in the hands and feet, such as the ability to hold a glass or the capacity to raise the feet; correct eye problems, like lagophthalmos, preventing keratitis, infection, and blindness; and improve aesthetics as in the surgical correction of nose collapse, which
2918
is nowadays rare,163 or the interosseous and first web space atrophy of the hands.164
COUNSELING
Counseling is a key process involved in leprosy patient management. Nerve damage and its management include counseling and harm reduction.165 Although there was improvement in the last decades by the presence of active social movements fighting against discrimination, helping to reintegrate people into society, and banning discriminatory laws, stigma is still present in modern society. Although curable, leprosy is still a disease resulting in serious disabilities, and even patients diagnosed at the first stages of disease fear evolution through incapacities. Therefore, counseling should be available for every person diagnosed with leprosy, and their families.166 Self-care groups are necessary, but they should not be exclusive. Leprosy-related disability care and management must be included with care for disabilities caused by other diseases in the general health services.167
TREATMENT ALGORITHM
TREATMENT ALGORITHM
See Fig. 159-38.
PREVENTION/SCREENING
PREVENTION/SCREENING
There is one fundament requirement for leprosy prevention, that being contact examination. It should be a mandatory part of any leprosy program in endemic countries to examine all household contacts, and some programs expand this concept to social contacts, those who work or have closer proximity with the index case. A household contact has a 5- to 8-fold higher risk of contracting leprosy than a person without contact with a case (Fig. 159-39). However, even if there is constant vigilance, only up to 30% of the cases in a community will be detected among the household contacts; therefore, other genetic or environmental factors may be involved in the maintenance of the infection.168
Early detection of cases is another tool for the efficient prevention of leprosy. Besides contact examination, leprosy campaigns in the general population or in special communities, such as schoolchildren,110 may be used to raise awareness, to diminish stigma, and to increase detection of early cases of leprosy. Although chemoprophylaxis with rifampicin has shown some degree of protection (57%) in the first 2 years, after 4 years no difference was observed in comparison between rifampicin and placebo groups169; therefore there is no current official recommendation to use chemoprophylaxis in leprosy contacts. For immunoprophylaxis, Brazil has been using Bacillus Calmette- Guerin (BCG) revaccination in contacts for a long time. An 18-year followup study found 56% protection for
23
Leprosy treatment algorithm
Primary Neural Leprosy
Indeterminate Leprosy TT Leprosy
Paucibacillary (PB)
PB MDT
Reversal Reaction (RR)
Check Glucose
Blood Pressure
BT Leprosy BB Leprosy BL Leprosy LL Leprosy
Multibacillary (MB)
MB MDT Erythema Nodosum Leprosum (ENL)
Test pregnancy Contraceptive
Calcium
ENL + RR ENL + Neuritis ENL + Organ inflammation
If pregnant or can’t use contraceptive
Vitamin D
Pentoxy filine
lvermectin Thalido mide
Prednisone oral daily or methylprednisolone pulse IV Associate
or
Chronic Neuritis or Neuropathy (CN)
Tricyclic antidepressants or anticonvuIsants
BCG-vaccinated contacts,170 compared those who were not vaccinated; hence, Brazil guidelines for leprosy continue to include BCG vaccination for all household contacts.
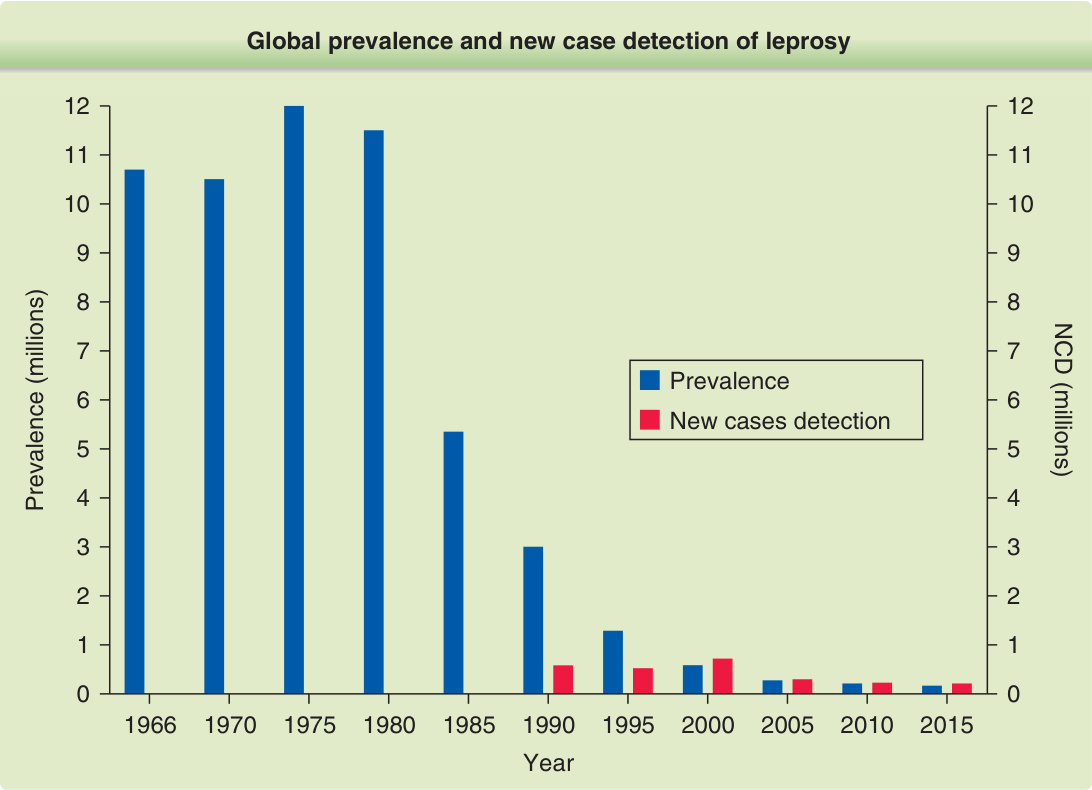
Figure 159-1 Historic evolution of global prevalence and new case detection of leprosy. The first formal attempt to estimate the global leprosy burden was made by WHO in 1966, when the case load was estimated to be 10,786,000, of whom 60% were not registered for treatment. Global detection was first reported in 1991, with 584,000 new cases detected worldwide in 1990. Currently, the new case detection is one of the most important epidemiologic indicators of leprosy burden, together with the proportion of children and proportions of grade 2 disability. (Used with permission from Prof. Josafá Barreto, Pará Federal University, Brazil.)
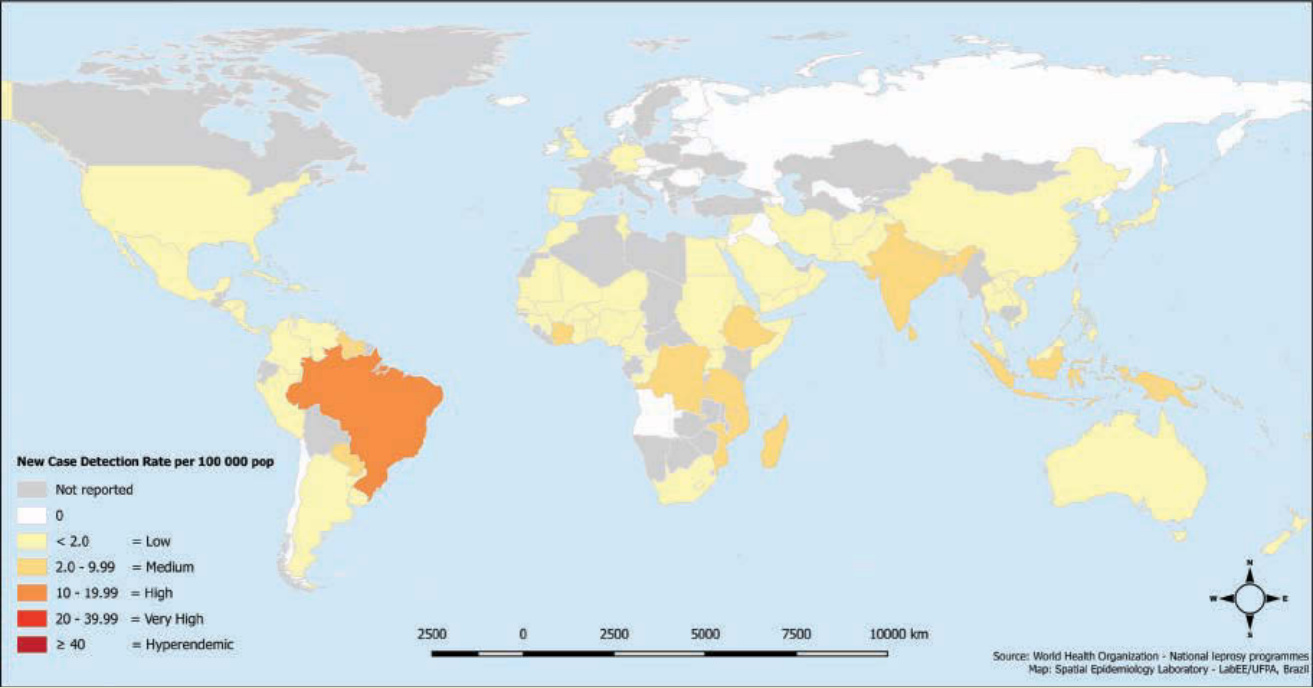
Figure 159-2 Leprosy new case detection rate per 100,000 population in the world, 2015. More than 210,000 new cases were reported in 136 countries or territories in 2015. India, Brazil, and Indonesia accounted for 81% of the global burden of leprosy. The global new case detection rate was 3.2. (Used with permission from Prof. Josafá Barreto, Pará Federal University, Brazil.)
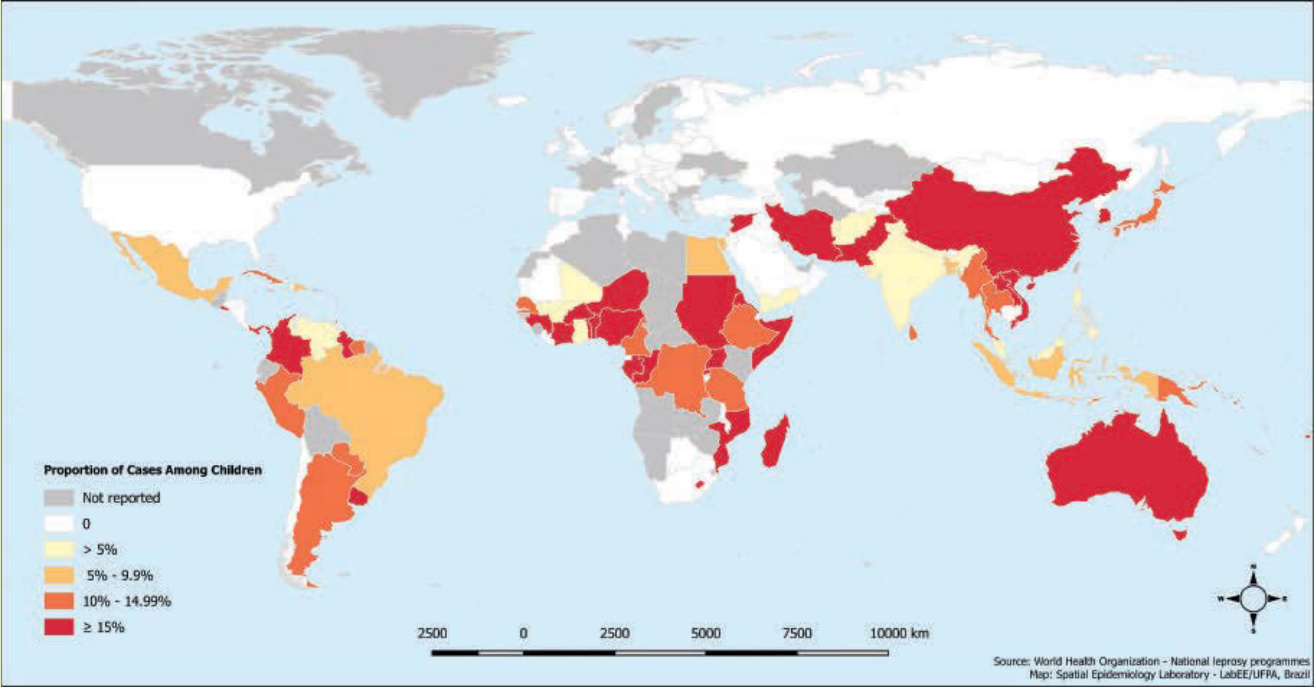
Figure 159-3 Proportion of leprosy cases among children below 15 years old, 2015. Although there is no specific classification from “low” to “high” for this indicator, it is a robust indicative of active source of infection in the community where they live. (Used with permission from Prof. Josafá Barreto, Pará Federal University, Brazil.)
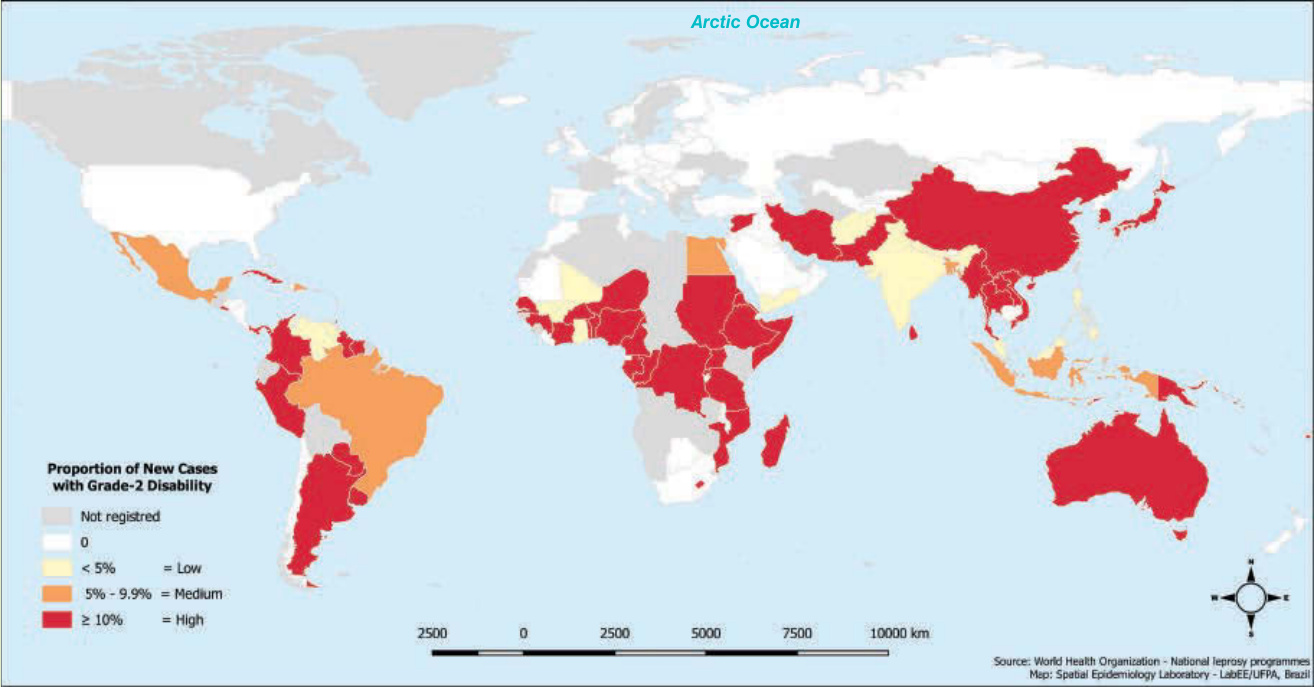
Figure 159-4 Proportion of new leprosy cases with grade 2 disability at diagnosis, 2015. It reflects long delays in the diagnosis of leprosy, highlighting a failure of the health services system and gaps in the approach to control the disease. (Used with permission from Prof. Josafá Barreto, Pará Federal University, Brazil.)
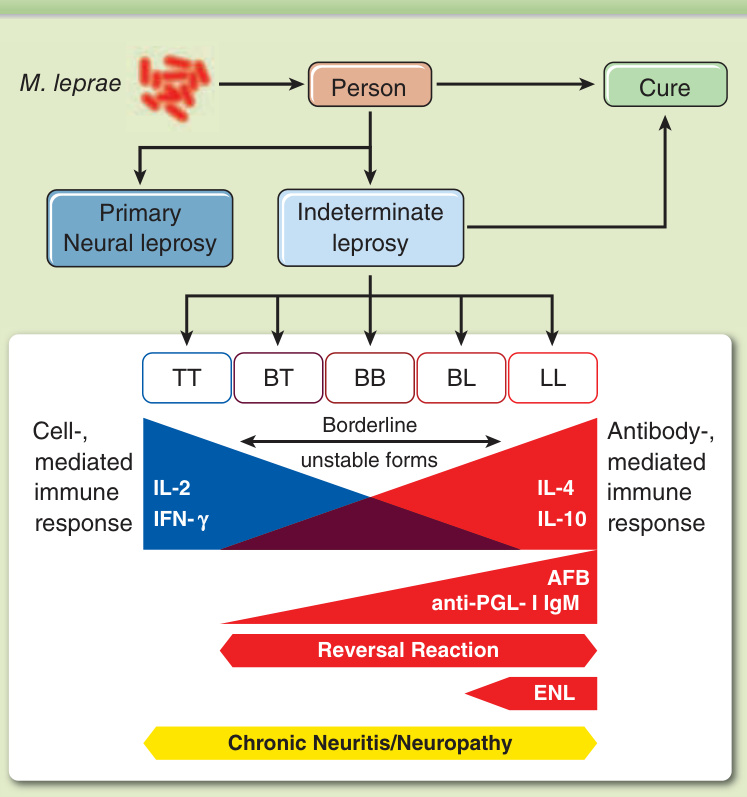
Figure 159-5 Leprosy clinical spectrum. Up to 80% of people exposed to M. leprae may solve the problem and get rid of the bacilli before appearance of symptoms or after subclinical leprosy. Some patients will develop primary neural leprosy, with no skin lesions. All those with skin lesions pass through an indeterminate form, and then evolve to a polar tuberculoid leprosy (TT) or lepromatous leprosy (LL) disease or to an unstable borderline form of leprosy. The paucibacillary (PB) pole toward TT has a good cellular immune response (CIR), with the presence of Th1 cytokines, while multibacillary pole toward LL present an impaired CIR and a high antibody response, with Th2 cytokines. Acid-fast bacilli and anti-PGL-I IgM are, both, low or negative on PB and increase through multibacillary pole. Reversal reaction may happen especially in borderline leprosy, whereas erythema nodosum leprosum occurs in borderline-lepromatous leprosy (BL) and LL patients. Chronic neuritis or neuropathy may happen in primary neural leprosy and in all but the indeterminate leprosy clinical form.

Figure 159-6 Indeterminate leprosy. Macular hypochromic lesion on the lower back.

Figure 159-7 Tuberculoid leprosy. A well-circumscribed lesion, with a central macular hypochromic and atrophic appearance, and a peripheric group of papules distributed in annular pattern.

Figure 159-8 Infantile nodular leprosy. Presence of 2 tuberous lesions on the face of a child from a family where 2 adults were diagnosed with multibacillary leprosy.

Figure 159-9 Lepromatous leprosy. Multiples nodules (hansenomes or lepromes) disseminated throughout the skin, associated to diffuse infiltration.

Figure 159-10 Lepromatous leprosy. Papules, nodules, and infiltration on the ear of a child. He had also many lesions on other parts of the skin.

Figure 159-11 Leonine facies. Lepromatous patient with diffuse nodules and infiltration on the face, resulting in a lion’s face appearance.

Figure 159-12 Lepromatous leprosy histoid or Wade leprosy. Presence of nodules, which may be disseminated or scattered, some resembling molluscum contagiosum lesions, as in the picture, but note the presence of a nodule on the right nipple, and also some infiltration with a claw formation on the left hand.

Figure 159-13 Lepromatous leprosy. Diffuse infiltration of the skin.

Figure 159-14 Borderline-tuberculoid leprosy. Presence of various hypochromic annular lesions, with papules and infiltration on the periphery, located on the buttocks and thighs of a child.

Figure 159-15 Borderline-borderline leprosy. Two foveolar lesions on the upper dorsal thorax.

Figure 159-16 Borderline-lepromatous leprosy. Foveolar and nodular infiltrated lesions.

Figure 159-17 Lagophthalmos on the right eye.

Figure 159-18 Ulcers in a hypotrophic and anhidrotic hand of a LL patient.

Figure 159-19 Fixed claws and bone resorption associated with anhidrosis and atrophy as sequels on the hands of a borderline-lepromatous leprosy patient.
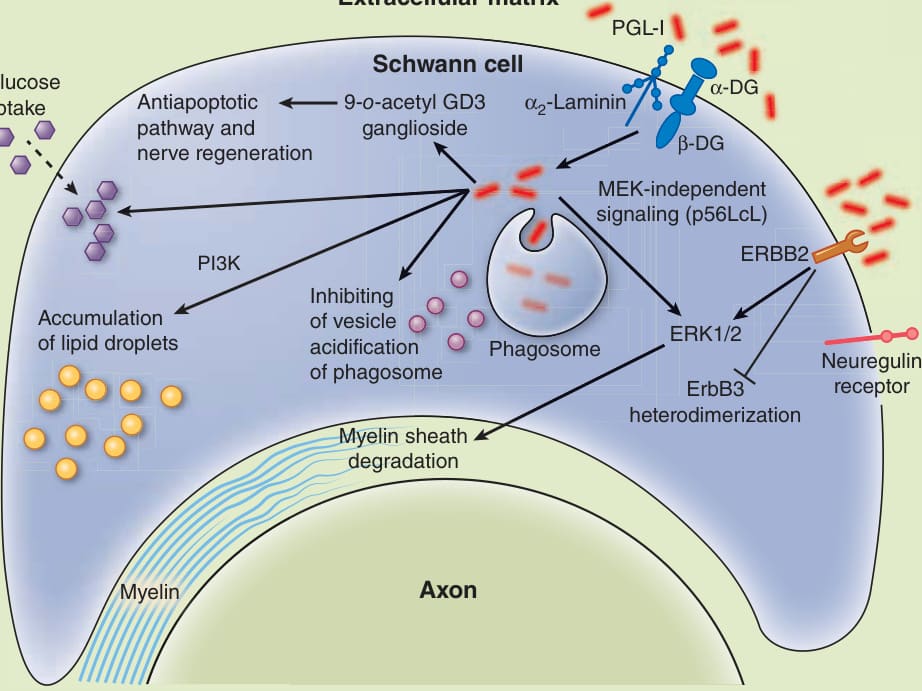
Figure 159-20 Host cell interaction of M. leprae. The figure shows the main mechanisms of entrance and maintenance of the bacteria inside a Schwann cell.
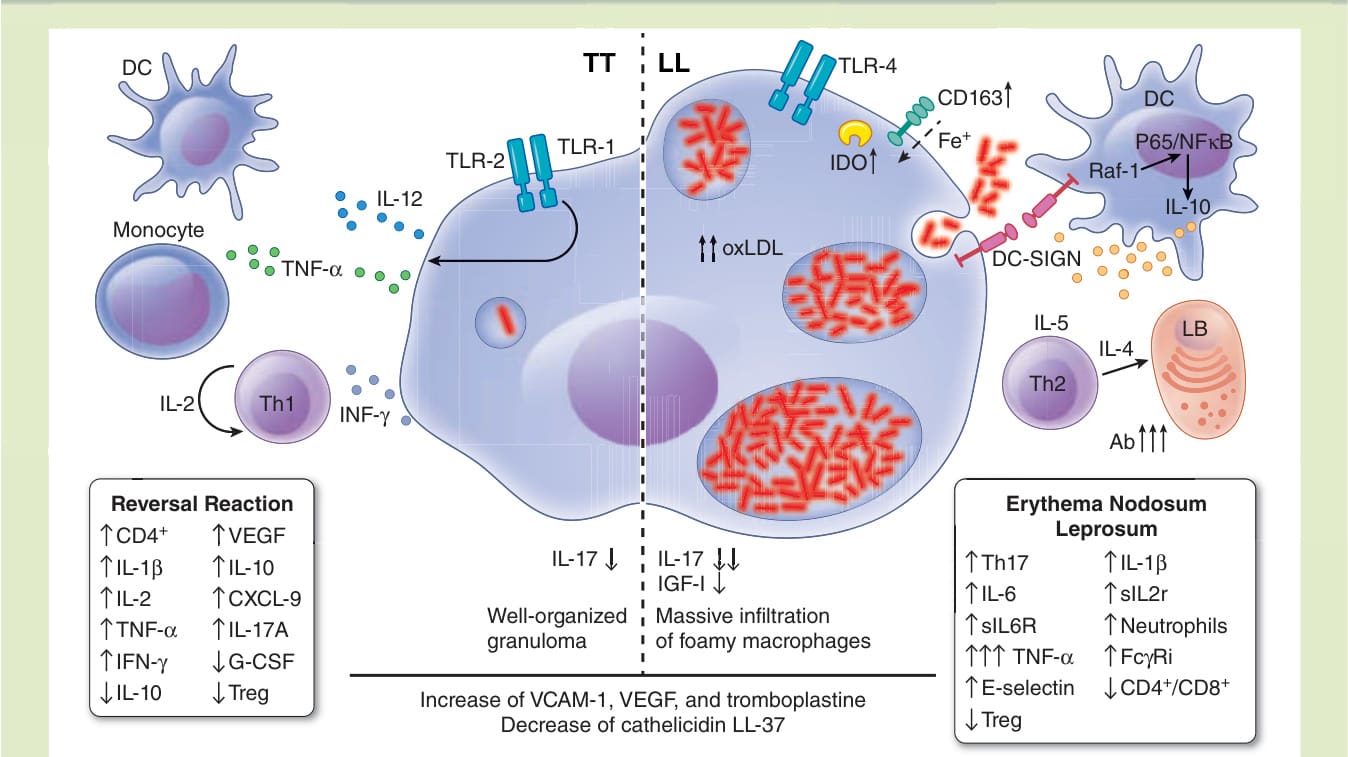
Figure 159-21 Immunology of leprosy. The main differences of tuberculoid leprosy and lepromatous leprosy poles are demonstrated, together with the key variations between reversal reaction and erythema nodosum leprosum.
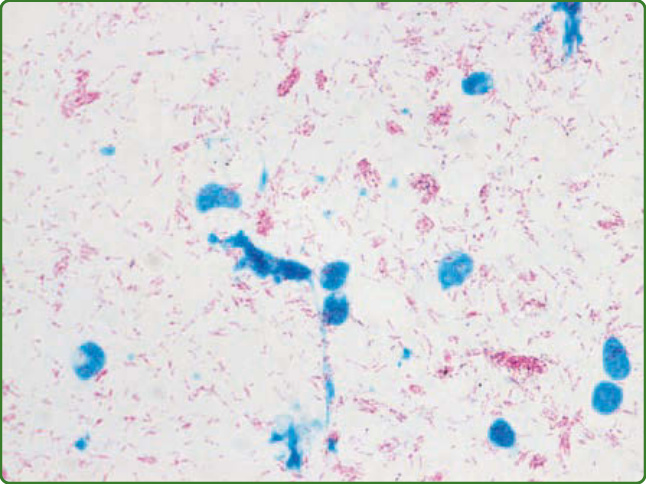
Figure 159-22 Acid-fast bacilli of a slit-skin smear of a lepromatous leprosy patient. The cells are in blue and the bacteria are in red, forming globi.
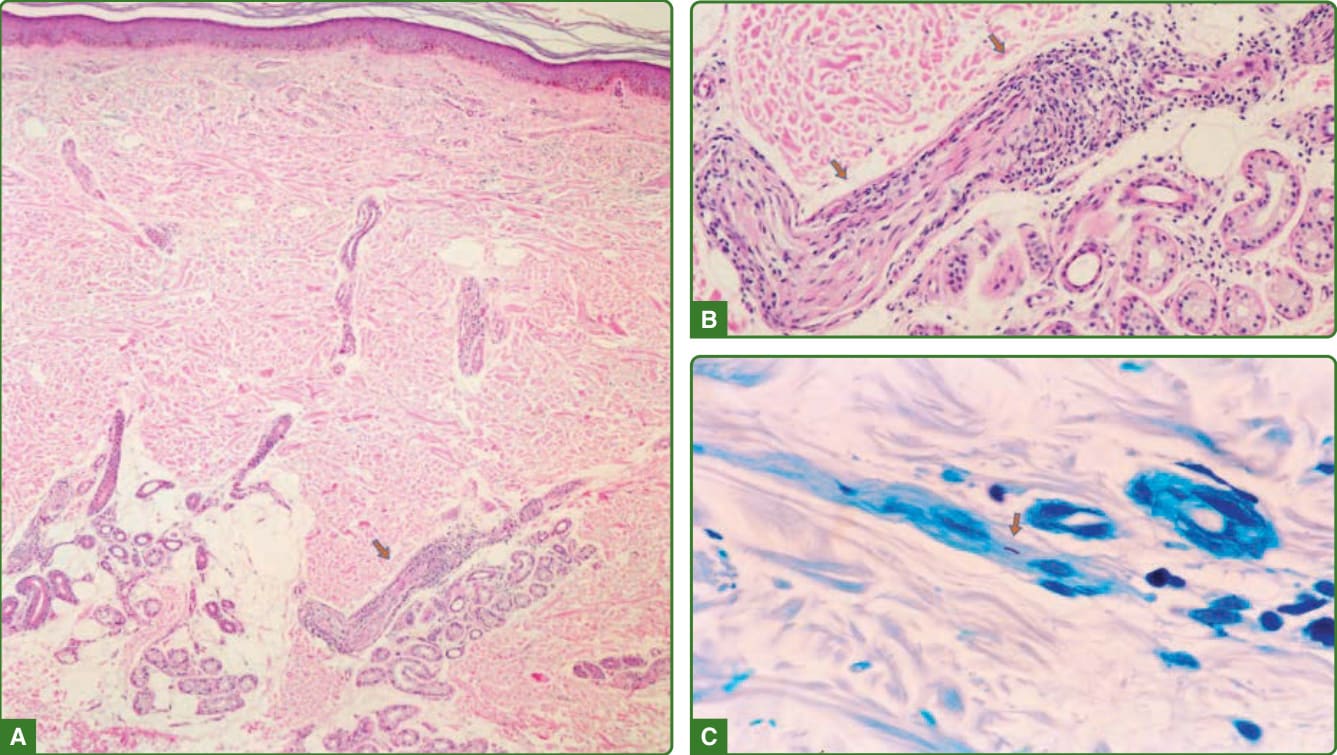
Figure 159-23 Indeterminate leprosy histopathology. Up to 70% of the indeterminate cases may have an unspecific histopathology. In 30% it is possible to observe a perineural infiltrate with nerve delamination (A and B, arrows), as demonstrated here, and if extensively searched, sometimes it is possible to find an acid-fast bacilli (C, arrow). (Used with permission from Dr. Jaison Barreto, Lauro de Souza Lima Institute, Brazil.)
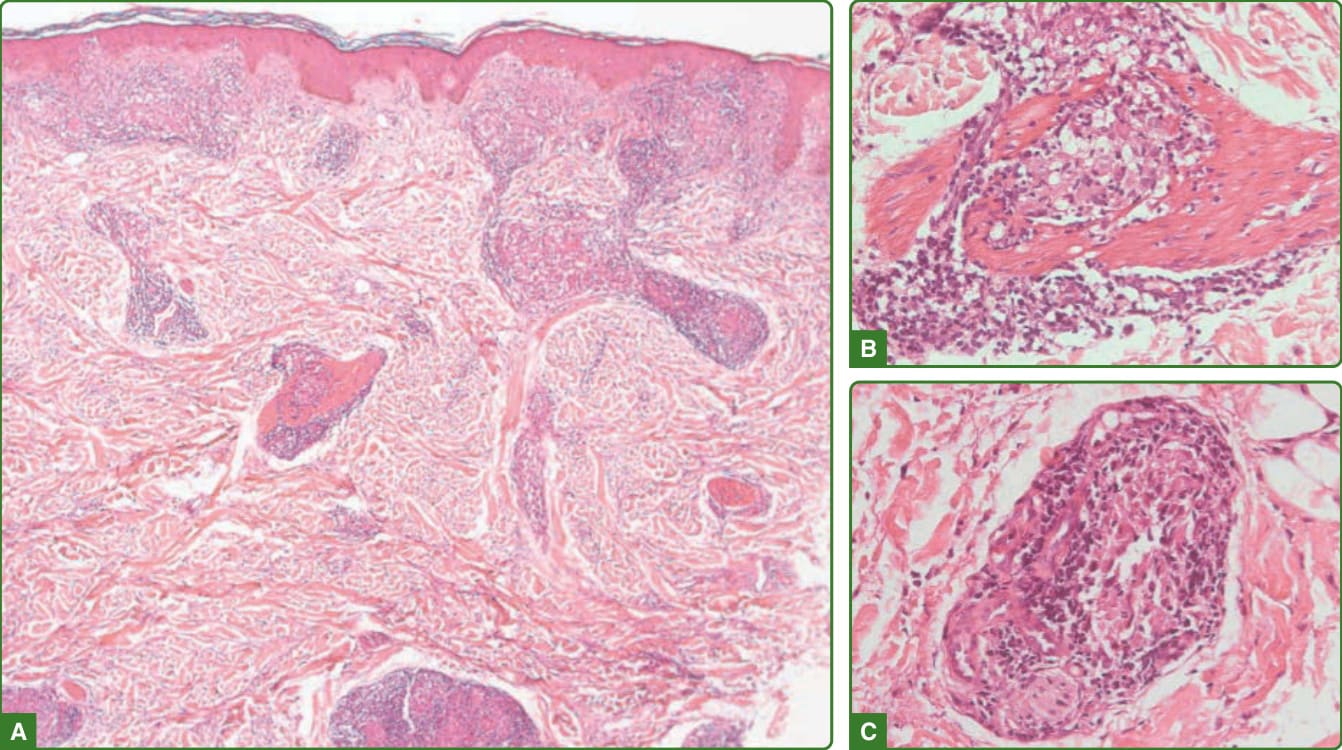
Figure 159-24 Tuberculoid leprosy histopathology. Presence of deep and superficial well-developed granuloma, that touch the epidermis (A), associated with lymphocyte infiltration surrounding or invading and destroying skin appendages, like nerves, erector pili muscle (B), or sweat gland (C).
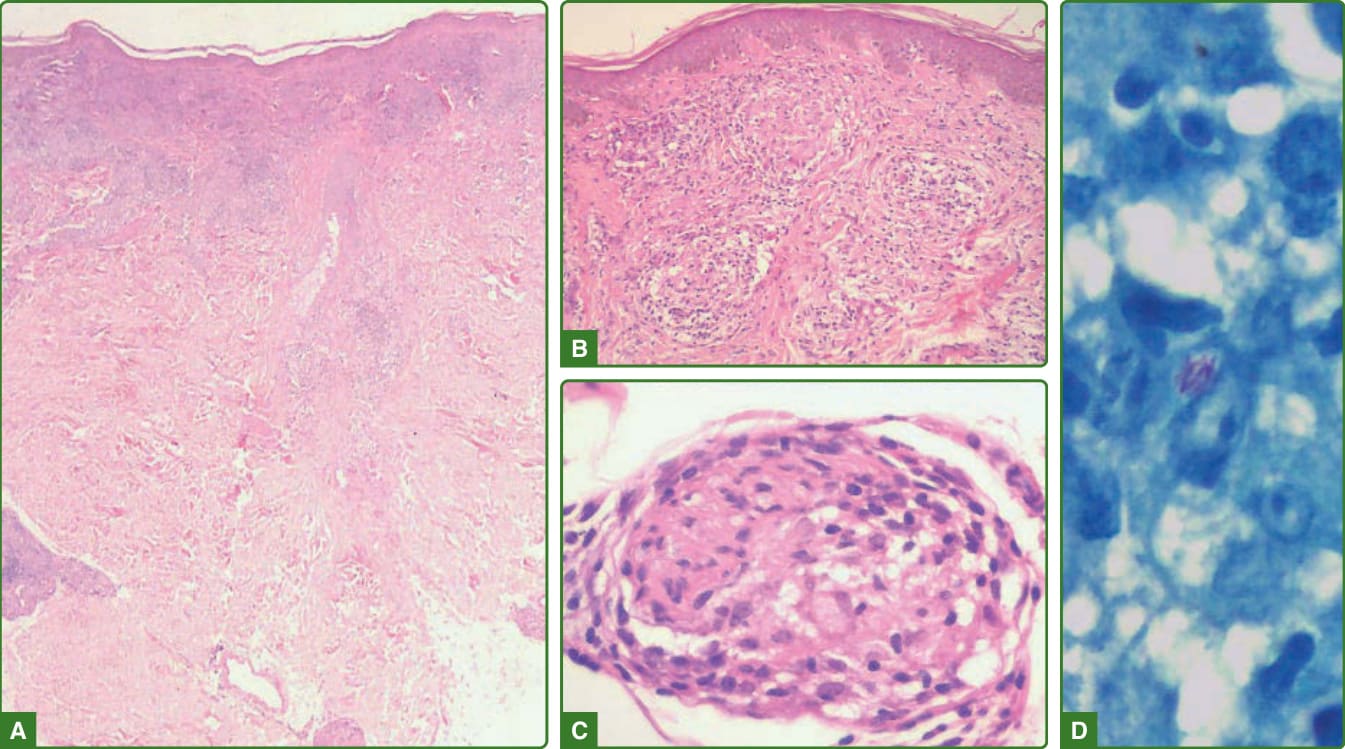
Figure 159-25 Borderline-tuberculoid leprosy histopathology. Deep and superficial tuberculoid granuloma (A) that does not touch the epidermis (B). The tuberculoid granuloma may be seen invading the nerves (C), and acid-fast bacilli can be found (D, 100×). (Used with permission from Dr. Jaison Barreto, Lauro de Souza Lima Institute, Brazil.)
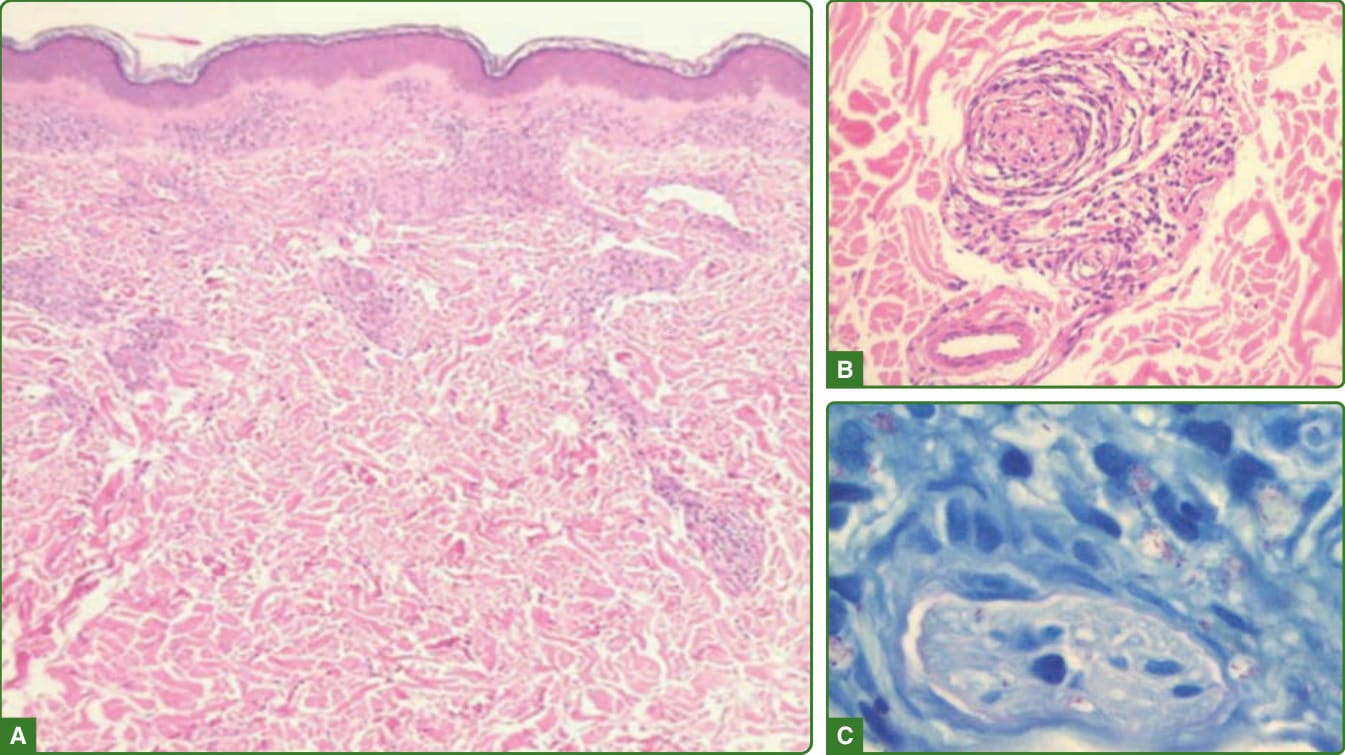
Figure 159-26 Borderline-borderline leprosy histopathology. Deep and superficial tuberculoid granuloma that does not touch the epidermis, starting to form a grenz zone (A). Inflammatory cells are invading cutaneous annexes and nerves, that are degenerated (B), and acid-fast bacilli can be found more easily, some forming globi (C). (Used with permission from Dr. Cleverson Soares, Lauro de Souza Lima Institute, Brazil.)
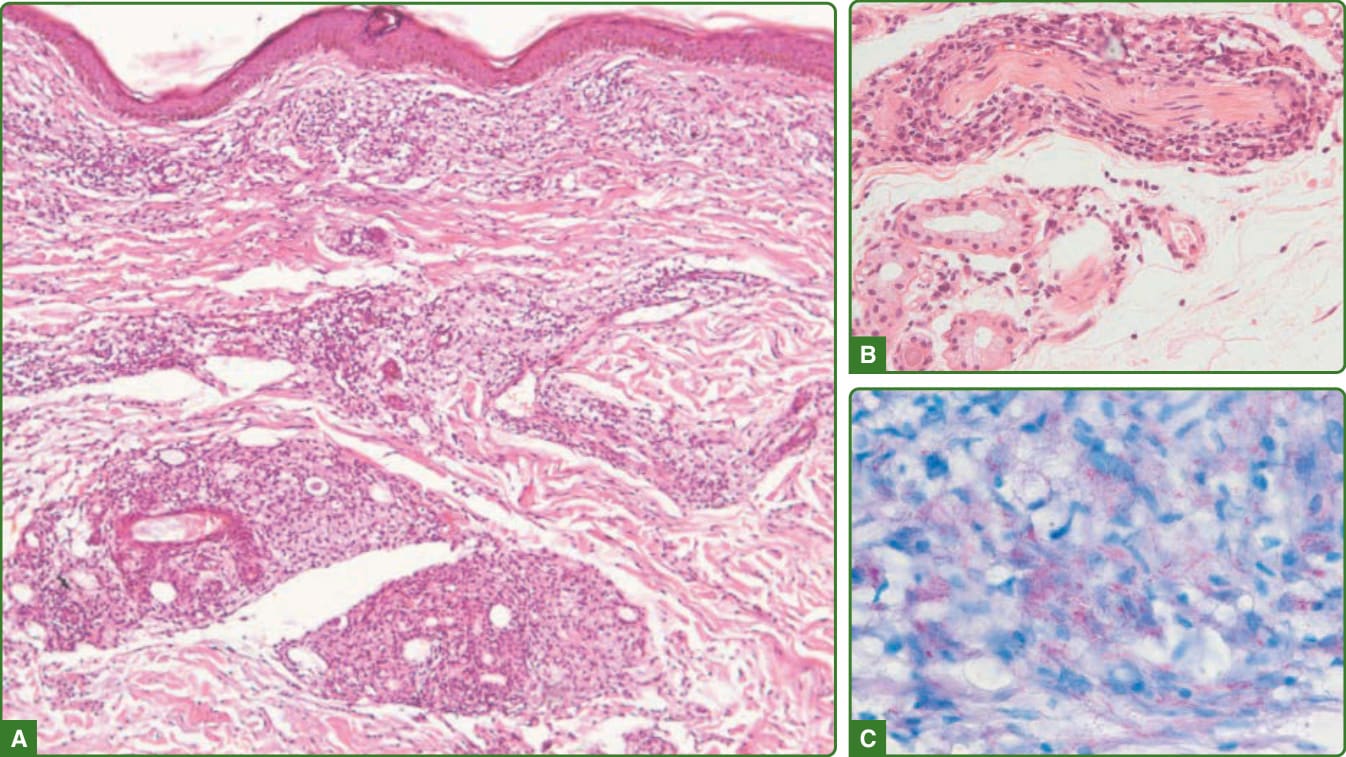
Figure 159-27 Borderline-lepromatous leprosy histopathology. There is a mixed macrophage lymphocytic inflammatory infiltrate (macrophage granuloma) on superficial and deep dermis (A). The mixed infiltrate does not touch the epidermis and may be seen surrounding or invading nerve bundles (B). A large number of acid-fast bacilli is seen (C).
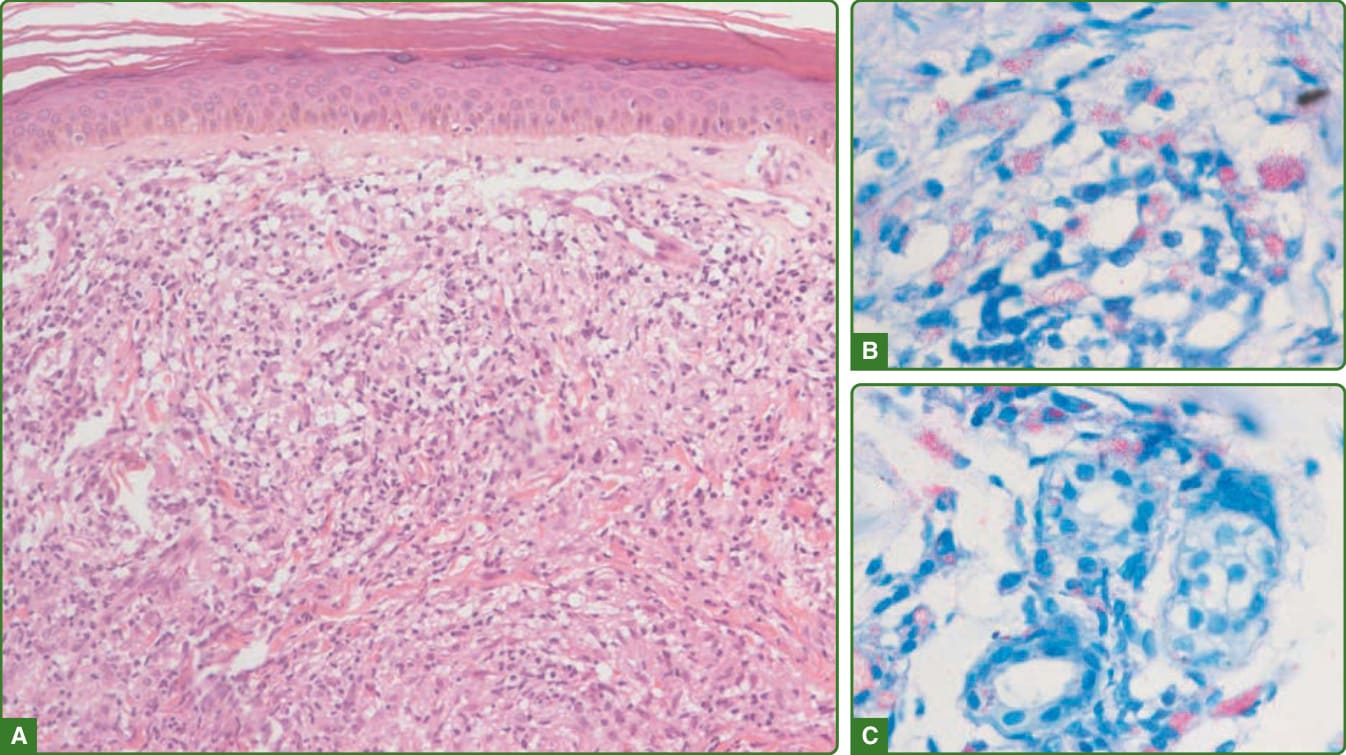
Figure 159-28 Lepromatous leprosy histopathology. An inflammatory infiltrate composed mostly by foamy macrophages is observed on the dermis. The epidermis is flattened, and there is a clear grenz zone on the dermal–epidermal interface (A). Fite-Faraco demonstrate acid-fast bacilli globi inside macrophages (B) and on sweat glands cells (C).
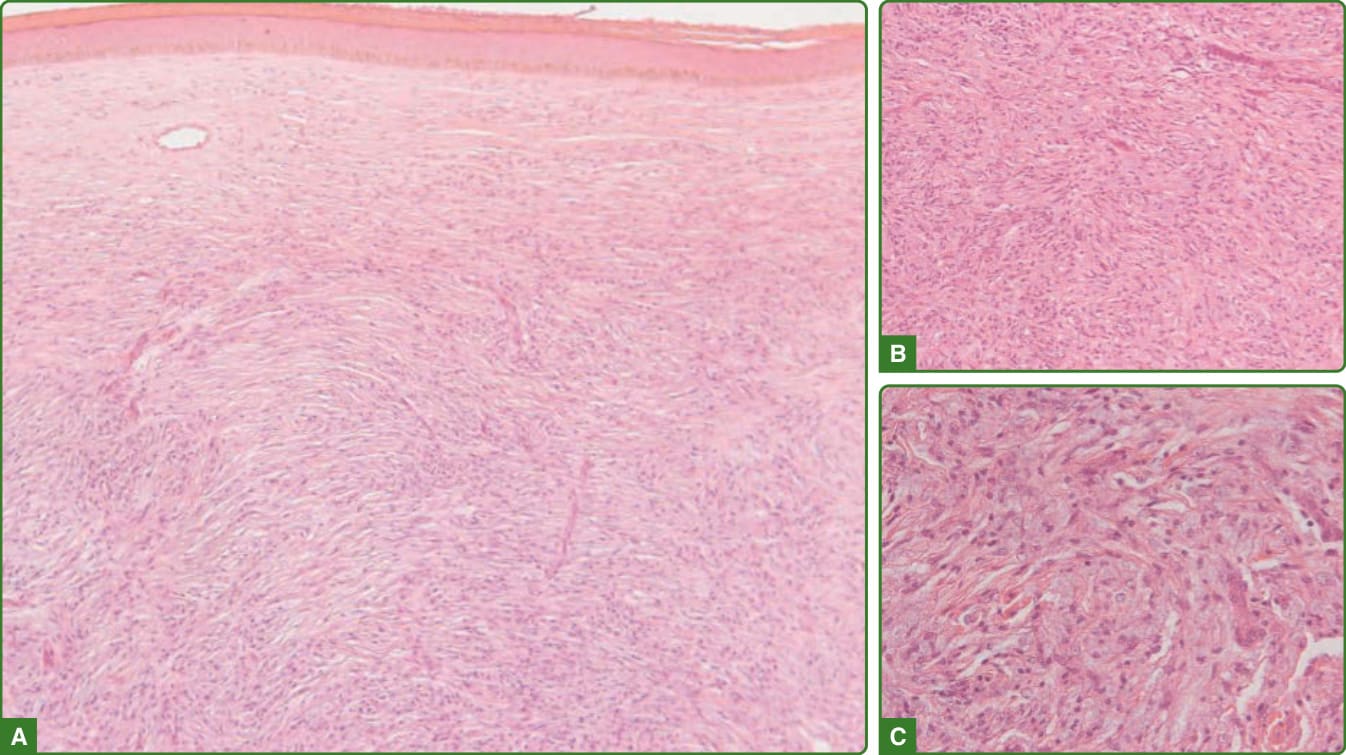
Figure 159-29 Lepromatous leprosy histoid Wade leprosy histopathology. A flattened epidermis is observed over a dense inflammatory infiltrate (A) of spindle and epithelioid cells arranged in a storiform or fasciculated pattern (B), which may have a foamy aspect on closer view (C).
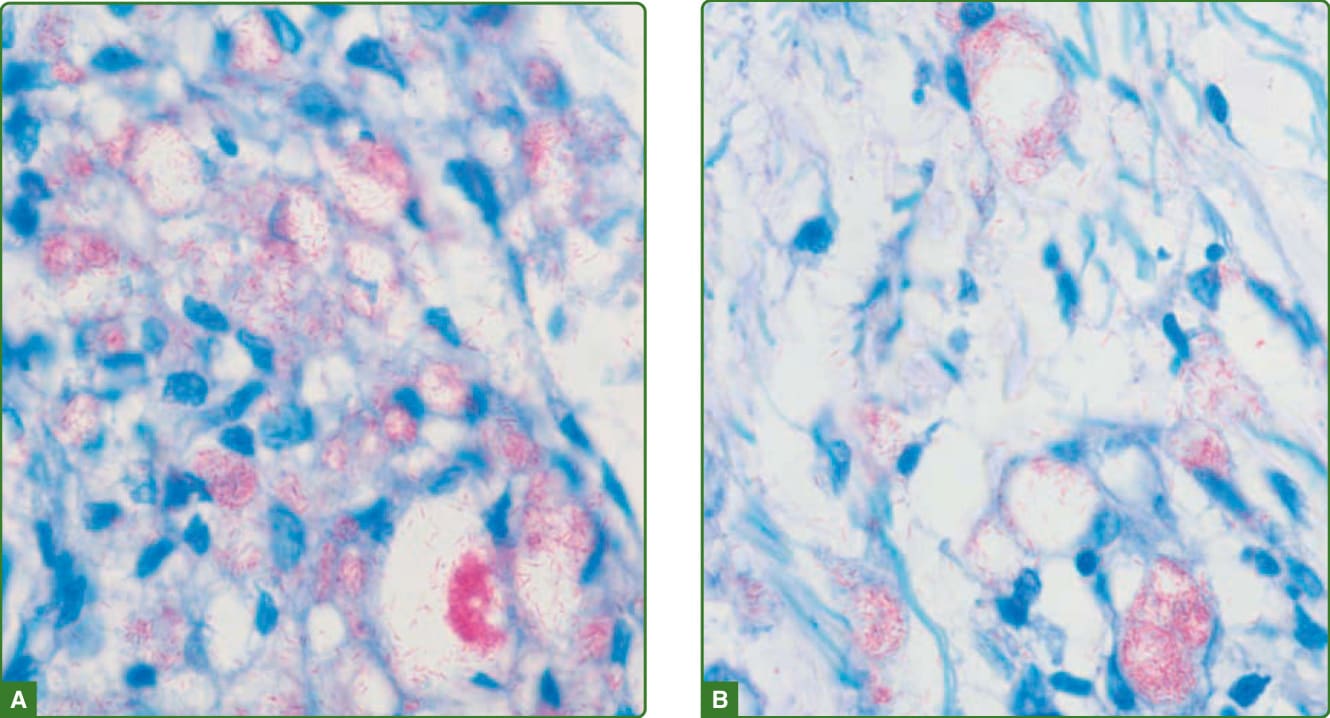
Figure 159-30 Globi. Aggregates of bacilli (globi) inside the host cells, as seen here inside macrophages (A and B), is a characteristic of M. leprae.
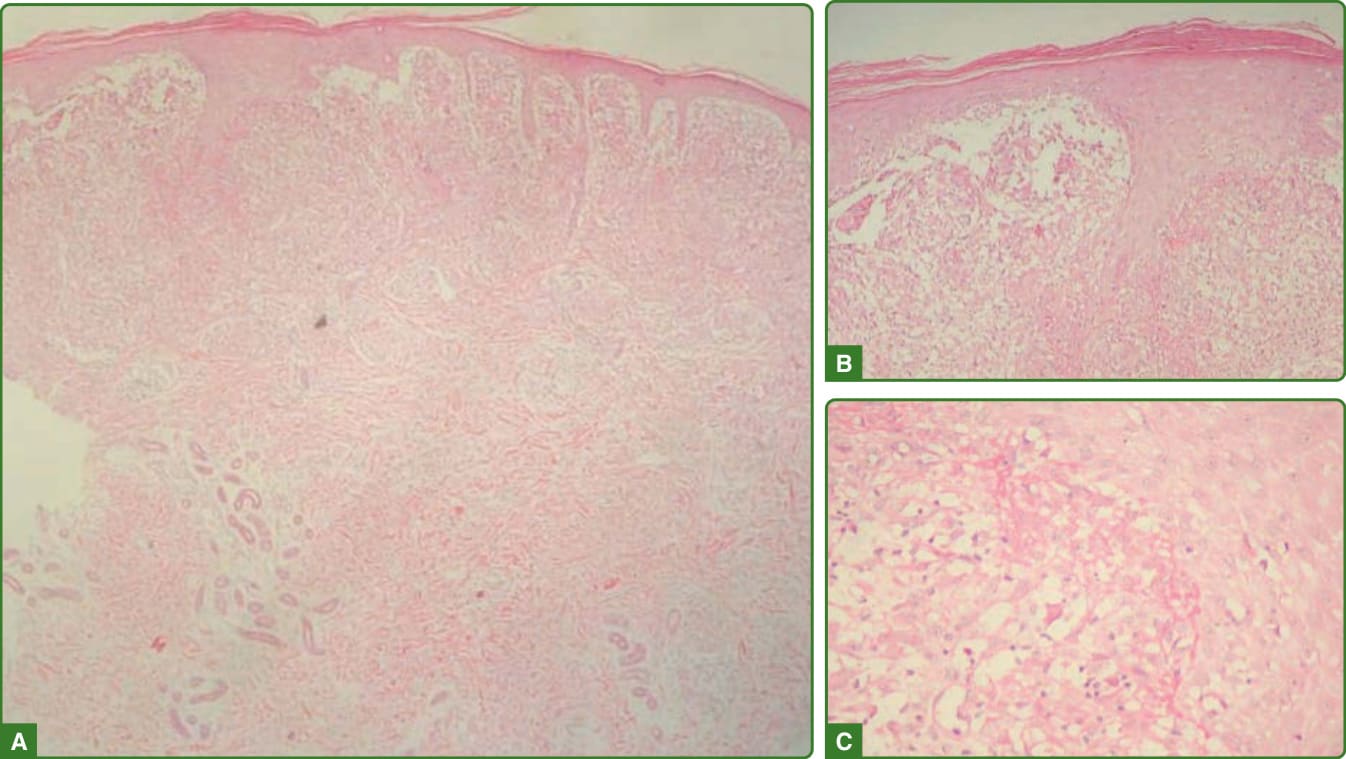
Figure 159-31 Histopathology reversal reaction. Presence of an inflammatory infiltrate, associated to epithelial hyperplasia (A) and foci of epidermal aggression with dermal edema (B) and fibrin deposit (C). (Used with permission from Dr. Jaison Barreto, Lauro de Souza Lima Institute, Brazil.)
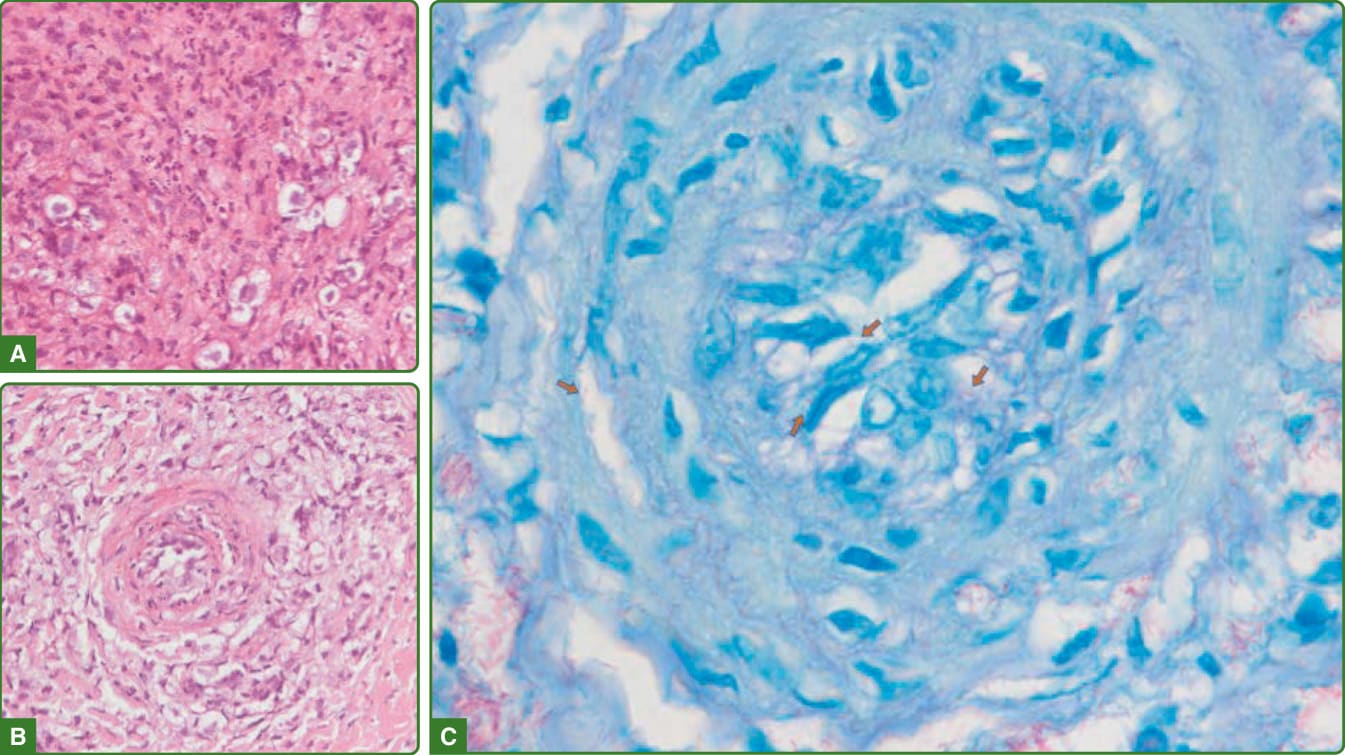
Figure 159-32 Histopathology erythema nodosum leprosum. A mixed inflammatory infiltrate, composed of foamy macrophages with large vacuoles and neutrophils (A) is shown. Foamy macrophages are also seen surrounding a vessel undergoing fibrinoid necrosis and presenting aggregates of inflammatory cells in its lumen and wall (B), where Fite-Faraco reveals the presence of large amounts of globi, and single bacilli inside a vessel and in its wall (C, arrows).
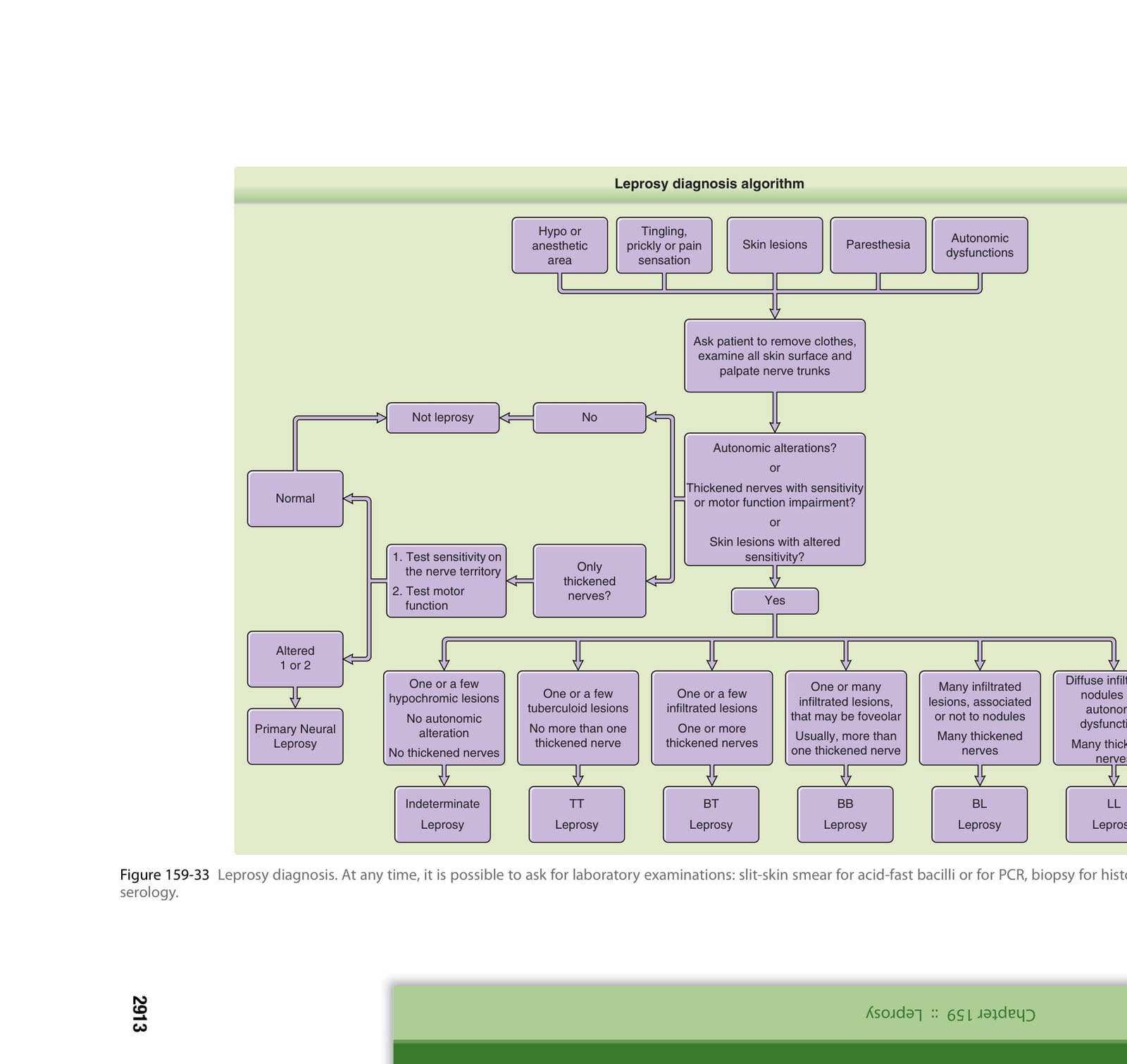
圖 159-33
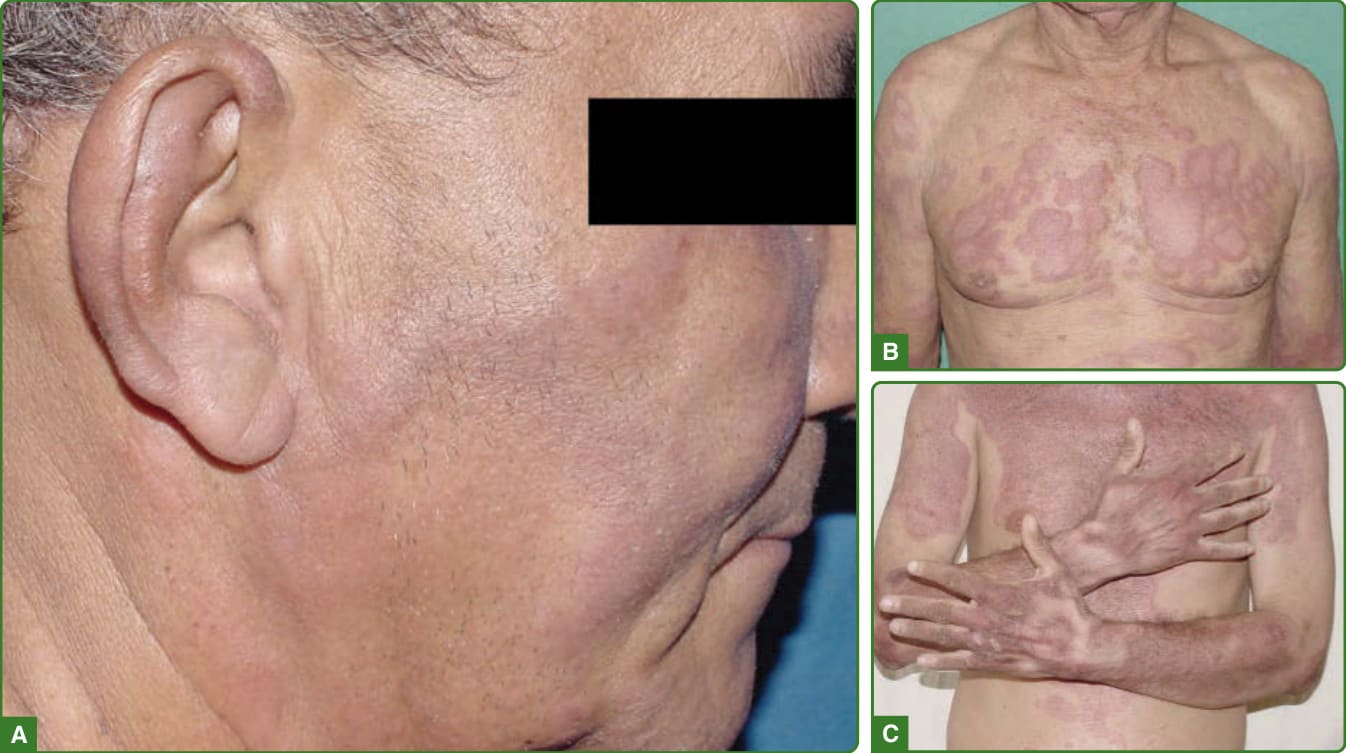
Figure 159-34 Reversal reaction. Reappearance or worsening of pre-multidrug therapy lesions, during or after treatment (A), usually presenting severe infiltrated lesions, that may coalesce in small, foveolar (B) or large scaly (C) plaques.

Figure 159-35 Erythema nodosum leprosum. Presence of fever and malaise with painful subcutaneous nodules that are easy to palpate, but much less apparent then reversal reactions lesions.

Figure 159-36 Lucio phenomenon. Small and large ulcers with infiltration in lepromatous leprosy patients. Slit-skin smear of those patients is loaded heavily with acid-fast bacilli.
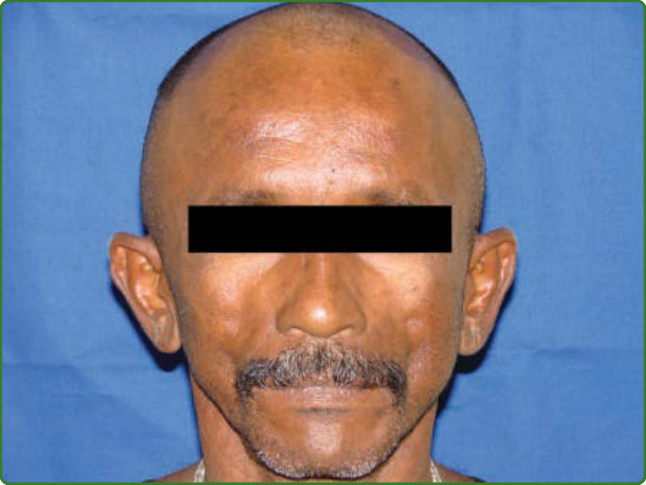
Figure 159-37. Clofazimine pigmentation. Brownish color and dry skin in a patient on multibacillary multidrug therapy.
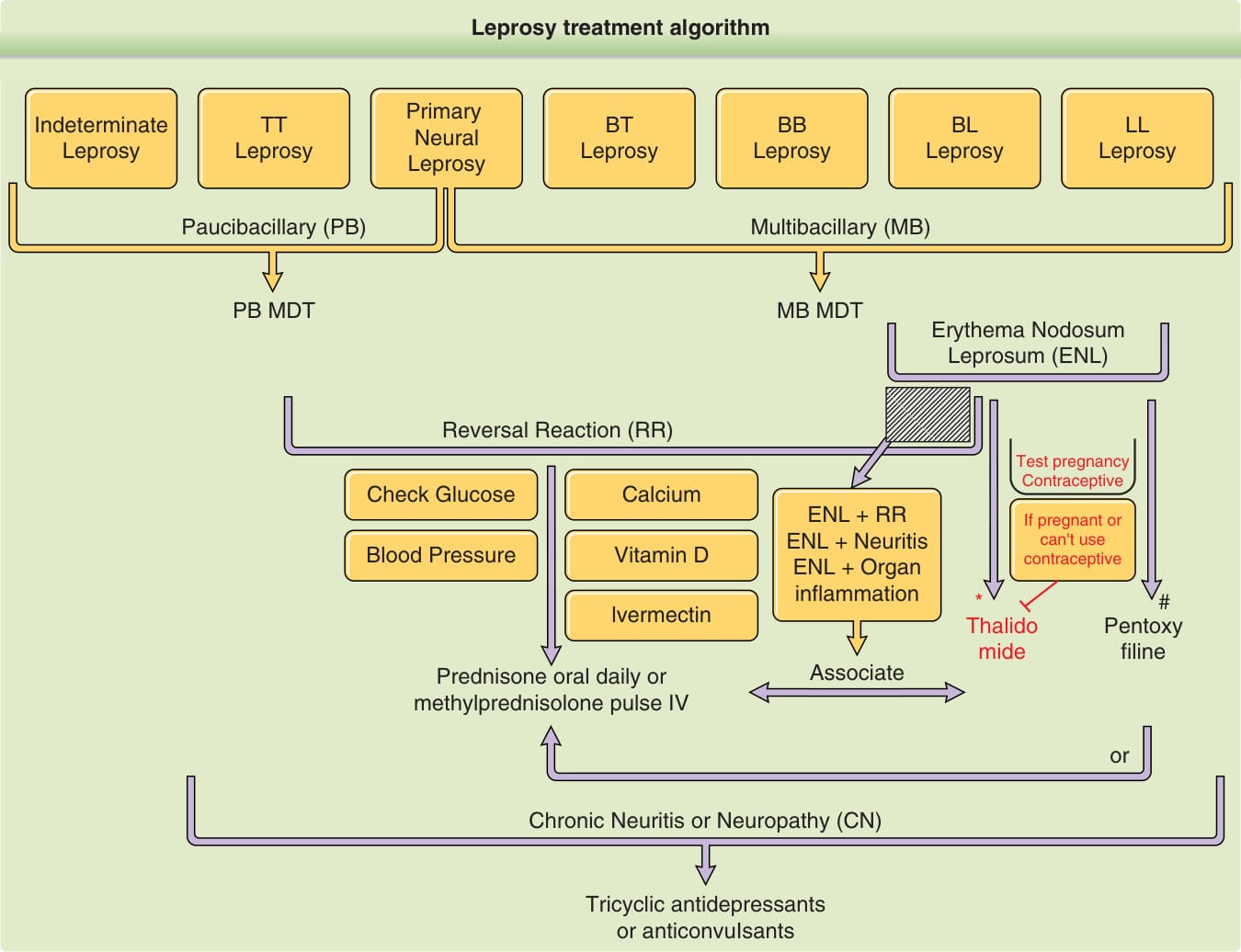
*Figure 159-38 Leprosy treatment. Multidrug therapy is the choice for leprosy treatment. However, when there is intolerance to any of the drugs, available alternatives may be used, as ofloxacin, minocycline, or clarithromycin. Also, if there is no answer to multidrug therapy, drug resistance may be tested, and the same alternative drugs used in place of 1 or more multidrug therapy drugs. For reactions, thalidomide is not available in all countries, and may even be prohibited. It is not permitted to prescribe thalidomide to pregnant women or to women of childbearing age. If it is necessary to use it, some countries have strict rules or laws that may require a pregnancy test and the use of contraceptives to prescribe thalidomide. pentoxyfiline is a “category C” drug for pregnancy and, therefore, it should be used only if the potential benefits justify the potential risk to the fetus.

Figure 159-39 Contact examination is mandatory on leprosy programs. Note the macular hypochromic anesthetic lesion on a child that the father was diagnosed with lepromatous leprosy.
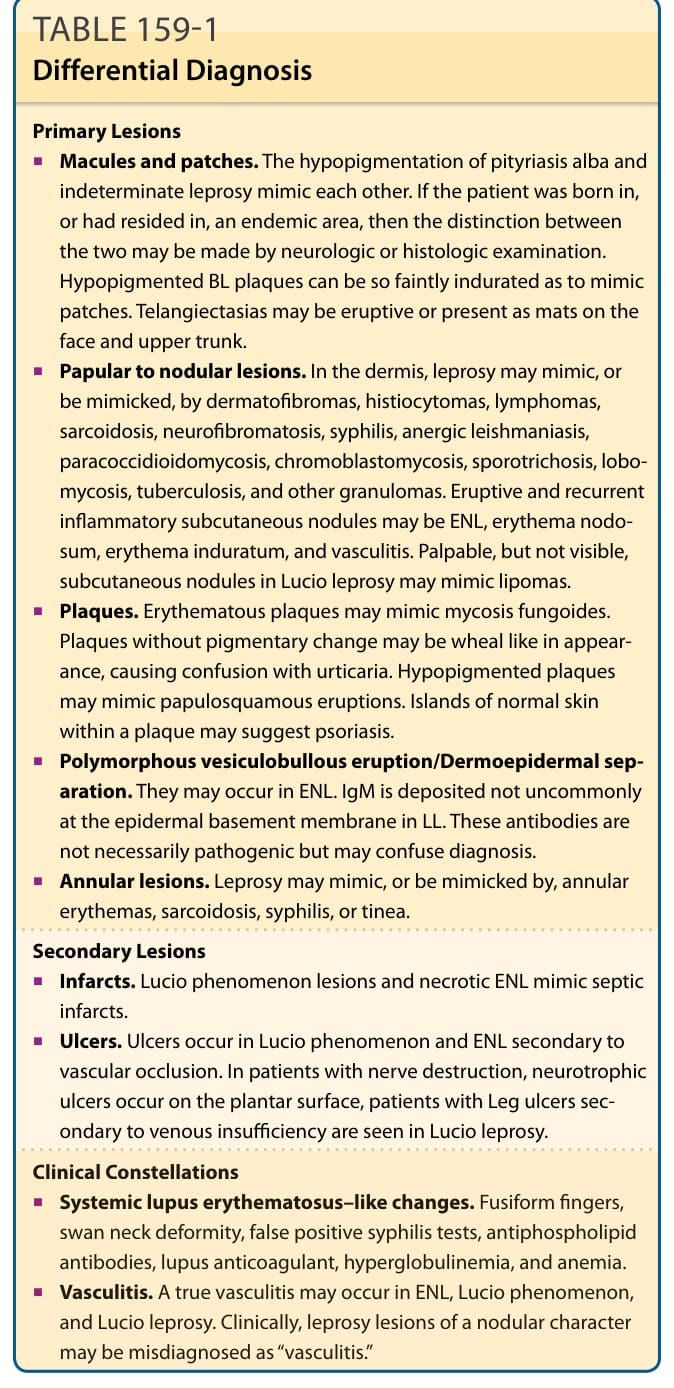
TABLE 159-1 Differential Diagnosis
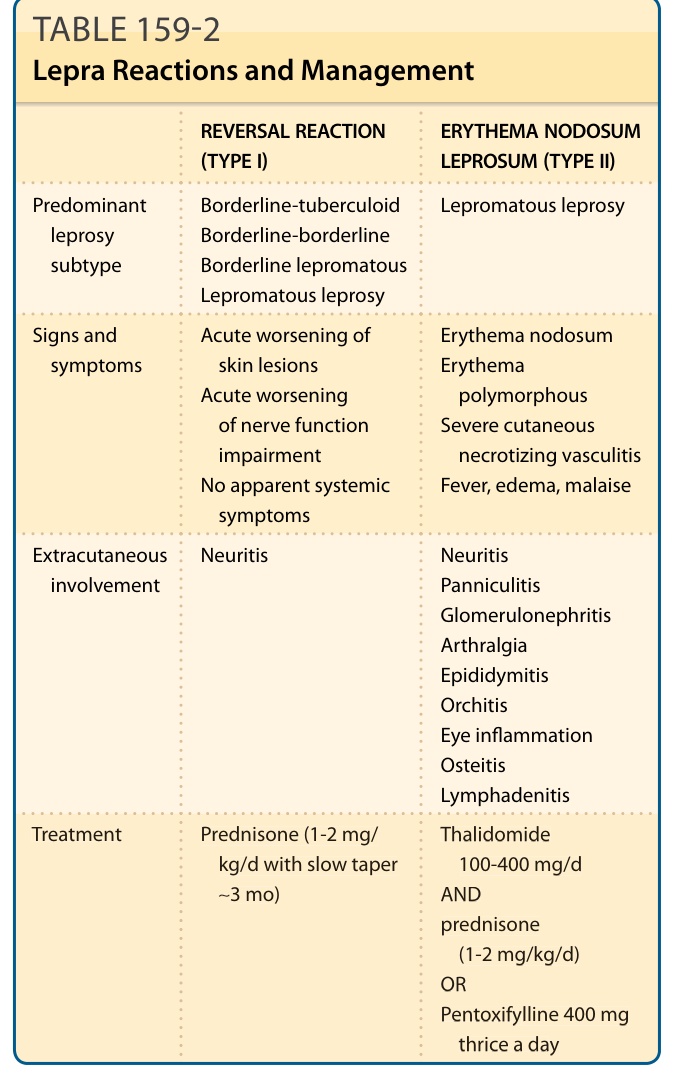
TABLE 159-2 Lepra Reactions and Management
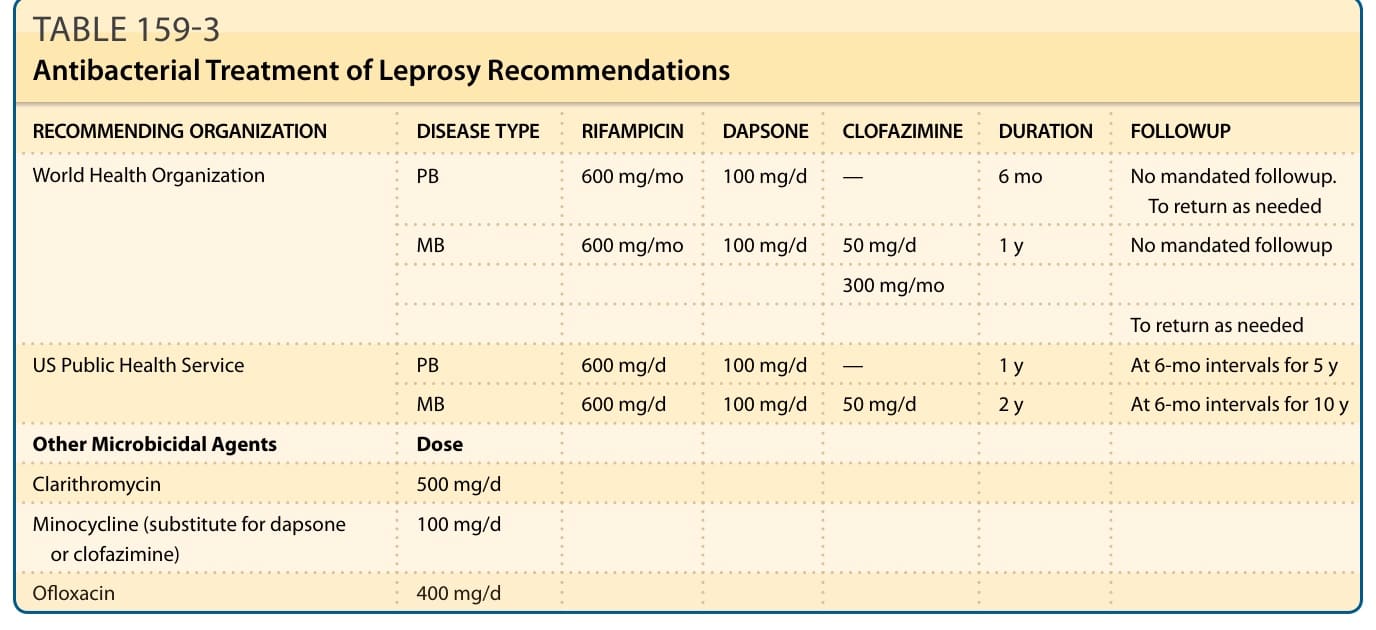
TABLE 159-3 Antibacterial Treatment of Leprosy Recommendations