Kawasaki Disease
22
AT-A-GLANCE
■ Kawasaki disease (KD) is a multisystem inflammatory process of unknown but suspected infectious etiology.
■ Highest incidence is in Asian children; 1 in 80 Japanese children develops KD by age 5 years.
■ KD is the most common cause of acquired heart disease in children in developed nations.
■ KD affects all blood vessels in the body, but primarily damages medium-sized muscular arteries such as the coronary arteries.
■ Major symptoms are prolonged high fever, conjunctival injection, oral mucosal changes such as red lips and pharynx and strawberry tongue, redness and swelling of the hands and feet, erythematous polymorphic rash, and cervical lymphadenopathy.
■ Inflammation in the coronary arteries can lead to aneurysms with subsequent myocardial infarction, aneurysm rupture, and sudden death.
■ Treatment with intravenous immunoglobulin (IVIG) and aspirin, when given in the first 10 days of fever, reduces the prevalence of coronary artery abnormalities from 25% in those treated with aspirin alone, to 5% in those who receive IVIG with aspirin.
■ Long-term complications are confined to the heart and vascular tree, primarily thrombosis and stenosis of the major coronary arteries with myocardial ischemia.
Kawasaki disease (KD), the leading cause of acquired heart disease in children in developed nations, is a multisystem inflammatory illness that particularly affects blood vessels, especially the coronary arteries. Approximately 25% of untreated children develop coronary artery abnormalities, including dilation and aneurysms that can lead to myocardial infarction and sudden death.1,2 The etiology is unknown, but clinical and epidemiologic data support an infectious cause. In KD, an intense inflammatory cell response develops in a wide array of organs and tissues3; in medium-sized arteries such as the coronary arteries, this response can damage collagen and elastin fibers in the vessel walls and lead to loss of their normal structural integrity with resultant ballooning or aneurysm formation. Despite a limited understanding of KD pathogenesis, a very effective therapy exists in the form of intravenous immunoglobulin (IVIG) with aspirin; when given in the first 10 days of fever, this therapy reduces the
prevalence of coronary artery abnormalities from 25% in untreated patients to 5% in those who receive the therapy.4 Because the etiology is unknown, no diagnostic test exists, and the diagnosis is made clinically. Classic KD is diagnosed in a patient with prolonged fever and 4 of 5 other clinical features. However, incomplete forms of illness, in which a child manifests prolonged fever with fewer than 4 other clinical features of the illness and subsequently develops coronary artery abnormalities, are well-recognized. The existence of these incomplete forms of illness results in a major diagnostic dilemma for physicians in establishing the diagnosis accurately in children with prolonged fever of uncertain cause.
HISTORICAL PERSPECTIVE
KD is named for Dr. Tomisaku Kawasaki, a Japanese pediatrician who first recognized the clinical features of the illness. He described 50 cases of a new illness in 1967 in the Japanese-language literature that he termed mucocutaneous lymph node syndrome.5 It was not until later that some of the children with this newly described illness experienced sudden death; autopsy revealed myocardial infarction from thrombosis of coronary artery aneurysms. Prior to Dr. Kawasaki’s description of the clinical features, KD was recognized only by pathologists at autopsy, who called the disease infantile periarteritis nodosa.6 Dr. Kawasaki described the illness in the English-language literature in 1974; this report was closely followed by a description of the same illness, observed independently in the early 1970s in Hawaii by Dr. Marian Melish and colleagues.7,8
Since that time, it has become clear that although the attack rate of KD is highest in Asian, particularly Japanese, Korean, and Chinese children, all racial and ethnic groups around the world are affected by the illness.
EPIDEMIOLOGY
KD is predominantly an illness of young children, with 80% of cases occurring in children ages 6 months to 5 years.9,10 However, infants younger than 6 months of age can be affected, often manifest incomplete forms of the illness, and can have particularly severe KD.11,12
Similarly, KD can occur in older children and teenagers, in whom the diagnosis is often delayed, and who may also have more-severe KD with a higher prevalence of coronary artery abnormalities.11-13 Therefore, the diagnosis must be considered in all pediatric age groups. Boys are more commonly affected than girls at a ratio of 3:2. The incidence of KD is approximately 10-fold higher in Japanese than in white children.9,10
Approximately 1 in 80 Japanese children develop KD by the age of 5 years; the peak age of illness is 9 to 11 months of age in both Japan and the United States.9,10 The higher attack rate in Japanese children persists in those who adopt a Western diet and lifestyle, and is likely related to a genetic predisposition to KD among Asian children.14 The risk of KD in siblings is 10-fold higher than in the general population, and the incidence of KD in children born to parents who had KD is twice as high as in the general population.15,16 Recurrence is rare, occurring in approximately 3% of cases in Japan.10
Many epidemiologic features of KD suggest an infectious agent is the cause. Among these are the welldescribed epidemics of illness14,17-19 and the geographic wave-like spread of illness during an epidemic, compatible with spread of an infectious agent.19 Cases in the United States are more common in the winter and spring.9
CLINICAL FEATURES
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
A generalized exanthem is commonly observed in KD, is most pronounced on the trunk and extremities, and generally takes 1 of 3 forms: morbilliform (Fig. 142-1A), targetoid (Fig. 142-1B), or scarlatiniform (diffuse erythema, Fig. 142-1C). Bullae, vesicles, and ulcerative lesions are not observed, but a fine micropustular rash, especially on the extensor surfaces, occasionally occurs. The rash may be pruritic. In the acute febrile phase of illness, groin erythema and desquamation are commonly observed (Fig. 142-2), and can be mistaken for candidal diaper dermatitis or even a staphylococcal scalded skin syndrome. The skin changes in the groin can be seen both in children in diapers and toilettrained children. Classic periungual desquamation of the fingers and toes does not begin until the second to third week after fever begins, and can progress to involve the entire hand and foot (Fig. 142-3); treatment should be administered well before its appearance. In the third to sixth week after illness, transverse lines across the fingernails (Beau lines) are often apparent. These grow out with the nail. In countries where bacille Calmette-Guérin vaccine is routinely administered, such as in Japan, a common finding in children with KD is erythema and swelling at the site of bacille Calmette-Guérin vaccine administration; the mechanism is unknown but the process resolves with treatment of KD. Although KD results in a vasculitis affecting all arteries and veins in the body, blood vessels in the skin are not prominently affected, and skin biopsy is not useful for diagnosis because pathologic findings are nonspecific.
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
KD should be considered in the differential diagnosis of any child with prolonged fever without other
22
A
B
C
2581
22
explanation. In KD, all clinical features may not be present simultaneously. Therefore, it is important to query parents and physicians who saw the patient during the course of a prolonged febrile illness as to the presence of the other 5 clinical features of the illness: conjunctival injection, oral mucosal changes, changes of the hands and feet, rash, and cervical adenopathy. Children with KD often have significant enough swelling and discomfort of the hands and feet that they will refuse to pick up objects or to walk (Fig. 142-4). This is not commonly observed in children with most other illnesses in the differential diagnosis of KD, and can provide an important clue to the diagnosis. Similarly, extreme irritability is common in KD, and not as common in most other illnesses in the differential diagnosis. Without specific therapy, fever in KD is daily, high spiking, intermittent, and lasts for 1 to 2 weeks. The
2582
illness is often divided into 3 stages: the acute febrile phase, the subacute phase (that begins when fever resolves and continues until all clinical features have normalized), and the convalescent phase (that follows the subacute phase and continues until the erythrocyte sedimentation rate [ESR] normalizes, usually at 6 to 8 weeks after the onset of fever). Conjunctival injection in KD is bilateral and nonexudative. There may be limbal sparing (Fig. 142-5). Photophobia is a common accompanying feature. Oral findings include red, swollen, dry, cracked lips that may bleed (Fig. 142-6), a “strawberry” tongue, and erythema of the mouth and throat. Oral ulcers are not a feature of KD. Palmar and plantar erythema is a common feature, and there can be an abrupt transition from marked erythema to normal skin at the wrists and ankles. The hands and feet can be edematous and painful. Cervical adenopathy is the least commonly observed clinical feature, occurring in approximately 75% of children with classic KD, but can be the most prominent feature in a subset of patients who are often treated with multiple different courses of antibiotic therapy without improvement before the correct diagnosis is made.20 Cervical adenopathy is usually
unilateral, may or may not be associated with superficial erythema and/or tenderness to palpation, and is nonfluctuant. Because KD is a multisystem inflammatory process, many organs and tissues are involved in the inflammatory process, leading to a variety of associated clinical features (Table 142-1). In particular, arthritis can occur during the acute febrile phase, involving the small interphalangeal joints and larger
Cardiovascular
■Coronary artery aneurysms
■Myocarditis
■Pericardial effusion
■Aneurysms of other medium-sized arteries (uncommon)
■Valvular disease (rare)
■Peripheral gangrene (rare)
Respiratory
■Pneumonitis: interstitial or peribronchial infiltrates on chest X-ray, usually without respiratory distress
■Pulmonary nodules (rare)
Gastrointestinal
■Hepatitis
■Obstructive jaundice
■Gallbladder hydrops
■Diarrhea
Musculoskeletal
■Arthritis
Genitourinary
■Urethritis
■Hydrocele
Neurologic
■Marked irritability
■Aseptic meningitis
■Facial palsy (uncommon)
■Sensorineural hearing loss (uncommon)
Other
Other
■Anterior uveitis
■Anterior uveitis
■Erythema and induration at the site of a bacille Calmette-Guérin (BCG) vaccine
■Erythema and induration at the site of a bacille Calmette-Guérin
(BCG) vaccine
22
joints, or may occur during the subacute phase of illness, usually involving the larger joints such as the knees and ankles. Aseptic meningitis is a common finding in patients who undergo lumbar puncture.
COMPLICATIONS
COMPLICATIONS
As noted above, approximately 25% of untreated children develop coronary artery abnormalities, including dilation and aneurysms (Fig. 142-7), which can result in myocardial infarction, aneurysm rupture, and sudden death. Myocardial infarction can occur from thrombosis of an aneurysm, which is most common in the first few months after the onset, or from coronary artery stenosis, which occurs months to years following the illness. Aneurysm rupture is less common and usually occurs within the first month after the onset. More than 50% of KD patients have myocarditis during the acute febrile phase, manifested clinically as tachycardia disproportionate to fever, which generally improves rapidly with IVIG therapy. In the acute phase of illness, a pericardial effusion can be present; this resolves spontaneously. In patients with the mostsevere coronary artery aneurysms, aneurysms of other medium-sized arteries can also be observed, most commonly in the iliac, femoral, and axillary arteries. Valvulitis significant enough to require valve replacement is rarely reported. Although KD is a systemic inflammatory disease affecting multiple organs and tissues, there are no known long-term consequences of the disease outside of the heart and blood vessels.
ETIOLOGY AND PATHOGENESIS
The etiology of KD remains unknown. The hypothesis that best fits the available clinical, immunologic, and epidemiologic data is that KD results from infection
2583
22
with a ubiquitous etiologic agent that usually results in asymptomatic infection, but causes KD in a small subset of genetically predisposed individuals. Genetic predisposition is a common theme in susceptibility and host response to infectious diseases. It is likely that KD is polygenic. Intensive investigation of genetic factors influencing susceptibility to KD is ongoing by several international collaborative groups. A functional polymorphism in the ITPKC gene, which is a negative regulator of T-cell activation, is associated with KD susceptibility and risk of developing coronary artery abnormalities21; other immune genes, such as CASP3, BLK, CD40, FCGR2A, and ORAI1, also appear to be associated with KD susceptibility.22-24
Three linked pathologic processes are characteristic of KD vasculopathy, which most significantly affects the coronary arteries: neutrophilic necrotizing arteritis, which occurs in the first 2 weeks after fever onset; subacute/chronic vasculitis, which begins in the first 2 weeks but can persist for months to years and is comprised of lymphocytes (predominately CD8 T lymphocytes25), plasma cells (particularly immunoglobulin [Ig] A plasma cells26,27), eosinophils, and macrophages; and luminal myofibroblastic proliferation, which is closely associated with subacute/chronic vasculitis and can result in progressive arterial stenosis.28 These 3 processes explain the potential adverse outcomes of KD. Necrotizing arteritis can result in necrosis and sloughing of the intima and media; in its most severe form only a thin layer of adventitia may remain, resulting in giant aneurysms that occasionally rupture, but more commonly accumulate layers of thrombi, which can become occlusive and cause myocardial infarction. Subacute/chronic arteritis is associated with luminal myofibroblastic proliferation and progressive arterial stenosis, which with or without overlying thrombi can lead to myocardial infarction.28 Adaptive immune responses in KD have been demonstrated to be antigendriven.29-31 The presence of IgA plasma cells and CD8 T cells as primary components of the inflammatory infiltrate in acute KD suggests an immune response to an intracellular pathogen with a respiratory portal of entry. Synthetic versions of these oligoclonal IgA antibodies identify antigen in acute KD tissues, which appears to reside in intracytoplasmic inclusion bodies containing protein and RNA, and are highly suggestive of a viral etiology, although the specific agent has so far eluded identification, perhaps because of a lack of homology to known viral families.32-35 The immune transcriptional profile of KD arteritis has features of an antiviral immune response, such as activated cytotoxic T-lymphocyte and Type I interferon-induced gene upregulation;36 this information should help guide the development of new immunomodulatory therapies for KD arteritis.
RISK FACTORS
RISK FACTORS
Asian children, particularly Japanese, Chinese, and Korean children, have the highest attack rates of
2584
KD.10,14 Infants and older children have the highest prevalence of coronary artery abnormalities following KD.11-13 Risk-scoring systems have been developed in Japan that are useful in determining those KD children who are at highest risk of developing coronary artery disease and allowing for selective intensification of primary KD therapy.37 However, these scoring systems do not accurately predict risk of coronary artery disease in non-Japanese, multiethnic populations.38
DIAGNOSIS
In the absence of knowledge of the etiology of KD, a diagnostic test is not available. Laboratory findings in acute KD are nonspecific but quite characteristic. A complete blood count reveals either a normal or elevated white blood cell count with a neutrophil predominance. A low white blood cell count with lymphocyte predominance would be distinctly unusual in KD. A normochromic, normocytic anemia can be present, and resolves spontaneously with resolution of KD. The platelet count is normal in the first week of illness, although thrombocytopenia has been reported to be associated with a more severe outcome. Thrombocytosis, with platelet counts sometimes exceeding 1,000,000/mm3, is characteristic of the subacute phase of KD, peaking in the second to third week after the onset of fever. This feature, like periungual desquamation, is not useful in making a diagnosis of KD in the first week of fever. Patients with anemia and low albumin levels may be at higher risk of developing coronary artery disease. A mild elevation of the liver transaminases is commonly observed in acute KD. Occasionally, obstructive jaundice occurs. Gallbladder hydrops, with accompanying right upper quadrant abdominal pain, resolves spontaneously and does not require surgical intervention. Sterile pyuria is also commonly observed. Acute-phase reactants such as the C-reactive protein (CRP) and the ESR are characteristically elevated in patients with acute KD, and the CRP is sometimes used to follow clinical response in patients refractory to IVIG therapy. Once IVIG is given, the ESR cannot be used to follow clinical response, because IVIG itself transiently increases the ESR. A complete blood count and CRP or ESR should be performed at baseline, and the CRP repeated at 2 to 3 weeks and 6 to 8 weeks after onset to monitor for resolution of inflammation.
PATHOLOGY
PATHOLOGY
Skin and lymph node biopsies reveal nonspecific findings in KD and are not useful in establishing the diagnosis.
IMAGING
IMAGING
Echocardiography should be performed in all children with suspected KD, and should be performed at
diagnosis, at 2 to 3 weeks after fever onset, and at 6 to 8 weeks after fever onset.39 The peak time to detect coronary artery dilation is 2 to 3 weeks after onset of fever, during the subacute phase of illness. Patients who do not manifest coronary artery abnormalities on any of these 3 echocardiograms may not require additional studies, although some centers perform 1 additional echocardiogram at 1 year after the onset. In patients who develop coronary artery dilation, more frequent echocardiograms will be needed during the acute phase and in followup; these should be scheduled in consultation with a pediatric cardiologist. In particular, frequent echocardiograms are advisable in the first few weeks in patients in whom coronary artery luminal diameters are continuing to expand; these patients are at particularly high risk of developing coronary artery thrombosis. Electrocardiogram in the acute febrile phase of illness most often shows a prolonged PR interval and/or nonspecific ST- and T-wave changes. CT angiography or magnetic resonance angiography can be useful in evaluating the coronary arteries of teenagers in whom adequate images of the coronary arteries may be difficult to obtain by echocardiography, and of children with particularly severe coronary artery disease.40,41
DIAGNOSTIC ALGORITHM
DIAGNOSTIC ALGORITHM
A diagnosis of classic KD is made in the presence of prolonged fever lasting 5 or more days, with 4 of the following 5 clinical features in the absence of another explanation for the illness: (a) nonpurulent bulbar conjunctival injection; (b) red, swollen, dry lips, which may crack and bleed; (c) redness and swelling of the hands and feet; (d) rash; and (e) cervical lymphadenopathy, 1.5 cm or larger in diameter (Table 142-2). Experienced physicians can make a diagnosis of KD before the fifth day of fever in children with classic features. A patient with prolonged fever and fewer than 4 of the other features of the
Fever ≥5 days,a high spiking and intermittent, with at least 4 of the
Fever ≥5 days,a high spiking and intermittent, with at least 4 of the 5 clinical featuresb:
- Bilateral, nonexudative conjunctival injection.
- Oral mucosal changes, including red, dry, cracked lips, pharyngeal erythema, and/or strawberry tongue.
- Changes of the hands and feet: erythema of palms and soles and/or swelling of the hands and feet during the acute phase, and/or periungual desquamation of the fingers and toes during the subacute phase.
- Rash: erythematous morbilliform, scarlatiniform, or targetoid.
- Cervical lymphadenopathy ≥1.5 cm in diameter.
5 clinical featuresb:
- Bilateral, nonexudative conjunctival injection.
- Oral mucosal changes, including red, dry, cracked lips, pharyngeal
erythema, and/or strawberry tongue.
3. Changes of the hands and feet: erythema of palms and soles
and/or swelling of the hands and feet during the acute phase, and/or periungual desquamation of the fingers and toes during the subacute phase.
4. Rash: erythematous morbilliform, scarlatiniform, or targetoid.
5. Cervical lymphadenopathy ≥1.5 cm in diameter.
aThe diagnosis can be made before the fifth day of fever by experienced physicians if the patient has the other clinical features of the illness.
bIn the absence of another explanation for the illness.
22
illness can be diagnosed with KD if coronary artery abnormalities develop. Incomplete (or atypical) KD refers to children with prolonged fever and fewer than 4 of the other features of illness who have a laboratory profile compatible with KD. Such patients should undergo echocardiography and be considered for treatment with IVIG because KD patients, particularly infants, do not always manifest classic diagnostic criteria during the acute febrile phase of illness, yet can develop coronary artery abnormalities. The American Heart Association Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease has published an algorithm to assist the clinician in diagnosing incomplete KD.39 This algorithm emphasizes the importance of combining clinical features, laboratory findings, and echocardiographic findings in making a diagnosis (Table 142-3). In difficult cases, consultation with a KD expert should
Fever for ≥5 days with 2 or 3 compatible clinical features of KD and
Fever for ≥5 days with 2 or 3 compatible clinical features of KD and
■ESR ≥40 mm/h and/or CRP ≥3.0 mg/dL
■ESR ≥40 mm/h and/or CRP ≥3.0 mg/dL
■If patient has at least 3 compatible laboratory features,a perform echocardiogram and begin treatment.
■If patient has at least 3 compatible laboratory features,a perform
echocardiogram and begin treatment.
■If patient has fewer than 3 compatible laboratory features,a but has dilated coronary arteries by echocardiogram (Z score of LAD or RCA ≥2.5), begin treatment.
■If patient has fewer than 3 compatible laboratory features,a but
has dilated coronary arteries by echocardiogram (Z score of LAD or RCA ≥2.5), begin treatment.
■If patient has fewer than 3 compatible laboratory featuresa and LAD and RCA Z scores <2.5, but has at least 3 supportive echocardiographic features,a begin treatment.
■If patient has fewer than 3 compatible laboratory featuresa
and LAD and RCA Z scores <2.5, but has at least 3 supportive echocardiographic features,a begin treatment.
■If patient has fewer than 3 compatible laboratory features,a LAD and RCA Z scores <2.5, and fewer than 3 supportive echocardiographic features,b then follow patient and consider other diagnoses. If fevers persist and no other diagnosis is established, consider repeating laboratory tests and echocardiogram and consider consulting a KD expert. If fever resolves, KD is unlikely.
■If patient has fewer than 3 compatible laboratory features,a LAD
and RCA Z scores <2.5, and fewer than 3 supportive echocardiographic features,b then follow patient and consider other diagnoses. If fevers persist and no other diagnosis is established, consider repeating laboratory tests and echocardiogram and consider consulting a KD expert. If fever resolves, KD is unlikely.
■ESR <40 mm/h and/or CRP <3.0 mg/dL
■ESR <40 mm/h and/or CRP <3.0 mg/dL
■Follow patient. If fever continues, reevaluate clinically and consider repeating ESR and CRP. If fever resolves but patient develops typical periungual desquamation, perform echocardiogram.
■Follow patient. If fever continues, reevaluate clinically
and consider repeating ESR and CRP. If fever resolves but patient develops typical periungual desquamation, perform echocardiogram.
aCompatible laboratory features:
-
Albumin ≤3.0 g/dL
-
Anemia for age
-
Elevated alanine aminotransferase
-
Platelet count ≥450,000/mm3 after the 7th day of illness
-
White blood cell (WBC) ≥15,000/mm3
-
Urinalysis with ≥10 WBC/high-power field
bSupportive echocardiographic features:
- Lack of tapering
- Decreased left ventricular function
- Mitral regurgitation
- Pericardial effusion
- Z scores of LAD or RCA of 2.0 to 2.5 CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; LAD, left anterior descending coronary artery; RCA, right coronary artery. Data from Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110(17):2747-2771.
2585
22
be considered. If the patient is not treated for KD but develops typical periungual desquamation after fever has resolved, and an alternative diagnosis that could explain this clinical finding has not been established (such as scarlet fever), an echocardiogram should be repeated. Infants 6 months of age or younger can have mild or subtle clinical findings with KD, but have a high risk of developing coronary artery abnormalities. Therefore, infants with fever for 1 week or longer without other explanation should have laboratory testing performed. If evidence of an inflammatory process is present, an echocardiogram should be ordered and KD considered, even in the absence of other clinical features of the illness.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
The KD child with prolonged high fever, marked conjunctival injection, red, swollen hands and feet, erythematous rash, and red, cracked, bleeding lips who has a markedly elevated ESR and/or CRP and an elevated peripheral white blood cell count with a neutrophil predominance has a very distinctive illness and usually does not pose any difficulties in diagnosis. In other patients who have only some of the clinical features of KD, or in whom clinical findings are not as dramatic, other diagnoses must be carefully considered (Table 142-4). In areas where measles is still prevalent, differentiating the 2 disorders can be difficult. Classically, patients with measles have rash that begins on the face behind the ears and Koplik spots in the mouth; neither of these features is observed in KD. Later in the course of measles infection, the rash becomes diffuse and Koplik spots are no longer visible. Conjunctival injection and edema of the hands and feet can be observed in both disorders. In uncomplicated measles, the peripheral white blood cell count and the ESR are generally low. The measles IgM antibody is virtually always positive by the appearance of the measles rash, and is the best single test to differentiate the two conditions. Group A streptococcal infection should be considered in the differential diagnosis of a KD patient with
■Measles
■Adenovirus infection
■Enterovirus infection
■Scarlet fever
■Staphylococcal scalded skin syndrome
■Toxic shock syndrome
■Drug hypersensitivity reaction
■Juvenile rheumatoid arthritis
If patient has epidemiologic risk factor:
If patient has epidemiologic risk factor:
■Rocky Mountain spotted fever
■Rocky Mountain spotted fever
2586
■Leptospirosis
■Leptospirosis
a scarlatiniform rash, and can be excluded by a negative throat culture. Diagnostic uncertainty could arise in a KD patient who is a group A streptococcal carrier. Administration of antibiotic therapy followed by reevaluation in 24 to 48 hours generally clarifies the diagnosis; children with group A streptococcal pharyngitis have a rapid response to therapy, while antibiotics are ineffective in KD. Adenovirus infection can mimic KD. The presence of exudative conjunctivitis and exudative pharyngitis suggests adenovirus as the most likely diagnosis. Other viruses can occasionally cause prolonged fever, such as enterovirus; in differentiating KD patients from those with uncomplicated viral infection, laboratory tests such as the ESR, CRP, and urinalysis can be helpful, as pyuria and markedly elevated acute-phase reactants are more typical of KD. Drug hypersensitivity reactions can mimic KD. Oral and mucosal ulcers observed in Stevens–Johnson syndrome are absent in KD. Edema of the face, particularly around the eyes, is much more suggestive of drug reaction than KD. In general, the ESR and CRP are either normal or only mildly elevated in drug hypersensitivity reactions. Staphylococcal scalded skin syndrome is easily distinguished by the classic finding of painful skin in staphylococcal scalded skin syndrome, which is not observed in KD, and by flaccid blisters, desquamation, and a positive Nikolsky sign, which is present in staphylococcal scalded skin syndrome and absent in KD. Although hypotension is unusual in KD, a KD shock syndrome occurs rarely,42,43 and toxic shock syndrome is in the differential diagnosis of such patients. Renal involvement and elevated creatinine phosphokinase are more likely to be observed in toxic shock syndrome than in KD. IVIG administered for a possible diagnosis of KD may serve as adjunctive therapy for toxic shock syndrome. Juvenile rheumatoid arthritis is a diagnosis of exclusion, and an occasional patient with this disorder might initially be diagnosed with and treated for incomplete KD. The correct diagnosis may become apparent when fever recurs following reduction of high-dose aspirin therapy, implying an original clinical response to aspirin rather than to IVIG.
CLINICAL COURSE AND PROGNOSIS
Approximately 85% of KD children treated with IVIG and aspirin within the first 10 days of illness respond with rapid resolution of fever and other clinical signs. The vast majority of KD patients who are promptly diagnosed and treated do well, without developing cardiac complications. However, approximately 15% of KD children treated within the first 10 days of illness continue to have fever following a single infusion of IVIG with aspirin and require additional therapy; these patients have a higher risk of developing coronary
artery abnormalities.44 A study assessing KD patients treated within the first 10 days of illness indicated that 18% had a coronary artery Z score higher than 2 at week 5 after the onset.45 The larger the aneurysm, the less likely that the luminal diameter will return to normal over time. Very large or “giant” coronary artery aneurysms are associated with the most-severe outcomes.46 A decrease in luminal diameter of an aneurysm can result from thrombosis or luminal myofibroblastic proliferation, which can lead to coronary artery stenosis and myocardial infarction.28 In young infants and children, myocardial infarction usually presents as shock, emesis, and/or abdominal pain.47 Patients with significant coronary artery disease may require catheter intervention procedures,48 coronary artery bypass surgery,49 or, rarely, heart transplantation.50 Cardiovascular risk assessment should be performed at intervals dependent upon the severity of coronary artery abnormalities.39
MANAGEMENT
INTERVENTIONS
INTERVENTIONS
MEDICATIONS
A single infusion of IVIG 2 g/kg with aspirin (80-100 mg/kg/day given every 6 hours orally) should be administered to children with acute KD as soon as possible after diagnosis (Table 142-5) as demonstrated in a study by Newburger and colleagues.51 This regimen, when administered to children with KD within the first 10 days of fever, was shown to reduce the prevalence of coronary artery abnormalities from 25% in untreated patients to 5% in those who receive the therapy. However, this study was performed prior to use of coronary artery Z scores to identify coronary artery dilation, and more recent studies suggest a higher prevalence of coronary artery dilation in KD patients overall than was previously appreciated.45,52
Most children experience rapid resolution of fever and other clinical signs following treatment, as well as improvement in acute-phase reactants. The mechanism of action of IVIG in KD is unknown. Aspirin is given in high doses during acute KD for antiinflammatory effect. It is generally continued at 80 to 100 mg/kg/day until the 14th illness day, or
■Intravenous gammaglobulin (IVIG) 2 g/kg infused over 10 to 12 hours; monitor vital signs carefully during infusion, with aspirin 80 to 100 mg/kg/day divided every 6 hours orally until the 14th illness day or until patient is afebrile for at least 2 days, then reduce dose to 3 to 5 mg/kg/day as a single daily dose.
■Intravenous gammaglobulin (IVIG) 2 g/kg infused over 10 to
12 hours; monitor vital signs carefully during infusion, with aspirin 80 to 100 mg/kg/day divided every 6 hours orally until the 14th illness day or until patient is afebrile for at least 2 days, then reduce dose to 3 to 5 mg/kg/day as a single daily dose.
■Aspirin is discontinued if echocardiograms at 2 to 3 weeks and 6 to 8 weeks are normal and when acute-phase reactants have normalized.
■Aspirin is discontinued if echocardiograms at 2 to 3 weeks and
6 to 8 weeks are normal and when acute-phase reactants have normalized.
22
until the patient has been afebrile for at least 2 days. Aspirin is then reduced to 3 to 5 mg/kg/day given in a single daily dose, for its antithrombotic effect. Aspirin is discontinued at 6 to 8 weeks after onset if all echocardiograms have been normal and acute-phase reactants have normalized. If coronary artery abnormalities develop, low-dose aspirin is continued. Depending upon the severity of coronary artery disease, other therapies, such as clopidogrel and warfarin, may be indicated39; such decisions should be made in consultation with a pediatric cardiologist. IVIG and aspirin is also given to KD patients who present after the 10th day of illness if fever and/or clinical and laboratory signs of ongoing inflammation are present, although the efficacy of the therapy in this clinical situation is uncertain. In Japan, risk-scoring systems have been developed that can predict which Japanese children are at highest risk of developing coronary artery abnormalities with good accuracy, and the “RAISE” study showed that primary therapy with IVIG and a tapering course of prednisolone over 2 to 3 weeks improved outcomes in high-risk patients.37
Unfortunately, risk-scoring systems have thus far performed poorly in multiethnic populations such as in North America, making the selection of patients in non-Japanese populations for intensified primary therapy more problematic.38
Approximately 15% of acute KD patients do not respond to initial therapy; optimal therapy for these patients with “refractory” KD is unknown. Most of these patients will respond to a second 2 g/kg IVIG infusion.44 In patients who do not respond to initial therapy and are already in a high-risk category because of the presence of coronary artery dilation, a second dose of IVIG given with prednisolone in a tapering regimen over 2 to 3 weeks should be considered.53
Other options for IVIG nonresponders include highdose intravenous methylprednisolone once daily for 3 days or infliximab.54,55 More specific therapy awaits the identification of the cause of KD.
COUNSELING
Patients who do not develop coronary artery abnormalities are not known to develop any long-term sequelae. Patients who have coronary artery abnormalities with normalization of the luminal diameter over time should be followed by a pediatric cardiologist; these patients may be at risk of developing arterial stenoses in the future. Patients with significant persisting coronary artery abnormalities should be followed by a pediatric cardiologist who can make recommendations about long-term therapy and activity restrictions based upon guidelines established by the American Heart Association.39
TREATMENT ALGORITHM
TREATMENT ALGORITHM
2587
22
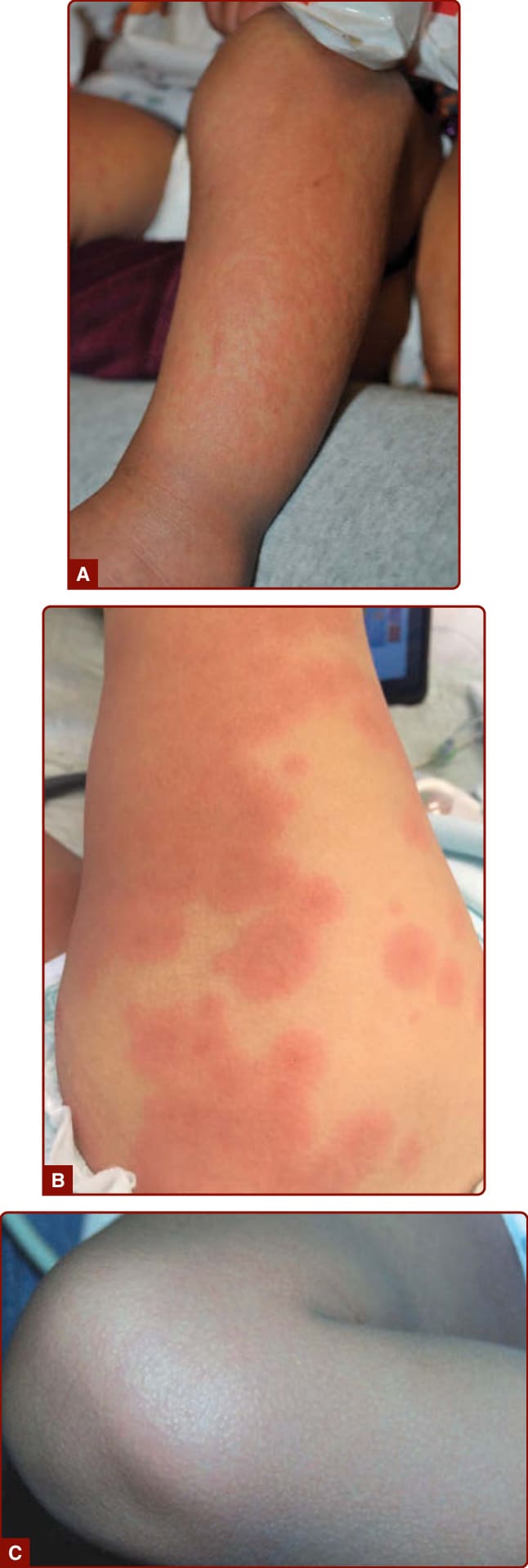
Figure 142-1 The exanthems observed acute in Kawasaki disease. A, Erythematous morbilliform exanthem; B, targetoid or urticarial changes; C, diffuse erythema.

Figure 142-2 Erythematous desquamating groin rash of acute Kawasaki disease.

Figure 142-3 Desquamation of the feet in the subacute phase of Kawasaki disease; this process began periungually and progressed to involve the entire soles.

Figure 142-4 Erythema and edema of the hands in Kawasaki disease.

Figure 142-5 Conjunctival injection with limbal sparing in acute Kawasaki disease.
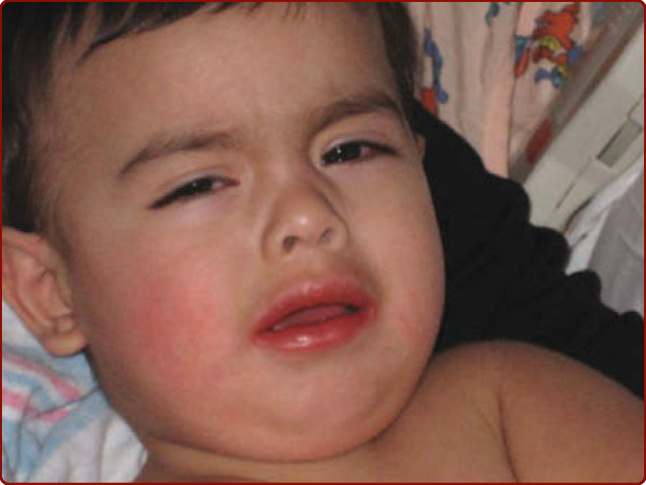
Figure 142-6 Typical facial features of acute Kawasaki disease showing conjunctival injection and red dry lips.
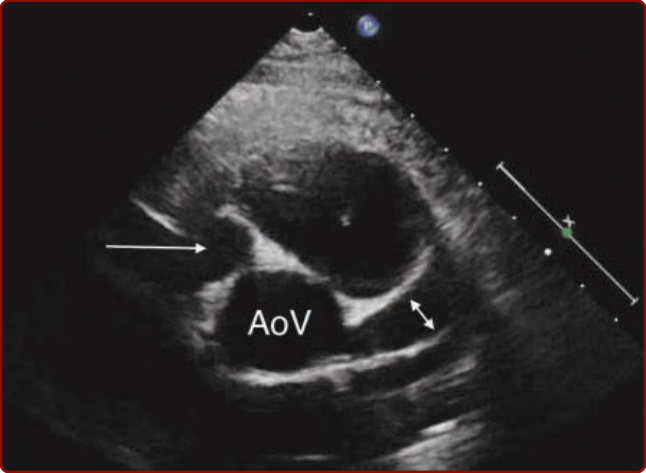
Figure 142-7 Coronary artery aneurysms in Kawasaki disease demonstrated by echocardiography. AoV, aortic valve; double arrow, aneurysm of proximal left anterior descending coronary artery; single arrow, large aneurysm of proximal right coronary artery.
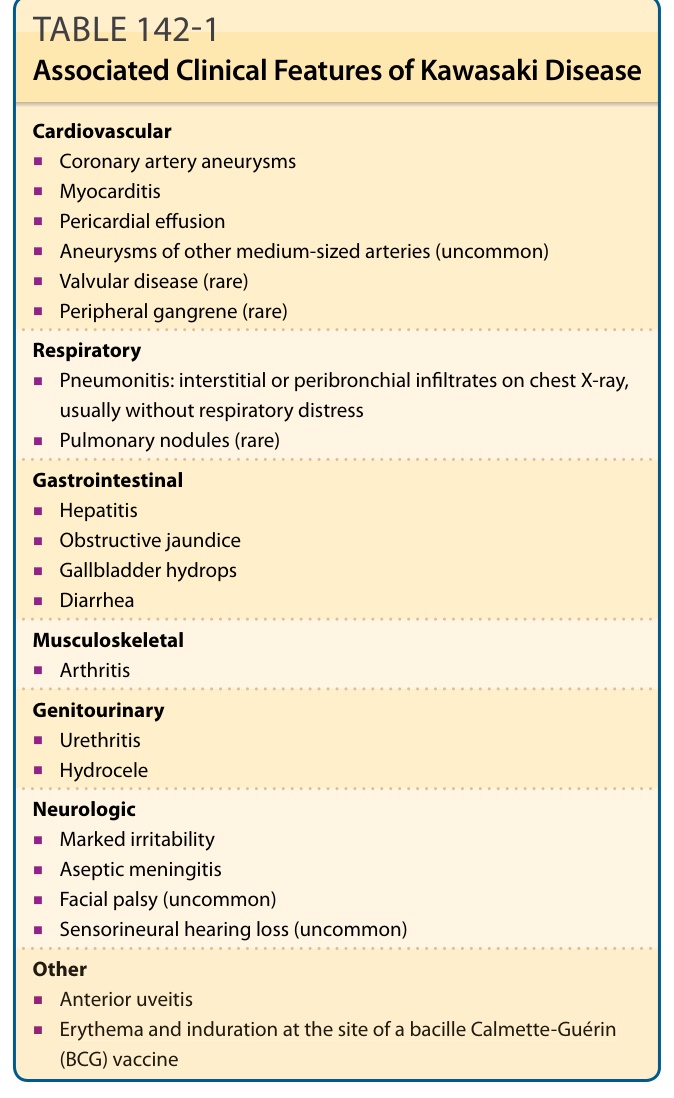
TABLE 142-1 Associated Clinical Features of Kawasaki Disease
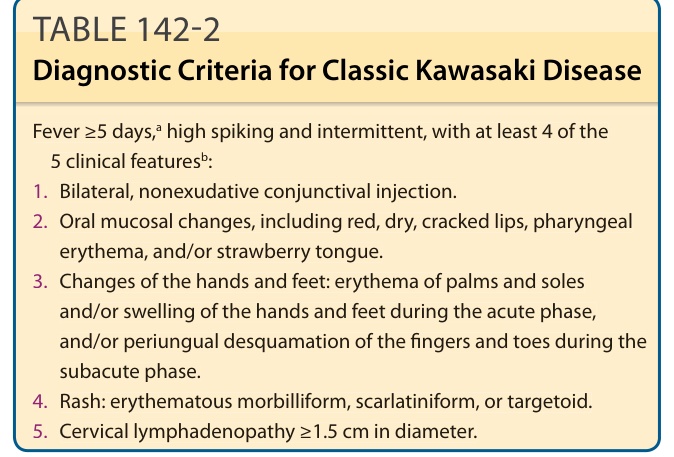
TABLE 142-2 Diagnostic Criteria for Classic Kawasaki Disease
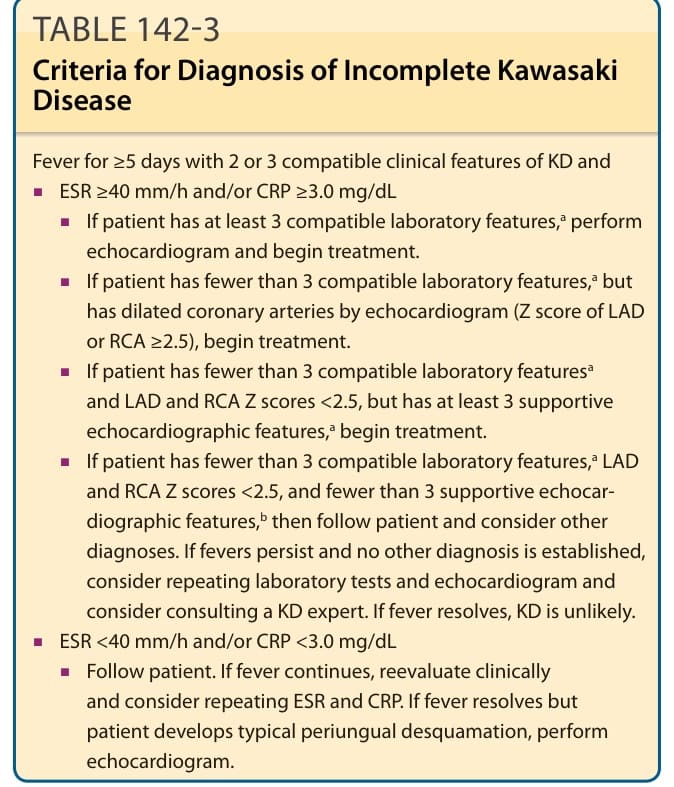
TABLE 142-3 Criteria for Diagnosis of Incomplete Kawasaki Disease
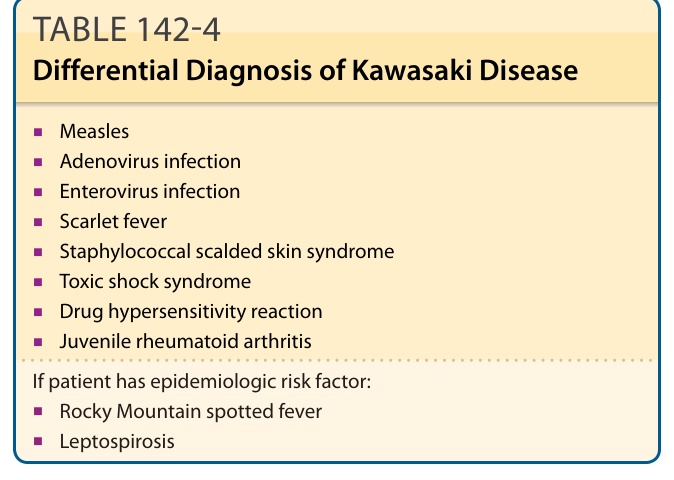
TABLE 142-4 Differential Diagnosis of Kawasaki Disease
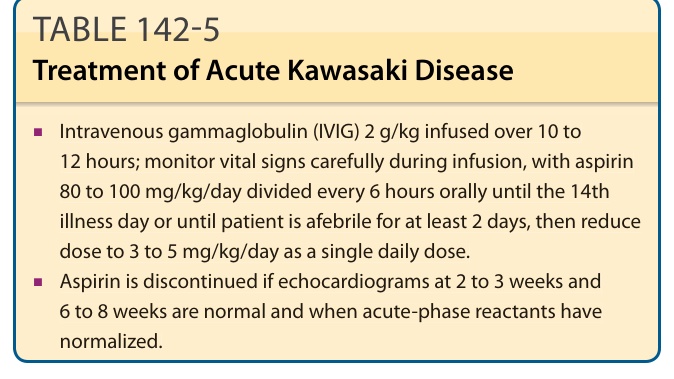
TABLE 142-5 Treatment of Acute Kawasaki Disease