Cellulitis and Erysipelas
23
AT-A-GLANCE
■ Common infection of the deep dermis and subcutaneous tissue most often caused by streptococcal and staphylococcal species, resulting in erythema, swelling, warmth, and pain of the affected site.
■ Unilateral lower-extremity involvement is typical and systemic symptoms are usually absent.
■ Important local risk factors include compromise of the skin barrier or underlying lymphovascular system.
■ Diagnosis is most often made clinically because of frequently equivocal or negative workups.
■ Treatment consists of antibiotics, but multiple recurrences may be observed.
■ Common variants:
■ Erysipelas: sharply demarcated, bright red, edematous plaques resulting from superficial lymphatic infiltration.
■ Purulent cellulitis: localized pustules or abscesses associated with cellulitis.
Cellulitis is a common infection of the deep dermis and subcutaneous tissue, most often caused by bacteria, that presents with the classic signs of inflammation as described by the Roman scholar Celsus in the first century ce: redness (rubor), swelling (tumor), heat (calor), and pain (dolor). Erysipelas is a variant of cellulitis that predominantly affects the superficial lymphatic vessels and surrounding tissue. Unlike the ill-defined plaques characterizing classic cellulitis, erysipelas demonstrates sharply marginated edematous plaques and is strikingly red in color. Diagnosis may be challenging and relies predominantly on clinical findings as laboratory, serologic, microbiologic, histopathologic, and imaging studies are often equivocal or negative. For these reasons, despite the high prevalence of these infections, misdiagnosis is common and may lead to both treatment-related morbidity and significant health care costs.
DEFINITIONS
Most modern studies group classic cellulitis and erysipelas together under the simple term cellulitis when evaluating pathogenesis, risk factors, diagnosis, and treatment; this chapter follows that convention. Other cutaneous bacterial infections, including pyodermas (Chap. 150), toxin-mediated infections (Chap. 152), and necrotizing soft-tissue infections (Chap. 153) are considered separately.
HISTORICAL PERSPECTIVE
Skin and soft-tissue infections have been described for thousands of years.1 In the preantibiotic era, cellulitis had a mortality rate of approximately 11% and only two-thirds of patients treated were cured with treatment.2 Early therapies in the antibiotic era, including ultraviolet light, penicillin, and sulfonamide, significantly reduced mortality, although study designs were comparatively simpler than modern clinical trials.2 In recent years, the emergence of community-acquired methicillin-resistant Staphylococcus aureus (MRSA), an increasingly common cause of cellulitis, has affected the epidemiology and treatment of this infection.
EPIDEMIOLOGY
Cellulitis is common and has increased in prevalence: in 1997 there were 4.6 million ambulatory visits for cellulitis or abscess in the United States, and this increased to 9.6 million in 2005.3 The incidence rate increased from 17.3 to 32.5 per 1000 population during this time period, which parallels the rise of communityacquired MRSA.3,4 In the United States, rates appear to have stabilized, although they continue to rise in other economically developed nations.5,6 More than 10% of hospitalizations for infectious diseases in the Unites States are because of cellulitis, and hospitalizations for cellulitis in the United States have increased from approximately 300,000 in 1999 to more than 530,000 in 2013, with an estimated cost of $3.7 billion.7,8
Recurrent cellulitis represents 22% to 49% of patients, but its specific epidemiology is not well characterized.9,10 Each reoccurrence increases the risk of subsequent episodes, because of local and systemic risk factors (see section “Risk Factors”).11,12 Most patients with recurrent cellulitis can be managed in the ambulatory setting and only a minority require hospitalization.10
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
Classic cellulitis presents acutely with spreading, illdefined erythema and edema, and is often warm and painful. The lower extremity is the most common site in adults, but the upper extremities, trunk, and head and neck may be involved (Fig. 151-1). Children are more likely than adults to have facial involvement. It is unilateral in the vast majority of cases, and bilateral involvement should prompt consideration of an alternative diagnosis, except in rare circumstances.13 Linear
streaking, lymphangiitis, and tender regional lymphadenopathy may be observed, as well as small areas of spared intervening skin, so-called “skip areas.” When there is significant involvement of the lymphatics or superficial edema, the skin may acquire a peau d’orange appearance. Bulla formation and superficial necrosis can result in epidermal sloughing or erosions (Fig. 151-2). Hemorrhage may be observed as the result of disruption of superficial vessels by inflammation and edema. The presence of crepitus, anesthesia,
A
B
23
or pain disproportionate to clinical findings should raise concern for a necrotizing soft-tissue infection (see Chap. 153).
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
Fever is an inconsistent complication of cellulitis and may be present in 12% to 71% of hospitalized patients; it may be even less common in patients who require only outpatient management.13,14 Tachycardia may be observed.13 Hemodynamic instability should prompt assessment for complicating sepsis, toxin-mediated systemic illness, or other serious infection.
COMPLICATIONS
COMPLICATIONS
Lymphatic damage leading to lymphedema is a frequent complication of cellulitis that increases the risk of recurrence (Fig. 151-3).9,11,12 Superficial thrombophlebitis may be seen in the acute setting, but the risk of deep venous thrombosis is low.15 More serious complications in treated patients are uncommon, but may include bacteremia, which occurs in approximately 5% of patients, and its sequelae, including sepsis, bacterial endocarditis, postinfectious glomerulonephritis, and toxin-mediated systemic syndromes (see Chaps. 152 and 155).16,17 Spread of infection to deeper tissues is rare in the absence of other risk factors or chronic systemic disease.
CLINICAL VARIANTS
CLINICAL VARIANTS
Erysipelas shares many clinical features with classic cellulitis, but the area of involvement is sharply demarcated and bright red in color. The most common site
2747
23
of involvement is the leg in 76% to 90% of cases, followed by the face and upper extremity (Figs. 151-4 and 151-5).18,19 Fever is more common than in classic cellulitis.18 Recurrence may be observed but systemic complications are uncommon. Purulent cellulitis is defined by the presence of pustules or abscess development, which may precede or
2748
follow cellulitis (Fig. 151-6A). There should be a higher suspicion for Staphylococcus aureus as the causative organism.20 If purulent collections are identified by physical examination or ultrasonography, there should be strong consideration for incision and drainage in addition to culture-directed and sensitivity-directed antibiotics (see also Chap. 150). Surgical site infections localize to the site of surgery and are often accompanied by purulence (see Fig. 151-6B). S. aureus is commonly cultured, but other organisms may predominate depending upon the anatomic location and type of surgery. Bite wounds may give rise to cellulitis at the site of inoculation in 20% to 30% of cases (see Chap. 182).21
Dog bites are usually associated with crush injuries, whereas cat bites, because of the sharper teeth of cats, inject organisms into deeper tissue spaces, including joint spaces, tendon sheaths, and bone. Human bites are often polymicrobial and can result from direct biting or indirectly from contact of a fist to another person’s teeth (“fight bite”). Periorbital or preseptal cellulitis is an infection anterior to the orbital septum, and demonstrates erythema, swelling, warmth, and pain in a periorbital distribution. Like classic cellulitis, there may be a clear portal of entry for infection. Patients may or may not have systemic symptoms, and neurologic sequelae are absent.22
Orbital cellulitis, in contrast, is infection posterior to the septum with involvement of the orbit proper. It usually results from direct extension of sinusitis, and may manifest with similar cutaneous findings to periorbital cellulitis.22 Proptosis, bulbar conjunctival edema, ophthalmoplegia, and decreased visual acuity are important clues to diagnosis, and necessitate rapid evaluation and treatment.22 Orbital cellulitis may be complicated by permanent vision loss or posterior spread of infection into the brain. Bilateral cellulitis, where infection occurs simultaneously on both extremities, is rare in the absence of predisposing factors such as penetrating trauma. Most of these patients are misdiagnosed (see section “Differential Diagnosis”); however, patients with deficient cellular immunity, such as solid organ transplantation recipients or individuals with HIV, may be at greater risk of true bilateral infection. In this patient population atypical causes of cellulitis should be considered, including disseminated cryptococcosis.23,24
ETIOLOGY AND PATHOGENESIS
Microbial pathogens gain access to the deep dermal and subcutaneous tissues through breaks in the skin, where they can spread into lymphatics, blood vessels, and interstitial spaces. A portal of entry can be identified in up to 62% of patients, with toe web infections as the most common etiology.19 Disseminated infection with secondary seeding of the skin is a rare cause of cellulitis that may occur in immunocompromised patients.
23
B
A
Given the difficulty in culturing or identifying causative pathogens, cellulitis may be relatively paucimicrobial, with a significant portion of the clinical symptoms and signs due to host inflammatory responses to killed bacteria and bacterial exotoxins.
MICROBIOLOGY
MICROBIOLOGY
Group A β-hemolytic streptococci (Streptococcus pyogenes) and staphylococci (particularly S. aureus) are the most commonly identified pathogens, but the specific incidence is difficult to characterize as identification of the causative organism occurs in less than one-third of cases.16,19,25,26 Historically, erysipelas was attributed solely to streptococci, but recent studies have found a microbial profile that is similar to the microbial profile of classic cellulitis.16 Other streptococcal species (groups B, C, and G) and coagulase-negative
staphylococci are less-often encountered, but may be of increasing importance in hospitalized patients. Prior to widespread vaccination, which began in the late 1980s, Haemophilus influenzae Type B was observed in up to 6% of children with any systemic infection.27 Surgical site infections, pressure or diabetic ulcers, and those with cellular immunodeficiency may be at greater risk for polymicrobial or atypical infections, including enterococci, Pseudomonas spp., Gram-negative anaerobes, mycobacteria, and disseminated fungal infections such as cryptococcosis. Cellulitis resulting from bite wounds may be polymicrobial and include Gramnegative anaerobes such as Pasteurella spp., Eikenella spp., and Capnocytophaga canimorsus (see Chap. 182). Aquatic trauma may lead to cellulitis from atypical organisms including Aeromonas spp., Erysipelothrix rhusiopathiae, Mycobacterium marinum or other atypical mycobacteria, and Vibrio vulnificus.28
TYPE OF INFECTION MOST COMMON CAUSE (S) SELECT UNCOMMON CAUSES
Cellulitis and erysipelas (including periorbital/orbital cellulitis)
Group A streptococci (Streptococcus pyogenes); Staphylococcus aureus Groups B, C, or G streptococci; coagulase-negative staphylococci; Streptococcus iniae; Streptococcus pneumoniae; Haemophilus influenzae (children); Escherichia coli, Proteus spp., other Enterobacteriaceae, and other Gram-negative anaerobes; Neisseria spp.; Moraxella spp.; Campylobacter jejuni; Cryptococcus spp. and other disseminated fungal organisms (immunocompromised); Legionella pneumophila, Legionella micdadei; Pseudomonas aeruginosa (secondary to bacteremia)
Cellulitis from animal and human bites (see Chap. 182) Pasteurella spp.; streptococci, staphylococci Bacteroides spp.; Bartonella henselae (cat); Capnocytophaga canimorsus (dog); Eikenella spp. (human); Fusobacterium spp.; Moraxella spp.
Aeromonas spp.; Erysipelothrix
Cellulitis from aquatic trauma
Cellulitis from aquatic trauma (exposure-specific) Aeromonas spp.; Erysipelothrix rhusiopathiae; Mycobacterium marinum and other atypical mycobacteria; Vibrio vulnificus
rhusiopathiae; Mycobacterium marinum and other atypical mycobacteria; Vibrio vulnificus
(exposure-specific)
2749
23
Systemic/Environmental
Systemic/Environmental
Local
Local
■Age
■Disrupted skin barrier (toe web infections such as tinea pedis, inflammatory dermatoses, penetrating trauma, including iatrogenic causes)
■Age
■Disrupted skin barrier (toe
■Obesity
■Obesity
web infections such as tinea pedis, inflammatory dermatoses, penetrating trauma, including iatrogenic causes)
■Systemic disease: renal, hepatic, or autoimmune connective tissue diseases, malignancy; immunosuppressiona (including diabetes, HIV, and iatrogenic)
■Systemic disease: renal,
hepatic, or autoimmune connective tissue diseases, malignancy; immunosuppressiona
■Compromised lymphovascular system (edema/lymphedema, venous insufficiency, peripheral arterial disease)
■Compromised lymphovas-
(including diabetes, HIV, and iatrogenic)
cular system (edema/lymphedema, venous insufficiency, peripheral arterial disease)
■Summer season
■Summer season
aControversial as a risk factor for routine cellulitis. Immunosuppression should prompt consideration of unusual presentations or atypical pathogens and may require more aggressive treatment.
RISK FACTORS
RISK FACTORS
Cellulitis is more common in men than women, and its incidence rises during summer months and markedly with increasing patient age.6,8 Other systemic or epidemiologic risk factors include obesity, renal or hepatic disease, connective tissue disease, and malignancy, but immunodeficiency (including iatrogenic or from systemic conditions such as HIV or diabetes) as a predisposing factor for routine cellulitis is controversial.6,29-31
Compromise of the skin barrier or underlying lymphovascular system are important local risk factors, and may result from lymphedema, toe web infection, inflammatory dermatoses, peripheral vascular disease, or iatrogenic causes, including IV line placement, surgical site intervention (which may disrupt both the skin barrier and underlying lymphovascular system), and postradiation changes.6,29,31 Of these, lymphedema confers the highest risk at more than 70-fold, followed by disruption of the skin barrier at nearly 24-fold.31
Recurrent cellulitis has similar risk factors to primary infection. Lymphedema, age, obesity, and prior surgical site intervention are among the most important.32 Like primary cellulitis, recurrent infection is frequently misdiagnosed (see section “Diagnosis” and “Differential Diagnosis”).
DIAGNOSIS
The diagnosis of cellulitis is most often made by clinical history and physical examination as there are no reliably accurate diagnostic studies. The cardinal symptoms and signs of erythema, swelling, warmth, and pain, even when accompanied by fever, leukocytosis, or elevated inflammatory markers, may be observed in clinical mimics of cellulitis known collectively as pseudocellulitis (see section “Differential Diagnosis”).29
2750
Misdiagnosis rates of greater than 30% have been
observed in acute care settings (emergency department or hospital) and lead to hundreds of millions of dollars in avoidable health care spending.33-36 Consultation of a dermatologist improves diagnostic accuracy, shortens duration of unnecessary antibiotic use, and improves short-term clinical outcomes.35,37 Despite its high prevalence, there is clear need for improved diagnostic testing for cellulitis.
SUPPORTIVE STUDIES
SUPPORTIVE STUDIES
LABORATORY TESTING
Leukocytosis (≥10,000 cells/µL) is present in 34% to 50% of patients, and inflammatory markers such as the erythrocyte sedimentation rate and C-reactive protein are elevated in more than 75% of patients, but these laboratory findings are nonspecific and also may be seen in pseudocellulitis.13,19,38 Procalcitonin has been reliably used in serious systemic bacterial infections, but its usefulness as a surrogate biomarker in localized cellulitis has not been consistent, and additional prospective studies are necessary.39-41
Serologic tests for cellulitis are controversial, as they may not reliably distinguish acute infection from prior exposure. Antistreptolysin O responses are more limited in cutaneous than upper respiratory tract infections, typically appear after 1 week, peak at 3 to 6 weeks, and decline at less-well-defined rates, thereby complicating the diagnosis of both primary and recurrent cellulitis.42 The anti-DNase B test peaks at 6 to 8 weeks, later than is useful for clinical decision making in the acute setting.42
MICROBIAL CULTURE
Skin swabs and surface wound cultures are often unhelpful, as they are commonly polymicrobial and determination of colonization versus true pathogenicity is challenging.14,29 Positive polymerase chain reaction swabs for MRSA carriage have correlated with an increased overall risk of cellulitis, but their usefulness in acute infection is debated.43 Needle aspiration followed by aspirate culture has shown widely disparate diagnostic usefulness, ranging from less than 5% to 40%, but may be more useful in patients with underlying systemic risk factors.14,44 Blood cultures are not routinely performed in uncomplicated cellulitis as they are positive in only approximately 5% of cases.16,17 However, in certain high-risk populations, such as the elderly, the immunocompromised, the systemically ill, and those with penetrating trauma, or if there is concern for atypical or severe systemic infection, blood cultures should be drawn. The 2014 update to the Infectious Diseases Society of America (IDSA) guidelines on the diagnosis and management of skin and soft-tissue infections does not recommend routinely culturing blood or cutaneous aspirates or swabs.26 In contrast, pustules, abscesses, or
other fluid collections associated with purulent cellulitis should be drained and cultured early during diagnostic workup.26,29
PATHOLOGY
Because the histopathologic findings of cellulitis are nonspecific, biopsy is not routinely performed. A sparse to moderately dense superficial and deep perivascular lymphocytic infiltrate with variable amounts of neutrophils may be seen, sometimes with background dermal edema, but Gram stains are frequently negative. Skin biopsy can be useful in evaluating for pseudocellulitis, depending upon the underlying etiology. Submission of skin biopsies for tissue culture is not routinely recommended, as the biopsies are positive in only 20% to 30% of cases.26 If there is concern for an atypical causative organism, including mycobacteria, fungi, or viruses, or in immunocompromised or other high-risk patient populations, a biopsy for histopathologic evaluation and tissue culture should be performed. Molecular techniques for microbe detection, including polymerase chain reaction of skin biopsies, do not reliably differentiate clinically involved from uninvolved skin and are often negative.26,39 Routine use has not been widely adopted.
IMAGING
For uncomplicated cellulitis, imaging studies are not diagnostic. Ultrasonography or MRI can be helpful in identifying localized fluid collections in purulent cellulitis for guidance of incision and drainage. MRI also may be used to identify involvement of deeper tissues, such as pyomyositis or osteomyelitis, rare complications of severe or longstanding cellulitis. CT or MRI can be useful in differentiating cellulitis from necrotizing soft-tissue infections.
EMERGING DIAGNOSTIC MODALITIES
Given the high rate of misdiagnosis and lack of accurate and reliable studies, there is interest in finding better diagnostic methods for cellulitis. The ALT-70 (Table 151-3), a risk prediction model generated to predict the likelihood of lower-extremity cellulitis among
Asymmetry (unilateral) 3 pointsa
Leukocytosis ≥10,000 cells/µL 1 point
Tachycardia ≥90 beats/min 1 point
70 years of age or older 2 points
70 years of age or older 2 points
aA score of 0 to 2 = ≥83.3% likelihood of pseudocellulitis; a score of ≥5 points = ≥82.2% likelihood of true cellulitis.
23
admitted patients, is based on asymmetry (unilaterality) of infection, leukocytosis equal to or greater than 10,000 cells/µL, tachycardia equal to or greater than 90 beats/min, and patient age equal to or greater than 70 years.13 A score of 0 to 2 points indicates a negative predictive value greater than 83.3%, and 5 points or higher indicates a positive predictive value greater than 82.2% for cellulitis.13 A skin surface temperature gradient greater than 0.47°C (0.85°F) between a patient’s involved and uninvolved skin, as determined by thermal imaging, has also shown promise, with a sensitivity of 96.6% for the diagnosis of cellulitis, but additional confirmatory studies are needed.45 Genetic testing may prove useful; a recent pilot study found that HLA-DQA1 expression was 34-fold higher among cases with cellulitis than controls.39
DIFFERENTIAL DIAGNOSIS
The differential diagnosis for cellulitis is broad, and includes causes of pseudocellulitis as well as causes of other infectious etiologies (Table 151-4). In difficult cases, skin biopsy or other laboratory markers may be useful for diagnosis when placed into the clinical context of the patient. The most common cause of pseudocellulitis is stasis dermatitis.29,30,46,47 Stasis dermatitis is commonly bilateral, which may aid in differentiating it from cellulitis; however, it is often asymmetric and may be unilateral (Fig. 151-7A). The chronicity, association of scaling and pruritus, absence of fever or leukocytosis, and response to compression, elevation, and topical corticosteroids can assist in diagnosis. Other lymphovascular diseases
Inflammatory
Infectious
■Stasis dermatitis
■Dermatophytoses
■Irritant/allergic contact dermatitis and other eczematous dermatitides
■Cutaneous candidiasis
■Erythema migrans
■Necrotizing soft-tissue infections
■Drug eruption
■Vasculitides
■Acute/chronic paronychia
■Panniculitides (eg, lipodermatosclerosis, erythema nodosum)
■Cutaneous mycobacterial infections Neoplastic/Paraneoplastic
■Neutrophilic dermatoses (eg, pyoderma gangrenosum, Sweet syndrome)
■Cutaneous lymphoma
■Paget disease
■Carcinoma erysipeloides
■Follicular occlusion (eg, hidradenitis suppurativa)
■Erythromelalgia Miscellaneous
■Sarcoidosis
■Arthropod bite
■Autoimmune connective tissue diseases
■Gout/pseudogout
■Calciphylaxis
■Radiation dermatitis Vascular
■Wells syndrome (eosinophilic cellulitis)
■Edema/lymphedema
■Hereditary periodic fever syndromes (eg, familial Mediterranean fever)
■Deep venous thrombosis
■Superficial thrombophlebitis
■Hematoma
2751
aCommonly misdiagnosed pseudocellulitides are highlighted in bold.
23
A
B
and sequelae, including deep venous thrombosis, hematoma, lipodermatosclerosis, and chronic edema or lymphedema, are commonly encountered and may mimic cellulitis. Eczematous dermatitides, such as allergic or irritant contact and asteatotic dermatitis, are usually discriminated by the presence of scaling and pruritus and absence of fever or leukocytosis. Bilateral involvement or geometric borders may be observed and aid diagnosis. Gout or pseudogout may mimic localized, early cellulitis, and can be accompanied by fever and leukocytosis, but typically overlies a joint. Erythema nodosum and small-vessel vasculitides tend to present as multifocal eruptions, but fever and leukocytosis are variably present (Fig. 151-7B). Erythema migrans is an important infectious mimic of cellulitis in endemic areas, may not present in the classic annular configuration, and can be accompanied by fever or systemic symptoms. The patient may not recall a history of tick bite. Other arthropod bites are usually multifocal without systemic symptoms. It is important to exclude necrotizing soft-tissue infections
2752
when evaluating cellulitis, as they require emergent surgical evaluation and debridement.
CLINICAL COURSE AND PROGNOSIS
The natural history of acute cellulitis is rarely observed in the modern era, however prior to use of antibiotics, therapeutic cure was achieved in approximately twothirds of patients with an 11% mortality rate.2 Cure rates are difficult to estimate in clinical trials because of the lack of definitive biomarkers for infection, but average approximately 80% to 85%, and are interestingly higher in complicated cellulitis than uncomplicated cases.48 These relatively low cure rates may be related to inadvertent inclusion of pseudocellulitis into antimicrobial trials, or prolonged time to complete recovery beyond the usual clinical assessment period.48,49 Without treatment, infection can spread into the bloodstream and become life-threatening. Prognosis for treated cellulitis is good and modern mortality rates are negligible in uncomplicated cases treated with antibiotics. The recovery period is usually several weeks, although by 30 days as many as 20% of patients have not yet returned to normal activities.49
Recurrence occurs in more than 10% of patients.11 This risk increases with number of previous reoccurrences, which is suggestive of predisposing systemic or local risk factors for infection. The common practice of outlining the involved area of cellulitis may be useful to monitor response to treatment, although indistinct margins, presence of “skip areas,” and occasional transient progression of erythema despite other evidence of clinical improvement may make interpretation difficult in some patients.50
Serial high-quality photographs can provide an alternative, reliable method to monitor treatment response, particularly in the inpatient setting where the primary provider may change during a patient’s hospitalization.50
MANAGEMENT
Empiric antibiotic therapy directed against streptococcal and staphylococcal species is recommended for the treatment of cellulitis, but the evidence of superiority for one regimen over another has not been definitively established.51 Treatment recommendations vary based upon the presence of purulence, systemic symptoms, and overall clinical assessment, the patient’s underlying risk factors, and community rates of drug-resistant pathogens. Outpatient therapy with oral antibiotics is appropriate in hemodynamically stable patients without evidence of systemic infection, but hospitalization may be required in the seriously ill, immunocompromised patients, or with failure of outpatient therapy.
23
DISEASE SEVERITY FIRST-LINE ANTIBIOTICS ALTERNATIVE ANTIBIOTICS
Nonpurulent cellulitis Mild (no evidence of systemic disease); outpatient setting with oral therapy
Moderate (≥2 SIRS criteria or failure of outpatient therapy); acute care setting with IV therapy
Severe (≥2 SIRS criteria with rapid progression, hypotension, or evidence of end-organ damage) or immunocompromised; hospitalization with IV therapy
■Consider surgical evaluation for necrotizing soft-tissue infection
■Cultures and sensitivities
Purulent cellulitis Mild (no evidence of systemic disease); outpatient setting with oral therapy
■Incise and drain; consider cultures and sensitivities
Moderate (≥2 SIRS criteria or failure of outpatient therapy); acute care setting with IV therapy
■Incise and drain; cultures and sensitivities
Severe (≥2 SIRS criteria with rapid
Severe (≥2 SIRS criteria with rapid progression, hypotension, or evidence of end-organ damage) or immunocompromised; hospitalization with IV therapy
progression, hypotension, or evidence of end-organ damage) or immunocompromised; hospitalization with IV therapy
■Consider surgical evaluation for necrotizing soft-tissue infection
■Consider surgical evaluation for
necrotizing soft-tissue infection
■Incise and drain; cultures and sensitivities
■Incise and drain; cultures and
sensitivities
■Cephalexin
■Clindamycin
■Dicloxacillin
■Macrolides (azithromycin, erythromycin)
■Penicillin V
■Cefazolin
■Clindamycin
■Ceftriaxone
■Consider vancomycin if associated IVDU or known MRSA colonization/infection
■Penicillin G
■Broad-spectrum with vancomycin and piperacillin-tazobactam
■Narrow as appropriate per cultures and sensitivities
■Clindamycin
MSSA suspected:
■Cephalexin
■Dicloxacillin MRSA suspected:
■Clindamycin
■Tetracyclines (doxycycline, minocycline, tetracycline)
■Trimethoprim-sulfamethoxazole
■Clindamycin
MSSA suspected:
■Oxacillin
■Linezolid (MRSA)
■Nafcillin
■Cefazolin MRSA suspected:
■Vancomycin
■Clindamycin
■Broad-spectrum with vancomycin and piperacillin-tazobactam
■Clindamycin
■Broad-spectrum with vancomy-
■Clindamycin
■Daptomycin
■Daptomycin
cin and piperacillin-tazobactam
■Narrow as appropriate per cultures and sensitivities
■Ceftaroline
■Narrow as appropriate per cul-
■Ceftaroline
■Telavancin
■Telavancin
tures and sensitivities
■Tigecycline
■Tigecycline
IVDU, IV drug use; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive Staphylococcus aureus; SIRS, systemic inflammatory response syndrome (temperature >38°C [100.4°F] or <36°C [96.8°F]; pulse >90 beats/min; respiratory rate >20 breaths/min; or leukocyte count >12,000 cells/µL or <4000 cells/µL).
ANTIBIOTICS
ANTIBIOTICS
NONPURULENT CELLULITIS
Nonpurulent cellulitis without systemic evidence of infection should be treated with oral antistreptococcal antibiotics such as cephalexin, dicloxacillin, or penicillin V. In cases of true Type I hypersensitivity reactions to penicillins or cephalosporins, clindamycin or macrolides should be considered.26,29 No difference in failure rate between β-lactams and non–β-lactams has been demonstrated, although some studies have shown higher rates of treatment-related adverse events
(predominantly GI symptoms) among patients treated with non–β-lactams.52,53 Addition of clindamycin or trimethoprim-sulfamethoxazole, both agents with activity against MRSA, to β-lactam antibiotics have not demonstrated significant benefits over β-lactam coverage alone for uncomplicated nonpurulent cellulitis.49,54
Patients with evidence of systemic infection, including 2 or more systemic inflammatory response syndrome criteria (temperature >38°C [100.4°F] or <36°C [96.8°F]; pulse >90 beats/min; respiratory rate >20 breaths/min; or leukocyte count >12,000 cells/µL or <4000 cells/µL), or those who fail outpatient treatment should receive parenteral antibiotics such as cefazolin, ceftriaxone, or penicillin G.26 Clindamycin
2753
23
should be used in patients with true Type I hypersensitivity reactions to penicillins or cephalosporins. If there is associated penetrating trauma, including injection drug use, or known MRSA colonization or infection elsewhere, empiric coverage with vancomycin may be indicated. Severe infections with rapid progression, hypotension, end-organ dysfunction, or in immunocompromised patients or in those suspected of having atypical or resistant organisms should be treated with broad-spectrum parenteral antibiotics and narrowed according to culture and sensitivity results.26,29
PURULENT CELLULITIS
Patients with purulent cellulitis should be cultured and fluid collections incised and drained. In mild disease, empiric therapy with oral anti-staphylococcal antibiotics should be initiated while awaiting culture and sensitivity results. The decision to treat for methicillin-sensitive S. aureus (MSSA) versus MRSA should depend upon clinical suspicion based on host or environmental factors, including history of known MRSA colonization, patient risk factors, and local rates of MRSA infections. Cephalexin and dicloxacillin are first-line agents of choice in MSSA, whereas clindamycin, tetracyclines, and trimethoprim-sulfamethoxazole are used in MRSA. In these cases, concomitant coverage for streptococcal species may be required.26,29 If penicillin or cephalosporin allergy exists, clindamycin is an alternative. Note some geographic regions demonstrate high rates of inducible clindamycin resistance in S. aureus isolates. Patients with systemic infection or failure of outpatient treatment require parenteral antibiotics (Table 151-6). Oxacillin, nafcillin, and cefazolin, or clindamycin in penicillin-allergic or cephalosporinallergic patients, are appropriate for MSSA.26,29
Vancomycin, clindamycin, or linezolid are preferred in MRSA.26,29 Severe infections or infections in special patient populations require broad-spectrum parenteral antibiotic coverage, including against MRSA, while awaiting culture and sensitivity results.
DURATION
The optimal duration of antibiotic therapy has not been identified in clinical trials. The IDSA guidelines recommend 5 days for uncomplicated patients, with extension of therapy if signs of infection persist.26 In
At least 2 or more of the following Temperature >38°C (100.4°F) or <36°C (96.8°F) Pulse >90 beats/min Respiratory rate >20 breaths/min Leukocyte count >12,000 cells/µL or <4000 cells/µL or Failed outpatient treatment
2754
general, 5 to 10 days are recommended for uncomplicated patients with slightly longer courses (7 to 14 days) for immunocompromised patients.29 Reassessment at 24 to 72 hours is important to assess response to therapy.
RECURRENT CELLULITIS AND PROPHYLAXIS
Recurrent episodes of cellulitis may require longer treatment courses or hospitalization, although the majority can be managed in the ambulatory setting. Risk factors for recurrence should be addressed (see section “Prevention”). Although controversial, prophylactic antibiotics, such as low-dose penicillin or erythromycin, should be considered if there are 3 to 4 recurrences per year despite these efforts.26 Prophylaxis may reduce both the incidence of first reoccurrence after primary cellulitis and subsequent recurrences, but these effects diminish after discontinuation of therapy.55-58 Optimal type, dosing, and duration of antibiotics require further investigation. Prophylaxis has demonstrated cost-effectiveness, but long-term tolerability data is lacking and its effects on antibacterial resistance patterns are unknown.59
ADJUNCTIVE TREATMENTS
ADJUNCTIVE TREATMENTS
Combination therapy with antibiotics and adjunctive antiinflammatories, including nonsteroidal antiinflammatory drugs (NSAIDs) and systemic corticosteroids, may be beneficial in some patients. NSAIDs may reduce time to regression of inflammation.60,61 However, there are concerns over their effects on neutrophil chemotaxis as NSAID use has been correlated with an increased risk of skin infection in children with varicella.62,63
Despite concerns over immunosuppressive effects, the addition of prednisolone to antibiotics has demonstrated shortened time to healing in uncomplicated erysipelas with a trend toward decreased relapse, and oral corticosteroids in combination with parenteral antibiotics reduced resolution time and ocular complications in orbital cellulitis.64-66 The IDSA guidelines recommend consideration of systemic corticosteroids in nondiabetic adult patients with cellulitis.26
PREVENTION
PREVENTION
Treatment of predisposing factors, including lymphedema, toe web infections, and local skin barrier defects, and underlying medical conditions is recommended to prevent primary and recurrent episodes of cellulitis. Decolonization strategies for MRSA carriage are controversial and their effectiveness in reducing the risk of cellulitis requires further study.67
ACKNOWLEDGMENTS
The author acknowledges the contributions of Adam D. Lipworth, Arturo P. Saavedra, Arnold N. Weinberg, and Richard Allen Johnson, the former authors of this chapter.
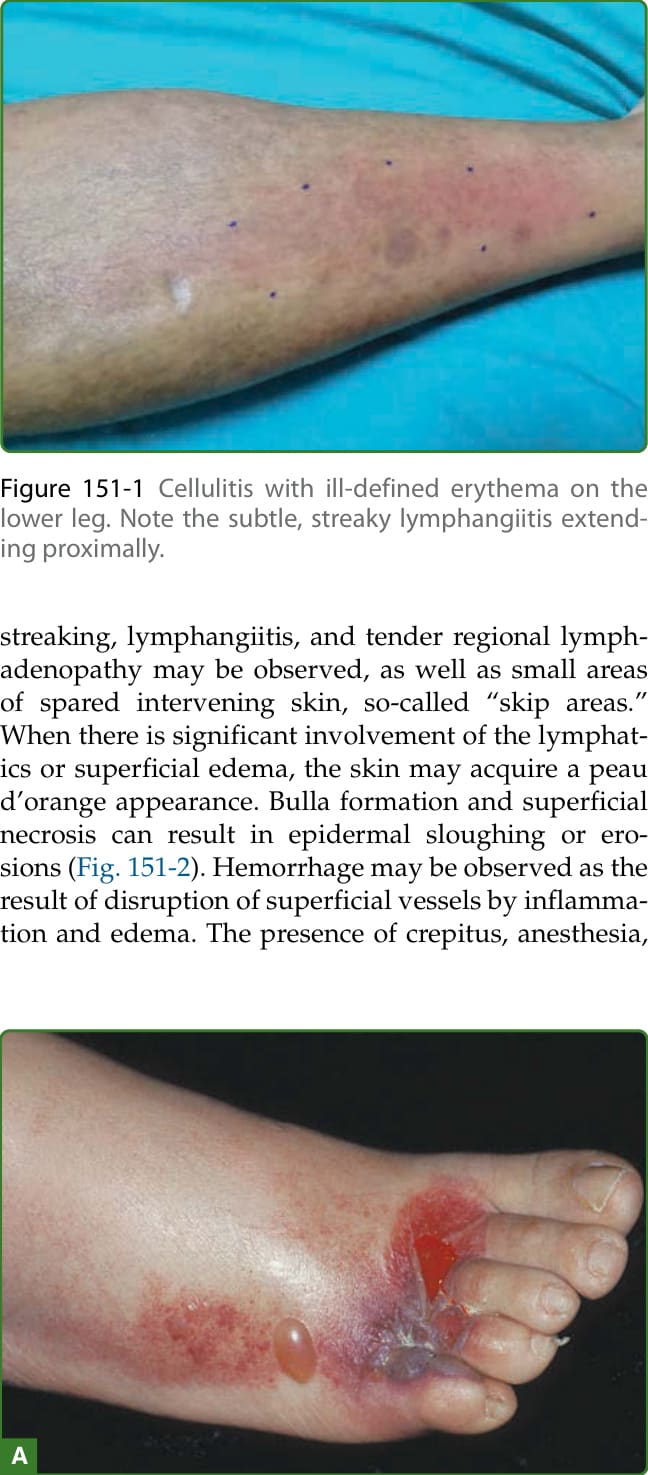
Figure 151-1 Cellulitis with ill-defined erythema on the lower leg. Note the subtle, streaky lymphangiitis extending proximally.

Figure 151-2 Cellulitis with swelling, erythema, and tenderness. A, Note blister formation on the lower extremity. B, Cellulitis emanating from an upper-extremity abscess.
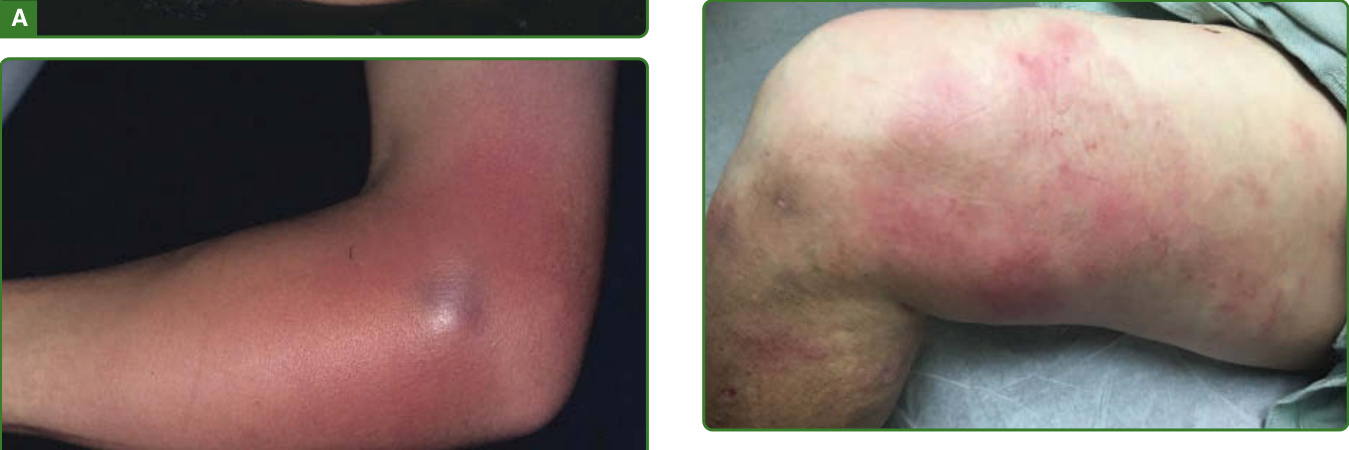
Figure 151-3 Recurrent cellulitis. Note the patchy, illdefined erythema with “skip areas” on the medial thigh and lower leg. This pattern may be observed more frequently in recurrent cellulitis as a result of underlying lymphatic damage.

Figure 151-4 Erysipelas. There is painful, warm erythema of the lower extremity with well-defined borders.
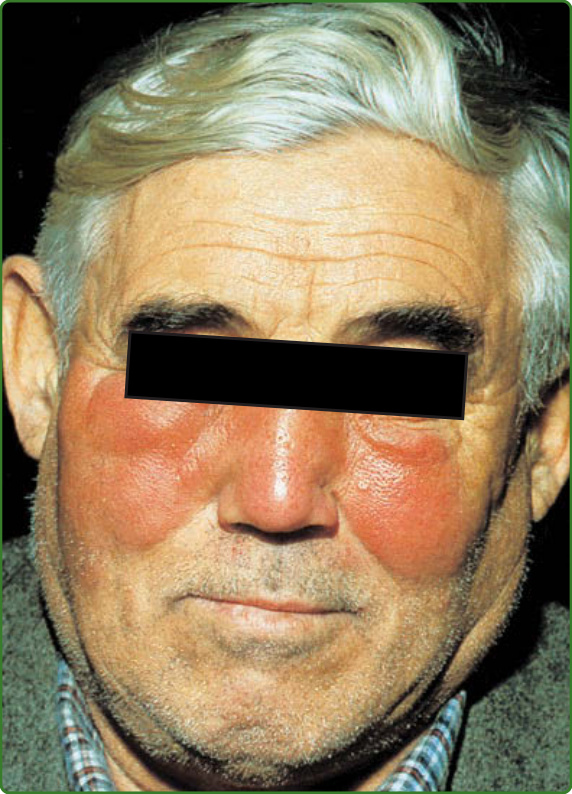
Figure 151-5 Erysipelas. Painful, edematous erythema with sharp margination on both cheeks and the nose. There is tenderness, and the patient has fever and chills.

Figure 151-6 A, Cellulitis after puncture trauma. The forearm is swollen, erythematous, and tender; there is abscess formation. B, Cellulitis, caused by Staphylococcus aureus infection, arising at the site of a surgical excision. Note discharge of pus.

Figure 151-7 A, Stasis dermatitis with linear excoriations. The eruption is eczematous with evidence of scratching (because of pruritus), which would be atypical in cellulitis. Note the “marker sign,” commonly observed in hospitalized patients seen by dermatology consultants, which is testament to the difficulty of diagnosis. B, Cutaneous small-vessel vasculitis attributed to naproxen use. The purpuric eruption is bilateral and located in areas of dependency, consisting of coalescing papules and plaques with secondary blister formation. This patient has low-grade elevated temperatures.
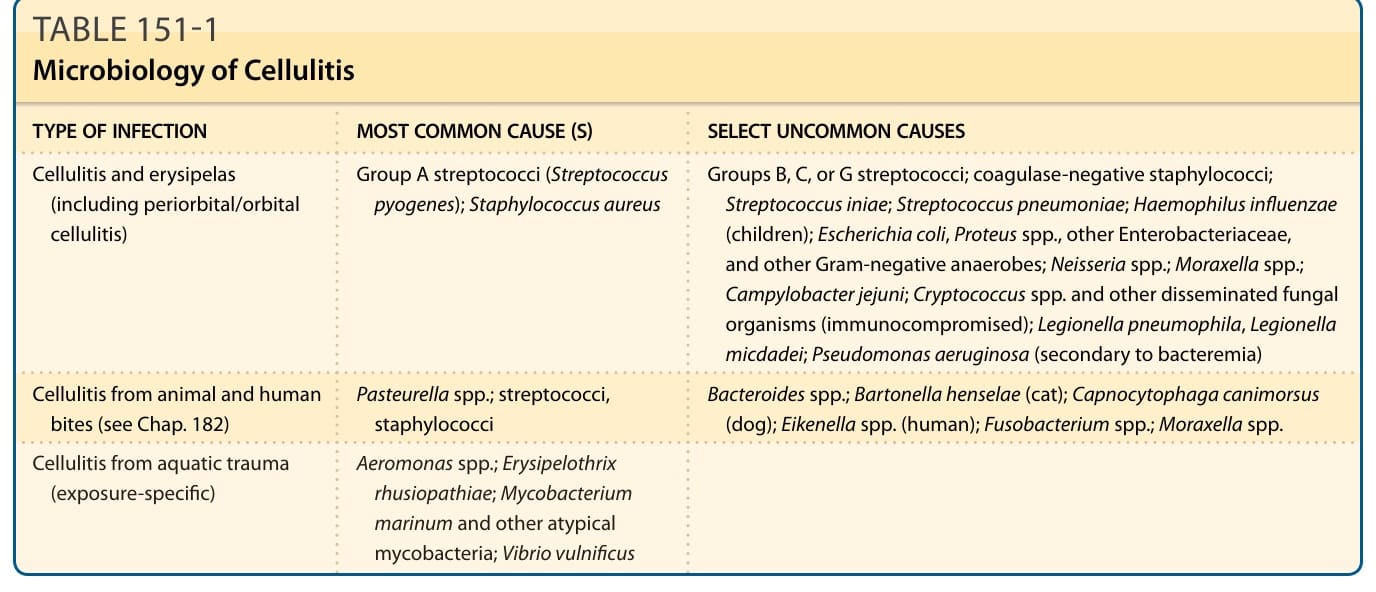
TABLE 151-1 Microbiology of Cellulitis
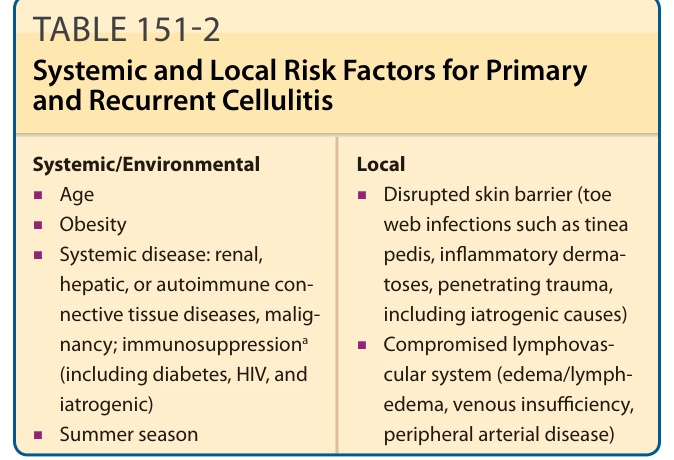
TABLE 151-2 Systemic and Local Risk Factors for Primary and Recurrent Cellulitis
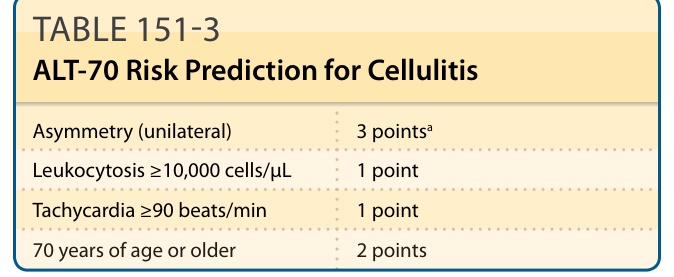
TABLE 151-3 ALT-70 Risk Prediction for Cellulitis
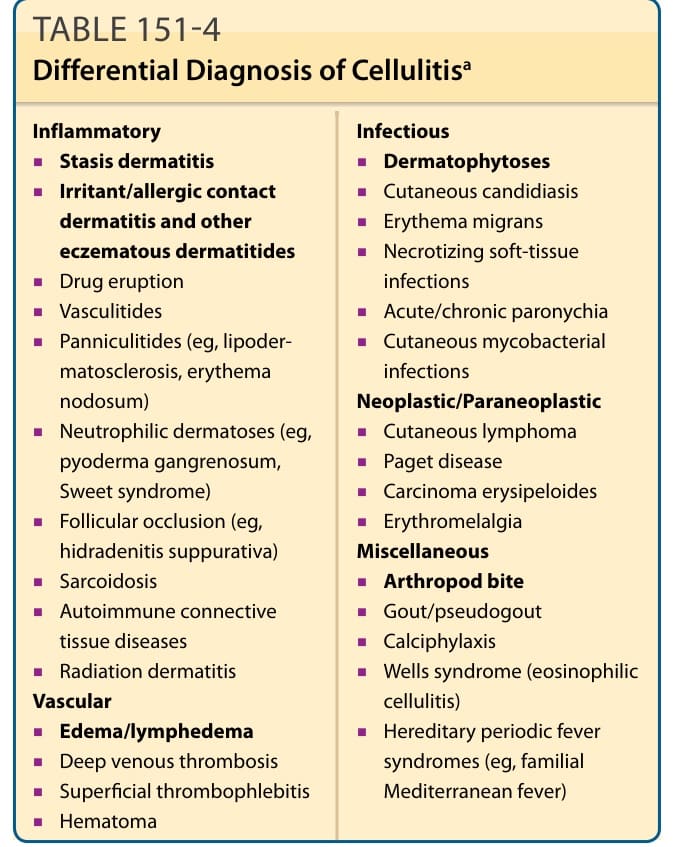
TABLE 151-4 Differential Diagnosis of Cellulitisa
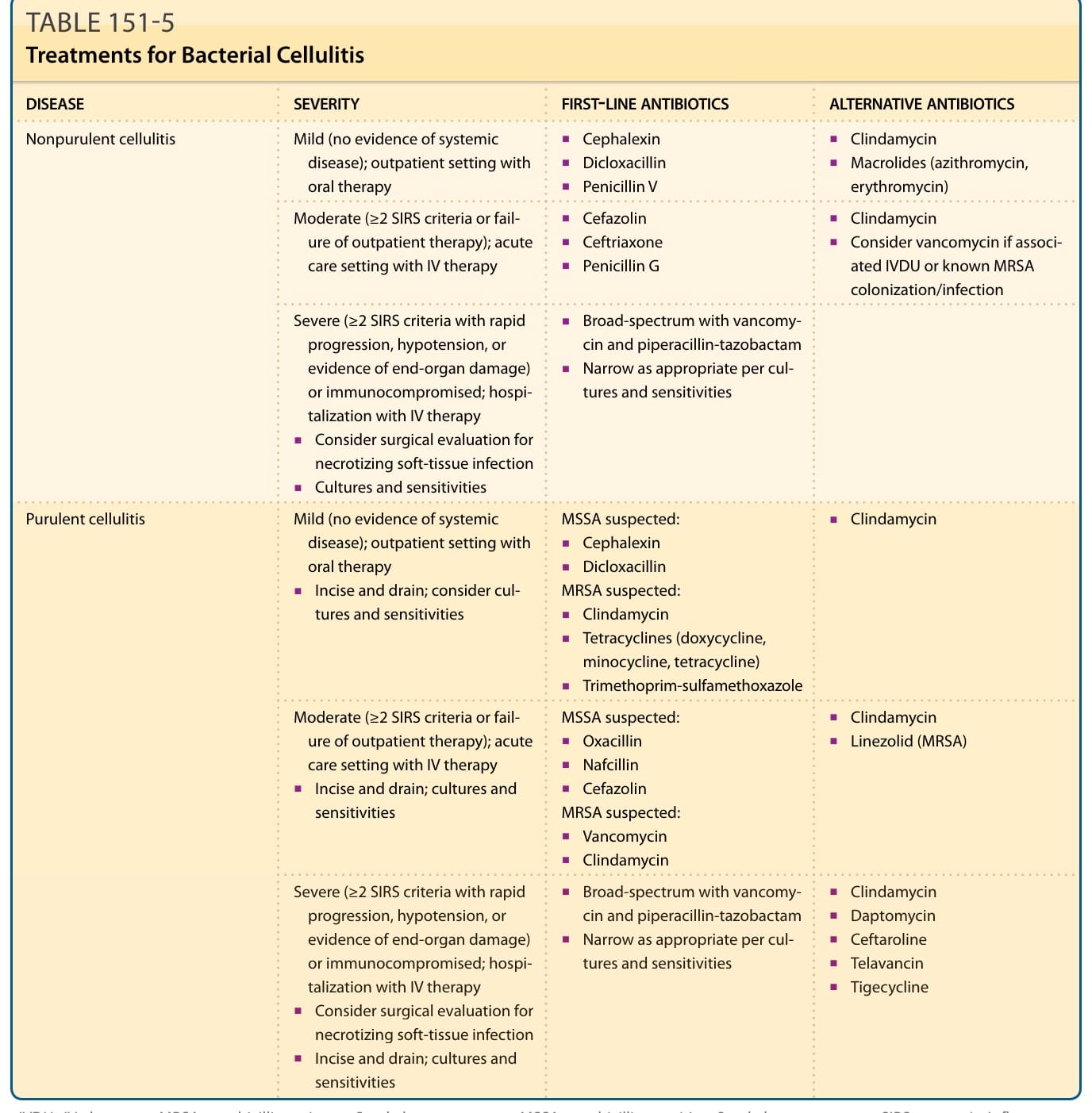
Table 151-5 outlines the treatments for bacterial cellulitis.