Lipogenic Neoplasms
20
AT-A-GLANCE
■ Lipogenic neoplasms represent the most frequent mesenchymal neoplasms.
■ Lipogenic neoplasms include benign neoplasms (eg, lipoma, angiolipoma), intermediate, locally aggressive, nonmetastasizing neoplasms (eg, atypical lipomatous tumor), and clearly malignant lesions (eg, pleomorphic liposarcoma).
■ Anatomic site, depth, and size are responsible for striking differences in regard to incidence, morphology, and prognosis.
■ The clinical presentation of lipogenic neoplasms is usually nonspecific.
■ The majority of lipogenic neoplasms is characterized by distinct cytogenetic abnormalities that may have diagnostic and therapeutic value.
■ Surgical excision is the treatment of choice; in cases of malignant neoplasms not amenable for complete excision radiation therapy, however, chemotherapy or target-like therapy may be used.
Although lipogenic neoplasms represent the largest single group of mesenchymal tumors in the skin and in soft tissues, there are significant differences in regard to incidence, morphologic features, and prognosis between superficial and deep-seated lipogenic neoplasms that are important to know to avoid misdiagnosis and therapeutic errors. Whereas liposarcomas in deep soft tissues represent the most common sarcomas in adults, they are exceedingly rare in purely dermal location. Cases of spindle-cell/pleomorphic lipoma arising in the subcutis are encapsulated and occur predominantly in the neck and shoulder region of elderly male patients. In contrast, purely dermal spindle-cell/pleomorphic lipomas are ill-defined, infiltrative lesions that occur equally in both genders and show a broad anatomic distribution. The prognosis of atypical lipomatous tumor (“well-differentiated liposarcoma”) is strongly related to site and size of the neoplasms. Cases of atypical lipomatous tumor, arising in the retroperitoneum, intraabdominal, in the mediastinum and in the spermatic cord are associated with a poor clinical prognosis. These neoplasms often achieve a large size, recur repeatedly, and may cause death in a high number of cases as a result of uncontrolled local effects. In striking contrast, cases of atypical lipomatous tumor arising in surgically amenable soft tissue of the extremities usually do not recur after complete excision, and in general superficially located liposarcomas have a relatively good prognosis.
LIPOMA
AT-A-GLANCE
■ Lipoma is one of the most common benign mesenchymal neoplasms in adults.
■ Lipomas are composed of mature white adipocytes.
■ Lipomas show varying cytogenetic abnormalities.
■ Although surgical excision is curative, cases of intramuscular lipoma show a higher recurrence rate.
EPIDEMIOLOGY
EPIDEMIOLOGY
Lipoma is the most common benign mesenchymal neoplasm and tends to occur in adults without gender predilection. Cases in childhood and multiple lesions are rare.
CLINICAL FEATURES
CLINICAL FEATURES
Lipomas usually present as a painless, slowly growing mass involving the subcutaneous tissue of the trunk, neck, or extremities; involvement of the hands and feet is uncommon. Superficial lipomas are typically small, measuring less than 5 cm. In contrast, deepseated intramuscular and intermuscular lipomas may reach a considerable size. Parosteal lipoma arises on the surface of bone, and so-called lipoma arborescens represents a villous lipomatous proliferation of the synovial membrane.1 Lipomas may be seen as a manifestation of Gardner syndrome, and multiple lipomas together with macrocephaly, lymphangiomas, and hemangiomas are noted in Bannayan syndrome (Table 122-1).2
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Lipomas are cytogenetically heterogeneous and the most common abnormalities include aberrations involving 12q13-15, rearrangements involving 6p21-23, and deletions involving 13q.3 The HMGA2 gene, localized at 12q14.3, plays an important role in the pathogenesis
SYNDROME ASSOCIATED TUMORS
Gardner syndrome Familial adenomatous polyposis, desmofi- bromatosis, lipomas, osteomas, cysts
Bannayan-Riley- Ruvalcaba syndrome Macrocephaly, lipomas, lymphangiomas, hamartomas, intestinal polyposis, lentigines
Cowden syndrome Hamartomas, trichilemmomas, lipomas, oral papillomas, palmoplantar keratoses
Goldenhar-Gorlin syndrome Intracranial lipomas, hydrocephalus, oculoauriculovertebral dysplasia
Myoclonus epilepsy and ragged-red fibers syndrome
Symmetric lipomas
CLOVE syndrome Congenital lipomatous overgrowth, vascular malformations, epidermal nevi
Ekbom syndrome Cervical lipomas, cerebellar ataxia,
Ekbom syndrome Cervical lipomas, cerebellar ataxia, photomyoclonus, skeletal deformities
photomyoclonus, skeletal deformities
of some lipomas, and a recombination of HMGA2 with several genes has been reported.4
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Classical subcutaneously located lipomas are wellcircumscribed, encapsulated and lobulated lesions composed of mature adipocytes with thin and hypocellular fibrous septa containing thin-walled capillaries (Fig. 122-1). There is only slight variation in size and shape of adipocytes and no nuclear atypia is present. Immunohistochemically, tumor cells are negative for p16, MDM2, and CDK4. Cases of lipoma may show posttraumatic changes with fat necrosis and inflammation, and the presence of numerous histiocytes
A
20
containing enlarged nuclei that show a cytoplasmic staining for p16, MDM2, and CDK4 may mimic features of more aggressive atypical lipomatous tumor. Cases of lipoma may contain abundant fibrous tissue (fibrolipoma), cartilage (chondrolipoma) or bone (osteolipoma) (Fig. 122-2). Purely dermal lipomas are unencapsulated and rather ill-defined lesions (Fig. 122-3), and if sweat ducts and sweat glands are present within the lesion, the term adenolipoma has been used. Intramuscular and intermuscular lipomas are ill-defined, infiltrating neoplasms (Fig. 122-4) and preexisting skeletal muscle fibers often show features of atrophy.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Angiolipoma is characterized by a variable increased number of blood vessels containing fibrin thrombi, and often present as painful multiple lesions. Cases
B
2173
20
of atypical lipomatous tumor are characterized by striking variations in size and shape of lipogenic cells, and the presence of enlarged and hyperchromatic nuclei. The fibrous septa in atypical lipomatous tumor often contain atypical cells and lipoblasts may be present. Immunohistochemically, a focal expression of p16 is seen in atypical lipomatous tumor, and in a number of cases a focal nuclear staining for MDM2 and CDK4 is present. Fluorescence in situ hybridization (FISH) analysis reveals amplification of MDM2 and CDK4 in cases of atypical lipomatous tumor.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Classical lipomas are entirely benign and recur only rarely; in contrast, intramuscular and intermuscular
2174
lipoma shows a higher rate of local recurrences (up to 20%).5 The transition of a preexisting lipoma to an atypical lipomatous tumor represents an exceedingly rare phenomenon.6 Surgical excision is curative.
LIPOMATOSIS
AT-A-GLANCE
■ Lipomatosis is characterized by a diffuse overgrowth of mature adipose tissue infiltrating through preexisting structures.
■ Different clinical presentations are known.
EPIDEMIOLOGY AND CLINICAL FINDINGS
EPIDEMIOLOGY AND
CLINICAL FINDINGS
Diffuse lipomatosis occurs predominantly in children and rarely in adults. It is characterized by a diffuse overgrowth of mature lipogenic tissue involving subcutaneous tissue and skeletal muscle of the trunk and the extremities; in addition, osseous involvement may be seen. Pelvic lipomatosis is seen more frequently in black males, whereas symmetric lipomatosis (Madelung disease) develops in middleaged men of Mediterranean origin and has a predilection for the neck, shoulder, and proximal upper limbs. In addition, peripheral neuropathy is a common finding in these patients. HIV-positive patients treated with protease inhibitors may develop lipodystrophy with increased fat tissue at the neck, the breast, and visceral organs, and steroid lipomatosis is seen in patients on hormonal therapy or suffering from increased endogenous production of adrenocortical steroids.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Generally, the basic mechanisms in lipomatosis are not well understood; however, an association with mitochondrial dysfunction has been reported, and multiple deletions of mitochondrial DNA, as well as point mutations in mitochondrial genes, have been found.7
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
The gross appearance and the histologic features are the same for all of the different subtypes of
lipomatosis. Poorly circumscribed, infiltrating, soft, yellow, fat tissue that is identical to normal fat is seen.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Palliative surgical excision of the fat tissue is the treatment of choice; however, all forms of lipomatosis tend to recur, and massive accumulation of fat tissue may cause considerable clinical problems.
LIPOMATOSIS OF NERVE
AT-A-GLANCE
■ Lipomatosis of nerve is a rare lesion seen in infants and children.
■ Lipomatosis of nerve is a growing mass with a predilection for the hand.
■ Lipomatosis of nerve shows a proliferation of adipose and fibrous tissue within the epineurium and perineurium, mainly of the median nerve.
EPIDEMIOLOGY
EPIDEMIOLOGY
Lipomatosis of nerve, also known as fibrolipomatous hamartoma of nerve, arises most frequently at birth or in early childhood, and may be associated with macrodactyly of the digits innervated by the affected nerve.8
CLINICAL FEATURES
CLINICAL FEATURES
Clinically, the patients present with a slowly growing mass that is often associated with pain, paresthesia, and sensor or motor deficits. The median nerve and its branches, followed by the ulnar nerve, are most commonly affected, whereas an involvement of cranial nerves and the brachial plexus is seen only rarely.9,10
20
A
B
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Grossly, a fusiform enlargement of the affected nerve is seen, and histologically, the epineurial and perineurial compartments of the affected nerve are infiltrated by mature adipose tissue and collagenous fibrous tissue (Fig. 122-5). Concentric perineurial fibrosis is present, and, rarely, metaplastic bone formation has been reported.11
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Lipomatosis of nerve is an entirely benign lesion; surgical excision may cause severe damage of the affected nerve.
2175
20
NEVUS LIPOMATOSIS SUPERFICIALIS
AT-A-GLANCE
■ Nevus lipomatosis superficialis (Hoffmann- Zurhelle) represents a rare type of connective tissue nevus that affects children and young adults.
■ Nevus lipomatosis superficialis is usually found as a plaque-like, solitary lesion, which arises predominantly at the buttock, lumbar back, and posterior thigh.
■ The lesions are composed of mature adipose tissue and connective tissue components.
EPIDEMIOLOGY
EPIDEMIOLOGY
Nevus lipomatosus superficialis is a rare form of connective tissue nevus that usually affects children and young adults in the first decades of life with an equal gender distribution.
CLINICAL FEATURES
CLINICAL FEATURES
Cases of nevus lipomatosus superficialis present as plaques, papules, or solitary lesions with a predilection for the buttocks, upper posterior thighs, and lumbar back. A generalized form is extremely rare. The lesions are unilateral, and sometimes a linear or zosteriform arrangement is noted.
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Histologically, the ill-defined lesions are composed of mature adipose tissue that replaces the dermis. In addition, thickening of collagen bundles, as well as an increase of elastic fibers in deeper parts of the dermis and an increase of fibroblasts, may be seen. The overlying epidermis may show slight acanthosis and hyperpigmentation (Fig. 122-6).
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Rare dermal spindle-cell lipoma is composed of mature adipose tissue associated with bland spindled tumor cells that stain positively for CD34, show loss of Rb-1 expression, and the often myxoid
2176
A
B
stroma contains hyalinized collagen fibers and mast cells.
LIPOBLASTOMA/ LIPOBLASTOMATOSIS
AT-A-GLANCE
■ Lipoblastomas/lipoblastomatosis are benign lipogenic neoplasms arising predominantly in infancy and early childhood.
■ Lipoblastomas/lipoblastomatosis are wellcircumscribed, lobulated lesions composed of lipogenic cells showing a spectrum of maturation from primitive mesenchymal cells and lipoblasts to mature adipocytes.
■ Lipoblastomas/lipoblastomatosis show characteristic genetic changes.
EPIDEMIOLOGY
EPIDEMIOLOGY
Lipoblastomas/lipoblastomatosis are rare, benign neoplasms of embryonal white fat arising predominantly in infants and young children, with a male predominance.12-14 Infrequently, tumors are congenital or occur in young adults.15
CLINICAL FEATURES
CLINICAL FEATURES
Cases of lipoblastoma/lipoblastomatosis tend to occur on the trunk, at the extremities, and in the head and neck region, whereas visceral involvement and involvement of the retroperitoneum, pelvis, mediastinum, and the abdominal cavity is rarely seen. Most cases present as painless, slowly growing lesions. Lipoblastoma is a rather well-circumscribed neoplasm whereas lipoblastomatosis is characterized by an infiltrative growth that often extends into deeper structures. A significant number of patients have disorders of the CNS, such as seizures, autism, developmental delay, congenital anomalies, and/or Sturge-Weber syndrome.14
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Cytogenetically, the majority of analyzed cases of lipoblastoma/lipoblastomatosis show aberrations involving chromosome 8, and a recurrent translocation involving chromosome band 8q11-13 with rearrangements of the PLAG1 gene.16
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Lipoblastoma represents a well-circumscribed, lobulated tumor composed of an admixture of mature and immature lipogenic cells separated by fibrovascular septa (Fig. 122-7). Lobulation is less prominent in cases of lipoblastomatosis that show an infiltrative growth pattern. Lipoblasts are seen in different stages of development, and varying amounts of myxoid stroma with primitive spindled cells and a plexiform vascular pattern (reminiscent of the vascular pattern in myxoid liposarcoma) may be present (Figs. 122-8 and 122-9). Even though some tumors are predominantly composed of mature adipocytes as a manifestation of maturation, the characteristic lobular growth and the presence of fibrous septa are helpful clues for the diagnosis. A fibroblastic proliferation, chondroid metaplasia, or extramedullary hematopoiesis is seen occasionally. The lipogenic cells demonstrate an expression of S-100 protein, PLAG1, and CD34,14 the spindled cells stain often positively for desmin.17 Interestingly, cases of
20
2177
20
lipoblastoma may stain positively for p16, which represents a diagnostic pitfall in the distinction to atypical lipomatous tumor.18
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Myxoid liposarcoma represents one of the most important differential diagnoses of lipoblastoma/ lipoblastomatosis; however, this diagnosis in patients younger than 10 years of age is exceedingly rare. In older children, adolescents, and young adults, the differentiation can be quite problematic. A striking lobulation and lack of hyperchromatic nuclei support the diagnosis of lipoblastoma/ lipoblastomatosis; in addition, different molecular changes are helpful for the correct diagnosis. Further differential diagnoses include lipoma, lipofibromatosis, hibernoma, and atypical lipomatous tumor. Rare lipoblastoma-like tumor of the vulva arises in adults; the tumor lacks PLAG1 expression and shows loss of Rb-1.19
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Lipoblastoma/lipoblastomatosis has an excellent prognosis despite their potential to invade locally and their considerable size as seen in a number of cases. The reported rate of local recurrences is up to 46%,14 which is caused by incomplete excision or confined to diffuse-type lesions (lipoblastomatosis). There is no risk of tumor progression, metastasis, or malignant transformation.
ANGIOLIPOMA
AT-A-GLANCE
■ Angiolipoma is a common, often painful, entirely benign lipogenic lesion.
■ Angiolipoma affects young adults; multiple lesions often are seen.
■ Angiolipoma contains a variable number of thinwalled vessels that may contain fibrin thrombi.
EPIDEMIOLOGY
EPIDEMIOLOGY
Subcutaneous angiolipomas are frequent mesenchymal tumors that occur predominantly in young males; a familial incidence has been described.20
2178
CLINICAL FEATURES
CLINICAL FEATURES
Angiolipomas tend to be multifocal and often present as painful and tender subcutaneous lesions that occur predominantly on the forearm followed by the trunk, upper arm, and legs.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
In contrast to lipomas, all investigated angiolipomas have had a normal karyotype, and because cases of cellular angiolipoma can be almost exclusively composed of blood vessels, it has been speculated, that these lesions represent hemangiomas instead of lipomas.21
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Histologically, angiolipomas are well-circumscribed, encapsulated nodular lesions composed of mature adipocytes, a variable number of thin-walled capillaries, which may contain fibrin thrombi, and stromal spindled cells (Figs. 122-10 and 122-11). In cases of cellular angiolipoma the vessels predominate and lipogenic cells may be absent (Fig. 122-12).
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
The presence of fibrin thrombi and clinical features are helpful in the distinction of angiolipoma from cases of lipoma with an increased number of vessels. Cellular angiolipoma has to be distinguished from vascular neoplasms such as Kaposi sarcoma, kaposiform hemangioendothelioma, spindle-cell hemangioma, and angiosarcoma.
A
B
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
The clinical behavior of angiolipomas is entirely benign and simple resection is curative.
20
SPINDLE-CELL LIPOMA AND PLEOMORPHIC LIPOMA
AT-A-GLANCE
■ Spindle-cell lipoma and pleomorphic lipoma represent a morphologic continuum of a single clinicopathologic entity.
■ Spindle-cell lipoma and pleomorphic lipoma are related to mammary myofibroblastoma and cellular angiofibroma.
■ Classical cases of spindle-cell lipoma and pleomorphic lipoma occur as encapsulated subcutaneous lesions arising predominantly on the posterior neck, shoulder, and upper back of elderly males.
■ Purely dermal spindle cell lipoma and pleomorphic lipoma represent ill-defined, infiltrative lesions, show a broad anatomic distribution, and no gender preference.
■ Spindle-cell lipoma is composed of mature adipocytes and CD34+, bland spindled cells; multinucleated, CD34+ giant cells are present in pleomorphic lipoma.
■ Atypical spindle cell lipomatous tumor and atypical pleomorphic lipomatous tumor represent intermediate, locally aggressive, nonmetastasizing neoplasms.
EPIDEMIOLOGY
EPIDEMIOLOGY
Spindle-cell lipoma and pleomorphic lipoma form a morphologic spectrum of a single clinicopathologic entity with significant clinical, morphologic, and cytogenetic overlap. The majority of these rare neoplasms are seen in elderly males; very rarely have familial spindle-cell lipomas with multiple lesions in the affected patients have been reported.22 In contrast, purely dermal lipomas show no gender preference.23
CLINICAL FEATURES
CLINICAL FEATURES
Spindle-cell lipoma and pleomorphic lipoma usually present as an asymptomatic, often longstanding, mobile tumor in the subcutaneous tissue. The majority of these lesions are seen on the posterior neck, shoulder, and upper back. Infrequently, the face, oral cavity, and extremities are affected.24,25 Purely dermal spindlecell lipoma and pleomorphic lipoma show a broad anatomic distribution.23
2179
20
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The karyotype of spindle-cell and pleomorphic lipomas is complex and frequently hypodiploid with frequent partial losses and few balanced rearrangements. Many cases show monosomy and partial losses involving chromosomes 13 and 16.3 Given the overlapping clinical, histologic, and molecular features between spindle-cell lipoma, cellular angiofibroma, and mammary-type myofibroblastoma, these tumors probably represent points along a spectrum of a single clinicopathologic entity.26,27
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Subcutaneous spindle-cell lipoma represents an encapsulated lesion composed of mature adipocytes and a variable number of cytologically bland spindled tumor cells set in a collagenous and myxoid stroma containing blood vessels, hyalinized rope-like collagen fibers and, often, mast cells (Fig. 122-13). Mitotic activity is virtually absent. The spindled cells can predominate, and
A
B
2180
even cases without lipogenic cells have been reported that may cause significant diagnostic problems (Fig. 122-14).28 Occasionally, prominent myxoid stromal changes are seen, and numerous slit-like spaces resembling vascular channels are present in the so-called pseudoangiomatous variant (Fig. 122-15).29
A
B
A
B
Scattered lipoblasts may be present in otherwise typical cases of spindle-cell lipoma. The characteristic feature of pleomorphic lipoma is the additional presence of multinucleated giant cells with radially arranged nuclei (floret-like giant cells; Fig. 122-16); both lowfat and fat-free pleomorphic lipomas also have been reported.30 Purely dermal cases of spindle-cell lipoma
20
and pleomorphic lipoma are in contrast unencapsulated and infiltrative mimicking a more aggressive neoplasm (Fig. 122-17). Infrequently, cases of spindlecell lipoma and pleomorphic lipoma arise at unusual anatomic sites and show an infiltrative pattern and significant atypia of lipogenic cells, as well as of spindled and pleomorphic giant cells (Fig. 122-18). These cases are designated as atypical spindle cell lipomatous
A
B
C
2181
20
tumor and atypical pleomorphic lipomatous tumor, and show a clinical behavior comparable to atypical lipomatous tumor.31,32,32A,32B Immunohistochemically, spindled cells and pleomorphic tumor giant cells stain positively for CD34 (Fig. 122-19), and show loss of the expression of Rb-1 (Fig. 122-20).33 Very rarely an expression of desmin and S-100 protein by spindled cells has been reported.34,35
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Atypical lipomatous tumor shows striking variation of size and shape of the lipogenic cells and significant atypia with the presence of enlarged and hyperchromatic nuclei. In addition, a focal nuclear expression of MDM2 and CDK4 may be seen; FISH analysis reveals MDM2 and CDK4 amplification. Cases of solitary fibrous tumor may contain fat cells and tumor cells stain positively for CD34 as well. However, solitary fibrous tumor is characterized by a varying cellularity,
2182
the presence of hemangiopericytoma-like blood vessels, and tumor cells that show nuclear expression of STAT6. Dermatofibrosarcoma protuberans is composed of CD34+ spindled cells, however, these neoplasms show a diffuse, honey-comb infiltration of the subcutaneous tissue and different genetic changes.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Spindle-cell and pleomorphic lipomas are entirely benign, although local recurrences occur rarely. Cases of atypical spindle cell lipomatous tumor and pleomorphic lipomatous tumor are locally aggressive neoplasms and show an increased rate of local recurrences.31,32
CHONDROID LIPOMA
AT-A-GLANCE
■ Chondroid lipoma represents a rare benign lipogenic neoplasm.
■ Chondroid lipoma is seen more frequently in female patients.
■ Chondroid lipoma arises predominantly in deep soft tissues of the extremities.
■ Chondroid lipoma is composed of adipocytes, lipoblasts, and small vacuolated cells.
■ Tumor cells in chondroid lipoma are set in a myxoid–chondroid matrix.
■ A recurrent t(11;16)(q13;p13) is seen in cases of chondroid lipoma.
EPIDEMIOLOGY
EPIDEMIOLOGY
Chondroid lipoma, first described in 1993,36 is a very rare lipogenic neoplasm and arises predominantly in adults, with a predilection for females.
CLINICAL FEATURES
CLINICAL FEATURES
The majority of cases of chondroid lipoma presents as a painless, deep-seated mass, and may show a history of recent growth. The proximal extremities and limb girdles are the most frequently affected anatomic sites,36,37 but the trunk and the head and neck region, including the oral cavity,38 also may be affected. The neoplasms arise usually in deep subcutaneous tissue, fascia, and skeletal muscle.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Ultrastructural studies confirmed the lipogenic differentiation in cases of chondroid lipoma, and a spectrum of differentiation ranging from primitive mesenchymal cells, with features of prelipoblasts, to lipoblasts, preadipocytes, and mature adipocytes, has been reported.36,39 Cytogenetically, a balanced translocation involving chromosomes 11 and 16, t(11;16)(q13;p12-13) with a C11orf95-MKL2 fusion gene product has been found,40 and cyclin D1 (CCND1) expression without abnormalities of the CCND1 locus has been reported.41
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Chondroid lipomas are usually deep-seated, wellcircumscribed, encapsulated, nodular, and lobulated neoplasms. The neoplasms are composed of a variable admixture of mature adipocytes, multivacuolated lipoblasts with enlarged and hyperchromatic nuclei, and small, round cells containing an eosinophilic and vacuolated cytoplasm displaying a range of lipoblastic differentiation and containing small lipid droplets and periodic acid–Schiff–positive glycogen (Figs. 122-21, 122-22, and 122-23). The tumor cells are set in a myxoid–chondroid stroma and positive Alcian blue stainings at low pH indicate the presence of sulfated chondroitin. The lesions contain many vessels, and areas of hemorrhage, fibrosis, and calcification may be present. Mature lipogenic cells stain positively for S-100 protein, and, occasionally, a focal expression of pancytokeratin by lipogenic cells can be seen.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Given the depth and size of the lesion associated with the presence of nuclear atypia and lipoblasts,
20
benign chondroid lipoma has to be distinguished from more aggressive neoplasms, including atypical lipomatous tumor, myxoid liposarcoma, extraskeletal myxoid chondrosarcoma, and myoepithelioma of soft tissues.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Chondroid lipoma represents an entirely benign lipogenic neoplasm and simple surgical excision is curative. Local recurrences are rare and neither malignant transformation nor metastases have been reported as of this writing.
2183
20
MYOLIPOMA
AT-A-GLANCE
■ Myolipoma is a very rare benign mesenchymal neoplasm of deep soft tissue.
■ Myolipoma occurs predominantly in females.
■ Myolipoma is composed of an irregular mixture of mature adipocytes and smooth muscle cells.
EPIDEMIOLOGY
EPIDEMIOLOGY
Myolipoma represents a very rare neoplasm of soft tissues occurring in adult patients with a female predominance.42
CLINICAL FEATURES
CLINICAL FEATURES
Cases of myolipoma tend to occur in deep soft tissue of the retroperitoneum, abdominal cavity, and inguinal region, whereas an involvement of subcutaneous tissue of the extremities and the trunk is only rarely seen.42 Although these lesions may reach a considerable size, they are often found incidentally.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
HMGA2 alterations have been reported in cases of myolipoma, and most recently a fusion of the HMGA2 and C9orf92 genes with t(9;12)(p22;q14) has been detected.43
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Myolipoma of soft tissues is a well-circumscribed or encapsulated lesion composed of fascicles of cytologically bland smooth muscle cells associated with a variable amount of mature fat (Fig. 122-24). No cytologic atypia, mitoses, or thick-walled vessels are present. Immunohistochemically, smooth muscle cells stain positively for alpha-smooth muscle actin, desmin, and h-caldesmon (Fig. 122-25), and an expression of estrogen and progesterone receptors has been reported.44
No expression of HMB-45 by smooth muscle cells and no expression of MDM2 and CDK4 by lipogenic cells are noted.
2184
A
B
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
The differential diagnosis for myolipoma of soft tissues includes atypical lipomatous tumor, dedifferentiated liposarcoma, well-differentiated leiomyosarcoma, and angiomyolipoma.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Despite the large size, myolipoma of soft tissues represents an entirely benign mesenchymal neoplasm, and complete excision is curative.
HIBERNOMA
AT-A-GLANCE
■ Hibernoma represents a benign neoplasm of brown fat.
■ Hibernoma usually arises in adults and the most common anatomic site is the thigh.
■ Cases of atypical lipomatous tumor and myxoid liposarcoma may contain hibernoma-like areas.
EPIDEMIOLOGY
EPIDEMIOLOGY
Hibernoma is a rare neoplasm, and occurs predominantly in young adults, whereas it is only rarely seen in children and the elderly. Males are slightly more frequently affected than females.
CLINICAL FEATURES
CLINICAL FEATURES
Hibernoma represents a painless, slowly growing, mobile tumor arising in the subcutis or in deep soft tissues. The most common anatomic site for hibernoma is the thigh followed by the trunk, the chest wall, the shoulder area, the upper extremity, and the head and neck area.45 Rarely, hibernoma arises intraabdominally, in the retroperitoneum, in the mediastinum, or intraosseous.46,47
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The reported karyotypes of hibernoma appear to be more complex than those in other benign lipogenic
20
neoplasms, and structural rearrangements involving chromosome band 11q13-21 have been detected.48
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Hibernomas are well-circumscribed, lobular neoplasms containing a capillary network and are composed of a variable number of brown fat cells admixed with white fat cells and stromal cells. Typical hibernomas are composed of large, polygonal, brown fat cells with multivacuolation, granular cytoplasm, and a small, centrally located nucleus admixed with mature white fat cells (Fig. 122-26). The eosinophilic variant is composed of predominantly brown fat cells with a deeply eosinophilic and granular cytoplasm, the pale cell variant contains mostly large brown fat cells with palely staining vacuolated cytoplasm, and the mixed subtype is intermediate between the two. In addition, myxoid, spindle-cell, and lipoma-like variants are known.45
Prominent cytologic atypia and increased proliferative activity are not present. Immunohistochemically,
A
B
2185
20
tumor cells stain positively for S-100 protein and for uncoupling protein, a protein unique to brown adipocyte mitochondria.49 The spindled cells may express CD34.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Scattered brown fat cells as well as hibernoma-like areas may be present in cases of myxoid liposarcoma and atypical lipomatous tumor that have to be distinguished from hibernoma. Further differential diagnoses include granular cell tumor and spindle-cell lipoma.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Hibernoma is an entirely benign lipogenic neoplasm, and complete excision is curative.
ATYPICAL LIPOMATOUS TUMOR AND WELL- DIFFERENTIATED LIPOSARCOMA
AT-A-GLANCE
■ Atypical lipomatous tumor and well-differentiated liposarcoma are synonyms and describe lipogenic neoplasms with identical morphologic and cytogenetic features.
■ Atypical lipomatous tumor represents a locally aggressive, nonmetastasizing neoplasm.
■ Anatomic location, size, and depth of the lesions are important prognostic predictors.
■ Neoplasms arising at sites amenable to surgical excision (ie, extremities) show a low rate of local recurrence, risk of dedifferentiation, and mortality.
■ In striking contrast, neoplasms arising in the retroperitoneum, intraabdominal cavity, or in paratesticular location, where complete excision is difficult or not achievable, are characterized by a high rate of local recurrence, a high risk of dedifferentiation, and a poor clinical outcome.
■ The known morphologic variants have no prognostic value.
2186
EPIDEMIOLOGY
EPIDEMIOLOGY
Atypical lipomatous tumor represents the largest single group of clinically aggressive lipogenic neoplasms, and liposarcomas in general are the most frequent sarcomas in adults. The majority of neoplasms occurs in middle-age adults, with a peak incidence in the sixth decade.50-54 Cases in children are extremely rare, but have been described.55,56
CLINICAL FEATURES
CLINICAL FEATURES
Cases of atypical lipomatous tumor occur usually in deep soft tissues. The subcutaneous tissue may be occasionally involved, but purely dermal lesions that may present as a skin tag are extremely rare (Fig. 122-27).57
The predominantly affected site is the musculature of the extremities, especially the thigh, followed by the
A
B
retroperitoneum, the abdominal cavity, the groin, the paratesticular region, and the mediastinum. However, also other anatomic locations are rarely involved, as it is the oral cavity, the orbit, the larynx, and the vulva.58-61 An enlarging painless mass is the typical presenting sign and tumors may grow to a very large size before becoming symptomatic, especially in retroperitoneal and intraabdominal locations.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Cases of atypical lipomatous tumor are characterized cytogenetically by supernumerary ring and giant marker chromosomes derived from the 12q13-15 region and resulting in consistent amplification of the MDM2 and CDK4 genes.62,63
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Atypical lipomatous tumors are typically large, wellcircumscribed and lobulated lesions, and in retroperitoneal and intraabdominal locations, multiple discontinuous neoplasms may be present. Morphologically, atypical lipomatous tumor can be divided into 3 main subtypes; however, especially in large neoplasms of the retroperitoneum, more than 1 variant may be present. The most frequent adipocytic (lipoma-like) variant is composed of relatively mature adipocytic cells with marked variations in size and shape showing scattered enlarged and hyperchromatic nuclei. In addition, atypical stromal cells with enlarged nuclei located in fibrous septa, as well as multivacuolated lipoblasts, may be present; however, lipoblasts may be entirely absent (Fig. 122-28). The second most frequent sclerosing variant that is frequently seen in the retroperitoneal and paratesticular locations is characterized by the presence of enlarged stromal cells with large and hyperchromatic nuclei set in a paucicellular, fibrillary, collagenous stroma, and scattered atypical lipogenic cells and lipoblasts (Fig. 122-29). Rare, inflammatory atypical lipomatous tumors are mainly seen in retroperitoneal and intraabdominal locations, and show a prominent inflammatory infiltrate that mimics features of a lymphoma or an inflammatory pseudotumor.64 So-called well-differentiated spindlecell liposarcoma65 shows a predilection for the subcutaneous tissue of the shoulder girdle and the limbs and is composed of slightly atypical spindled cells with enlarged, hyperchromatic nuclei arranged in fascicles and whorls set in a fibrous and/or myxoid stroma associated with atypical adipocytic cells. Genetic studies emphasize that these neoplasms most likely represent atypical spindle cell lipomatous tumor with a clinical behavior almost identical to atypical lipomatous tumor.31,32,66 Very rarely, a heterologous differentiation with osseous or myogenic elements is seen. The term
20
A
B
C
lipoleiomyosarcoma has been applied to lesions showing morphologic features of atypical lipomatous tumor and well-differentiated leiomyosarcoma.67 Immunohistochemically, focal expression of p16, as well as nuclear staining for MDM2 and/or CDK4, is helpful in the differential diagnoses to other lipogenic and nonlipogenic lesions. However, especially, very welldifferentiated examples of atypical lipomatous tumor
2187
20
A
B
may not show MDM2 and/or CDK4 expression by immunohistochemistry. In these cases, FISH analysis may be very helpful.68,69
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
In contrast to atypical lipomatous tumor, typical cases of lipoma are composed of mature adipocytes without nuclear atypia and lipoblasts, and do not stain positively for p16, MDM2, and CDK4. However, traumatized lipomas may contain numerous histiocytes with enlarged nuclei that show a cytoplasmic staining for p16, MDM2, and CDK4, and may mimic a more aggressive neoplasm. Lipoblastoma is composed of a varying number of lipoblasts and may stain positively for p16,18 but the presence of a lobular lesion with characteristic septa, and the lack of MDM2/CDK4 expression are of help in the differential diagnosis. Spindle-cell lipoma and pleomorphic lipoma may contain scattered lipoblasts, but lack atypia, and neoplastic cells are negative for MDM2 and/or CDK4. Dedifferentiated liposarcoma contains a nonlipogenic component with strong expression of p16, MDM2, and CDK4. Angiomyolipoma is characterized by the presence of thick-walled blood
2188
vessels and a perivascular myogenic component staining positively for myogenic marker and HMB-45. Rare cases of massive localized lymphedema simulate clinically and histologically atypical lipomatous tumor,70 but no significant atypia and no expression of p16, MDM2, and CDK4 are noted in these lesions.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
The clinical behavior and the prognosis of atypical lipomatous tumor is strongly dependent on the anatomic site, the depth, and the size of the neoplasms. Surgical treatment is curative for lesions arising superficially, and at surgically amenable anatomic sites such as the extremities. The estimated rate of progressing to dedifferentiated liposarcoma is less than 2% with a mortality rate of virtually zero for cases arising at these anatomic locations. In striking contrast, cases of atypical lipomatous tumor arising in deep soft tissues of the retroperitoneum, the mediastinum, intraabdominal cavity, and paratesticular location, where complete surgical excision is problematic and not possible, tend to recur locally, may cause death as a result of uncontrolled local effects, and have a risk of dedifferentiation of more than 20%. The overall mortality of atypical lipomatous tumor in the retroperitoneum is more than 80%.53,71 Surgical excision is the primary therapeutic approach in cases of atypical lipomatous tumor; adjuvant chemotherapy and radiotherapy may be used in advanced cases.
DEDIFFERENTIATED LIPOSARCOMA
AT-A-GLANCE
■ Dedifferentiated liposarcoma represents the morphologic form of progression of atypical lipomatous tumor.
■ Dedifferentiated liposarcoma most frequently occurs in the retroperitoneum and intraabdominal cavity as a large tumor mass.
■ An abrupt or gradual transition from an atypical lipomatous tumor to a nonlipogenic sarcomatous component is seen in dedifferentiated liposarcoma.
■ The nonlipogenic component shows a variable morphology, and a heterologous differentiation is seen in a significant number of cases.
■ Dedifferentiated liposarcoma shows the same karyotypic changes as atypical lipomatous tumor.
■ Dedifferentiated liposarcoma is best regarded as an intermediate-grade sarcoma (grade 2 of malignancy).
EPIDEMIOLOGY
EPIDEMIOLOGY
Dedifferentiated liposarcoma represents the most common pleomorphic sarcoma in the retroperitoneum, and typically affects adult patients in the sixth decade.72 Dedifferentiation as a morphologic form of tumor progression represents a time-dependent phenomenon, and occurs in approximately 90% of cases as a de novo presentation, whereas 10% develop it in a local recurrence.
CLINICAL FEATURES
CLINICAL FEATURES
The majority of dedifferentiated liposarcomas occur in the retroperitoneum, intraabdominal, and paratesticular locations, whereas an involvement of deep soft tissues of the extremities is seen more rarely. Other rare locations include the trunk, and the head and neck region, presentation in subcutaneous tissue is very rare.73 Typically, cases of dedifferentiated liposarcoma present as a large painless mass, and are found in the retroperitoneum and intraabdominal locations by chance. A recent increase in size of a longstanding deep-seated mass in the extremities may indicate dedifferentiation in an atypical lipomatous tumor.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The karyotypic findings in dedifferentiated liposarcoma are similar to those seen in atypical lipomatous tumor; however, coamplification involving 1p32 and 6q23 with activation of the JUN and ASK2 genes has been reported.74
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
Histologically, an abrupt or gradual transition from areas showing features of atypical lipomatous tumor to nonlipogenic sarcoma areas is characteristic for dedifferentiated liposarcoma (Fig. 122-30). The extent and the morphology of the nonlipogenic component are variable, but in most cases, the dedifferentiated component shows features of a high-grade, undifferentiated, pleomorphic sarcoma (Fig. 122-31). Especially in the retroperitoneum and intraabdominal locations, intermediate-grade or high-grade myxofibrosarcoma areas are present. Occasionally, a low-grade dedifferentiation is noted that mimics features of low-grade fibrosarcoma or desmoid fibromatosis (Fig. 122-32). Heterologous differentiation is seen in approximately 10% of cases, and most often a myogenic or osteosarcomatous/chondrosarcomatous differentiation is detected (Fig. 122-33). More rarely angiosarcomatous
20
2189
20
and meningothelial-like whorls have been reported.75
Interestingly, the dedifferentiated component may show a lipoblastic differentiation that resembles pleomorphic liposarcoma, but molecular changes are identical to classical dedifferentiated liposarcoma.76
Immunohistochemically, a strong expression of p16, MDM2, and CDK4 is seen, especially in the nonlipogenic component (Fig. 122-34). Heterologous myogenic differentiation is reflected by positive staining for myogenic (actin, desmin, h-caldesmon, myogenin), osteosarcomatous (SATB2), chondrosarcomatous (S-100 protein), or angiosarcomatous (CD31, ERG) immunohistochemical markers (Fig. 122-35).
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Given the variable morphology of the nonlipogenic component, the differential diagnosis of dedifferentiated liposarcoma is broad and includes pleomorphic liposarcoma, myxofibrosarcoma, GI stromal tumor, leiomyosarcoma, rhabdomyosarcoma, malignant solitary fibrous tumor, rare fibrosarcoma, and desmoid fibromatosis. In addition, large lipomas with cytologic atypia and atypical spindle cell lipomatous tumor and atypical pleomorphic lipomatous tumor have to be considered, especially when dealing with a small biopsy.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Dedifferentiated liposarcoma is characterized by a protracted clinical course with a high risk for local recurrences and a locally aggressive growth. Almost all cases arising in the retroperitoneum and intraabdominal locations recur if followed long enough. However, in contrast to many other high-grade sarcomas, the
2190
A
B
overall risk of distant metastatic spread is estimated at approximately 15% to 20%.72,77 It can be speculated that the absence of complex karyotypic aberrations and the rarity of p53 mutations in cases of dedifferentiated
liposarcoma78 may explain the better outcome. As in cases of atypical lipomatous tumor, the anatomic location is the most important prognostic factor in dedifferentiated liposarcoma, and cases arising in retroperitoneum and intraabdominal locations are associated with a poor prognosis. It has been shown that myogenic differentiation and the histologic grade of the nonlipogenic tumor component are important prognostic parameters.79 The extent of dedifferentiation is prognostically not predictive. Complete surgical removal represents the treatment of choice; however, especially in the retroperitoneum and in intraabdominal locations, this is often impossible. New therapeutic options targeting the gene products of chromosome 12 or inhibitors of the Akt-mTOR and MAPK (mitogenactivated protein kinase) pathways are under discussion for use in nonresectable cases.80,81
MYXOID LIPOSARCOMA
AT-A-GLANCE
■ Myxoid liposarcoma usually occurs in deep soft tissues of the extremities, particularly the thigh, of middle-aged adults.
■ Myxoid liposarcoma is composed of small, primitive, mesenchymal cells and lipoblasts in varying stages of differentiation with a characteristic vascular pattern.
■ The presence of a round cell component is of adverse significant prognostic importance.
■ Myxoid liposarcoma is characterized by FUS-DDIT3 or EWSR1-DDIT3 rearrangements.
EPIDEMIOLOGY
EPIDEMIOLOGY
Myxoid liposarcoma represents the second most frequent variant of liposarcoma and approximately 5% of all soft-tissue sarcomas in adults. Most cases of myxoid liposarcoma arise in young to middleaged adults; however, a significant number of cases are seen in children and adolescents, representing the most frequent variant of liposarcoma in this age group, and these cases may show unusual morphologic features.82 In addition an expression of cancer testis antigens, ie, PRAME is seen.82A
CLINICAL FEATURES
CLINICAL FEATURES
Cases of myxoid liposarcoma present as a large, painless mass in deep soft tissues of the extremities, and the majority of neoplasms arise on the thigh. Only rarely, myxoid liposarcoma is seen in the subcutis and in the retroperitoneum or intraabdominal locations. The monoclonal origin of cases multifocal myxoid liposarcoma confirms an unusual metastatic pattern in these cases.83
20
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Cytogenetically, myxoid liposarcoma is characterized by a recurrent translocation t(12;16)(q13;p11) with FUS-DDIT3 fusion in the majority of cases; more rarely, a t(12;22)(q13:q12) with EWSR1-DDIT3 fusion is present.84,85
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
The nodular neoplasms are composed of an admixture of uniform, cytologically bland, small, oval, mesenchymal tumor cells, and small, univacuolated or bivacuolated lipoblasts set in a prominent myxoid stroma with microcystic spaces and characteristic branching, thin-walled blood vessels (Fig. 122-36). These well-differentiated neoplasms lack significant cytologic atypia, mitoses, and tumor necrosis. Myxoid/ round-cell liposarcoma, and predominantly roundcell liposarcoma, is characterized by progression to more cellular areas containing enlarged round tumor cells with enlarged and overlapping round nuclei (Fig. 122-37). Rarely, myxoid liposarcoma may show prominent adipocytic differentiation mimicking morphologic features of atypical lipomatous tumor (Fig. 122-38),86 which also has been reported in cases treated with neoadjuvant therapy.87 In addition, cases of myxoid liposarcoma may show a prominent spindlecell component (spindle-cell myxoid liposarcoma) or a pleomorphic component (pleomorphic myxoid liposarcoma), and these features are mainly seen in young patients.82 Immunohistochemically, S-100 protein is variably positive in the high-grade, round-cell component.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
The differential diagnosis includes benign lesions as lipoblastoma and chondroid lipoma, as well as malignant neoplasms of different lines of differentiation (myxofibrosarcoma, low-grade fibromyxoid sarcoma, extraskeletal myxoid chondrosarcoma, myxoid malignant melanoma).
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Myxoid liposarcoma tends to recur and may develop distant metastases in up to 40% of patients, and metastases at unusual locations in soft tissues or bone often are observed. Patients with “multifocal” disease at
2191
20
A
B
C
presentation have a poor prognosis, and adverse histologic features include the presence of a round-cell differentiation (>5%), tumor necrosis, p53 overexpression, and CDKN2A aberrations.88,89 It has been shown that advanced cases of myxoid liposarcoma can be treated successfully with trabectedin.90-92
2192
A
B
PLEOMORPHIC LIPOSARCOMA
AT-A-GLANCE
■ Pleomorphic liposarcoma represents a highgrade sarcoma containing a variable number of pleomorphic lipoblasts.
■ Pleomorphic liposarcoma shows a predilection for the extremities of adults.
■ Pleomorphic liposarcoma arises either de novo or represents the morphologic form of progression of atypical lipomatous tumor/dedifferentiated liposarcoma.
EPIDEMIOLOGY
EPIDEMIOLOGY
Pleomorphic liposarcoma represents the rarest subtype of liposarcoma (5%) and arises predominantly in the elderly with a slight male predominance.93,94
CLINICAL FEATURES
CLINICAL FEATURES
Clinically, pleomorphic liposarcoma usually presents as a fast growing neoplasm in deep soft tissues of the extremities (lower > upper extremities), while the trunk, the retroperitoneum, the abdominal cavity, the head and neck region, and the pelvis are only rarely involved. A small but significant number of cases of pleomorphic liposarcoma arise in subcutaneous tissues, whereas purely dermal neoplasms are exceedingly rare (Fig. 122-39).94-96
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Cytogenetically, many cases of pleomorphic liposarcoma closely resemble other pleomorphic sarcomas and show complex structural rearrangements. However, it has been shown that a small, but significant, number of cases reveal MDM2 and CDK4 amplifications, which suggests that these neoplasms represent a tumor progression from atypical lipomatous tumor/ dedifferentiated liposarcoma.76,97
HISTOLOGIC FEATURES
HISTOLOGIC FEATURES
The well-circumscribed or infiltrative neoplasms show features of a high-grade pleomorphic sarcoma
20
A
B
(high-grade fibrosarcoma or “malignant fibrous histiocytoma”) containing pleomorphic spindled cells and multinucleated tumor giant cells admixed with a variable number of pleomorphic lipoblasts. These pleomorphic lipoblasts contain enlarged and bizarre, hyperchromatic nuclei scalloped by cytoplasmic lipid droplets, and are scattered throughout the pleomorphic sarcoma or are arranged in larger sheets (Fig. 122-40). Often intracellular and extracellular eosinophilic droplets are noted. Many cases show morphologic features similar to intermediategrade or high-grade myxofibrosarcoma with scattered pleomorphic lipoblasts (Fig. 122-41). The epithelioid variant of pleomorphic liposarcoma is characterized by large, densely packed, epithelioid tumor cells with abundant eosinophilic cytoplasm and vesicular nuclei resembling renal clear cell carcinoma or adrenal cortical carcinoma.98 Immunohistochemically, tumor cells in pleomorphic liposarcoma may stain positively for actins, cytokeratins, CD34, and, rarely, desmin.
2193
20
A
B
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Dedifferentiated liposarcoma contains an atypical lipomatous tumor component and no pleomorphic lipoblasts. The presence of at least scattered pleomorphic lipoblasts in pleomorphic liposarcoma is important in the differential diagnosis to other pleomorphic, high-grade sarcomas (myxofibrosarcoma, leiomyosarcoma, rhabdomyosarcoma), as well as poorly differentiated, sarcomatoid melanoma and carcinoma.
CLINICAL COURSE, PROGNOSIS, AND TREATMENT
CLINICAL COURSE,
PROGNOSIS, AND
TREATMENT
Pleomorphic liposarcoma represents a high-grade sarcoma with a local recurrence and metastatic rate of 30-50%, and an estimated overall 5-year survival rate
2194
A
B
of 50% to 60%. The lung is the preferred metastatic site. The treatment is surgical excision with radiation and chemotherapy for advanced cases.
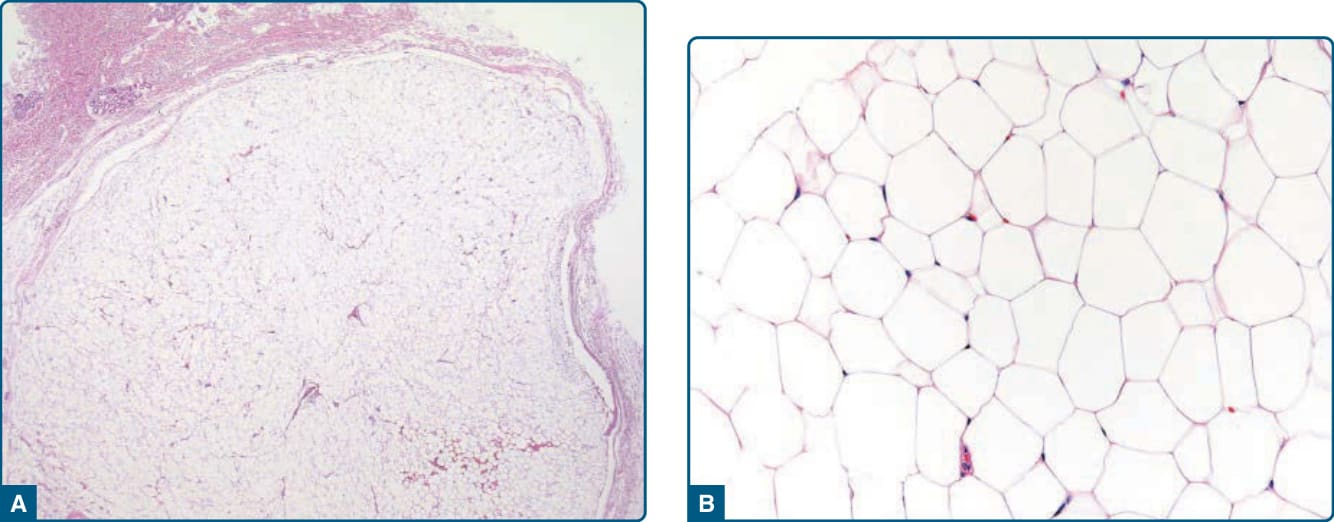
Figure 122-1 Lipoma. Subcutaneously located lipomas are well-circumscribed, often encapsulated lipogenic lesions (A), composed of mature univacuolated adipocytes showing only mild variation in size and shape (B).
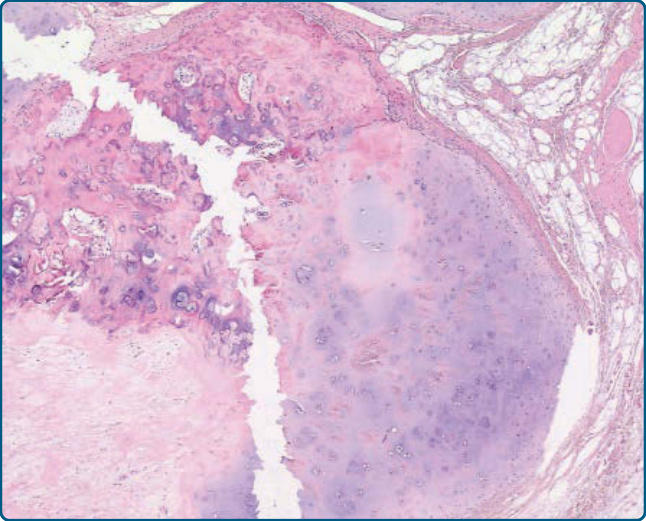
Figure 122-2 Chondrolipoma. An example of lipoma with prominent chondrous metaplasia.
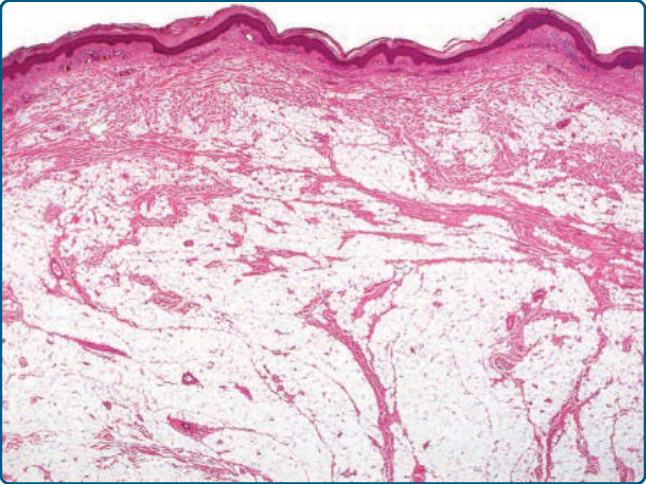
Figure 122-3 Intradermal lipoma. Mature lipogenic cells diffusely infiltrate preexisting dermal collagen bundles.
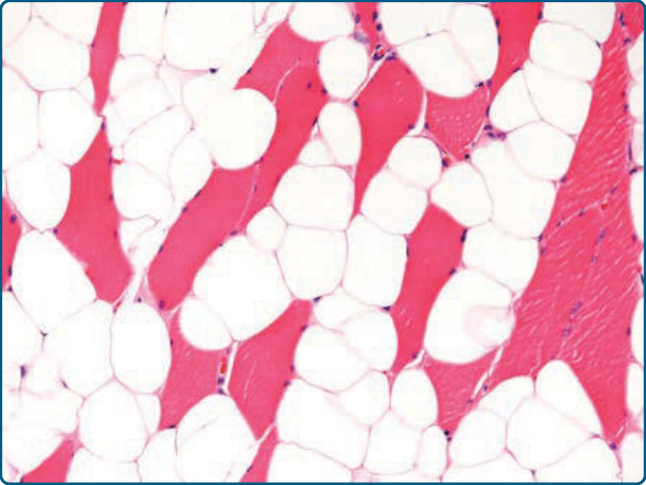
Figure 122-4 Intramuscular lipoma. Mature lipogenic cells show an infiltrative growth pattern within skeletal muscle fibers.
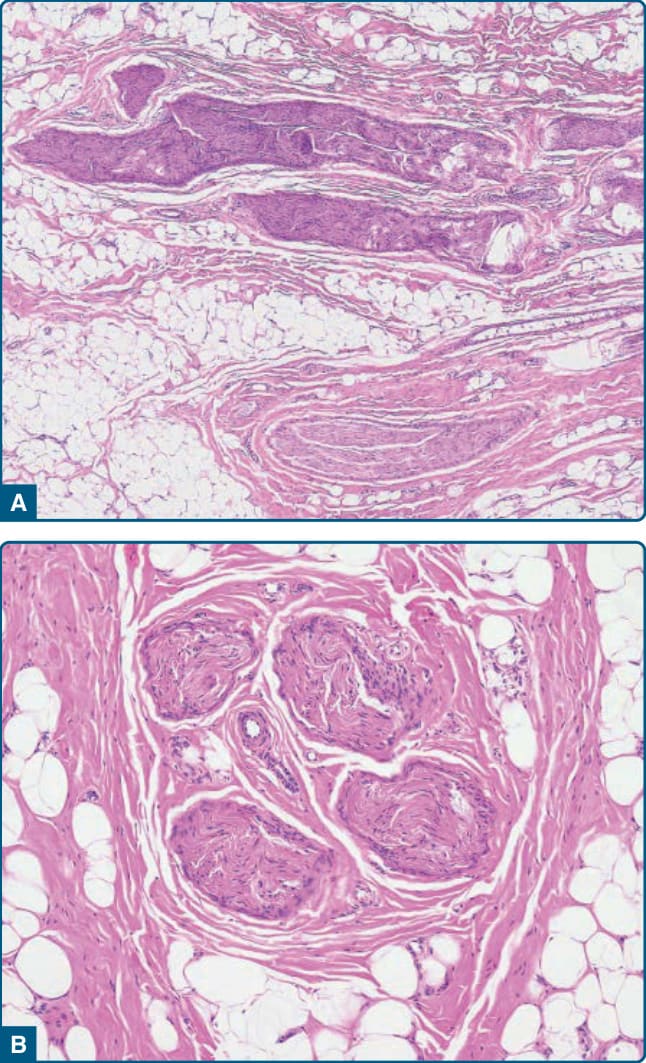
Figure 122-5 Lipomatosis of nerve. A, Epineural infiltration of lipogenic cells and collagenous fibrous tissue separating nerve bundles. B, Note the perineural fibrosis.
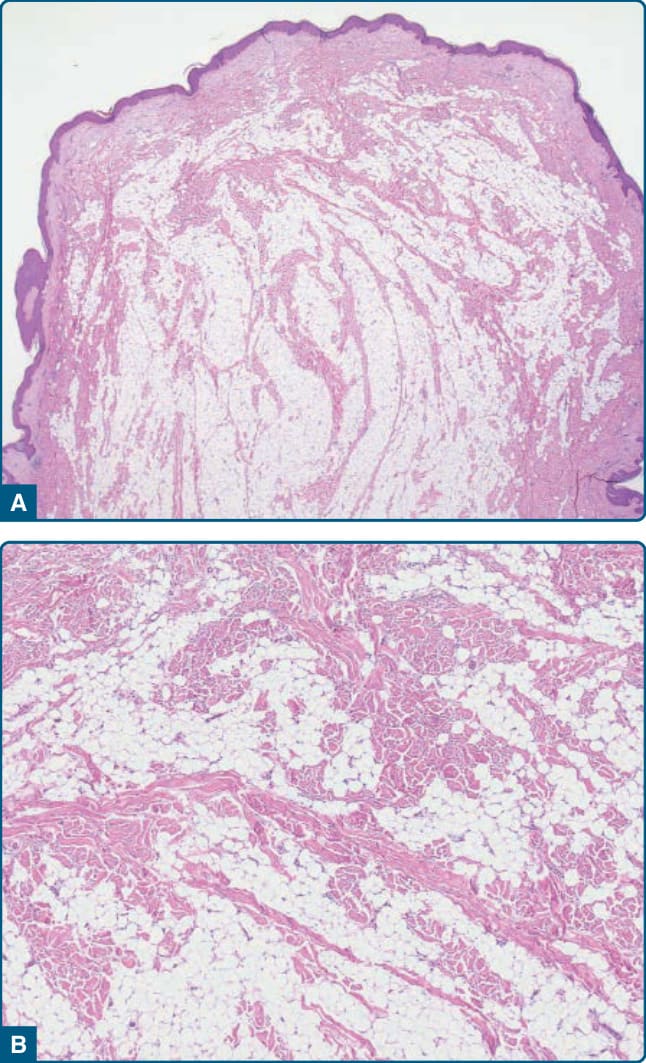
Figure 122-6 Nevus lipomatosus superficialis. Polypoid lesion with diffuse infiltration of the dermis by mature lipogenic cells (A), with typically hyalinized collagen bundles (B).
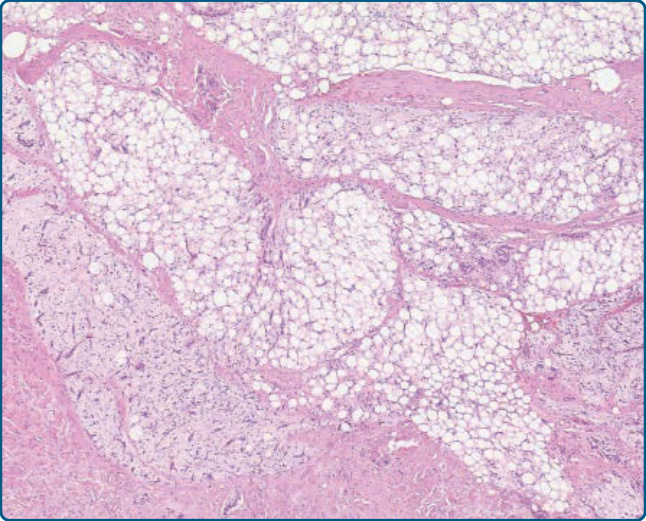
Figure 122-7 Lipoblastoma: lipoblastoma represents a well-circumscribed lipogenic neoplasm showing multilobulation and collagenous fibrous septa.
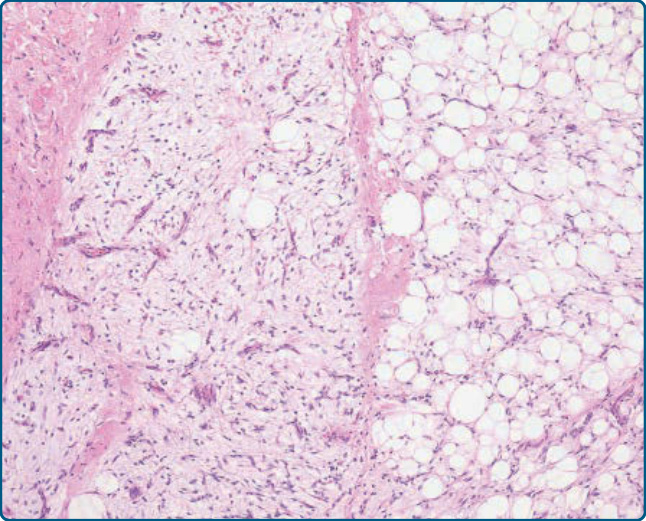
Figure 122-8 Lipoblastoma. Areas of lipogenic cells are admixed with myxoid areas showing a plexiform vascular pattern.
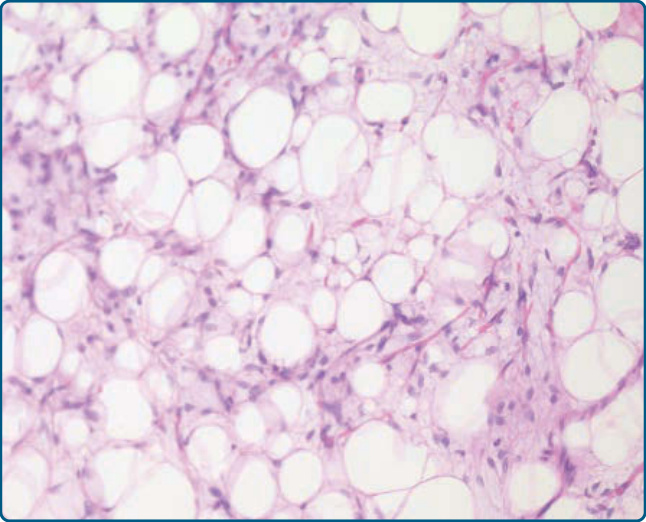
Figure 122-9 Lipoblastoma. Lipogenic cells in different stages of development are present.
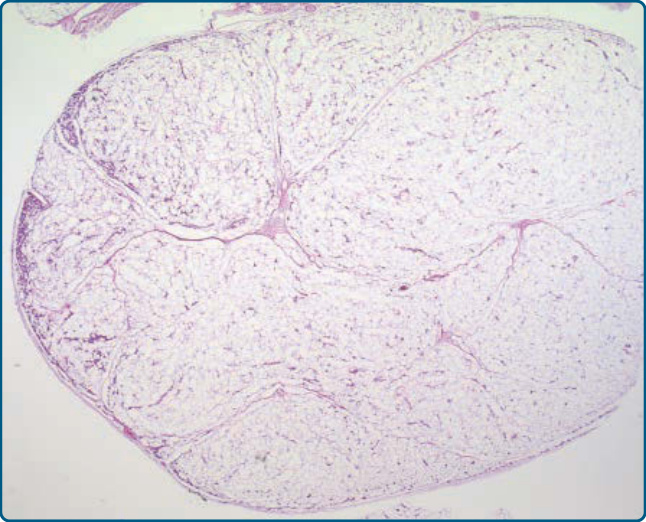
Figure 122-10 Angiolipoma. Low-power view shows an encapsulated, subcutaneously located lipogenic neoplasm with an increased number of vessels in the periphery.
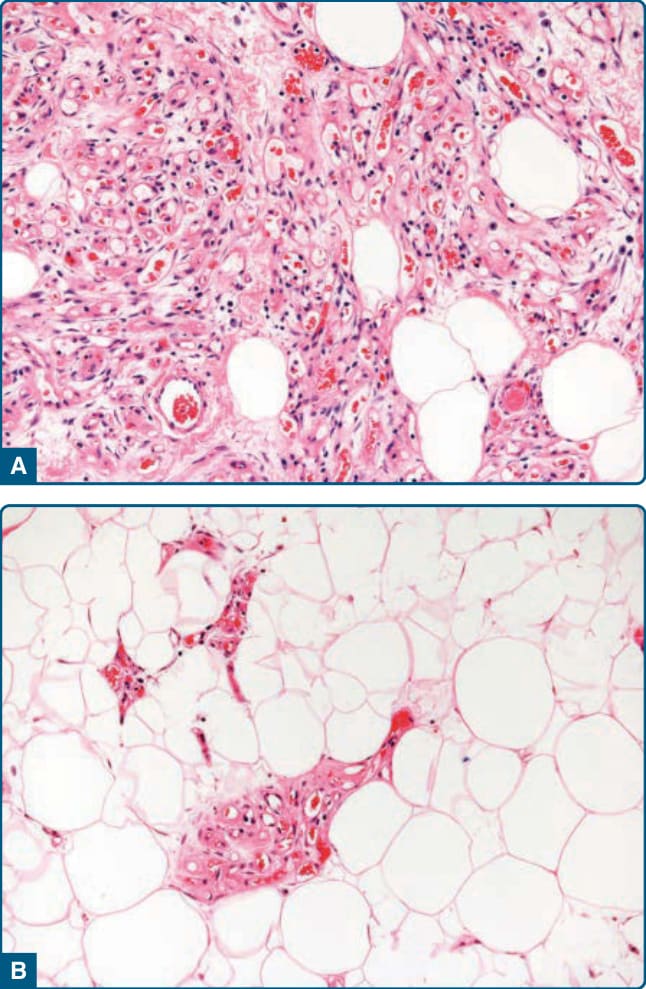
Figure 122-11 Angiolipoma. A, Narrow and dilated, thinwalled capillaries are admixed with mature adipocytic tissue. B, The adipocytic component can predominate.
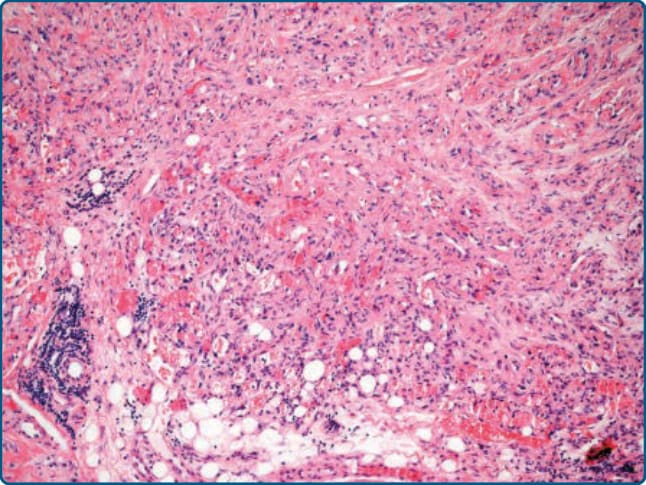
Figure 122-12 Cellular angiolipoma. Predominant vascular component mimicking a vascular neoplasm.
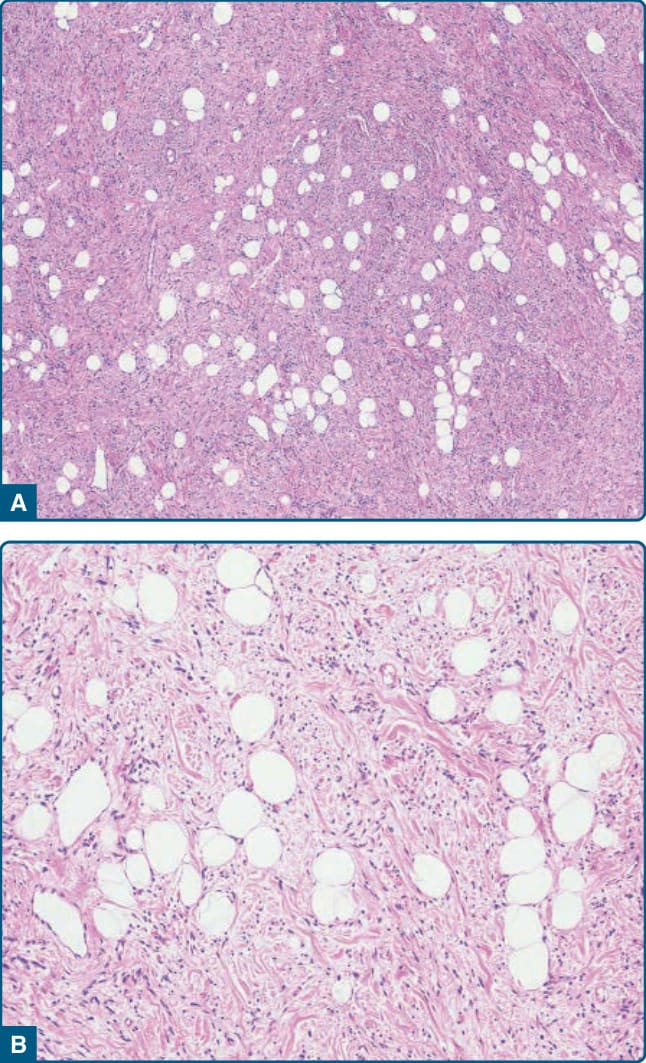
Figure 122-13 Spindle-cell lipoma. A, Mature adipocytes are admixed with short, loosely arranged spindled tumor cells. B, Hyalinized, rope-like collagen fibers are present.
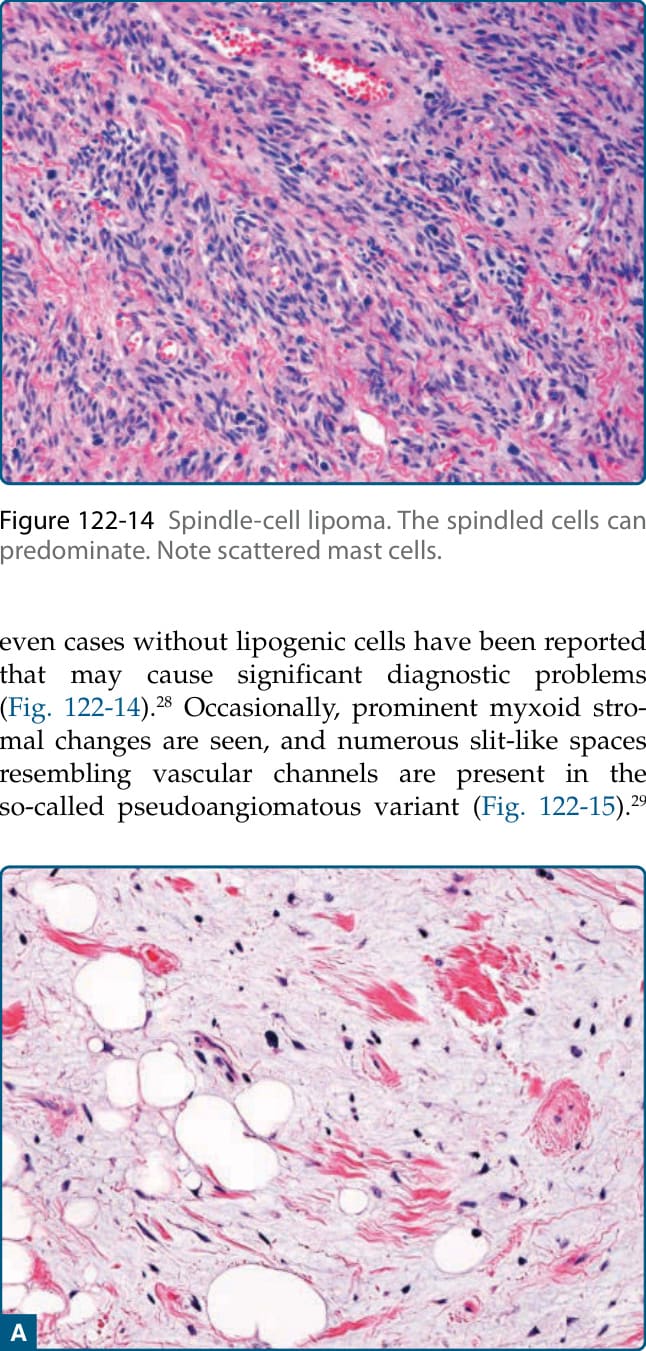
Figure 122-14 Spindle-cell lipoma. The spindled cells can predominate. Note scattered mast cells.
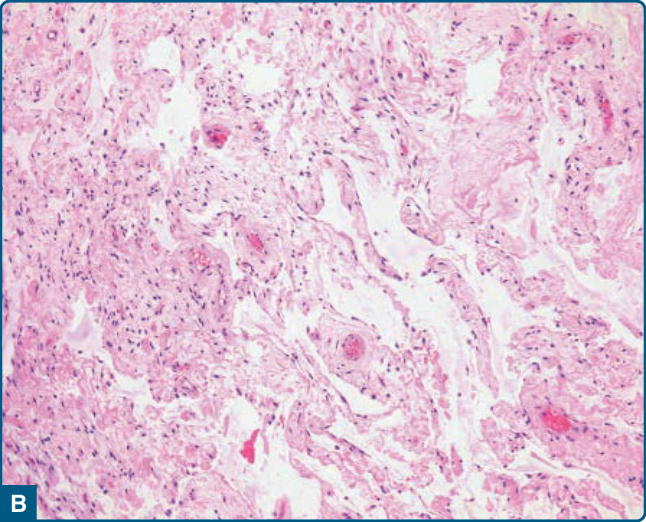
Figure 122-15 Spindle-cell lipoma. A, Prominent myxoid stromal changes; note that the tumor cell nuclei are slightly enlarged and hyperchromatic. B, Slit-like spaces are seen in the pseudoangiomatous variant.
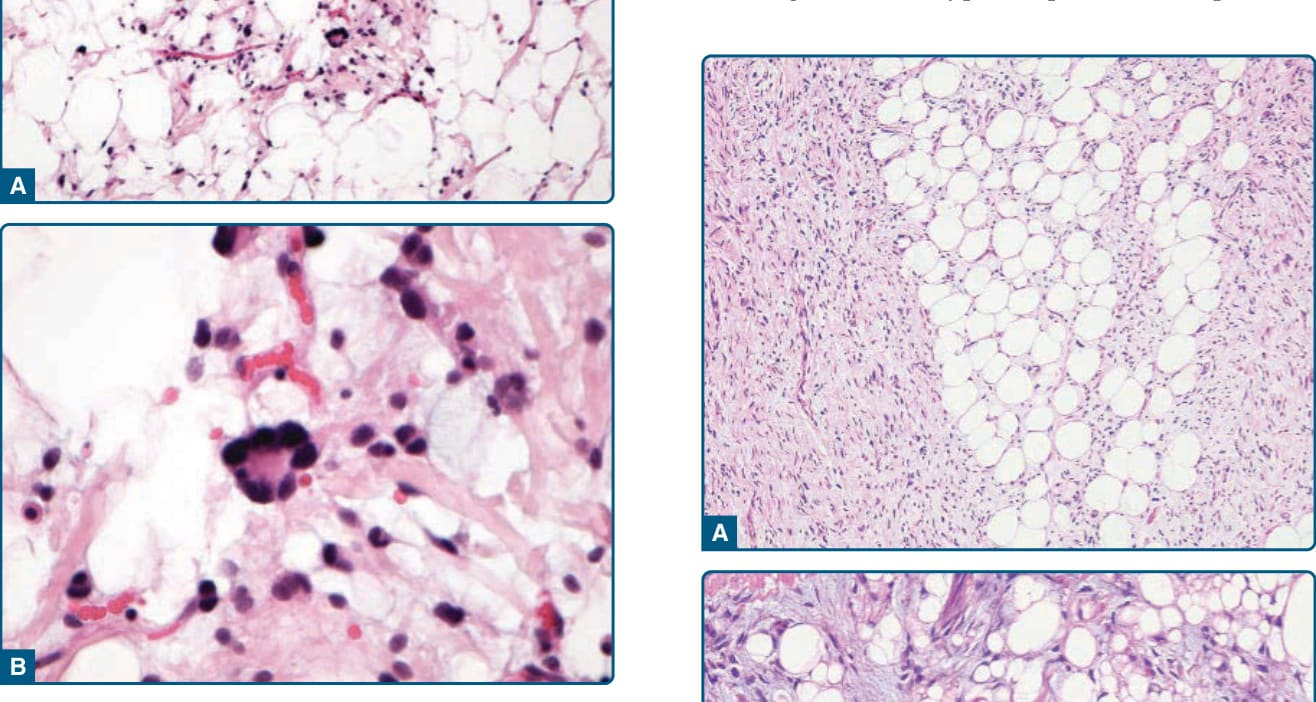
Figure 122-16 Pleomorphic lipoma. A, The characteristic floret-like multinucleated giant cells contain overlapping hyperchromatic nuclei in a circular or semicircular arrangement. B, Higher-power view of a floret-like tumor giant cell set in a myxoid stroma with scattered mast cells.
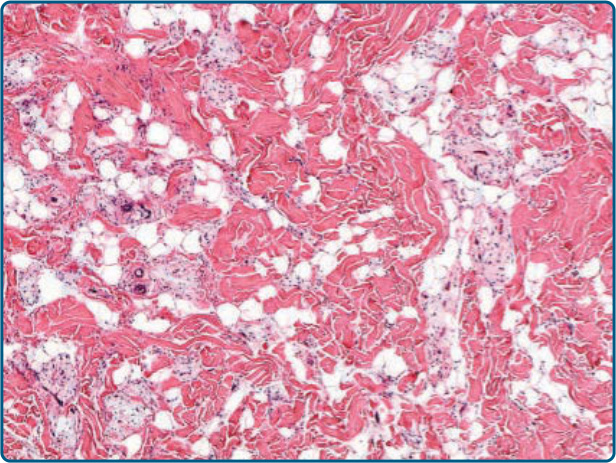
Figure 122-17 Dermal spindle-cell lipoma. Intradermal lesions are less circumscribed and show a diffuse infiltration of preexisting dermal collagen bundles.
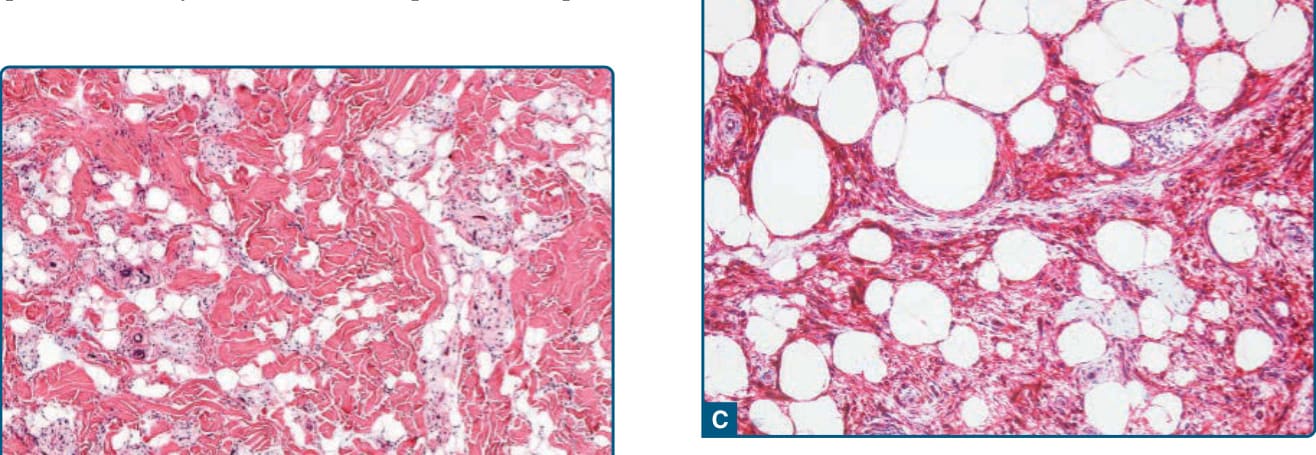
Figure 122-18 Atypical spindle cell lipoma. A, An irregular admixture of lipogenic cells with spindle-shaped tumor cells. B, Both components show at least sight nuclear atypia with enlarged and hyperchromatic nuclei; in addition lipoblastic cells are noted. C, Immunohistochemically, spindled cells stain positively for CD34.
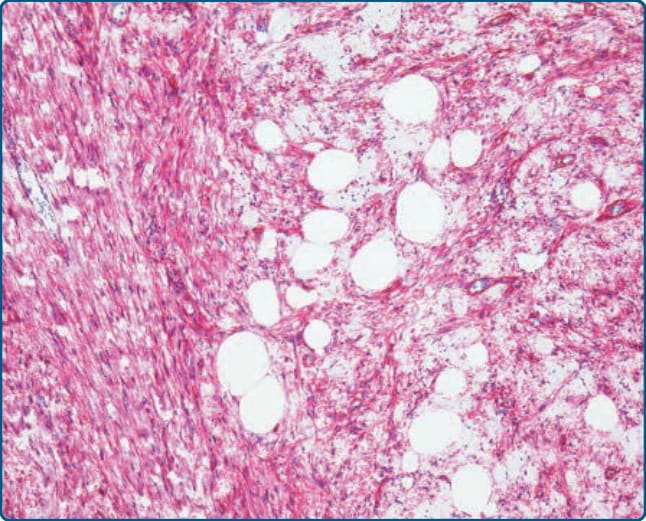
Figure 122-19 Spindle-cell lipoma Tumor cells stain positively for CD34.
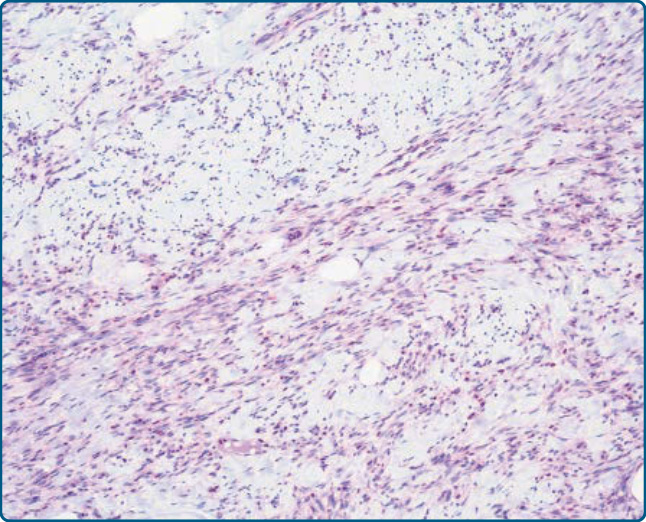
Figure 122-20 Spindle-cell lipoma. Tumor cells show loss of the expression of Rb1.
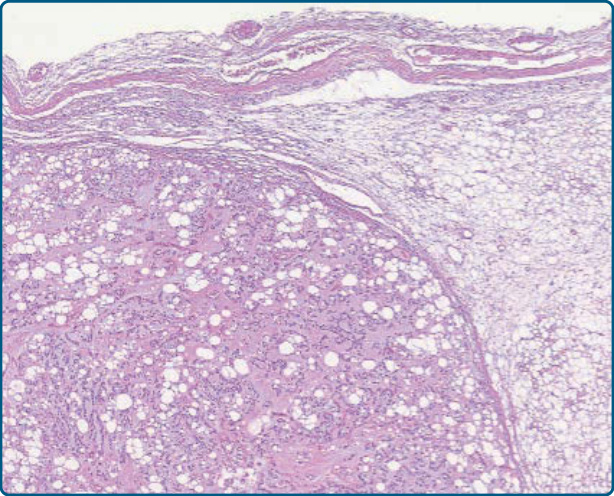
Figure 122-21 Chondroid lipoma. Encapsulated lipogenic neoplasm with a lobular growth.
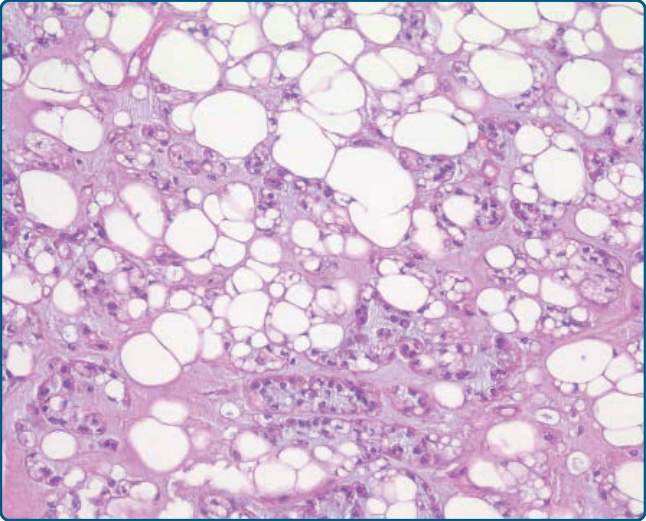
Figure 122-22 Chondroid lipoma. Univacuolated and multivacuolated lipoblasts are admixed with mature adipocytes.
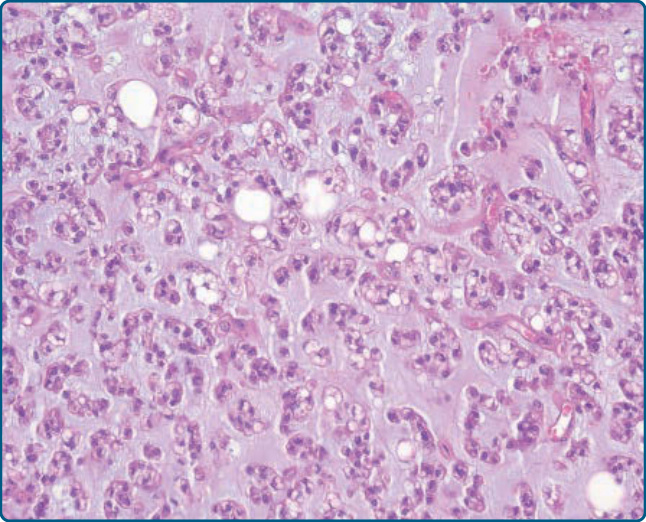
Figure 122-23 Chondroid lipoma. In addition, small, round tumor cells containing an eosinophilic and vacuolated cytoplasm are seen.
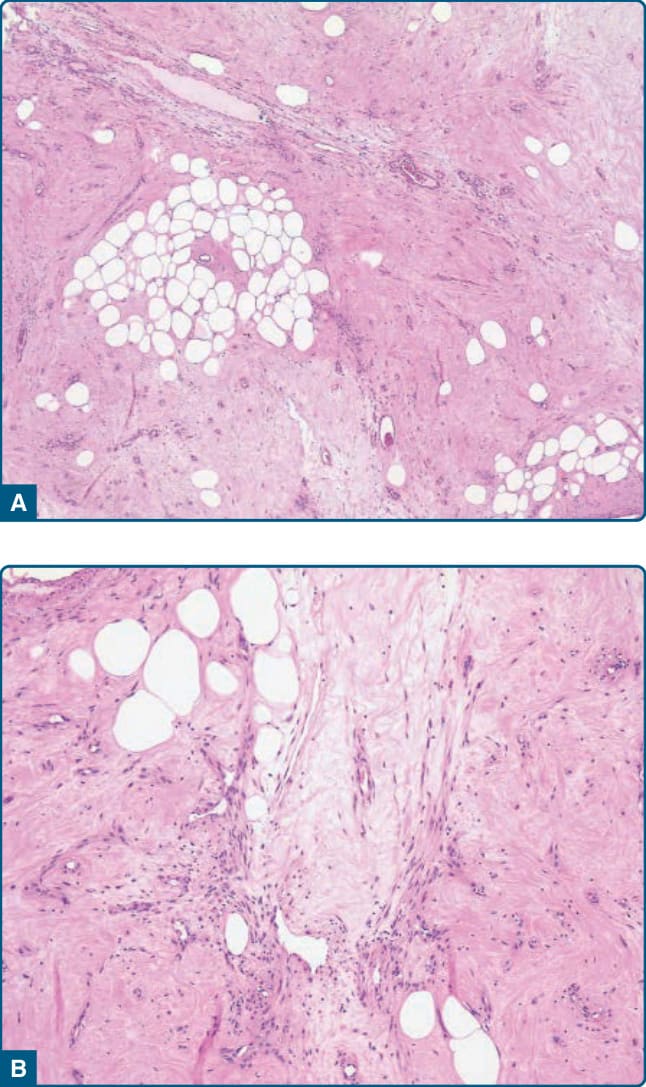
Figure 122-24 Myolipoma. A, Mature adipocytic cells are admixed with bland spindled cells. B, The myogenic spindled cells contain an eosinophilic cytoplasm and bland spindled nuclei.
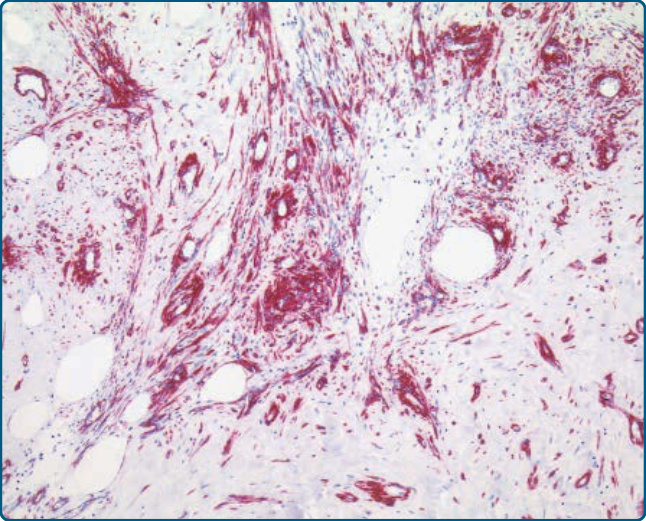
Figure 122-25 Myolipoma. Eosinophilic spindled tumor cells stain positively for h-caldesmon, confirming their smooth muscle differentiation.
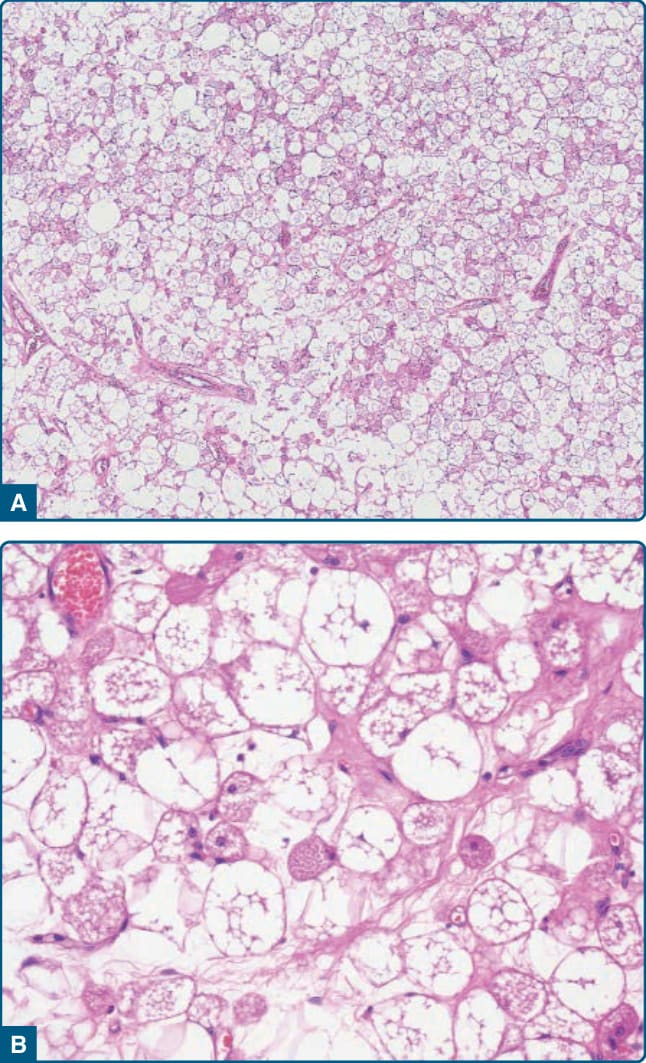
Figure 122-26 Hibernoma. A, Mature adipocytes are admixed with large multivacuolated cells and smaller eosinophilic cells. B, Vacuolated tumor cells with centrally placed nuclei and a clear or eosinophilic granular cytoplasm.
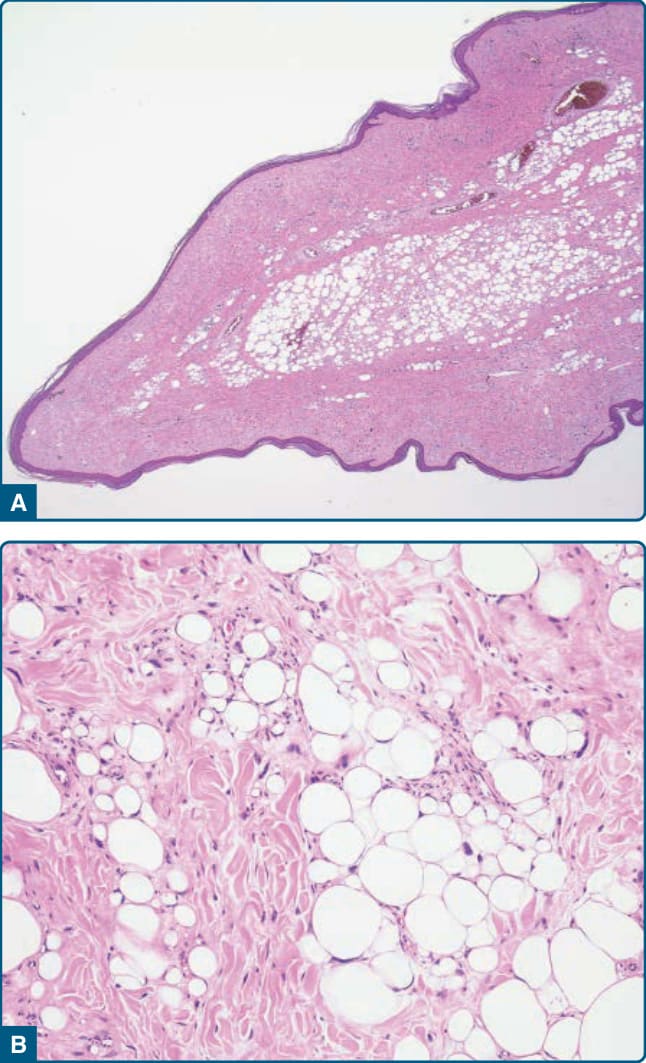
Figure 122-27 Dermal atypical lipomatous tumor. A, A polypoid lesion, clinically diagnosed as a skin tag, has been excised. B, Histologically, an atypical lipomatous tumor composed of atypical stromal cells and atypical lipogenic cells with enlarged hyperchromatic nuclei and scattered lipoblasts is seen.
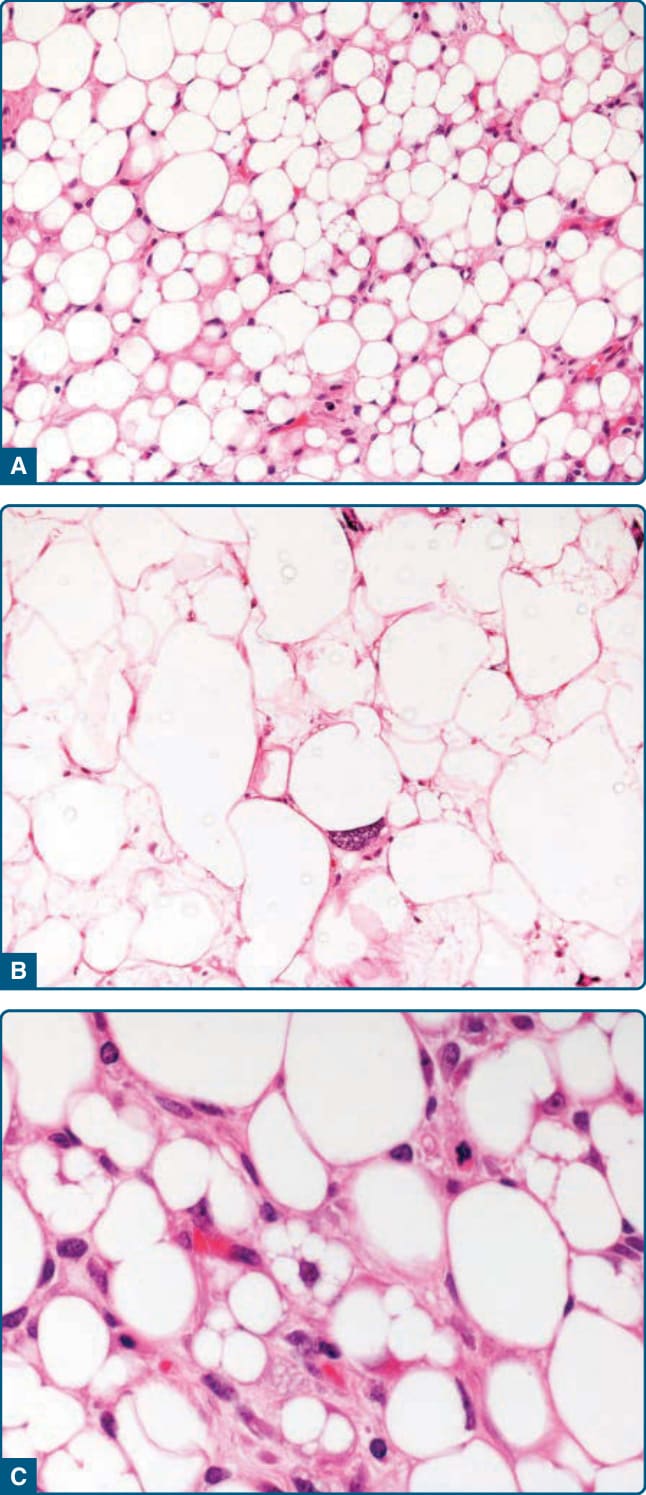
Figure 122-28 Atypical lipomatous tumor. A, The lipomalike variant is composed of lipogenic cells showing marked variation in size and shape. Scattered, enlarged, hyperchromatic nuclei and vacuolated lipogenic cells are noted. Higher-power view reveals enlarged and hyperchromatic nuclei (B), as well as multivacuolated lipoblasts (C).
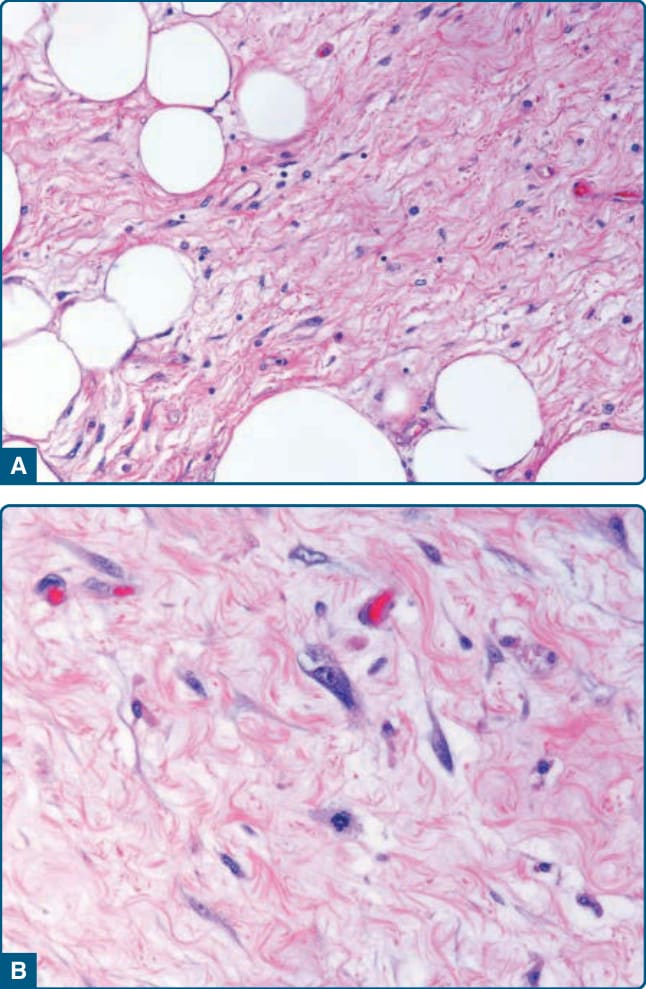
Figure 122-29 Atypical lipomatous tumor. A, The presence of a paucicellular stroma with admixed adipocytes characterizes the sclerosing variant. B, Note the presence of bizarre-appearing stromal cells set in a fibrillary stroma.
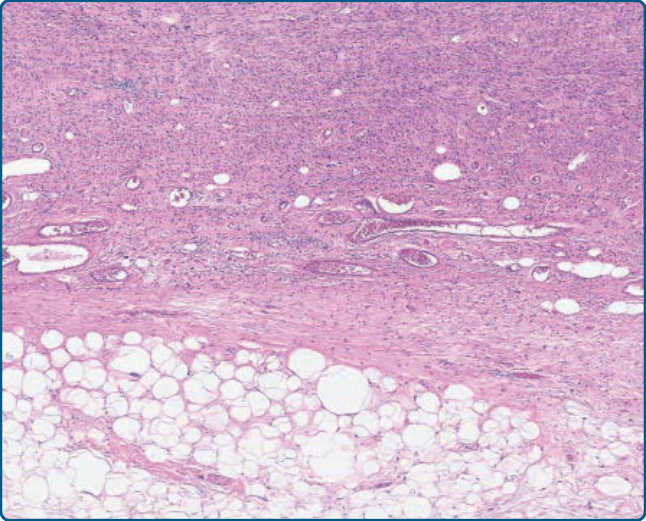
Figure 122-30 Dedifferentiated liposarcoma. A rather abrupt transition from areas showing features of an atypical lipomatous tumor (button) to a nonlipogenic sarcoma is seen.
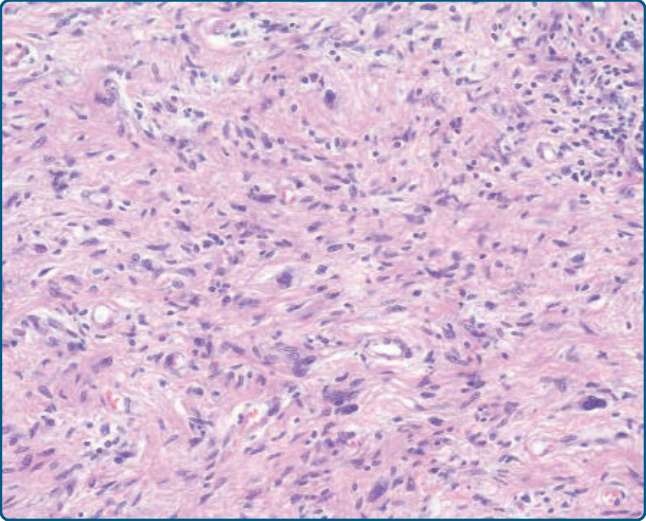
Figure 122-31 Dedifferentiated liposarcoma. The nonlipogenic component often shows features of a rather undifferentiated, pleomorphic sarcoma.
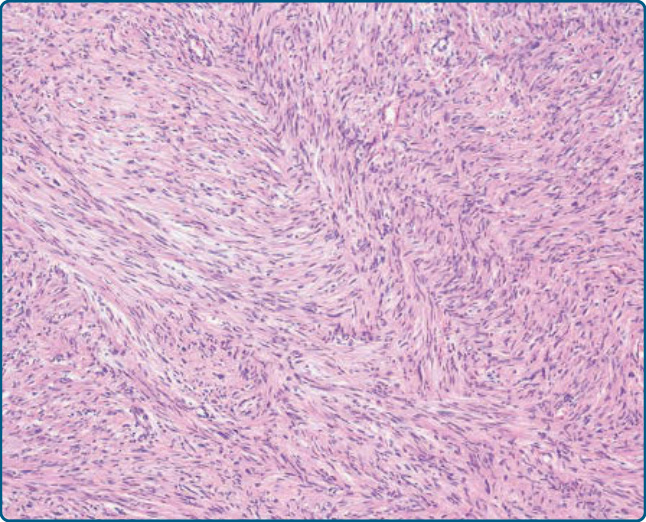
Figure 122-32 Dedifferentiated liposarcoma. Infrequently, a low-grade dedifferentiation with features of a low-grade fibroblastic sarcoma is noted.
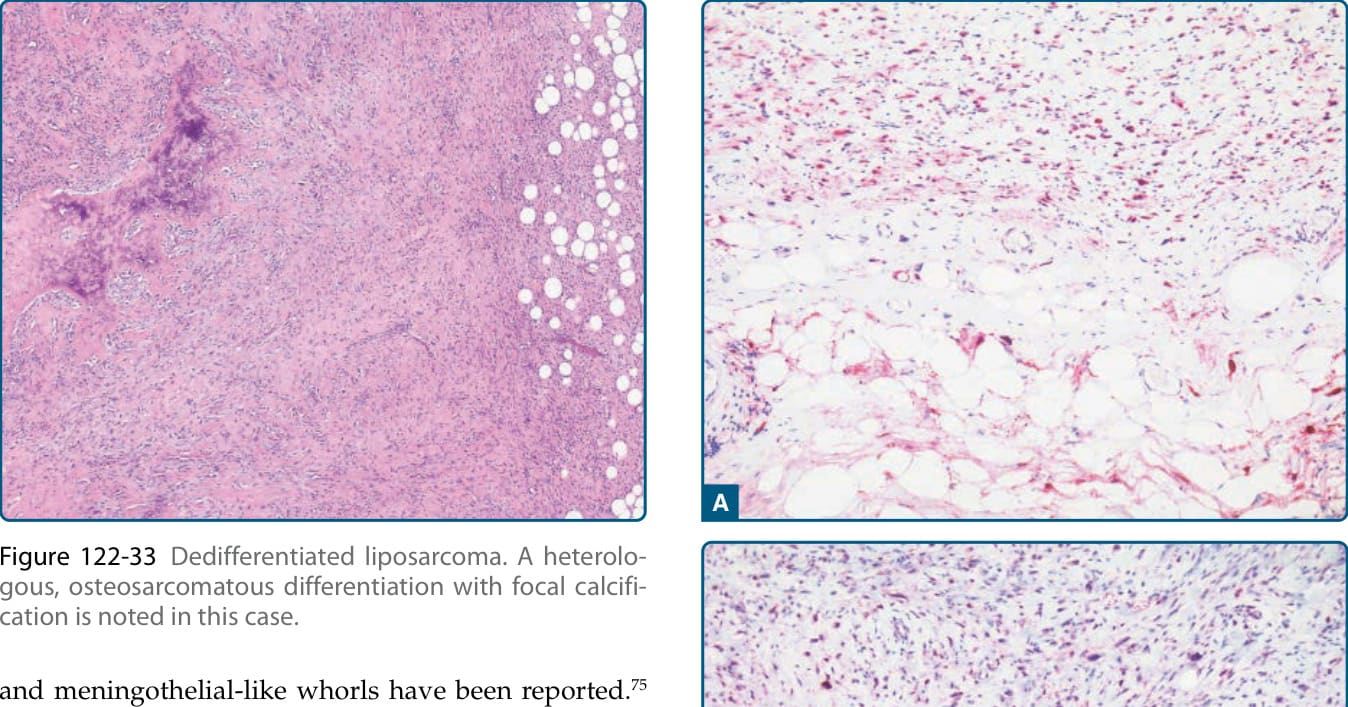
Figure 122-33 Dedifferentiated liposarcoma. A heterologous, osteosarcomatous differentiation with focal calcification is noted in this case.
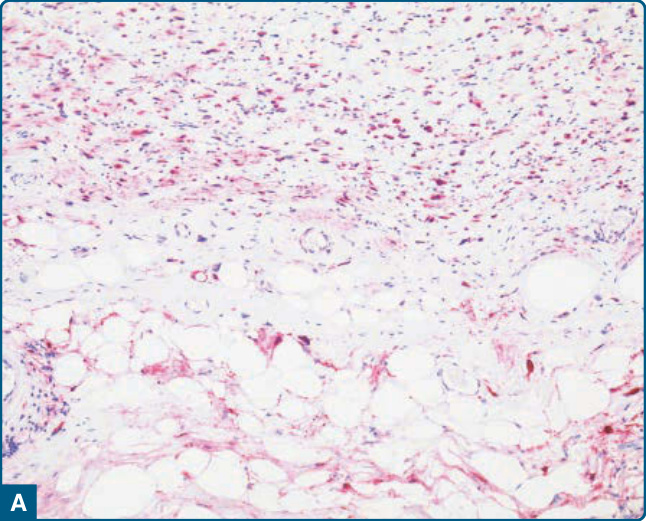
Figure 122-34 Dedifferentiated liposarcoma. Immunohistochemically, an expression of p16 (A) and MDM2 (B) is seen in the lipogenic and in the nonlipogenic component.
Figure 122-35 Dedifferentiated liposarcoma. Heterologous myogenic differentiation with strong expression of desmin by nonlipogenic spindled tumor cells.
Figure 122-36 Myxoid liposarcoma. A, The myxoid neoplasms are lobulated and composed of immature mesenchymal cells and atypical lipogenic cells. Note the increased cellularity in the periphery. B, The presence of univacuolated, bivacuolated, and multivacuolated lipoblasts and cytologically bland oval-shaped cells set in a myxoid stroma is a characteristic feature. C, Note the delicate branching, capillary sized vessels.
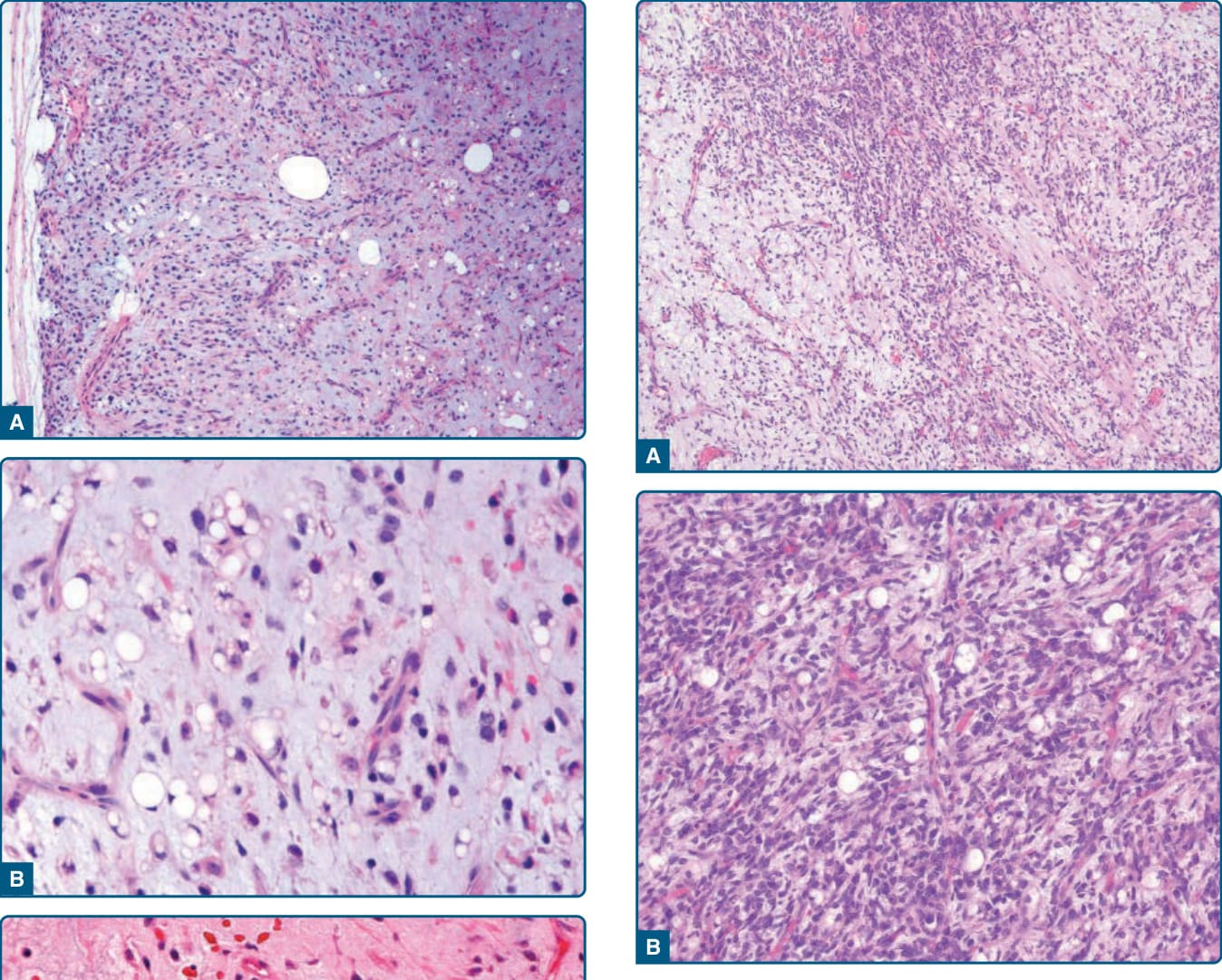
Figure 122-37 Myxoid/round cell liposarcoma. A, Areas of increased cellularity with slightly enlarged round tumor cells containing round nuclei are seen. B, High-grade round-cell liposarcoma is composed predominantly of enlarged round tumor cells without prominent pleomorphism. Note the characteristic vascular pattern and the presence of lipoblasts.
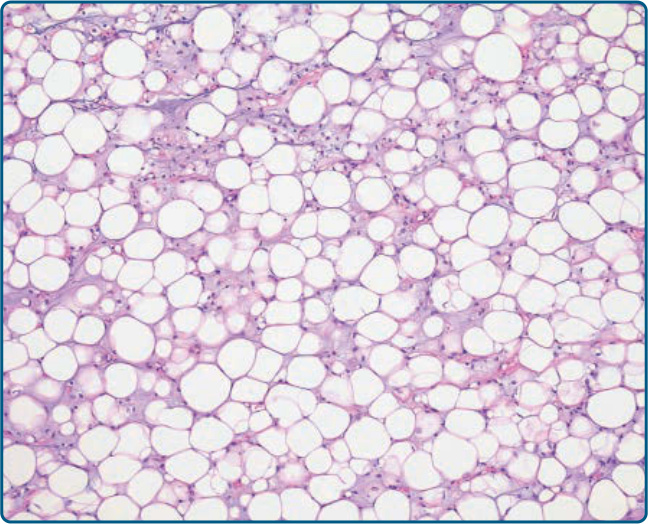
Figure 122-38 Lipogenic myxoid liposarcoma. In some cases of myxoid liposarcoma, a predominant lipogenic differentiation is seen mimicking an atypical lipomatous tumor.
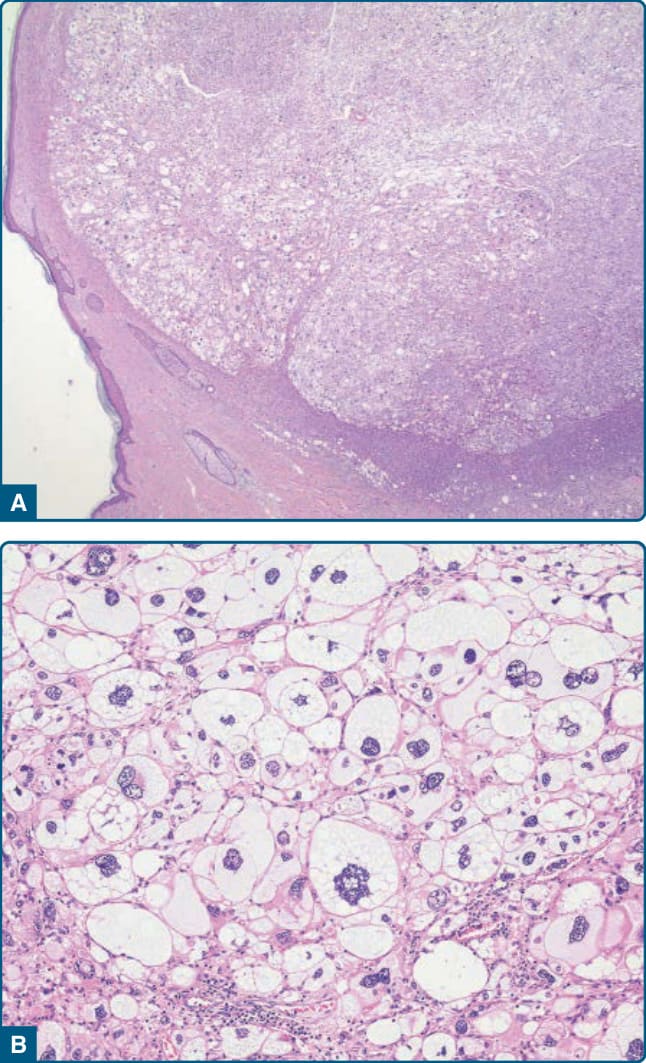
Figure 122-39 Superficial pleomorphic liposarcoma. A, An exophytic growing, purely dermal pleomorphic liposarcoma. B, Note the presence of pleomorphic lipoblasts, with bizarre, hyperchromatic nuclei.
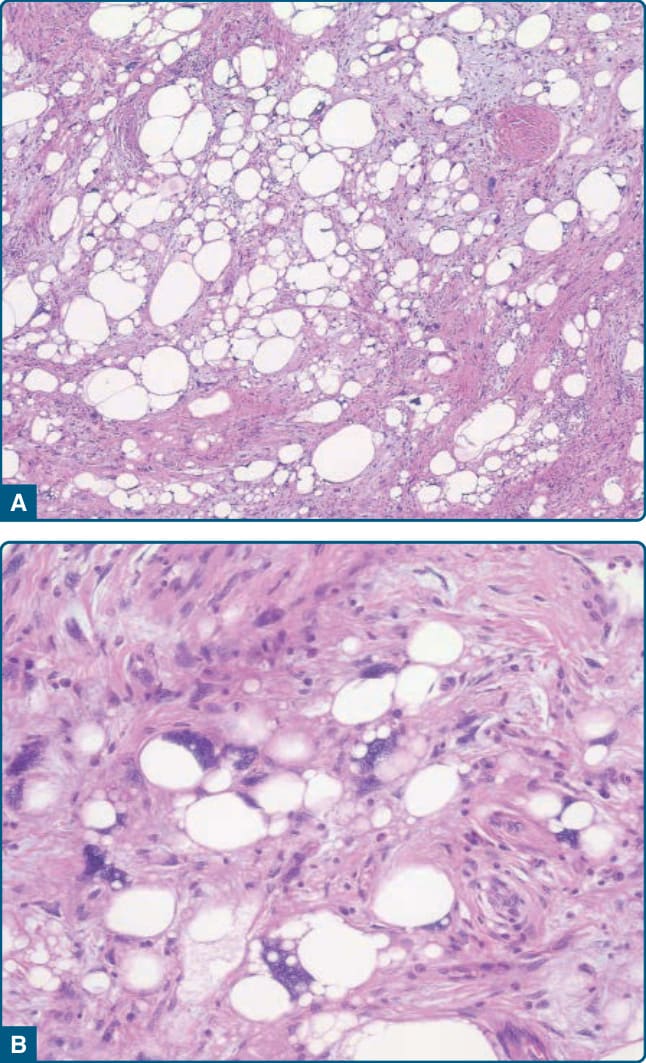
Figure 122-40 Pleomorphic liposarcoma. A and B, Pleomorphic lipoblasts and atypical lipogenic cells are irregularly admixed with sarcoma cells.
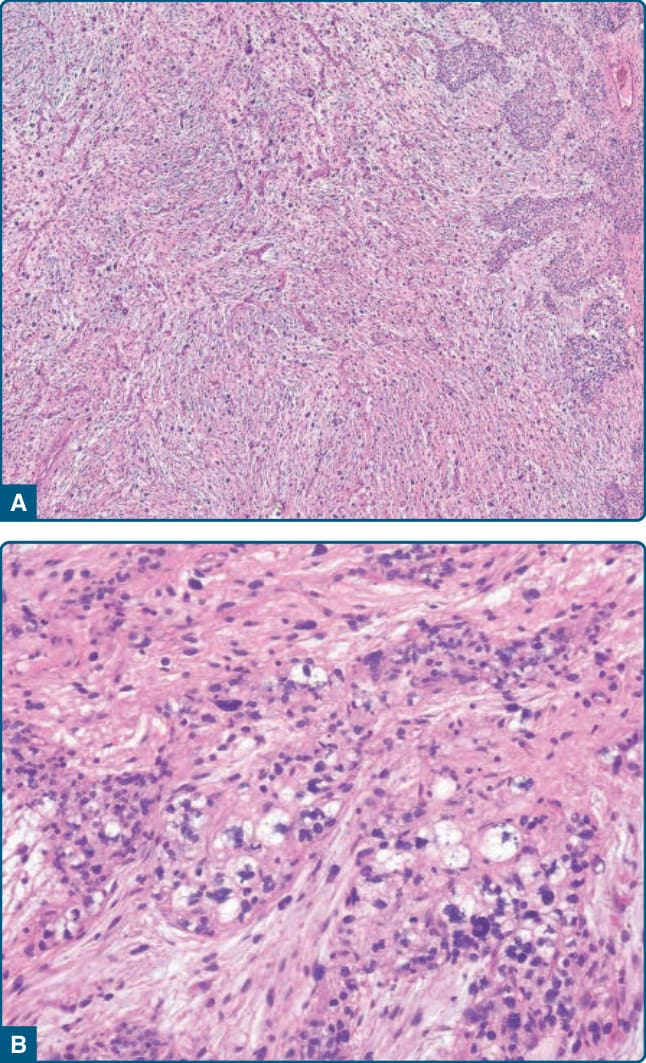
Figure 122-41 Pleomorphic liposarcoma. A, The neoplasm shows features of a higher grade myxofibrosarcoma. B, Pleomorphic lipoblasts are present at the right side.
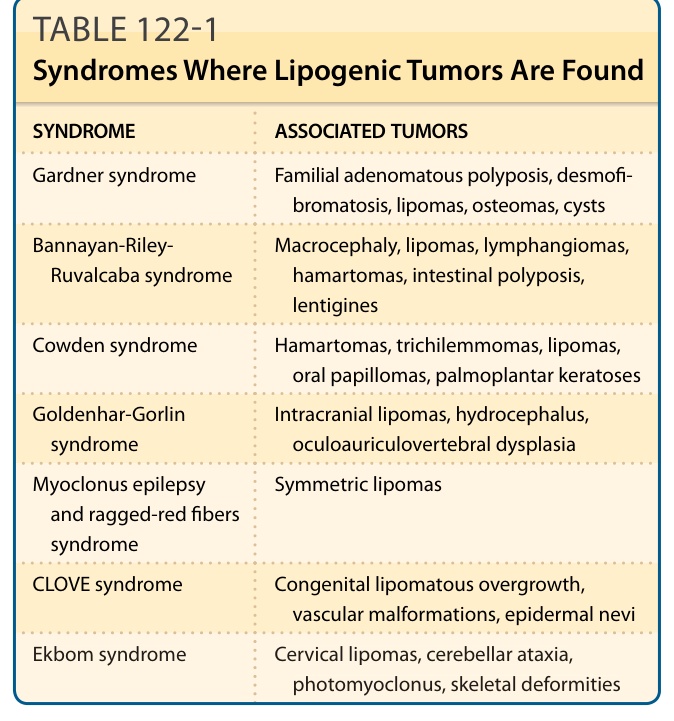
TABLE 122-1 Syndromes Where Lipogenic Tumors Are Found