Wound Healing
22
AT-A-GLANCE
■ While acute and chronic wounds are different, all chronic wounds start as an acute wound.
■ In acute wounds, there is an orderly progression from injury to coagulation, inflammation, cell and matrix proliferation, cell migration, and tissue remodeling.
■ In the initial phases, a wide range of growth factors, including platelet-derived growth factor and transforming growth factor-β1, play an important role. In the proliferation/ migration and modeling phases, tissue matrix metalloproteinases (MMPs), integrins, basic fibroblast growth factor, and epidermal growth factor are critical. MMP-1, MMP-9, and MMP-10 are essential for remodeling.
■ For acute wounds, moist wounds heal faster, and a variety of wound dressings are available, including hydrogels, polyurethane films, hydrocolloids, foams, alginates, superabsorbent dressings, and collagen-based products.
■ In chronic wounds, the linear progression between the sequential phases of acute wound healing is lost. Chronic wounds are often the result of ischemia, pressure, and infection; healing, in part, is dependent on addressing these factors.
■ Healing after skin grafting is also different, as it depends on revascularization, either neovascularization or inosculation.
Wound healing involves a complex but overlapping sequential series of events aimed at barrier restoration, from hemostasis to inflammation, proliferation, and remodeling. Many mediators, such as platelets, neutrophils, macrophages, cytokines, growth factors, matrix metalloproteinases, and their inhibitors regulate these events.1 Some wounds fail to move through these stages in an orderly and timely fashion and become chronic wounds. All these components play a role in healing, and alteration in one or more of these components may impair healing and/or lead to abnormal scar formation, such as a hypertrophic scar or keloid.2
Wounds can be categorized by the depth of the wound, which helps predict the amount of scarring that will occur. Greater scarring occurs in full-thickness versus partial or spilt-thickness wounds. Figure 149-1 outlines these differences.
DIFFERENT TYPES OF WOUND HEALING
Primary healing, also called healing by primary or first intention, is the closure of the wound soon after wound creation, as seen in surgical wounds and clean lacerations. Wound closure is aided by approximation of the wound edges using sutures, glues, tapes, or mechanical devices, and in side-to-side closure and with grafts and flaps. Delayed primary healing is the slightly delayed closure of a wound, typically by a few days. As an example, a contaminated wound may first be treated with antimicrobials to assure eradication of bacteria that might delay healing. In healing by secondary intention, the open wound heals through a process that includes granulation tissue formation and epithelialization. Commonly employed after an excessive loss of soft tissue, such as major trauma or severe burns, the large defect requires ingrowth of granulation tissue and extracellular matrix (ECM) formation. Myofibroblasts plays a major role in this type of healing,1 appearing 3 days after the injury and reaching a maximum level 10 to 21 days postinjury. Secondary intention healing may result in wound contracture and can cause functional restriction. Tertiary intention occurs when a wound originally closed by primary intention dehisces and then heals by secondary intention. The time to complete healing depends on many factors such as the depth of the wound, location of the wound (eg, facial wounds heal faster than acral wounds), vascular supply, presence of infection, and wound shape (smaller diameter wounds heal faster than larger diameter wounds of the same size/area.)3
MECHANISMS OF WOUND HEALING
PHASES OF WOUND HEALING
PHASES OF WOUND HEALING
Tissue injury triggers a cascade of sequential, overlapping events that have been categorized into several phases, including: (a) coagulation, (b) the inflammatory phase, (c) the proliferative (and migratory) phase, and (d) the remodeling phase. Figure 149-2 illustrates these phases in diagrammatic form, and Fig. 149-3 shows specific events that take place during the various phases. The cell types primarily involved in wound
Split- and full-thickness wound areas
Full-thickness wound Split-thickness wound
Epidermis
Dermis
Subcutaneous tissue
22
healing are platelets, neutrophils, and macrophages, fibroblasts, endothelial cells, and epithelial cells. More recently, increasing importance is accumulating for the role, either directly or indirectly, of lymphocytes.4,5
COAGULATION
Immediately after injury, disruption of blood vessels leads to local release of blood cells and bloodborne elements, resulting in clot formation and activation of the intrinsic and extrinsic coagulation cascade.3
While the blood clot within the vessel lumen provides hemostasis, the clot within the injury site acts as a provisional matrix for cell migration, leads to further formation of ECM,6 and provides a reservoir for cytokines and growth factors.7,8 Platelets degranulate and release α granules which secret growth factors including platelet-derived growth factors, insulin-like growth factors, epidermal growth factors, transforming growth factor-β, and platelet factor 4. Platelets also release a number of chemotactic factors that attract other platelets, leukocytes, and fibroblasts to the site of injury.8,9 The clot also contains fibrin, fibronectin, vitronectin, von Willebrand factor, and thrombospondin, which provide a matrix for cell migration. Vasoactive amines released from platelets, such as serotonin, facilitate cell migration by increased microvascular permeability. Hageman factor XII is a specific enzyme released following platelet aggregation to initiate the intrinsic coagulation cascade. Prothrombin transforms into thrombin, converting soluble fibrinogen to insoluble fibrin. Additionally, injured
The different phases of wound healing
Phases of healing Main cell types involved
Coagulation phase Platelets
Inflammatory phase
Migratory/proliferative phase
Remodeling phase
Platelets Macrophages Neutrophils
Macrophages Fibroblasts Epithelial cells Endothelial cells
Fibroblasts Myofibroblasts
Injury Hours Days Weeks
2701
22
The phases of wound healing and key cells and events involved
Time Phases Main cell types Specific events
Coagulation
Platelets Fibrin plug formation, release of growth factors, cytokines, hypoxia
Hours
Inflammatory
Platelet aggregation and release of fibrinogen fragments and other pro-inflammatory mediators
Selectins slow down blood cells + binding to integrins diapedesis
Neutrophils Monocytes Macrophages
Cell recruitment and chemotaxis, wound debridement
Days
Migratory/proliferative
Hemidesomosome break-down keritinocyte migration
Keratinocytes Fibroblasts Endothelial cells
Epidermal resurfacing, fibroplasia, angiogenesis, ECM deposition, contraction
Remodeling
Scar formation and revision, ECM degredation, further contraction and tensile strength
Cross-talk between MMPs, integrins, cells, cytokines cell migration, ECM production
Phenotypic switch to myofibroblasts from fibroblasts
Myofibroblasts
Weeks to months
tissue releases a tissue factor that activates the extrinsic coagulation pathway.9
INFLAMMATION
Inflammation begins with activation of classic and alternative complement cascades and subsequent neutrophil infiltration to the wound site within 24 to 48 hours of injury. White cells have multiple functions, including phagocytosis of necrotic material and bacteria, as well as the production of certain critical cytokines.10,11 Leukocytes adhere to the adjacent blood vessels (margination) and actively move through the vessel wall via diapedesis. Leukocytes release enzymes and oxygen-derived free radicals. After the first few days, the constituency of white cells changes as neutrophils are replaced by macrophages.12
Macrophages, often considered the most important regulatory cells in the wound healing inflammatory process, typically appear in the wound site 72 hours after the injury. Macrophages, key regulator cells for repair, are the main phagocytic cells and release proteolytic enzymes such as a variety of collagenases. Macrophages also produce growth factors responsible for the smooth muscle proliferation and endothelial cell and fibroblast proliferation, all of which contribute to ECM production. This hypoxic environment is associated with high levels of proteases and low pH, both of which contribute to activation of growth factors.11
Monocytes are attracted to the injury site by kallikrein, fibrinopeptides, and fibrin-degradation products; some
2702
of these same chemoattractants are also responsible for recruitment of neutrophils.13,14 Other more specific chemoattractants further recruit monocytes, including collagen fragments, fibronectin, elastin, and transforming growth factor (TGF)-β1. Monocytes undergo a phenotypic change to tissue macrophages critical for the progression of healing.15,16 Macrophages release chemotactic factors to attract fibroblasts to the wound area. Importantly, they display impressive plasticity, and at least 2 subsets of macrophages exist and have distinct phenotypes in various stages of healing (see below). They also produce a variety of growth factors, such as platelet-derived growth factor (PDGF), fibroblast growth factors (FGFs), and vascular endothelial growth factors (VEGFs), as well as TGF-β and TGF-α. Alterations in tissue macrophages or circulating monocytes lead to poor intrinsic debridement, delay proliferation of fibroblasts, and allow for inadequate angiogenesis and overall poor healing.17
Macrophages are divided into M1 (or classically activated) and M2 (or alternatively activated) macrophages. M1 phenotype macrophages are activated by interferon-γ and tumor necrosis factor (TNF)-α following wound formation. They release interleukin (IL)-12 and promote a proinflammatory T-helper (Th)-1 immune response early on. Subsequently, M2 macrophages, activated by IL-4 and IL-13, work to downregulate inflammation by releasing antiinflammatory cytokines such as IL-10. These M2 macrophages present later in healing during granulation tissue formation.17-19
ABNORMAL INFLAMMATORY PHASE
Immediately after injury, local vasodilation, extravasation of blood and fluid, and lymphatic drainage blockage (in some cases) can lead to cardinal symptoms of inflammation such as heat, redness, pain, and swelling. The acute inflammatory response may last 2 weeks; however, prolongation of inflammation (chronic inflammation) may delay healing.20
With chronic inflammation, the wound often contains necrotic tissue and pathogenic organisms. In this case, granulocytes disappear and mononuclear cells, particularly monocytes, lymphocytes, and macrophages, become the predominant cells at the site of inflammation. From the clinical standpoint, certain wounds, such as pyoderma gangrenosum, have excessive inflammation and treatment, with corticosteroids for example, leads to downregulation of inflammation and healing. Fine-tuning the inflammatory response may represent a therapeutic target for other wounds as well.21
PROLIFERATION
The proliferative phase, characterized by fibroblast migration, deposition of ECM, and formation of granulation tissue, normally starts at about day 3 after wounding and lasts for 2 to 4 weeks. Figure 149-4 illustrates events that occur in the proliferative/migratory and remodeling phases. An important event in this phase is reepithelialization. This critical event also involves migration of keratinocytes and the interdependence between keratinocyte movement over the provisional fibrin matrix, recruitment of fibroblasts and endothelial cells, and ECM formation.22
Growth factors, such as PDGF and TGF-β, attract fibroblasts to the wound. Fibroblasts subsequently
22
proliferate and produce a matrix consisting of fibronectin and hyaluronan initially, and collagen and proteoglycans later. These components are essential for new ECM formation and tissue repair. ECM serves both as turgor of soft tissue and as a scaffold and regulator of cell adhesion and growth. It is made of an interstitial matrix of adhesive proteins embedded in proteoglycan and glycosaminoglycan gel as well as the fibrinous structural proteins collagen and elastin.23
Fibroblasts make collagen, the most abundant protein in the body, and noncollagenous proteins. During the proliferative phase, collagen synthesis is induced by PDGF, basic FGF (bFGF), TGF-β, IL-1, and TNF. There are 18 different types of collagen. Fibrillar collagens, such as I, III, and V, form the connective tissue in the healing wound, and nonfibrillar forms, such as collagen IV, form the basement membrane. Collagen gene expression is regulated by multiple factors such as TGF-β and FGF. TGF-β stimulates production of collagen I and collagen III. The overexpression of matrix metalloproteinases (MMPs) and/or impaired counteraction of tissue inhibitor of metalloproteinases (TIMPs) contributes to delayed healing and fibrosis. Interaction between these cytokines is extremely important. The fibroblasts in patients with longstanding diabetic foot ulcers show a decreased response to TGF-β1 and decreased expression of TGF-β receptors. Although overexpression may be problematic, tissue matrix MMPs and other enzymes, such as plasminogen activator inhibitor, are critical to the movement of cells through provisional structural matrix components. Adhesive proteins, including fibronectin (FN), laminin, thrombospondin, and integrins, help guide cellular migration.24 FN is a large heterodimer linked to cell surfaces, basal membranes, and the ECM. FN can attach to ECM components such as collagen, fibrin,
Epidermal migration Keratinocyte proliferative burst
Fibrin plug
Hair follicle keratinocyte contribution after injury
Hemidesmosome disassembly/keratinocyte migration
Angiogenesis Cell migration and recruitment
ECM deposition stimulated by growth factors, cytokines
2703
22
and proteoglycan, or to integrins and directly mediate the cell migration. FN also activates intracellular signaling pathways to increase the sensitivity of certain cells, such as endothelial cells, to growth factors.25
Integrins are important in cell–cell and cell–matrix adhesion, serving to regulate interaction between ECM and the cytoskeleton. The integrins, consisting of at least 24 αβ heterodimers (18 α and 8 β subunits), are transmembrane cell surface receptors that bind the ECM to cytoskeletal structures.25 The integrin profile is very dynamic during the repair process. For example, dermal fibroblasts undergo a switch from α2 to α3 and α5 integrin subunits. As another example, endothelial cells cannot respond to angiogenic stimuli without the expression of αvβ5 integrin. Certain polypeptide growth factors are essential to angiogenesis, including bFGF and VEGF.25,26 Table 149-1 highlights the main cytokines and growth factors shown to play a role in the repair process. Another constituent of ECM are noncollagenous proteins such as proteoglycans, which are glycosaminoglycans (dermatan sulfate, heparin sulfate) linked
to a protein backbone that modulate cell growth and differentiation. Additionally, glycosaminoglycans without a protein core (hyaluronan) are also important components of the ECM. Histopathology of a granulating wound bed shows proliferation of fibroblasts and capillaries in a loose ECM. Neovascularization, or formation of new blood vessels, is characteristic of this stage. Several factors induce angiogenesis as a part of granulation tissue development; new capillaries sprout, invading the fibrin and FN-rich clot. The density of blood vessels is reduced over time with scar formation and as the wound moves toward the remodeling phase.26
Fibroblast replication and longevity are enhanced in hypoxia, and low oxygen tension stimulates clonal expansion of dermal fibroblasts seeded as single cells.27
Moreover, the synthesis of a number of growth factors is enhanced in hypoxic cells. After a provisional matrix has formed, keratinocytes migrate to epithelize the wound. MMP function is critical for allowing keratinocytes at the edge of the wound to detach from their hemidesmosomal and
GROWTH FACTOR MAJOR SOURCES FUNCTION
Epidermal growth factor (EGF) Platelets, macrophages, fibroblasts Epithelialization Fibroblast proliferation Keratinocyte proliferation Angiogenesis
Transforming growth factor (TGF)-α Keratinocytes, macrophages, fibroblasts, lymphocytes Keratinocyte migration
TGF-β Macrophages, fibroblasts, keratinocytes, platelets Inflammation, angiogenesis, reepithelialization, connective tissue regeneration, remodeling TGF-β1, TGF-β2: promote fibrosis and scar formation TGF-β3: antiscar properties
Activins Fibroblasts, keratinocytes Epithelialization
Fibroblast growth factor (FGF) Keratinocytes, fibroblasts, smooth muscle cells, chondrocytes, endothelial cells, mast cells
FGF-2: granulation tissue formation, reepithelialization, tissue remodeling, fibroblast migration, collagen formation FGF-7, FGF-10: increase transcription factors, detoxification of reactive oxygen species FGF-7: neovascularization
Platelet-derived growth factor Platelets, macrophages, vascular endothelium, fibroblasts Fibroblast proliferation Angiogenesis Matrix formation
Vascular endothelial growth factor (A-E) Keratinocytes, endothelial cells, fibroblasts, smooth muscle cells, platelets, neutrophils, macrophages
Granulocyte-macrophage colony-stimulating factor Macrophages Fibroblasts Endothelial cells Natural killer cells Mast cells
Interleukin (IL)-1 Monocytes Macrophages Keratinocytes
IL-6 Neutrophils Monocytes
Angiogenesis
Keratinocyte proliferation Epithelialization Cell migration Chemotaxis Angiogenesis
Keratinocyte proliferation Fibroblast proliferation Angiogenesis Neutrophil chemotaxis
Keratinocytes proliferation Neutrophil chemotaxis
IL-6 Neutrophils Monocytes Keratinocytes proliferation Neutrophil chemotaxis
2704
desmosomal attachments and migrate across the provisional matrix. Other proteins play important roles, including plasminogen activator inhibitor, a serine protein inhibitor that functions as the main inhibitor of tissue plasminogen activator, and urokinase plasminogen activator.28
Upregulation of tissue plasminogen activator and urokinase plasminogen activator are important for keratinocyte migration, which may depend on crosstalk and interactions between α3β1, keratinocytes, and collagen. These events lead to the induction of MMP-1 (collagenase-1 or interstitial collagenase), which is important for keratinocyte migration and epithelialization.6 MMP-9 plays a fundamental role in “cutting” Type IV and Type VII collagen, which are essential components of the basement membrane and anchoring fibrils, and promotes inflammation and neutrophil migration. For keratinocyte migration to occur, a necessity exists to break down these complex structures anchoring the basal keratinocytes to the basement membrane and neighboring keratinocytes. This process is as complex as the structure itself, and involves interactions between MMPs, integrins, growth factors, and structural proteins. In the normal resting state, laminin-332 is bound to α6β4-integrin, the latter linking the intracellular keratin filaments of keratinocytes to the basement membrane. As a result of the interaction of integrins (including their phosphorylation status) with the ECM and their receptor clustering on the surface of keratinocytes, important morphologic changes, such as lamellipodia formation, occur for keratinocyte locomotion.29-31 Migration of keratinocytes is essential for resurfacing of the wound.26,32
Keratinocytes begin to migrate from the wound edge and from skin appendages within the first 24 hours. The hair bulge, the germinative portion of the hair, is an important reservoir for keratinocytes in partial thickness wounds. A series of events in migration involves elongation of keratinocytes, development of pseudopod-like projection of lamellipodia, loss of cell-to-cell adhesion, retraction of intracellular tonofilaments, and formation of actin filaments at the edge of the cytoplasm, all of which occur while the proliferative ability of keratinocytes is inhibited. To facilitate migration, there is a marked increase in mitotic activity within the basal epithelial cells of the wound edge from 12 hours, extending lamellipodia along the wound edges. Subsequently keratinocytes lose their attachment to the underlying dermis to migrate in a leapfrog fashion. Eventually a new basement membrane forms and further growth and differentiation of epithelial cells establishes the stratified epithelium. The process of epithelialization is facilitated in a moist environment, serving as the biologic basis for modern occlusive dressings.
REMODELING
The final phase, remodeling, is typically the longest phase, involving the continuous synthesis and
22
breakdown of collagen as the ECM evolves. Starting early in the healing process, wound remodeling may continue for months. The interaction of ECM and fibroblasts causes wound contraction and is influenced by multiple cytokines, including TGF-β, PDGF and bFGF. The remodeling of the ECM, as well as the movement of cells, is highly dependent on MMPs and serine proteases.33 An important component of this dependence on MMPs is MMP-driven degradation of ECM and the resulting exposure of selective bioactive ECM segments that influence cell behavior, including migration and proliferation.6,33
Metalloproteinases produced by fibroblasts, neutrophils, keratinocytes, and macrophages, include interstitial collagenase (degrades collagen Types I, II, and III), gelatinases (degrades denatured collagen and FN) and stromelysins (degrades proteoglycans, laminin, FN, and amorphous collagen). MMP-10 (stromelysin) breaks down other noncollagenous ECM components and facilitates migration.6,11,34 Other mediators, such as thymosin-β, upregulate MMPs during wound repair.35 The activity of MMPs are tightly regulated because they may degrade essential collagens and impair healing. They are activated by certain proteins (plasmin) and inhibited by specific tissue inhibitors of metalloproteinases. Table 149-2 summarizes certain MMPs and their prominent effect in wound healing. During the remodeling process, a phenotypic switch occurs in certain cell subpopulations from fibroblasts to myofibroblasts.36 Although the early process of healing relies largely on matrix accumulation, which, in turn, facilitates cell migration, later healing requires a dampening of ECM formation to a level that at least approximates the preinjury state. However, the remodeling phase is more than a breakdown of excess macromolecules formed during the proliferative phase of wound healing. During this phase, cells within the wound are returned to a stable phenotype, ECM material is altered (ie, collagen Type III to collagen Type I), and granulation tissue disappears.11,26 Granulation tissue evolves to a scar composed of less-active fibroblasts, dense collagen, and fragments of elastic tissue along with the rest of ECM. Scar matures and the tensile strength increases to a maximum of 80% strength of noninjured skin. In full-thickness wounds, contraction is responsible for 40% of the decrease in wound size.
FETAL HEALING
FETAL HEALING
During early embryogenesis, wounded fetal tissue heals without fibrosis. Regeneration, as opposed to repair, occurs. Later in embryogenesis (last trimester) and after childbirth, repair (as opposed to regeneration) occurs, with resulting fibrosis. Among factors that affect scarring, fibromodulin is a small glycoprotein that mediates scarless healing in fetal skin.37
2705
22
EFFECT COMMON NAMES CORRESPONDING MMP DESIGNATION SOME SPECIFIC EFFECTS
Keratinocyte proliferation and migration
Collagenase 1 Gelatinase A Stromelysin 2 Matrilysin-1 Epilysin
Endothelial cell (EC) migration
Collagenase 3 Gelatinase A MT1-MMP
Cell migration
Stromelysin 1 Stromelysin 2 Matrilysin-2
Inflammation
Collagenase 2 Gelatinase A Gelatinase B Matrilysin-1
MMP-1 MMP-2 MMP-10 MMP-7 MMP-28
Increased migration
MMP-13 MMP-2 MMP-14
Increases EC migration Needed for angiogenesis Needed for angiogenesis
MMP-3 MMP-10 MMP-26
Required for excisional wounds
MMP-8 MMP-2 MMP-9 MMP-7
Antiinflammatory Antiinflammatory Promotes inflammation
Neutrophil migration
Gelatinase B MT6-MMP MMP-9 MMP-25
Increases neutrophil migration
Apoptosis Collagenase 2 MT1-MMP MT2-MMP MT6-MMP
Apoptosis
Collagenase 2 MT1-MMP MT2-MMP MT6-MMP
MMP, matrix metalloprotease; MT, membrane type.
GROWTH FACTORS AND CYTOKINES
GROWTH FACTORS AND
CYTOKINES
Wound healing is regulated by multiple growth factors and cytokines released at the wound site. Growth factors are biologically active polypeptides that can alter the growth, differentiation and metabolism of a target cell. They are important elements in the healing of wounds. Table 149-1 lists the major growth factors and cytokines involved in healing and their respective roles.38-40 Although potentially important in healing from a therapeutic standpoint, only PDGF-BB, bFGF, and granulocyte-macrophage colony-stimulating factor (GM-CSF) are used clinically in the management of wounds, and only PDGF is approved for wound healing by the U.S. Food and Drug Administration (FDA).
EPIDERMAL GROWTH FACTOR FAMILY
Epidermal growth factor (EGF) family members bind to a tyrosine kinase transmembrane protein or EGF receptor.41 EGFR normally localizes throughout the epidermis with its membranous presence being more prominent in the basal layer. EGFR plays an important role in reepithelialization by increasing keratinocyte proliferation and cell migration.42,43
2706
MMP-8 MMP-14 MMP-15 MMP-25
Prevents apoptosis Antiapoptotic
MMP-8 MMP-14 MMP-15 MMP-25
Prevents apoptosis Antiapoptotic
EGF is secreted in a paracrine fashion by platelets, macrophages and fibroblasts and acts on keratinocytes. Faulty location of the EGF receptor may be problematic in some nonhealing wounds. An in vitro study demonstrated the presence of EGFR in the cytoplasm, rather than the extracellular membrane, of cells in non,healing wounds, suggesting receptor downregulation within chronic wounds.42-44 TGF-α is another member of the EGF family that is secreted by keratinocytes, macrophages, fibroblasts, and lymphocytes, and works in an autocrine fashion.45,46 TGF-α induces expression of keratin 6 and keratin 16 (present in proliferating keratinocytes) and increases keratinocyte migration.47
TRANSFORMING GROWTH FACTOR-β FAMILY
TGF-β family members include TGF-β1 to TGF-β3, bone morphogenic proteins, and activins. TGF-β1, TGF-β2, and TGF-β3 promote the migration of fibroblasts and endothelial cells and deposition of extracellular matrices by fibroblasts during granulation tissue formation. TGF-β1 predominates in wound healing.48 Interestingly, TGF-β1 and TGF-β2 promote fibrosis and scar formation, whereas TGF-β3 has antifibrotic properties.49 TGF-β, produced by macrophages, fibroblasts, keratinocytes, and platelets, is important
in the wound healing processes of inflammation, angiogenesis, reepithelialization, and connective tissue regeneration.48,50 TGF-β1 facilitates recruitment of inflammatory cells, and promotes macrophage mediated debridement and granulation tissue formation. During reepithelialization, TGF-β1 shifts keratinocyte integrin expression toward a more migratory subtype.51 In the remodeling phase, TGF-β1 plays a major role in collagen production and inhibits collagen breakdown by inhibiting MMP-1, MMP-3, and MMP- 9, and promoting TIMP-1.52,53
TGF-β1 plays an important role in the formation of hypertrophic scars and keloids by overexpression of connective tissue growth factor.54 In fetal wounds, deceases in TGF-β1 transcription help explain the scarless healing that is seen.55
Activins are members of the TGF-β family produced by fibroblasts and keratinocytes and play role in reepithelization. Activin inhibits keratinocyte proliferation and induces terminal differentiation of keratinocytes. bone morphogenic proteins are another member of the family involved in keratinocyte differentiation. Overexpression of bone morphogenic protein-6 is associated with delayed healing.39,56
FIBROBLAST GROWTH FACTOR FAMILY
The 3 main members of the FGF family involved in wound healing are FGF-2, FGF-7, and FGF-10. FGFs are produced by keratinocytes, fibroblasts, smooth muscle cells, chondrocytes, endothelial cells, and mast cells.57 FGF receptors 1 to 4 are tyrosine kinase transmembrane proteins that work like EGFR.45
bFGF or FGF-2 plays a role in granulation tissue formation, reepithelialization, and tissue remodeling.58
FGF-2 regulates the synthesis of ECM components, and facilitates keratinocyte and fibroblast migration and collagenase formation. bFGF is decreased in chronic wounds.59
FGF-7 or keratinocyte growth factor-1 and FGF 10 or keratinocyte growth factor-2. FGF-7 and FGF-10 are secreted in a paracrine fashion, found only on keratinocytes, and have a role in reepithelialization. FGF-7 and FGF-10 increase transcription factors involved in detoxification of reactive oxygen species. FGF-7 is a strong mitogen of vascular endothelial cells and is important during neovascularization.60
PLATELET-DERIVED GROWTH FACTOR FAMILY
PDGFs, produced by platelets, macrophages, vascular endothelium, fibroblasts, and keratinocytes, bind to 2 different transmembrane tyrosine kinase receptors (α and β).61 Upon injury PDGF is released from degranulating platelets. PDGF, chemotactic for monocytes, macrophages, and neutrophils, is a mitogen for fibroblasts and smooth muscle cells in vitro. PDGF also stimulates macrophages to produce growth
22
factors such as TGF-β.62 PDGF plays an important role in blood vessel maturation and works synergistically with hypoxia to stimulate VEGF formation in vitro. However, PDGF angiogenic activity is less than FGF and VEGF.63 While not directly affecting keratinocyte migration, PDGF plays role in reepithelialization by in vitro production of insulin-like growth factor-1 and thrombospondin-1. PDGF also enhances the proliferation of fibroblasts and, in turn, the production of ECM. Recombinant human PDGF-BB (becaplermin) is the only FDA-approved drug for nonhealing neuropathic diabetic foot ulcers.64,65
VASCULAR ENDOTHELIAL GROWTH FACTOR FAMILY
Members of the VEGF family include VEGF-A to VEGF-E and placental growth factor.66 VEGF-A, which is secreted by keratinocytes, endothelial cells, fibroblast smooth muscle cells, platelets, neutrophils, and macrophages, binds to a tyrosine kinase surface receptor that is located on the endothelial surface of blood vessels, early in wound healing angiogenesis.67 Platelets release VEGF-A upon injury. Macrophages release VEGF-A directly but also release TNF-α, which induces VEGF-A expression on keratinocytes and fibroblasts. Hypoxia is a major stimulus for release of VEGF-A, and the VEGF-A gradient parallels the hypoxia gradient. VEGF-A is also involved mainly in the inflammatory stage of wound healing. Placental growth factor is expressed by keratinocytes and endothelial cells as a proangiogenic molecule. Placental growth factor stimulates cultured fibroblast migration and stimulates granulation tissue formation.68
GRANULOCYTE-MONOCYTE COLONY-STIMULATING FACTOR
GM-CSF has particular importance in the inflammatory stage of wound healing by increasing keratinocyte proliferation and enhancing reepithelialization. GM-CSF promotes proliferation and differentiation of neutrophils and hence increases host defenses.69
GM-CSF indirectly upregulates IL-6. In 2 studies on diabetic foot ulcers, in total 67 patients with infected diabetic foot ulcers were treated either with placebo or topical GM-CSF. Although GM-CSF improved neutrophil function and increased absolute neutrophil numbers, the addition of topical GM-CSF to standard care had no additional beneficial clinical effect.69
PROINFLAMMATORY CYTOKINES
Proinflammatory cytokines, including IL-1, IL-6, and TNF-α, are upregulated in the inflammatory phase of wound healing. IL-1 is produced by monocytes, macrophages, monocytes, and keratinocytes, with both paracrine and autocrine functions. IL-1 induces expression of keratin 6 and keratin 16 in migrating keratinocytes,
2707
22
and activates fibroblasts to secrete FGF-7.70 IL-6 is produced by neutrophils and monocytes with mitogenic and proliferative effect on keratinocytes and chemoattractive effects on neutrophils. TNF-α and IL-1β are increased in chronic wounds. The effect of exogenous TNF is dependent on the concentration and duration of exposure.70,71 TNF-α at low levels promotes healing by stimulating inflammation and increasing macrophage-produced growth factors, whereas at higher levels TNF-α impairs wound healing by suppressing production of ECM and TIMP and increasing MMPs. Chronic inflammation stimulates production of TNF-α and IL-1β that synergistically increases production of MMPs and suppress production of TIMPs.72
CHEMOKINES
Chemokines are a family of small cytokines or signaling proteins that attract neutrophils to the site. Macrophage chemoattractant protein-1 (or CCL2) is induced by keratinocytes and is chemoattractant for monocyte/ macrophages, T cells, and mast cells.73
Interferon-inducible protein 10 (or CXCL10) is another cytokine that negatively impacts wound healing. Interferon-inducible protein 10 inhibits migration of fibroblasts. IL-8 increases keratinocyte migration and proliferation, and is a chemoattractant of neutrophils.74
CLINICAL ISSUES IN WOUND HEALING
WOUND BED PREPARATION
WOUND BED PREPARATION
Although the majority of wounds heal in a timely manner, a proportion of wounds stall and do not follow the stages of healing. A nonhealing wound needs wound bed preparation to promote healing. The concept of wound bed preparation has been summarized using the pneumonic TIME: Tissue debridement, Infection/inflammation, Moisture balance, Epithelia edge tissue.21,32,75
Tissue debridement plays a key role in tissue preparation by removing nonviable tissue and pathogenic bacteria. Multiple techniques to debride exist, including surgical, enzymatic, biologic, mechanical, and autolytic techniques. Newer tools, such as lowfrequency ultrasound and hydrosurgery devices, have been developed.76 Table 149-3 lists techniques used for tissue debridement. Treating infection and inflammation implies assessment of the need for topical antiseptic and/or systemic antibiotic use to control infection and subsequent inflammation. Although inflammation is a physiologic process in wound healing, inappropriate inflammation can cause delayed healing. Infection may be classically seen as a host response, as in cellulitis. Bacteria may also delay healing through formation of biofilm, seen in 60% of chronic wounds. Biofilms are colonies
2708
DEBRIDEMENT TECHNIQUES ADVANTAGES DISADVANTAGES
Surgical, sharp (with scissors and/or scalpel)
High speed Selectivity Painful procedure, expensive Needs skilled professionals Contraindicated in ischemic tissue and bleeding disorders
Enzymatic (collagenase) Low pain Medium cost and low selectivity Some patients are allergic to the enzyme preparation
Biologic (larval therapy) High speed and high selectivity Medium pain
High cost Contraindicated in bleeding diathesis and deep, tunneling wounds
Mechanical (wet to dry dressings, hydrotherapy, ultrasonography)
Medium speed Painful Nonselective
Autolytic
Low pain Low speed Low selectivity Relatively high cost Contraindicated in
Autolytic (endogenous enzymes with moisture-retentive dressings)
Low pain Low speed Low selectivity Relatively high cost Contraindicated in infected wounds Risk of exposed bone/ tendon and friable skin
(endogenous enzymes with moisture-retentive dressings)
infected wounds Risk of exposed bone/
tendon and friable skin
of microorganisms that protect themselves through community living, in part by a surrounding glycocalyx (Fig. 149-5). Disruption of biofilms with debridement, with or without antimicrobial agents, helps alleviate persistent inflammation.77
The term antimicrobial includes disinfectants, antiseptics, and antibiotics. Antiseptics are broad spectrum with less risk of bacterial resistance. The difference between antibiotics and antiseptics is that antiseptics are nonspecific, while antibiotics work specifically on bacteria functions or processes such as disputing cell wall function but also can allow bacteria opportunity to mutate and develop resistance. As a result, topical antibiotics are not recommended for chronic wounds because of the risk of antibiotic resistance. A variety of modern antiseptic-impregnated dressings have been used to reduce microorganism numbers in the dressings and, in theory, on the wound surface. Their effect on biofilm organisms is less-well defined. Table 149-4 lists these antiseptics. Moisture imbalance involves the assessment and management of wound exudate. While acute wound fluid promotes cell growth and is rich in cytokines and growth factors, chronic wound fluid inhibits cell growth and contains high levels of proteases and proinflammatory cytokines. Thus, acute wounds
22
Biofilm formation In Vivo
(Porcine)
SEM
Wound bed Staphylococcus aureus
72 hours
benefit from contact with wound fluid, whereas chronic wounds do not. Moisture can hinder wound healing in other ways as well: extra moisture can damage periwound skin, and lack of moisture can hinder keratinocyte migration. The major dressing types (Table 149-5) include hydrogels, transparent polyurethane films, hydrocolloids, gelling fibers, alginates, foams, superabsorbents, and collagen products. In determining the most appropriate dressing for a particular wound, one must consider the need for absorption of exudate (foams and alginates), the need for additional moisture (hydrogels), and whether the wound and its epithelial edges
can tolerate the often subtle (but important) trauma that comes from removal of adhesive dressings such as films. Thin contact layers, consisting of different polymeric materials, some with perforations, allow wound fluid to escape and are useful in preventing tissue injury upon dressing changes. Edge assessment involves the assessment of nonadvancing wound edges and proper use of therapies to advance the wound edge.21 Keratinocytes from the edge of chronic wounds often abnormally express c-myc and treatments, such as debridement, which remove or reverse this cellular biomarker, can promote keratinocyte migration.78-80
ANTISEPTICS MAIN ADVANTAGES MAIN DISADVANTAGES
Iodine Based:
■Broad spectrum
Povidine-iodine 10%
■Cadexomer iodine
■Good penetration to biofilm
■Inadine
■Proinflammatory
Chlorhexidine Based:
■PHMB (polyhexamethylene biguanide)—foam, gauze
■Broad spectrum
■0.02% concentration use for wound irrigation
Silver-Based:
■Microcrystalline silver
■Toxic to granulation tissue in high concentration
■Risk of thyroid dysfunction
■Risk of contact dermatitis
■May damage cartilage/ear toxicity
Antiinflammatory, antibacterial, antifungal, antiviral Silver toxicity, argyria with silver sulfasalazine; silver sulfadiazine + silver nitrate sticks may produce pseudoeschar/delay healing
■Silver sulfadiazine cream
■Silver nitrate sticks
Honey-Based:
■Honey alginate
■Honey alginate
■Honey gel Antiinflammatory, best for hard adherent eschar Risk of botulism; may promote bacterial growth
Antiinflammatory, best for hard
■Honey gel
adherent eschar
Risk of botulism; may promote bacterial growth
2709
22
DRESSING CATEGORY INGREDIENTS FUNCTION COMMENTS
Hydrogels
■Polymers with high water content
■Provide moisture
Films
■Semipermeable adhesive sheets of elastic polyurethane
■Impermeable to water and bacteria
Hydrocolloids
■Hydrophilic colloid particles bound to polyurethane film
■Some composed of gelatin, pectin, and carboxy methylcellulose
Calcium alginates
■Sheets (wick laterally)
■Ropes (wick upward)
■From seaweed-kelp
■Needs secondary dressings
■Nonpainful
■Contraindicated in infected wounds
■Needs frequent dressing change
■Transparent
■Adherent (trauma when removed)
■Nonabsorbent
■Long wear time
■Nonabsorptive
■Autolytic debridement
■Trauma with removal
■Allergy to adhesives
■Smell
■Hemostatic
■Need secondary dressing
■Absorptive
■Autolytic debridement
Gelling fibers
■Sheets or ribbons
■Absorptive
Foams
■Polyurethane foam fluid exchange with partial fluid retention if variable pore size
■Needs secondary dressing
■Autolytic debridement
■Absorbent
■Bulky and may macerate surrounding skin
■Fiber technology/conducts moisture
■Absorbent
Superabsorbent dressings
■Bulky
■Diaper technology
■Bovine-derived collagen dressings
■Promote healing
■Cost
■Bovine-derived collagen dressings ■Promote healing
Collagen-based dressings
Collagen-based
dressings
SKIN GRAFTS
SKIN GRAFTS
Skin grafts are categorized by the amount of tissue being grafting. For example, split-thickness grafts include a portion of dermis and full-thickness grafts contain the entire dermis. The likelihood of the survival and whether wound contracture is reduced depends on the amount of dermis in the graft. Split-thickness skin grafts can survive in areas with less vascularity but also are less likely to prevent wound contracture, whereas full-thickness skin grafts require better vascularity for survival and but can better prevent contracture. While skin grafting is centuries old, modern grafting is thought to have begun with the first skin autotransplant done in 1869 by Reverdin and then in 1929 by Brown and colleagues who introduced the technique of the splitthickness skin graft.81 The healing of a skin graft, however, is different from the description provided earlier of the events after acute injury. One distinguishing feature of skin graft “take” or healing is the dependence of the graft on the recipient wound bed for revascularization, which requires several unique physiologic events. Much of the remainder of skin graft healing involves events in common with the normal wound healing process. Infiltration by fibroblasts in the graft occurs 3 to 5 days after grafting, followed by a progressive increase in both graft and recipient fibroblasts within the graft.82,83 Although graft “take” allows for donor tissue to replace missing tissue in the recipient wound, skin grafts may also stimulate wound healing of the recipient site, and this ability can be augmented. For
2710
■Cost
■Reduce matrix metalloproteinases
■Reduce matrix
metalloproteinases
example “prewounding” of the donor site skin prior to grafting enhances the graft’s ability to stimulate healing.83,84 Ki67 antibody and β1-integrin expression after grafting has been noted, as has production of stimulatory growth factors and cytokines, implying that healing stimuli were provided by the grafts.85
SKIN SUBSTITUTES
SKIN SUBSTITUTES
Skin substitutes are divided into 2 main groups of cellular and acellular matrix products (Table 149-6).86
CELLULAR PRODUCTS
The cellular skin substitute products with best available evidence are the bilayered living cellular construct (BLCC), Apligraf (Organogenesis, Canton, MA) and cellular dermal matrix, Dermagraft (Organogenesis, Canton, MA). BLCC is a tissue-engineered cellular matrix composed of bovine Type I collage with neonatal foreskin fibroblasts for dermal component and human neonatal keratinocytes for epidermis.87 BLCC has FDA approval for venous leg ulcers (VLUs) greater than 4 weeks’ duration and for full-thickness diabetic foot ulcers present for longer than 3 weeks. The evidence supports the safety and efficacy of up to 5 applications of BLCC. An example of its efficacy is 47% of chronic, hard-to-heal VLUs present longer than 1 year treated with BLCC healed after 24 weeks compared to 19% in the group with compression alone.88
22
NAMES ADVANTAGE FDA APPROVAL
Cellular Matrices:
Bilayered living cellular construct (Apligraf, Organogenesis, Canton, MA) Dermal part: Bovine Type I collagen with human neonatal foreskin fibroblasts Epidermal part: keratinocytes
Noninfected partial- and full-thickness venous leg ulcers, >1 month duration Full-thickness diabetic foot ulcers, >3 weeks’ duration
Cellular dermal matrix (Dermagraft, Organogenesis, Canton, MA) Human neonatal foreskin fibroblasts cultured onto a bioresorbable glycolic acid scaffold (polyglactin 910)
Dehydrated human amnion/chorion membrane (DHACM) (Epifix, MiMedx Group Inc., Marietta, GA)
Full-thickness diabetic foot ulcers >6 weeks’ duration that do not involve tendon, muscle, joint capsule, or bones
DHACM is composed of a single layer of epithelial cells, a basement membrane, and an avascular connective tissue matrix
DHACM is composed of a single layer of epithelial cells, a basement membrane, and an avascular connective tissue matrix
Cryopreserved placental membrane (Grafix, Osiris Therapeutics, Inc., Columbia, MD) Human viable wound matrix provides the wound with mesenchymal stem cells, neonatal fibroblasts, epithelial cells, growth factors, and angiogenic factors
Acellular Matrices:
Dermal regeneration matrix (Integra Dermal Regeneration Template, Integra, Life Sciences, Plainsboro, NJ)
Human viable wound matrix provides the wound with mesenchymal stem cells, neonatal fibroblasts, epithelial cells, growth factors, and angiogenic factors
Composed of a crosslinked bovine tendon collagen and glycosaminoglycan dermal equivalent, and a semipermeable polysiloxane (silicone) epidermal equivalent
FDA-approved device (510[k] for diabetic foot ulcers)
Porcine small intestinal submucosa (Cook Biotech, West Lafayette, Indiana) Derived from small intestinal submucosa of porcine; 3-dimensional extracellular matrix that acts as a scaffold to allow for cellular migration, formation of granulation tissue, and vascularization of the wound
FDA-approved 510(k)-cleared medical device
Cadaveric allograft (AlloDerm Regenerative Tissue Matrix [RTM], LifeCell, , Branchburg, NJ) Cadaveric human skin that has been processed to remove the epidermis and cells that lead to tissue rejection and graft failure
Poly-N-acetyl glucosamine–derived membrane
Regulated by the FDA as human tissue for transplantation
Composed of poly-N-acetyl glucosamine short-
Poly-N-acetyl glucosamine–derived membrane (Talymed, Marine Polymer Technologies Inc., Danvers, MA)
FDA approved—510(k)
Composed of poly-N-acetyl glucosamine shortened fibers that are derived from microalgae FDA approved—510(k)
(Talymed, Marine Polymer Technologies Inc., Danvers, MA)
ened fibers that are derived from microalgae
Cellular dermal matrix is composed of human neonatal foreskin fibroblasts cultured onto a bioabsorbable glycolic acid scaffold. The fibroblasts secrete collagen, matrix proteins, growth factors, and cytokines. It has FDA approval for diabetic foot ulcers of longer than 6 weeks’ duration. Human placental products also are used to speed healing of chronic wounds. The 2 supported by evidence (albeit less robust) include dehydrated human amnion/chorion membrane (Epifix, MiMedx, Marietta, GA) and cryopreserved placental membrane (Grafix, Osiris Therapeutics Inc.). Epifix is composed of a single layer of epithelial cells, a basement membrane, and a connective tissue matrix. Grafix is composed of placental membrane, a source of mesenchymal stem cells, neonatal fibroblasts, epithelial cells, growth factors, and angiogenic cells.89-92
ACELLULAR PRODUCTS
Acellular products function as a scaffold for cellular migration, proliferation, and matrix formation. Examples of acellular products include dermal
regeneration matrix, porcine small intestinal submucosa, cadaveric allograft, and poly-N-acetyl glucosamine.86
INTEGRA Dermal Regeneration Template (Integra LifeSciences Corp.) is a bilayered acellular matrix composed of crosslinked bovine tendon collagen, a glycosaminoglycan dermal equivalent, and a semipermeable polysiloxane epidermal equivalent. It is approved for burns and diabetic foot ulcers. In a recent study on diabetic foot ulcer patients, 51% of patients on Dermal Regeneration Template achieved complete healing, compared to 32% of controls.93,94 Porcine small intestine submucosa (Oasis, Smith, & Nephew) is a scaffold for cellular migration, granulation tissue formation and neovascularization. The evidence supports the successful use of small intestine submucosa in patients with diabetic foot ulcers and VLUs.95 Cadaveric allograft is made of cadaveric human skin. It is indicated for tissue repair in abdominal wall and breast reconstruction.96 Poly-N-acetyl glucosamine (Talymed) is derived from microalgae and has FDA approval for a variety of wounds. Poly-N-acetyl glucosamine has also antibacterial properties.97
2711
22
STEM CELL THERAPY
STEM CELL THERAPY
The use of stem cells in the management of wounds aims to replace the wound resident cells with new cells with the potential to respond to wound healing process signals. Numerous animal studies and a small number of pilot studies in human have shown that bone marrow mesenchymal cells can promote wound healing.98,99 In 2003, freshly applied autologous bone marrow aspirate and cultured bone marrow cells helped 3 wounds heal.100,101 In animal models, the use of stem cells is associated with healing and increase in tensile strength. In addition to bone marrow–derived cells, other sources of stem cells, such as fat and hair follicles, may be beneficial.98
However, most studies of adult stem cell therapy for human wounds have used cultured bone marrow– derived mesenchymal stem cells.102 The improvement of wounds with adult stem cells may be a result of either integration of the stem cells or their paracrine effects.103 Topically applied autologous mesenchymal stem cells accelerate the healing of human and murine wounds.104 The first randomized, controlled trial reported the use of bone marrow mesenchymal stem cell application via IM and subcutaneous injection to chronic nonhealing wounds with success compared to standard care.105
CHRONIC WOUNDS AND IMPAIRED HEALING
CHRONIC WOUNDS AND
IMPAIRED HEALING
Acute wounds, such as those created by surgery or by trauma, have a predictable time-frame for healing and generally heal quite readily when not interrupted. Impaired healing in chronic wounds may be a consequence of many factors. Some chronic wounds are the result of ischemia, pressure, and infection or a combination, thereof.26
There is still considerable controversy whether hyperglycemia itself plays a pathophysiologic role in the development of ulcers in patients with diabetes mellitus, although neutrophil function is impaired in this setting, and the propensity to infection is enhanced in the diabetic state.26 Importantly, the notion of “small vessel disease” in diabetes mellitus has not been shown to be an obstructive phenomenon. Revascularization of the diabetic foot is now viewed as standard care in the presence of large vessel disease and good run-off circulation. Perhaps the best example of truly impaired healing, not related to undue pressure and poor arterial supply, is venous ulceration. The underlying abnormality in the development of venous ulcers is the presence of sustained ambulatory venous pressure, also known as venous hypertension, which refers to the inability of venous pressure in the leg and feet to decrease in response to exercise.106 It should also be recognized that the tissue surrounding chronic wounds is not normal and has been altered by the primary pathogenic
2712
mechanisms or inability to heal readily. Clinically, the best example of this is the intense fibrosis surrounding venous ulcers, as seen in lipodermatosclerosis.107,108
Lipodermatosclerosis is a risk factor for ulceration, and venous ulcers surrounded by lipodermatosclerosis are more difficult to heal.109,110
Evidence suggests an alteration of the cellular makeup of wounds that do not heal. Fibroblasts derived from venous ulcers are unresponsive to certain selected cytokines and growth factors.111 For example, venous ulcer fibroblasts are unresponsive to the action of TGF-β1 and PDGF.111,112 The lack of response to stimuli such as TGF-β1 may be because of decreased expression of Type II TGF-β receptors. This receptor abnormality also leads to decreased phosphorylation of key TGF-β signaling proteins, including Smad2, Smad3, and mitogen-activated protein kinases.113 Cells in diabetic ulcers are altered, such that chronic wounds are said to be “stuck” in a certain phases of the repair process.114 An association has been reported between some of these cellular alterations and the inability to heal.115,116
AGE-RELATED CHANGES IN WOUND HEALING
AGE-RELATED CHANGES IN
WOUND HEALING
The population is aging, and older adults are more prone to develop all type of wounds, including VLUs, arterial ulcers, and pressure ulcers. For both acute and chronic wounds, aging is associated with delayed healing. The healing response by ECM changes throughout life.117 Overexpression of MMPs has been shown in elderly skin.117 The vasoregulation in aged skin includes fewer progenitor cells, impaired perfusion and changes in temperature regulation. Ageassociated aberrations in macrophage function delay vascularization, collagen formation, and remodeling. Mitochondrial dysfunction and lower levels of antioxidants also are associated with aging. Comorbidities and polypharmacy may also factor into delayed healing in the elderly population.118-120
BASIC STANDARDS OF WOUND CARE
BASIC STANDARDS OF
WOUND CARE
Reversing or treating the underlying cause of impaired healing is the focus of wound care treatment. Treatment relies in part on wound etiology. A thorough history and examination, along with adjunctive diagnostic tests, such as wound biopsy, vascular studies, imaging, tissue culture, and laboratory analysis may help with diagnosis.121,122 The most common lower extremity ulcers are venous, diabetic, and arterial ulcers. Chronic wounds are common. VLUs have a 2% prevalence in developed countries, and diabetic foot ulcers occur in 1 in 4 patients with diabetes mellitus over their lifetime.17,123,124
Using VLUs as an example, the fundamental of treatment is compression therapy with adjunctive medical and surgical therapies.109,110,125,126 With regard to medical therapy, pentoxifylline has been tested in several large randomized trials for its ability to accelerate the healing of venous ulcers. The results have varied, and it may be that a high dose of pentoxifylline, 800 mg 3 times a day, is more effective than 400 mg 3 times a day.127 Whether the use of pentoxifylline should be considered standard therapy for venous ulcers is unclear at the moment. The anabolic steroid stanozolol has been effective in diminishing the induration of lipodermatosclerosis, and in the acute and painful phase of lipodermatosclerosis, when compression bandages and stockings are too painful to use.128
Danazol may be a useful substitute for stanozolol if it is not available. Recent studies show an effect of statins in the healing of VLUs (and possibly diabetic foot ulcers).129,130 The only known medical approach for decreasing recurrence of venous ulcers seems to be graded elastic stockings, with a pressure at the ankle in the range of 40 mm Hg along. Surgical therapy is an adjunct, if indicated. Stockings should be considered a lifelong therapy to help prevent ulcer recurrence and the other manifestations of venous disease.
PREDICTING WOUND CLOSURE
PREDICTING WOUND
CLOSURE
Several recent studies now allow the prediction of whether a wound will heal in a timely fashion from simple observation in the first 3 to 4 weeks of therapy. The methods used to predict wound closure range from simple measurements of wound size (width and length) and change in wound area, to computerized planimetric analysis and assessment of migration of the wound edge.131 In a study of 56,488 wounds, it was shown that a percent change of approximately 30% at 4 weeks could predict wound closure with a sensitivity of 0.67, a specificity of 0.69, and had a positive and negative predictive value of 0.80 and 0.52, respectively.132
In practical terms, the appearance of the wound edge is important. Steep edges imply no progress of the wound, while the edges of healing wounds become less steep and begin to migrate toward the center. The implications of the ability to predict closure are very important. By 4 weeks, the clinician should be able to determine whether the current therapy should be continued or whether a change is required, including a complete reassessment of the clinical situation. The prognostic value of the healing rate by 4 weeks of therapy has been confirmed.132,133
CONCLUSIONS
Wound healing is a complex process of overlapping phases of inflammation, proliferation and remodeling. The burden of wounds on millions of people is globally underappreciated. There are still challenges,
22
in terms of improving the fundamentals of care in limited-resource countries, as well as research gaps in smart biologic dressings, bioengineered skin, and stem cell therapy. We need continued and increased understanding of the science involved. It is also possible that lessons learned from failure to heal, as in chronic wounds, will provide valuable lessons for the general principles of surgical and acute wound healing.
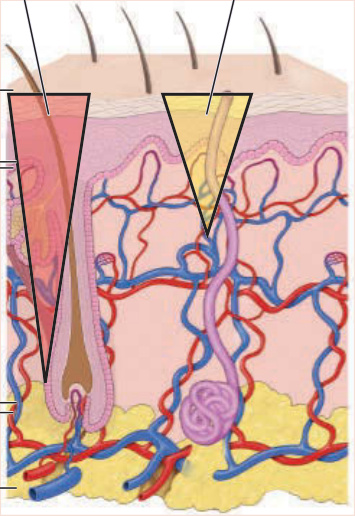
Figure 149-1 Diagrammatic representation of the skin, with 2 inverted triangles representing either a splitthickness or full-thickness wound. Extending the injury below the reservoir of keratinocytes present in skin appendages (full-thickness wound) removes the capability of the keratinocytes to populate the defect from within the wound bed, which means healing has to occur from the wound edges and more scarring takes place.
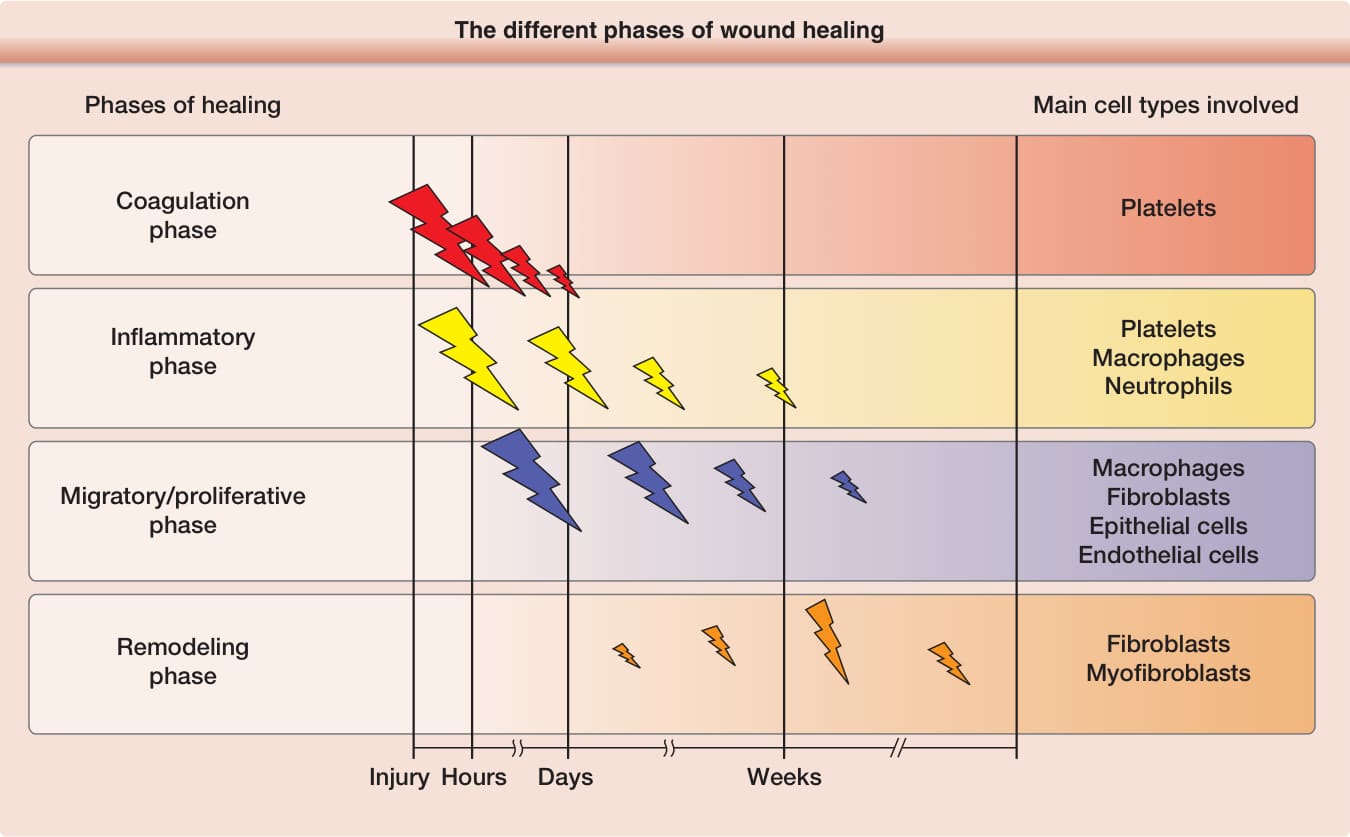
Figure 149-2 Schematic, different of the different phases of wound healing.
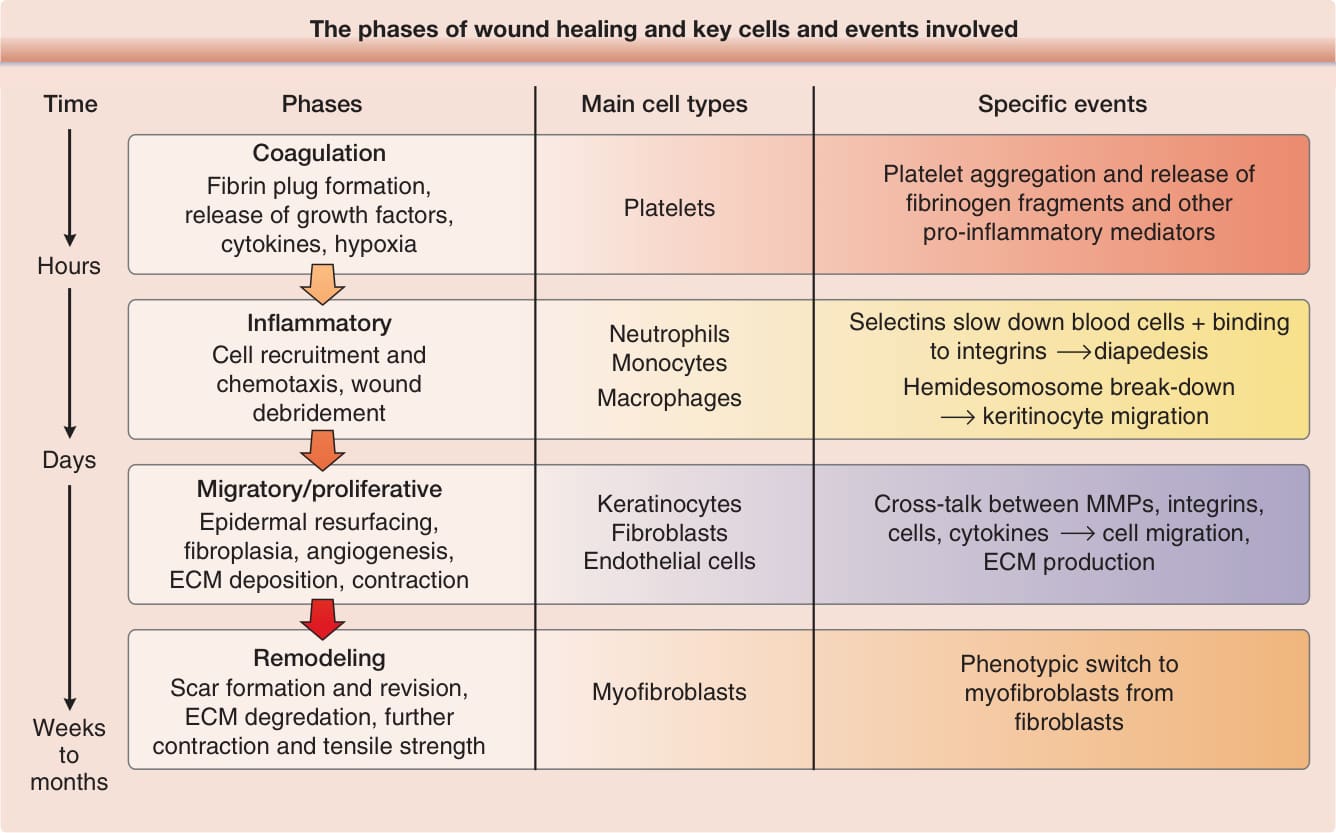
Figure 149-3 The phases of wound healing, and key cells and events involved. (Reprinted from Falanga V. Wound healing and its impairment in the diabetic foot. The Lancet. 2005;366:1736-1743; with permission. Copyright © Elsevier.)
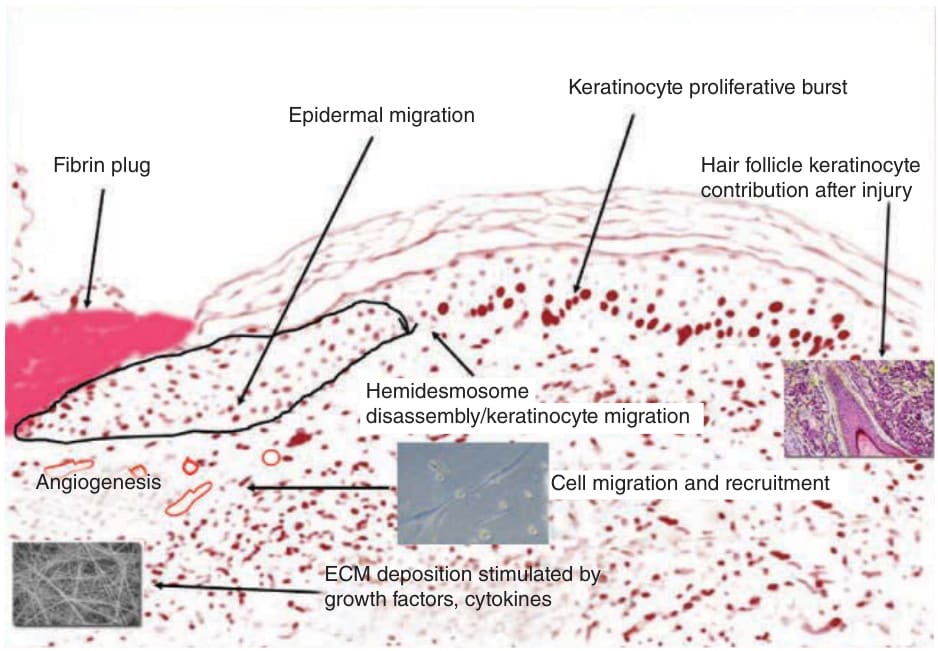
Figure 149-4 Schematic, using a modified photomicrograph section, of the events taking place shortly after injury, including formation of a fibrin plug, epidermal migration, and extracellular matrix deposition.
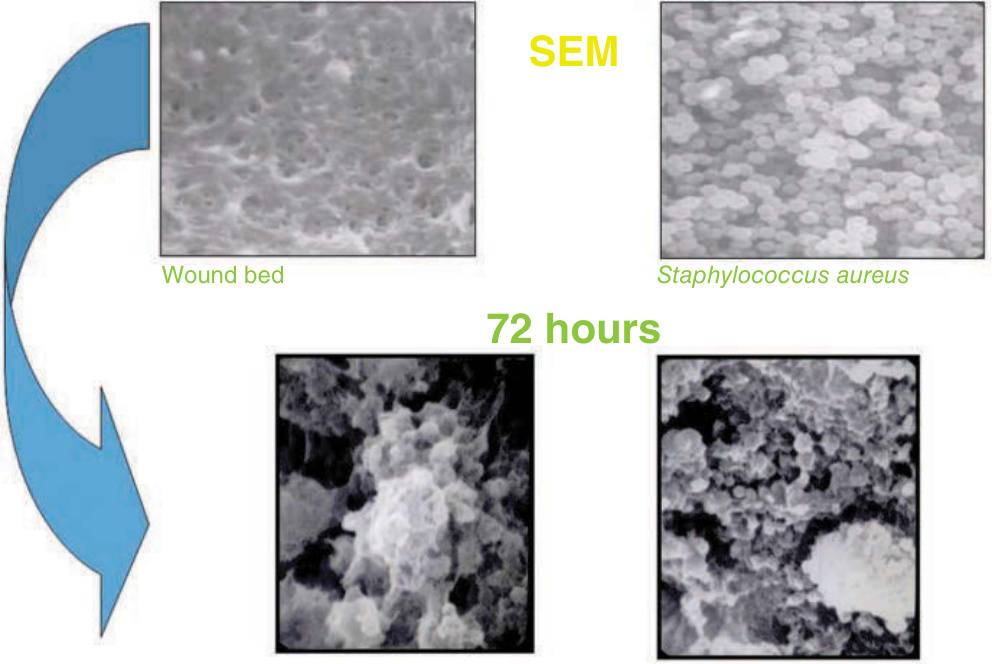
Figure 149-5 Biofilm formation. Colonies of microorganisms with a surrounding glycocalyx. SEM, scanning electron micrograph.
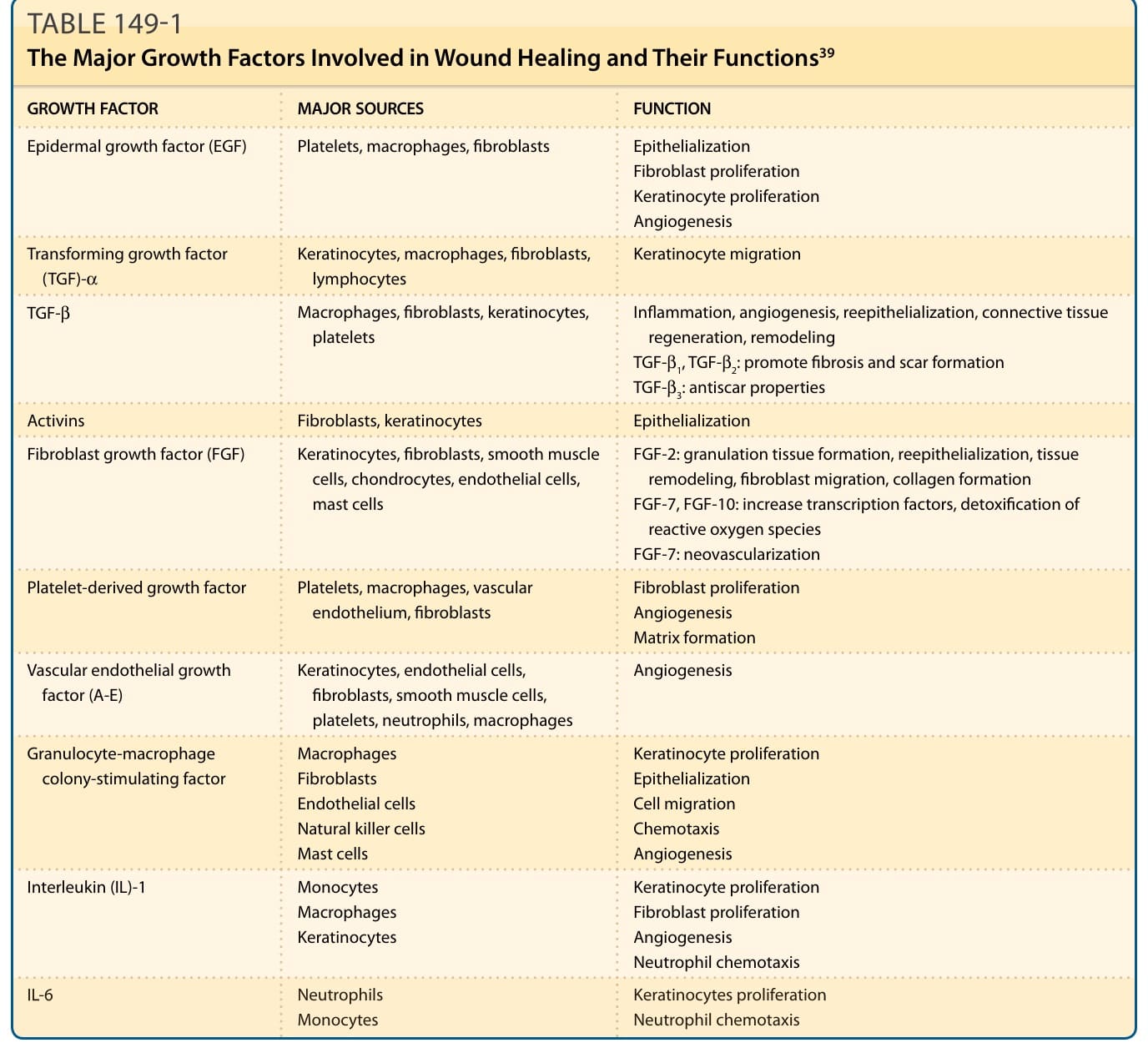
TABLE 149-1 The Major Growth Factors Involved in Wound Healing and Their Functions39
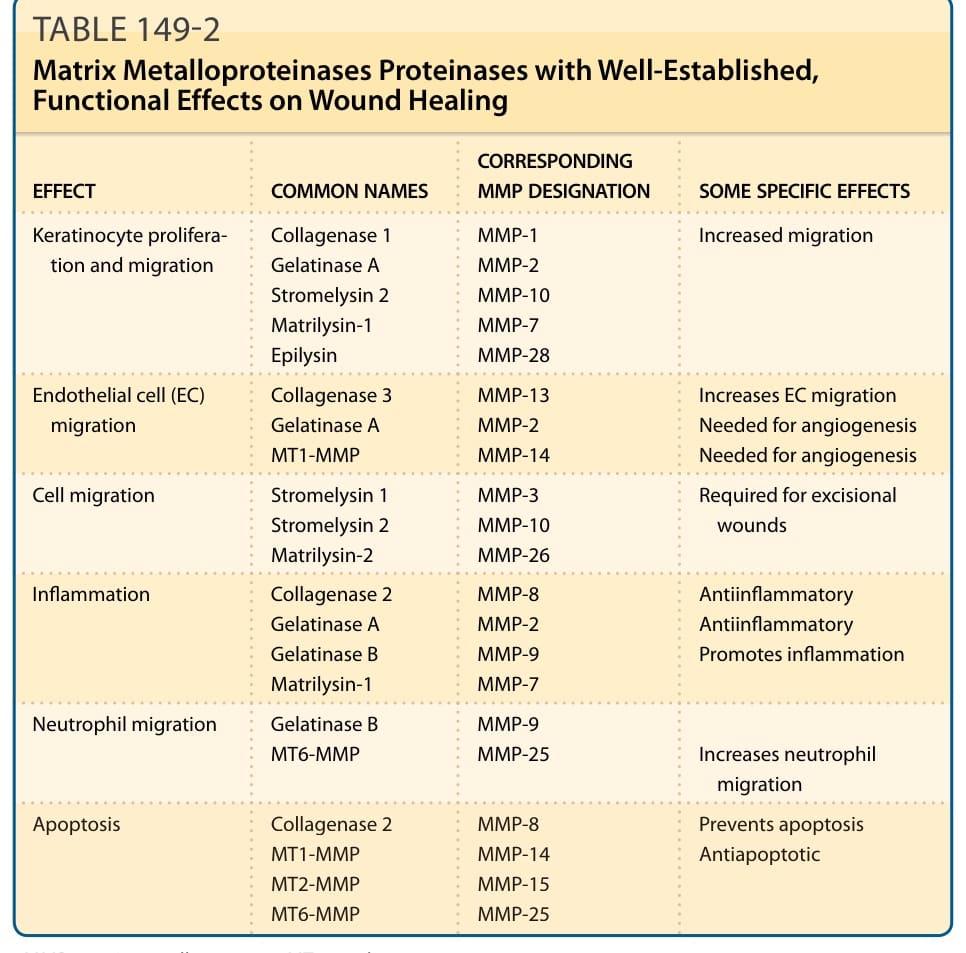
TABLE 149-2 Matrix Metalloproteinases Proteinases with Well-Established, Functional Effects on Wound Healing
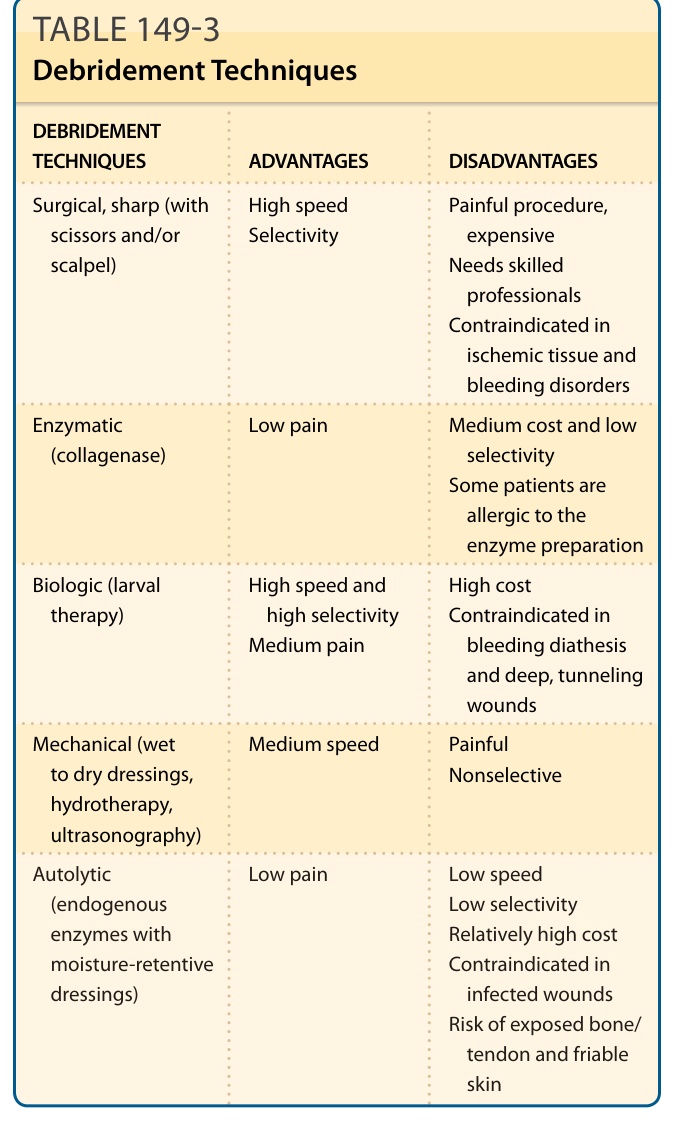
TABLE 149-3 Debridement Techniques
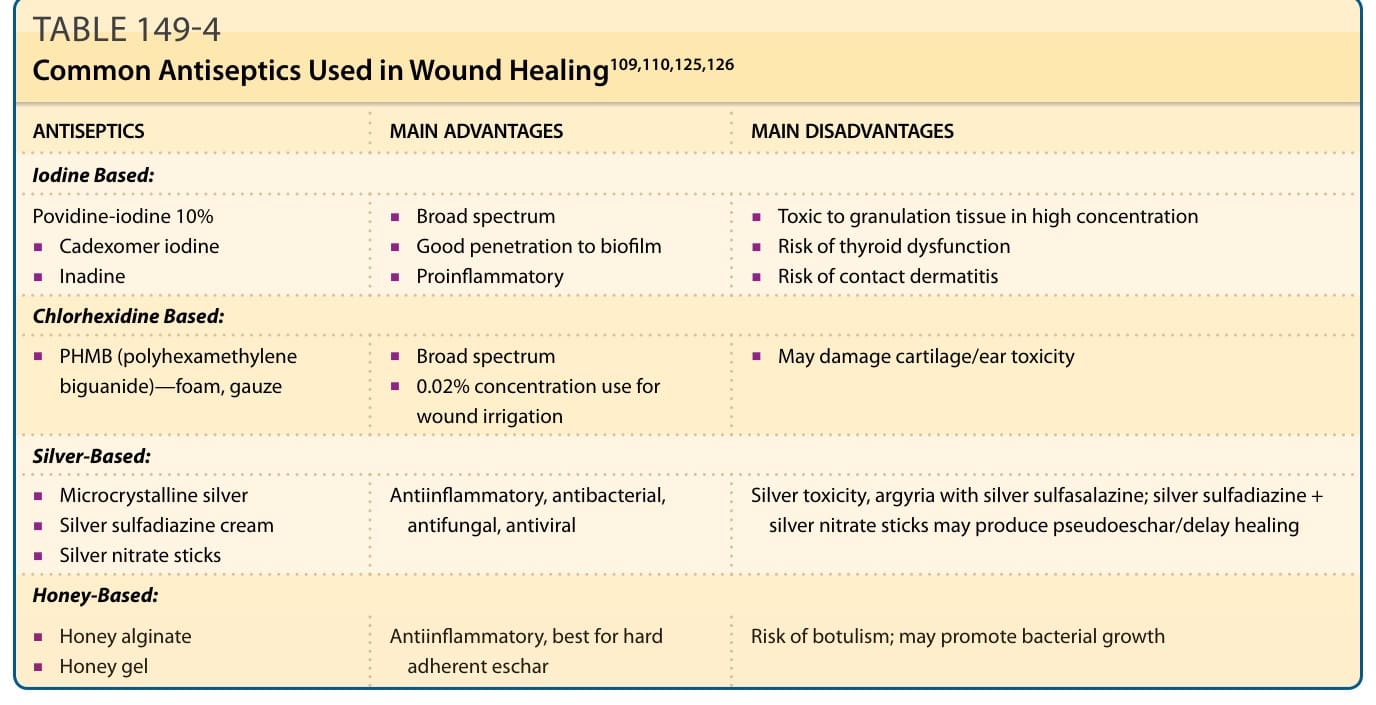
TABLE 149-4 Common Antiseptics Used in Wound Healing109,110,125,126
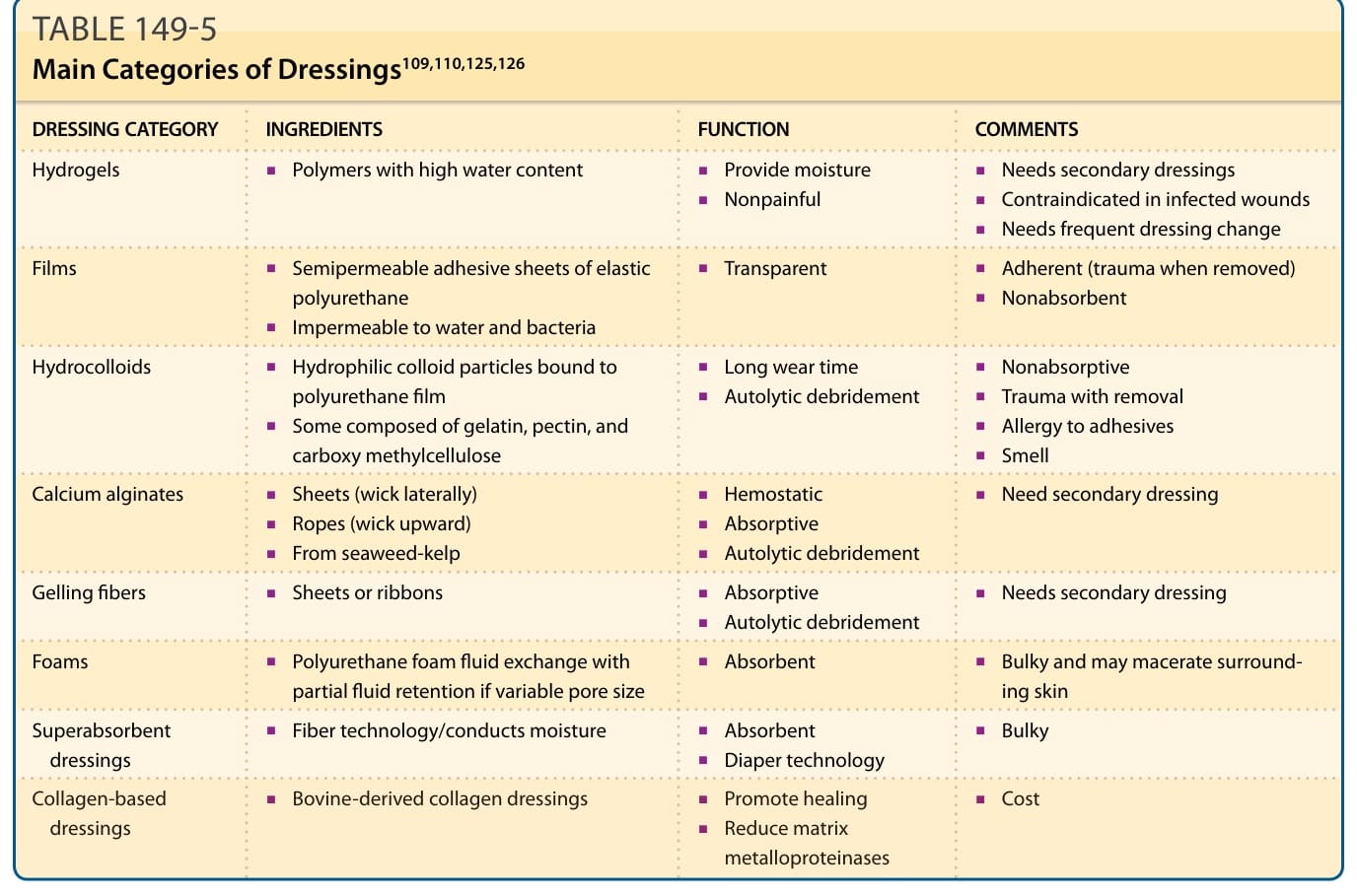
TABLE 149-5 Main Categories of Dressings109,110,125,126
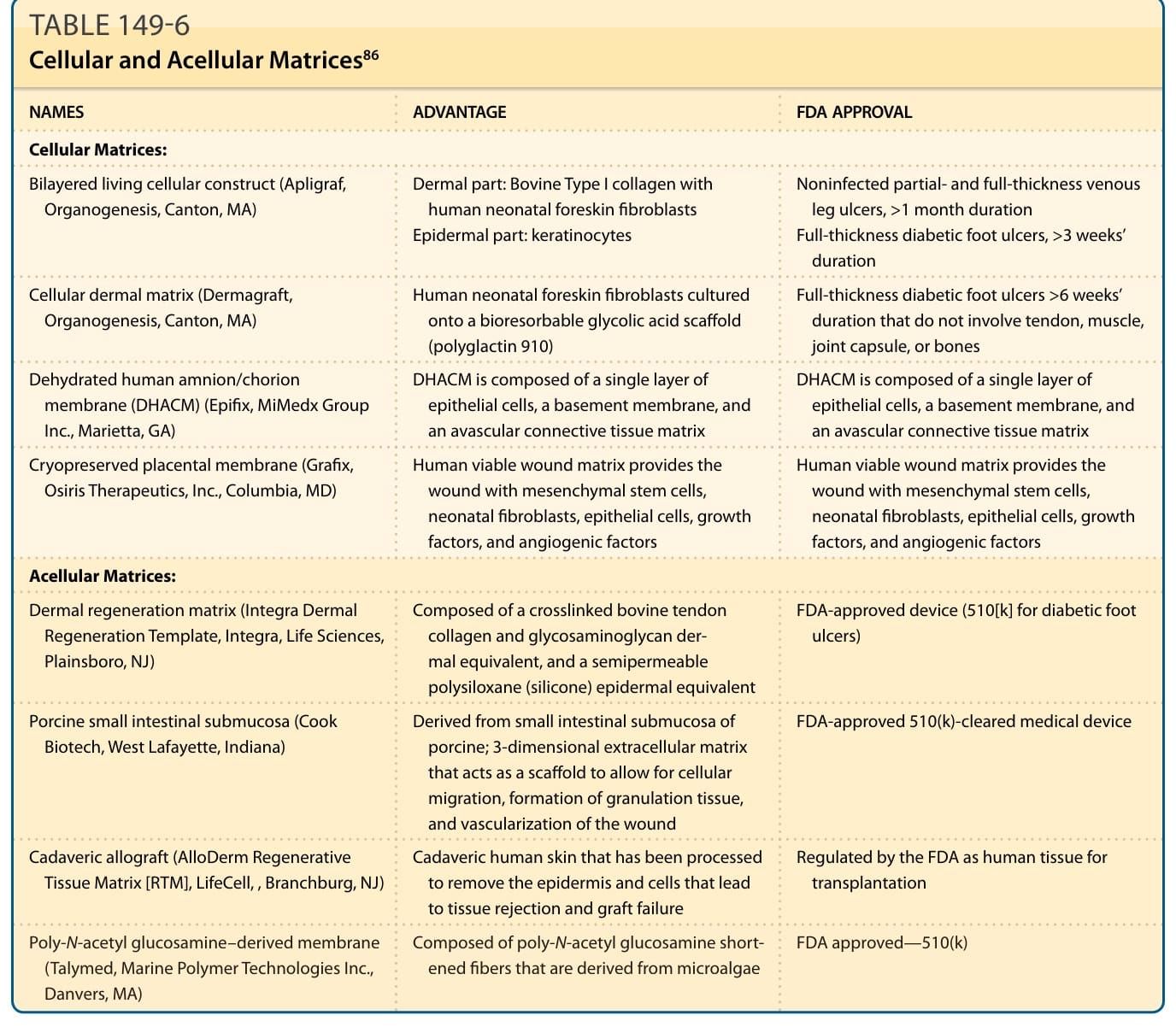
TABLE 149-6 Cellular and Acellular Matrices86