Melanocytic Nevi
20
CONGENITAL MELANOCYTIC NEVI INTRODUCTION
This chapter discusses melanocytic nevi, defined as benign neoplasms of melanocytes, most of which manifest themselves as cutaneous pigmented lesions. They are characterized by the presence of banal melanocytic cells in nests (defined as three or more melanocytes in direct contact [also known as thèque]), within the epidermis, dermis, or in other tissues. The melanocytic cells forming these nevi are referred to as nevomelanocytes. The term melanocytic hyperplasia is a descriptive term used to indicate increased melanocytes confined to the basal layer of the epidermis in the absence of nest formation. Simplistically, melanocytic nevi can be divided into those that arise from junctional melanocytes (often termed acquired nevi) and those that arise from neural-crest derived melanocytic precursors that migrate along neurovascular bundles, stop before they reach the epidermis, and proliferate at those sites. The latter are termed congenital melanocytic nevi (CMNs). Dysplastic nevi are defined as those that display atypical architectural and cytologic features. Historically, the nomenclature associated with these lesions includes B-K moles (recognizing the first two families described with such lesions whose surnames began with the letters B and K),1 familial atypical multiple mole and melanoma syndrome,2
atypical mole syndrome,3 Clark nevus,4 atypical moles, and nevus with architectural disorder and (varying degrees of) cytologic atypia.5 Although the nomenclature for these lesions remains contentious, the term dysplastic nevus (DN) is most frequently utilized5,6 and is the term that will be used in this chapter. It is also important to note that in practice, the terms dysplastic and atypical are sometimes used as a modifier for other melanocytic neoplasias (eg, Spitz nevi) or hyperplasias to indicate a variation from a typical pattern or to recognize an increased concern for malignant biologic potential. The nevi described in this chapter include CMNs, nevus spilus, common acquired melanocytic nevi, blue nevi, Spitz nevi, pigmented spindle cell nevi (PSCN), dysplastic nevi, and nodal nevi. Benign melanocytic hyperplasias include lentigo simplex and solar lentigo.
AT-A-GLANCE
■ Pigmented neoplasms of melanocytes that are evident at birth or shortly thereafter.
■ Lesions may be small, medium-sized, or large and cover substantial body surface area.
■ Large or giant lesions have a significant risk for melanoma development. Cranial or midline congenital melanocytic nevi and those with satellite lesions have an increased risk of leptomeningeal involvement.
■ Histology shows extensive nevomelanocytic infiltration of the dermis, accentuation along the adventitia of skin adnexa and nerves, single-filing between collagen bundles, often with involvement of subcutaneous tissues.
EPIDEMIOLOGY
EPIDEMIOLOGY
CMNs are found in approximately 1% to 3% of neonates across ethnicities.7 The majority of lesions are small to medium in size and are present at birth; however, there are also congenital nevi (>1.5 cm) that appear for the first time between 1 month and 2 years of life (termed tardive congenital nevi). A significant gender predilection has not been demonstrated. CMNs occur most commonly on the trunk and extremities, although scalp and facial involvement are seen. Giant CMNs are uncommon. CMNs that attain 99 mm or more in diameter occur in approximately 1 of every 20,000 newborns, and those with a garment distribution affect 1 of every 500,000 newborns.8
CLINICAL FEATURES
CLINICAL FEATURES
Nevi of congenital onset have traditionally been grouped based on diameter into small, medium, and
large sizes. The size limits of each type are arbitrary because the diameter of these lesions lies on a continuum. There is some rationale for standardizing congenital nevi by size because there is increased risk of melanoma associated with large and giant CMNs.9,10 The most accepted system is based on the expected size of the nevus in adult life11 because CMNs have been shown to grow in proportion with the affected anatomic region.12 Small CMNs are less than 1.5 cm in diameter (projected adult size), medium ones are divided into two groups—M1, 1.5 to 10 cm and M2, >10 to 20 cm— as are large ones—L1, >20 to 30 cm and L2, >30 to 40 cm. Last, giant CMNs are categorized as G1, >40 to 60 cm and G2, >60 cm (Fig. 115-1). This classification scheme also rates the number of satellite nevi (S1: <20, S2: >20–50, S3: >50).
CUTANEOUS FINDINGS
Although CMNs are on average larger than acquired nevi, there is no specific size limitation that can be used to reliably predict whether a given nevus is congenital or acquired. Pigmented lesions attaining a diameter of 1.5 cm or more are likely to be CMN, dysplastic nevi, or melanoma. Most CMNs present as flat brown patches or plaques with smooth or slightly uneven borders. Many show hypertrichosis compared to surrounding unaffected skin. Hair growth may be present at birth or commence in the years thereafter. Most congenital nevi begin with even pigmentation, but some variability of pigmentation and irregularity of surface texture eventuates in most medium- and large-sized lesions over time. Lesions may have a pebbly, rugose, verrucous, or lobular appearance. Dermoscopic features are variable and include a reticular, globular, homogeneous, and cobblestone
20
pattern or a combination thereof. Dermoscopic findings in dysplastic nevi sometimes overlap with those of CMN. In one study, most of the features related to dysplastic nevi, including atypical dots and globules, focal hypopigmentation, and perifollicular hypopigmentation, were observed in CMN.13 Therefore, eliciting a history with regards to the time of lesion onset is important. In large CMN, there can be significant variability in pigmentation and structure, and melanomas may develop in the deep components, potentially limiting the utility of dermoscopy in such lesions. Some CMNs show an atypical clinical appearance, including significant color variegation and irregularities in outline and surface contour. Color variations include dark brown, black, or hues of blue. These features often correlate with atypical histopathologic findings. Loss of pigmentation, halo depigmentation, and regression can also occur.
RELATED PHYSICAL CONDITIONS
One of the most important related physical conditions in patients with CMNs on the head, neck, or posterior midline is neurocutaneous melanosis (NCM). In this condition, the cells of the congenital nevus involve the meninges or even the parenchymal cells of the brain. Most patients with NCM have many cutaneous congenital nevi, either in the form of a giant nevus with many satellites or in the form of many medium-sized lesions. Symptomatic NCM presents with seizures and hydrocephalus in the first few years of life when melanocytes are diffusely distributed along the meninges. There may be neurologic deficits and vomiting from increased intracranial pressure. When an intracranial mass is present, symptoms may present later in life.14
The prognosis is poor if neurologic symptoms develop. Patients often die within 3 years of symptom onset.
COMPLICATIONS
The most important complication of congenital nevi is that they can give rise to melanoma. The overall incidence of this complication is approximately 1% to 2%.9
The risk of melanoma appears to be proportionate to the number of melanocytes that comprise the nevus. This in turn is closely related to its size. Thus, small- and medium-sized lesions have a low risk of developing melanoma, but large- and giant-sized lesions have greater risk. Additionally, satellite nevi are associated with increased risk of melanoma. In one systematic literature review, melanoma arising from CMN exceeded 40 cm in 74% of 52 cases studied and 94% of those had satellite nevi.15 The lifetime risk of melanoma development in lesions exceeding 40 cm (projected adult size) with satellite nevi has been estimated at 10% to 15%.9
Although melanoma arising from CMN may occur at the dermal–epidermal junction (DEJ) (as they do in acquired nevi), they show a tendency to arise in deeper dermal and subcutaneous components of the nevus. These tumors are highly aggressive in part because of
1945
20
their greater Breslow thickness at presentation. They present with the sudden appearance of a dermal or subcutaneous nodule. Sometimes lymph node metastasis precedes clinical detection of the primary melanoma. Other clinical features that should raise concern for melanoma include very dark pigmentation, ulceration, bleeding, or onset of other sensory symptoms. There is no ethnic predilection for melanoma developing in CMN. For cranial, midline, or CMN with multiple satellite lesions, there is a risk of leptomeningeal involvement (NCM). Symptomatic NCM carries a poor prognosis, even in the absence of malignant degeneration (central nervous system [CNS] melanoma). A recent literature review revealed that 37% of 178 melanomas arising in patients with congenital nevi were primary CNS melanomas rather than of cutaneous origin, and most of these (53.9%) developed in patients with multiple medium-sized CMNs.16
Proliferative nodules also constitute a significant complication of congenital nevi because they need to be removed. They typically present as a lightly pigmented or flesh-colored nodule developing in a preexisting congenital nevus. Although they almost always behave in a benign fashion, histopathologic examination of a lesion that is clinically indistinguishable from a proliferative nodule may show the findings of a clear-cut melanoma.
RISK FACTORS
RISK FACTORS
There are rare reports of familial clustering of congenital nevi (Fig. 115-2).17 Patients with neurofibromatosis type 1 appear to have an increased incidence of giant CMNs.18
1946
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
CMN result from postzygotic somatic mutations of proteins involved in the mitogen-activated protein kinase (MAPK) pathway within the embryonic melanocyte. These primarily include mutations of NRAS, resulting in abnormal accumulation of melanocytic cells along migration pathways during normal development. Whereas NRAS mutations are most prevalent in large- and giant-sized CMNs, small- and mediumsized lesions have been reported to have either NRAS mutations or in a small number of cases, activating mutations in BRAF. It should be noted that the proportion of cases with NRAS or BRAF mutations vary between studies in the literature, which probably reflects the different methodologies used (ie, whether CMN was defined as historically being present at birth, the exact measurements that were used, whether both genes were sequenced, and so on).19 In one study of 32 congenital nevi confirmed to be present at birth, the authors found that 81% of cases had mutations in NRAS, but no BRAF mutations were detected; furthermore, 7 of the 10 proliferating nodules that developed within the congenital nevi also harbored mutations in NRAS rather than BRAF. In contrast, 20 of 28 nevi studied that had a congenital pattern histologically but were not confirmed to be present since birth harbored BRAF mutations (similar to acquired nevi); only 7 had mutations of NRAS.20
Clinical findings such as a congenital divided nevus of the eyelid can give us insight into when these mutational events may occur (Fig. 115-3). The palpebral buds develop during the 7th week of gestation and
the upper and lower eyelids fuse by week 9 or 10. The eyelids then begin to separate during the 20th week, and complete separation commences between weeks 28 and 30.21 Because of the contiguous nature of the lesion on the upper and lower eyelids, it may be presumed that the nevus cells migrated into this location sometime during or after eyelid fusion but before the eyelids separated.
DIAGNOSIS
DIAGNOSIS
The diagnosis of a congenital nevus is usually straightforward. The more challenging problem is whether the nevus contains any areas that necessitate biopsy. For patients with congenital nevi on the head or axial midline, an important question is whether there is subjacent NCM. This is best addressed by imaging studies (see later).
PATHOLOGY
Although there are histopathologic features that are suggestive of a congenital nevus, there are no criteria with absolute sensitivity and specificity for predicting whether a lesion is of congenital onset. Prototypical large- or medium-sized CMNs involve the entire skin from the junctional zone to the subcutis (Fig. 115-4). Small, round melanocytes are present in subcutaneous septae and to a lesser extent in lobules, with progressively (slightly) larger cells in the upper levels of the dermis and along the junctional zone. Some lesions are densely cellular, and there is a propensity for the cells to surround neurovascular bundles, appendageal structures, and folliculosebaceous units. Subendothelial protrusion by nevomelanocytes within lymphovascular spaces is sometimes prominent. The junctional zone may be involved by cells
20
distributed singly and in small nests. These are often separated from the upper dermal part of the lesion by a zone of uninvolved papillary dermis. The junctional cells are usually larger than those beneath them, and basilar hyperpigmentation is common. A rim of pigmented melanocytes is often present along the upper border of the dermal component, which often extends along the innermost perifollicular melanocytes. In some large and in most small congenital nevi, the subcutis is not involved. In such cases, at the base of the lesion, melanocytes splay between collagen bundles in cords and strands within the deep or mid reticular dermis. Congenital nevi that undergo neurotization show areas where schwannian differentiation occurs. Instead of small round melanocytes, one sees small S-shaped spindle cells. These can form thin, wavy fascicles with clefts in between them containing mucin. Admixed adipocytes are commonly seen. Collections of neuroid cells can form pseudomeissnerian corpuscles, a palisaded arrangement of cells around a cellular mass of homogeneous material, simulating native Wagner-Meissner corpuscles. In highly neurotized lesions, one may not be able to morphologically distinguish between nevus and neurofibroma. Neural differentiation is sometimes responsible for the lobulation and redundancy of tissue corresponding clinically with soft rugose areas of the nevus. Other histologic variations seen include cells with a combined epithelioid cell (Spitz) phenotype, which are often admixed with more conventional round cell and neuroid elements. CMNs may also have elements of blue nevus (either common or cellular type) with heavily pigmented spindle-shaped melanocytic cells or show features of inverted type-A or deep penetrating nevus. In a recent series of 197 congenital nevi in children younger than 3 years of age, 74% of patients studied had atypical histopathologic features. These included cytologic atypia (mostly mild or moderate),
A B C
1947
20
architectural disorder (mostly mild or moderate), and pagetoid scatter; no cases of melanoma were identified in these patients with a mean follow-up period of 7.3 years.22
Proliferative nodules feature large, round hypercellular aggregates of melanocytes that appear discrete on scanning magnification but tend to blend in with the background nevus cells. True to their name, they often contain mitotic figures. The melanocytes in these nodules may have a range of appearances, including cells with small to moderately enlarged nuclei, cells with epithelioid cytology, spindled cells, and blue nevus– like features. Proliferative nodules tend to have lower mitotic counts than melanoma and are less likely to show ulceration or the cytogenetic or epigenetic aberrations detected in melanoma.23,24
SPECIAL TESTS
Imaging studies to detect NCM include magnetic resonance imaging of the brain or spinal cord concordant with the anatomic location of the nevus.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-1.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
CMNs have a dynamic evolution during body growth. CMNs at birth usually distort the skin surface at least slightly when assessed by oblique lighting and may become more elevated over time. Surface pigmentation also may change. Lightly pigmented CMNs may become more darkly pigmented, and darkly pigmented CMNs eventually may become less pigmented. CMNs may also develop a halo of depigmentation, potentially heralding spontaneous regression. Relatively hairless CMNs at birth may develop long, dark, coarse hair or may maintain a relatively normal hair density. CMNs
■Café-au-lait macule
■Café-au-lait macule
■Nevus spilus
■Nevus spilus
■Lentigo simplex
■Lentigo simplex
■Nevus of Ota/Ito
■Nevus of Ota/Ito
■Dermal melanocytosis (Mongolian spot)
■Dermal melanocytosis (Mongolian spot)
■Becker melanosis
■Becker melanosis
■Arrector pili (smooth muscle) hamartoma
■Arrector pili (smooth muscle) hamartoma
■Epidermal nevus
■Epidermal nevus
■Nevus sebaceous
■Nevus sebaceous
1948
■Solitary mastocytoma
■Solitary mastocytoma
generally expand in direct proportion to growth of a given anatomic region.12 Proliferative nodules present as flesh-colored or lightly pigmented nodules that develop and then stabilize. CMNs in fully grown individuals should remain stable. The prognosis is excellent unless complicated by NCM or melanoma.
MANAGEMENT
MANAGEMENT
TREATMENT
The treatment of CMN depends on the perceived risk of melanoma plus cosmetic and functional considerations. The risk of developing melanoma is related to its size, and melanoma may arise in large CMNs even in the first few years of life. Therefore, debulking of large nevi and excision of smaller or medium-sized ones is desirable when feasible. This can be done for large nevi in serial stages. It is probably prudent to delay treatment until after the first 6 months of life to reduce surgical and anesthetic risks. Management of patients with large and giant CMNs must be individualized. Extensive involvement of the body surface, with little or no normal skin available for graft sites, may necessitate abandoning efforts at prophylactic excision and accepting lifelong surveillance to detect the earliest signs of malignant change. It may be impossible to remove every nevomelanocyte in large CMN, particularly when there is involvement of vital structures or deep anatomic zones. The treatment goal is to remove as much of the nevus as possible while preserving function and improving cosmetic appearance. Other indications for surgical excision include symptomatology (ie, chronic pruritus, pain, ulceration). Unlike surgical excision, dermabrasion, lasers, and other modes of destructive therapy do not address the malignant potential of CMN; nevomelanocytes will still be left behind in the dermis, and the cosmetic results associated with destructive therapy are not always predictable. Although atypical-appearing CMN should be considered for immediate excision, careful surveillance without excision may be an option for clinically benign lesions depending on gross appearance, size, location, cosmetic and functional deficits (or improvement) resulting from excision, and general health issues. Given the risk of general anesthesia, for lesions perceived to be at low risk during the first decade of life, it is appropriate to consider waiting until the child is old enough to tolerate local anesthesia. All CMNs should be documented at birth, preferably in the form of high-quality photographs that can be used to aid follow-up by parents and physicians. Follow-up is complicated by the natural evolutionary changes that take place in a nevus during body growth (ie, surface, size, color, and hair), and periodic updates of photographs may be warranted. Suspicious changes in color, surface, or size require urgent evaluation.
PREVENTION AND COUNSELING
There is no known preventive approach to avoid the development of CMNs. UV radiation (UVR)–induced mutations play no role in the initial development of lesions already present at birth. The issues around body image and social adjustment raised by large and giant congenital nevi may benefit from counseling and support groups, including Nevus Network (www .nevusnetwork.org) and Nevus Outreach, Inc. (www .nevus.org).
NEVUS SPILUS
AT-A-GLANCE
■ Nevus spilus (derived from Greek spilos, meaning spot)—spotted nevus
■ Synonyms: speckled lentiginous nevus, zosteriform lentiginous nevus
■ Pigmented neoplasm of melanocytes that develops during infancy or early childhood.
■ Lesion presents with two components, a light brown patch (café-au-lait) containing speckled dark macules or papules.
■ Risk for melanoma is low but may occur.
■ Histology shows localized collections of nevus elements forming in the background of mild melanocytic hyperplasia.
EPIDEMIOLOGY
EPIDEMIOLOGY
Nevus spilus occurs in approximately 1% to 2% of the population. They are present either at birth or in the first years of life and have therefore been regarded as a variant of congenital nevus. There does not appear to be gender or ethnic predilection.
CLINICAL FEATURES
CLINICAL FEATURES
Darkly pigmented flat macules or papules are usually present within the nevus spilus on presentation. New pigmented elements may evolve within the lesion over time.
CUTANEOUS FINDINGS
The background pigmentation of a nevus spilus is circumscribed and similar in appearance to a café-au-lait macule in hue, with even light pigmentation. There are scattered superimposed more darkly pigmented macules or papules. The tan macular background
20
A
B
pigmentation can range in size from less than 1 cm to larger than 10 cm in diameter (Fig. 115-5). Lesions are most commonly found on the trunk and extremities, although any cutaneous site may be affected. Multiple lesions may be present and have a segmental distribution. There are rare reports of a divided nevus spilus of the eyelid25 as well as a report of one in the oral cavity.26
Dermoscopy reveals dark speckled foci with a reticuloglobular pattern in a background light brown and reticular pattern. Mixed patterns may occur that include combinations of homogeneous, reticular, globular, granular, and spitzoid patterns.27 Dermoscopy and reflectance confocal microscopy have been used for early detection of melanoma, a rare complication of nevus spilus.28
RELATED PHYSICAL CONDITIONS
Nevus spilus has been associated with other anomalies of vascular, CNS, or connective tissue origin. It has
1949
20
been proposed by Vidaurri-de la Cruz and Happle that two distinct forms of nevus spilus exist, those with macular and those with papular speckles.29 Whereas macular varieties are more commonly associated with phakomatosis spilorosea (previously classified as pigmentovascularis type III), the papular variant is typically seen in phakomatosis pigmentokeratotica. Phakomatosis spilorosea constitutes presentation of both nevus flammeus and nevus spilus with or without nevus anemicus. Systemic disease may or may not be present, which include vascular anomalies, ocular abnormalities, limb hemihypertrophy, or development of multiple granular cell tumors. Phakomatosis pigmentokeratotica includes nevus spilus plus organoid nevus with or without systemic symptoms, which include neurologic deficits and skeletal abnormalities.
COMPLICATIONS
The main concern that prompts a biopsy is a changing lesion, where one may see enlargement of dark macules or papules within the nevus spilus. One can see larger, irregularly shaped macules, sometimes with a central papule in so-called dysplastic nevus spilus. In such cases, the lesion can show any of the changes seen in dysplastic nevi. Rare cases of melanoma arise in nevus spilus and are recognizable as larger, irregularly shaped areas with variegated pigmentation. It is likely the risk of melanoma increases to some degree with the size of the nevus spilus, particularly with larger segmental lesions greater than 40 cm.30
RISK FACTORS
RISK FACTORS
There are no known risk factors for nevus spilus, aside from the association with phakomatosis spilorosea and pigmentokeratotica.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Nevus spilus is believed to develop secondary to a postzygotic mutational event initiating a clonal field of melanocytes susceptible of creating multiple melanocytic tumors within. These arise likely secondary to additional mutational or epigenetic events. Sarin and coworkers identified an activating HRAS mutation (c.37G->C, p.Gly13Arg) in eight of eight nevi spili studied, implicating this gene locus as the predominant causative mutation in sporadic nevi spili.31 The same author previously described a nevus spilus giving rise to agminated Spitz nevi with the same mutation.32
Kinsler and coworkers performed next-generation sequencing on three nevi spili with a distinct phenotype, large background café-au-lait–type patches with superimposed multiple medium or large pigmented patches indistinguishable from CMN.33 This phenotype
1950
was termed nevus spilus-type congenital melanocytic nevus. In contrast to the activating HRAS mutations seen in small sporadic nevi spili,30 nevus spilus–type CMNs displayed activating mutations of NRAS in all three patients (two with c.183A->Cp.Q61H, one with c.37G->Cp.G13R). Targeted exon capture of two skin samples from an additional patient also showed the same NRAS mutation (p.Q61H) in both the background pigmentation and the superimposed nevus.33
DIAGNOSIS
DIAGNOSIS
The diagnosis of nevus spilus is usually straightforward. Small lesions are sometimes mistaken for dysplastic nevi and large lesions for conventional CMN.
PATHOLOGY
Histologic sections reveal that the tan background corresponds to a diffuse area where there is slight epidermal hyperplasia with basilar hyperpigmentation, from no perceptible increase in melanocytes to a slight increase in singular melanocytes along the basal layer. The dark spots correspond to small lentiginous junctional and compound nevi featuring increased numbers of single melanocytes and small nests along the DEJ and small, round melanocytes in the superficial dermis, in cases of compound nevi. Rarely agminated nevi within a nevus spilus may have the phenotype of a blue nevus (pigmented dendritic melanocytes) or Spitz nevus (epithelioid and spindled melanocytes).
SPECIAL TESTS
There are no other diagnostic tests at present.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-2.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Nevus spilus is a benign lesion that may develop more spotted nevoid elements over time. After
■Agminated nevomelanocytic nevi
■Agminated nevomelanocytic nevi
■Agminated lentigines
■Agminated lentigines
■Becker melanosis
■Becker melanosis
■Congenital nevomelanocytic nevus with heterogeneous pigmentation
■Congenital nevomelanocytic nevus with heterogeneous
pigmentation
■Café-au-lait macule
■Café-au-lait macule
developing, they are presumed to persist throughout life, although it is possible that some elements within the nevus spilus or rarely the entire nevus spilus itself could regress with time. The prognosis is excellent with the exception of rare cases complicated by melanoma.
MANAGEMENT
MANAGEMENT
TREATMENT
No standard guidelines exist for the management of patients with nevus spilus. Clinical appearance (typical or atypical), history of stability or instability of pigmented elements, congenital or noncongenital onset, perceived risk of developing melanoma, and cosmetic concerns are considerations when determining whether to excise or recommend periodic clinical evaluation for life. Documentation with high-quality photographs can be used to aid followup by parents and physicians. Atypical-appearing new or unstable elements in nevus spilus should be evaluated by histopathologic examination to exclude melanoma.
PREVENTION AND COUNSELING
There are no preventive measures for nevus spilus. UV protection is theoretically prudent in light of the propensity for melanocytic neoplasms to develop within nevi spili, as well as the rare reported cases complicated by melanoma.
COMMON ACQUIRED MELANOCYTIC NEVUS
AT-A-GLANCE
■ Synonyms: nevocellular nevus, common nevus, melanocytic nevus
■ Lesions are pigmented or skin-colored macules or papules which tend to be uniform in appearance and relatively small in size.
■ They primarily develop during childhood or early adulthood.
■ Increased numbers of acquired nevi impart an increased risk for melanoma development.
■ Common nevi are subcategorized based on location of cells: cells in the epidermis (junctional), dermis (intradermal), or both areas (compound). Pathologically, the cells mature becoming smaller in size within the deeper dermis and express melanocytic antigen HMB-45 at lower levels.
20
EPIDEMIOLOGY
EPIDEMIOLOGY
Common acquired melanocytic nevi develop after birth, slowly enlarge symmetrically, stabilize, and regress after a period of time. The number of nevi peaks in the third decade of life and declines thereafter. A number of studies have quantified the number of acquired nevi in different age groups. In a study of 432 European with white skin between the ages of 4 days and 96 years, nevi that were 3 mm in diameter or larger were detected in females and males, respectively, at median numbers of 0 and 2 in the first decade, 10 and 16 in the second decade, 16 and 24 in the third decade, 10 and 19 in the fourth decade, 12 and 15 in the fifth decade, 4 and 12 in the sixth decade, and 2.0 and 3.5 in the seventh through the ninth decades.34 Numbers of nevi vary among study populations, but a similar agerelated trend has been documented in most other large epidemiologic studies. The prevalence of acquired nevi also varies according to ethnicity. In a longitudinal study of children in Colorado, non-Hispanic white children showed significantly more nevi than all other ethnic groups, developing an average of four to six new nevi per year from ages 3 to 8 years.35 Nevi tend to be increased in individuals with light skin tone and those who have a tendency to sunburn.
CLINICAL FEATURES
CLINICAL FEATURES
Acquired common nevi develop over the first 3 decades of life and can persist in a stable state for decades, and many regress thereafter. In later adult years, nevus counts are significantly less and the rate of new or growing nevi declines, but melanoma incidence increases. Therefore, a new, growing, or changing pigmented lesion in an adult assumes a greater risk of being melanoma.
CUTANEOUS FINDINGS
The majority of common acquired nevi are less than 6 mm in diameter. Individual lesions have a homogeneous surface and coloration pattern, are round to oval in shape, and have sharply demarcated borders (Fig. 115-6). Most are skin colored, pink, or brown. Very dark brown or black nevi are unusual for people with light skin tones and should be viewed with suspicion. On the other hand, darkly colored nevi are common in those with dark skin tones. Blue, gray, red, and white areas are not typical for common acquired nevi and should raise concern for melanoma. Lesions that are papillomatous or dome shaped tend to be lighter in color and display a more dominant intradermal component, but flat lesions tend to show more pigmentation and a more robust junctional component. Similar to congenital nevi, acquired nevi sometimes show hypertrichosis compared with the surrounding skin.
1951
20
A B
Common acquired nevi occur anywhere on the skin surface. However, compared with light-skinned individuals, those with dark skin more commonly develop nevi on the palms, soles, nail apparatus, and mucous membranes. Nevi on the palms and soles tend to be flat and may not distort the skin surface because of the thickness of the stratum corneum. Nevi of the nail apparatus commonly present as a linear longitudinal streak of dark or light-brown pigment from the nail matrix extending to the distal edge of the nail plate. Extension of pigment onto the proximal nail fold or beyond the distal nail groove should be considered suspicious for melanoma. Dermoscopy can reveal a number of patterns, but a reticular or globular pattern is commonly seen in
acquired nevi. Nevi on the palms and soles can show a parallel-furrow pattern, lattice-like, or fibrillar pattern. Nonuniform patterns and parallel-ridge patterns are worrisome for melanoma. Nail matrix nevi show regular lines on a brown background. A recent comparative analysis of the dermoscopic features of benign nail matrix nevi in adults and children revealed that those in children more often showed atypical melanomaassociated dermoscopic features.36
Halo nevi are usually asymptomatic, often multiple, and most commonly affect the trunk of teenagers (Fig. 115-7). The halo phenomenon signifies self-immunologic regression of a preexisting melanocytic nevus. Lesions present with a central pink or brown nevus
C B A
1952
centrally, surrounded by a symmetric round or oval halo of depigmented skin. The central nevus may be small and typical of common acquired nevi or be large in dysplastic or congenital nevi. The radial zone of depigmented skin around the nevus ranges from less than 5 mm to 5 cm. Over time, the central nevus may lose its pigmentation and disappear followed by gradual repigmentation of the entire area. Other names for the halo phenomenon include leukoderma acquisitum centrifugum, Sutton nevus, leukopigmentary nevus, perinevoid vitiligo, and perinevoid leukoderma. An atypical gross appearance of the central lesion or an asymmetric halo of depigmentation, particularly in adults, should raise suspicion for a DN or melanoma. The Meyerson’s nevus presents as an asymptomatic or slightly pruritic, red, and slightly scaly eczematous halo around a central nevus. Lesions occur most often on the trunk and proximal extremities and may be multiple. Unlike halo nevi, the skin does not depigment, and regression of the nevus does not occur. Eczematous changes often self-resolve over the course of months. The spontaneous and concurrent development of multiple nevi, often similar in appearance, is termed eruptive nevi. This phenomenon has been described in the context of blistering diseases of the skin (immunobullous as well as erythema multiforme–Stevens-Johnson syndrome–toxic epidermal necrolysis spectrum), immunosuppression, neoplasia, and drugs (particularly chemotherapeutic and immune-modulating agents). Eruptive nevi may be of the common acquired type, Spitz, or blue nevus varieties.
RELATED PHYSICAL CONDITIONS
There is a general increased risk of melanoma in patients with multiple nevi. This risk is further increased in the setting of multiple atypical nevi or a personal or family history of melanoma. In patients with eruptive nevi, there may be findings of bullous disease or immunosuppression. Halo nevi, particularly when multiple, may be associated with concurrent or subsequent development of vitiligo or other autoimmune disease.37 Halo nevi are also more frequent in patients with Turner syndrome.38
COMPLICATIONS
Several studies demonstrate that increased numbers of nevi indicate an increased risk for melanoma development. In one large meta-analysis, the relative risk for people with high nevus counts (101–120 nevi) was 6.89 compared with those with low nevus counts (0–15 nevi).39 In addition, those with five atypical nevi had a relative risk of 6.52 compared with those with no atypical nevi.39 Other risk factors such as skin color, freckling, and patterns of sun exposure may be multiplicative to the number of nevi in increasing melanoma risk. Most melanoma arise from normal skin and thus increased number of nevi are associated with a general
20
melanoma risk. However, approximately 20% of melanomas are reported to have associated nevus elements suggesting a precursor pathway. In one study of 131 melanomas, a history of frequent sunburns predicted the greatest risk for nevus-associated melanoma.40
RISK FACTORS
RISK FACTORS
Environmental exposure to UV radiation appears to be the most critical risk factor for the development of acquired nevi. In a US population-based longitudinal study of nevi in children (n = 443), spending 5 to 6 hours per week outside between 10 am and 4 pm, painful sunburn(s), decreased UV barrier protection, and male gender were significantly associated with increased number of nevi.41 Intermittent intense sun exposure appears to impose greatest risk for nevus development. A randomized trial assessing sunscreen use on nevi development in white school-aged children also demonstrated a significant reduction in the number of nevi on intermittently sun-exposed body sites compared with control participants.42
Genetic factors appear to play a role in their development. The size, frequency, and distribution patterns of acquired nevi tend to aggregate in families. This observation is also well documented for atypical nevi in the setting of DN and melanoma syndromes (see dysplastic nevi).
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Common acquired nevi are clonal neoplasms, the majority of which demonstrate activating BRAF mutations. It is likely that this mutation is an early or initiating event in melanocytic neoplasia. All cells within common nevi have been shown to be fully clonal and contain the same heterozygous BRAF mutation by droplet digital polymerase chain reaction.43
Eruptive nevi occur in the setting of immunosuppression or chemotherapy. BRAF mutations have been identified in eruptive melanocytic nevi associated with 6-mercaptopurine therapy.44 However in one case, eruptive nevi of the Spitz type showed absence of BRAF and HRAS mutations in 39 nevi analyzed.45
This is not surprising because of the diverse molecular pathways that have been implicated in Spitz nevus development (see Spitz nevi). Halo nevi are nevi in which the body attempts an immune-mediated attack on nevus cells orchestrated by effector CD8+ cytotoxic T-lymphocytes. In this phenomenon, increased levels of interferon—γ–inducible chemokine pair CXCL10–CXCR3 have been demonstrated, similar to that seen in vitiligo.46 The precise trigger for this immunologic phenomenon in the absence of disease remains unclear. In patients with Turner syndrome, there was a significantly higher
1953
20
association of HLA-CW6 in those who developed halo nevi, suggesting a genetic predisposition.38
DIAGNOSIS
DIAGNOSIS
The diagnosis of common acquired nevi is usually made by clinical inspection, assessing that the lesion is relatively small, symmetrical, has even borders, is not ulcerated, and has a limited variety of colors and normal pigment network.
PATHOLOGY
The common junctional nevus is circumscribed and mostly nested at the basal layer of the epidermis (Figs. 115-8 and 115-9). Junctional melanocytes have pale or pigmented cytoplasm and small, monomorphous nuclei with inconspicuous nucleoli. In some common junctional nevi, the nests of melanocytes are positioned toward the bases of rete ridges, but in
others, the rete ridge pattern is unrelated. Epidermal melanocytes between junctional nests are disposed as single typical cells along the basal layer, with overall numbers equal to or slightly greater than that in adjacent skin. The epidermis is often hyperpigmented with lentiginous architecture (elongated and club-shaped rete pegs). In compound nevi (see Fig. 115-9), the epidermis may be normal or hyperplastic, with an appearance similar to seborrheic keratosis complete with horn cysts or epidermal verrucous hyperplasia similar to epidermal nevus. The dermal component of compound and intradermal nevi has an orderly progression from top to bottom, with larger epithelioid cells above (within the epidermis and superficial dermis) blending into a pattern of smaller round and spindled cells in the deeper dermis. This orderly progression of larger, more epithelioid cells in the superficial aspect of the nevus to smaller cells in its deep aspect is known as maturation. In the epidermis and superficial dermis, nevomelanocytes frequently contain melanin pigment. With
A B C
D E F
1954
20
Types of nevi
Junctional MN Compound MN Dermal MN
descent into the dermis (see Fig. 115-9), nevus cells become smaller and lose their pigmentation. Nevomelanocytes in the dermis have a monotonous similarity to one another within the same anatomic level and an overall symmetry of architecture from top to bottom and side to side. Multinucleated nevomelanocytes occur occasionally within the superficial and mid-dermal portions of the nevus. Nevomelanocytes in the deep dermis may be disposed as spindle cells within a collagenous framework that is loose, pale, and wavy in formations similar to a neurofibroma or sometimes disposed in concentrically arranged whorls resembling Meissner tactile corpuscles. The term neural nevus is used when the vast majority of the nevus demonstrates a neural phenotype. Sometimes dermal nevus cells aggregate around epithelial adnexal structures or lie as cords and strands in the superficial reticular dermis, making these “congenital pattern nevi” or “congenital-like nevi.” Such histologic features are not limited to nevi that were present since birth. Other findings identified in nevi include fibrous, mucinous, and fatty degeneration. Inflammatory cellular infiltrates in typical, stable acquired nevi are usually scanty or absent. Melaninladen macrophages are usually apparent in the superficial papillary dermis of nevi; their number usually proportional to the degree of melanin production. Asymmetry between the junctional and dermal elements, poor circumscription, and lamellar fibroplasia (features frequently seen in dysplastic nevi) are usually not prominent in common acquired nevi. Histopathologic artifacts include shrinkage clefts, which may resemble lymphatics or vascular spaces, may be prominent in the midportion of nevi and in areas with hemorrhage. Separation of sheets of nevomelanocytes into parallel rows may be caused by improper cutting. Local anesthesia injection directly into the nevus also may be associated with artifactual changes. The balloon cell nevus is a histopathologic variant of common acquired nevus, composed of peculiar foam cells comprising a portion or all of a given lesion.
In addition to clear cells with a single central basophilic nucleus, multinucleated balloon cells may be seen. Electron microscopy suggests that vacuolization of nevomelanocytes in balloon cell nevi is a degenerative change, with melanosome swelling, microvacuole formation in nevus granules, and loss of particulate martrix.47 In contrast to balloon cell melanoma, a maturation pattern is evident, and no cytologic atypia or significant mitotic activity is present. The combined nevus refers to the intermingling of two different nevus types in one lesion. Most such lesions are composed of either an acquired or congenital nevus and blue nevus. Recurrent melanocytic nevus is the name given to recurrent lesions after incomplete removal of a benign nevus. A markedly atypical clinical and histopathologic appearance may accompany this recurrence, making these lesions worrisome for possible melanoma. Clinically, the recurrent nevus is confined to the scar but may be markedly irregular in appearance. Recurrent nevi demonstrate melanocytic hyperplasia in a lentiginous and junctional pattern (often to a greater extent than the original nevus). Junctional melanocytes are frequently hyperpigmented and may display moderate cytologic atypia, significant architectural disorganization, and pagetoid growth, raising concern for melanoma. However, such features do not extend beyond the scar, and banal-appearing nevus cells may be seen within the underlying dermis. It is important to review the original histopathologic specimen to ensure that the findings can be solely attributed to nevus regeneration when making determinations for reexcision. No distinguishing histopathologic features have been described for eruptive nevi. In halo nevi, the usual histopathologic findings are a central nevus associated with an obscuring dermal lymphohistiocytic infiltrate and a surrounding depigmented zone totally or almost devoid of epidermal melanocytes. Immunohistochemical staining with melanocytic markers such as Melan-A or Sox-10 may help to identify residual epidermal melanocytes or residual dermal melanocytes obscured by the inflammatory infiltrate. Lymphocytes in halo nevi are mostly of the CD8+ subset.
1955
20
Normal-growing nevi in childhood and adolescence may show histologically alarming features, including more prominent epithelioid cell change of melanocytes and architectural variability of junctional melanocytic nests. Rare mitotic figures may also be evident. Site-related changes also influence the histopathology of common acquired nevi. These are known as special site nevi because of their unconventional histopathologic appearances. Special site locations include the scalp, ear, nipple, abdominal milk line, umbilicus, anogenital region, and acral surfaces. At these locations, there is often more architectural variability of junctional nests, some of which may be larger and discohesive. Limited pagetoid scatter can be seen in the central portions of some lesions, particularly on acral surfaces or in areas with frequent friction. Anogenital nevi commonly share architectural features with dysplastic nevi, including lamellar fibroplasia, bridging of rete by junctional nests, and lymphocytic infiltrates. Worrisome features for possible melanoma include pagetoid upward migration of cells in the epidermis, cytologic atypia of melanocytes (including irregularity of size and shape of cells and nuclear hyperchromasia), failure of the cells to “mature” in the deeper dermis, persistence of pigment production in the deep dermis, lack of symmetry, increased or deep dermal mitotic figures, focal areas of necrosis, and desmoplasia or fibroplasia.
SPECIAL TESTS
Special tests are not usually required in the gross and microscopic assessment of melanocytic or nevomelanocytic nevi. However, for patients who have eruptive nevi, given the association with immunosuppression, immunologic tests may be in order. Immunohistochemical profiles may be of value for difficult to diagnose lesions. Low Ki67 activity and loss of HMB45 in deeper dermal cells may help support a benign diagnosis. Compared with melanoma, common acquired nevi are genomically stable.48 Fluorescence in situ hybridization (café-au-lait) or comparative genomic hybridization (CGH) analysis may be useful in discriminating a nevus from nevoid melanoma.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-3.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
There may be relatively sudden changes in nevi that are unrelated to malignant transformation. Any single nevus that is noted to suddenly change or become symptomatic independently should be cause for concern. Causes of sudden changes in a nevus (color,
1956
Pigmented Lesions
Pigmented Lesions
■Solar lentigo
■Solar lentigo
■Lentigo simplex
■Lentigo simplex
■Café-au-lait macule
■Café-au-lait macule
■Blue nevus
■Blue nevus
■Pigmented fibrous histiocytoma (dermatofibroma)
■Pigmented fibrous histiocytoma (dermatofibroma)
■Kaposi sarcoma
■Kaposi sarcoma
■Pigmented basal cell carcinoma
■Pigmented basal cell carcinoma
■Pigmented actinic keratoses
■Pigmented actinic keratoses
■Mastocytoma
■Mastocytoma
■Seborrheic keratoses
■Seborrheic keratoses
■Epidermal nevus
■Epidermal nevus
■Subungual hematoma
■Subungual hematoma
■Supernumerary nipple
■Supernumerary nipple
■Pigmented spindle cell nevus
■Pigmented spindle cell nevus
■Spitz nevus
■Spitz nevus
■Sclerosing hemangioma
■Sclerosing hemangioma
■Pyogenic granuloma
■Pyogenic granuloma
■Dysplastic (atypical) melanocytic nevus
■Dysplastic (atypical) melanocytic nevus
■Cutaneous melanoma
■Cutaneous melanoma
■Nonpigmented or pink lesion
■Nonpigmented or pink lesion
■Basal cell carcinoma
■Basal cell carcinoma
■Fibrous papule
■Fibrous papule
■Verruca vulgaris
■Verruca vulgaris
■Molluscum contagiosum
■Molluscum contagiosum
■Dermal mucinosis
■Dermal mucinosis
■Spitz nevus (epithelioid cell nevus)
■Spitz nevus (epithelioid cell nevus)
■Appendageal tumors
■Appendageal tumors
■Clear cell acanthoma
■Clear cell acanthoma
■Large cell acanthoma
■Large cell acanthoma
■Other lesions with halo phenomenon
■Other lesions with halo phenomenon
■Congenital nevomelanocytic nevus
■Congenital nevomelanocytic nevus
■Melanoma
■Melanoma
■Histiocytoma
■Histiocytoma
■Molluscum contagiosum
■Molluscum contagiosum
■Flat wart
■Flat wart
■Acrochordon
■Acrochordon
■Basal cell epithelioma
■Basal cell epithelioma
■Neurofibroma
■Neurofibroma
■Congenital dermal melanocytosis (mongolian spot)
■Congenital dermal melanocytosis (mongolian spot)
■Blue nevus
■Blue nevus
■Lichen planus
■Lichen planus
■Sarcoidosis
■Sarcoidosis
■Psoriasis
■Psoriasis
■Angioma
■Angioma
■Angiokeratoma
■Angiokeratoma
surface, or size, with or without pain, itching, ulceration, or bleeding) over days or weeks include cystic dilation of a hair follicle, folliculitis, abscess, trauma, hemorrhage, and, in the case of a pedunculated nevus, strangulation and thrombosis. These benign causes of sudden change may require close observation for several weeks until resolution occurs or removal for histopathologic examination. The vast majority of acquired nevi are harmless. New nevi may continue to appear and disappear throughout life, but most develop during childhood and early adulthood. New or growing nevi in older individuals are more worrisome. Melanoma risk
appears to be related to the number and size of nevi; patients with numerous nevi, dysplastic nevi, and a personal or family history of melanoma should be closely monitored with periodic surveillance examinations for life.
MANAGEMENT
MANAGEMENT
TREATMENT
The vast majority of acquired common nevi require no treatment. Indications for removal of benign-appearing lesions may include cosmetic concerns or continual irritation. Lesions with worrisome clinical features need to be excised for histopathologic examination. Dermoscopy may be used to differentiate benign from potentially malignant features. Photographic surveillance can play a critical role in identifying change, or lack of change, in suspicious nevi. Although a benign-appearing nevus associated with halo depigmentation does not require excision, it is reasonable to recommend periodic examination of affected individuals for dysplastic nevi, vitiligo, and melanoma. Atypical-appearing central nevi, presence of an asymmetric halo, eccentric placement of a melanocytic lesion within a halo, or in the setting of dysplastic nevi or melanoma (personal or family history) suggest the need for histopathologic examination for melanoma. Cover-ups or sunscreens should be recommended for sun-exposed areas of depigmentation to prevent acute burn, chronic actinic damage, and UVRinduced carcinogenesis. Complete removal of nevi is best accomplished by excision. Leaving a partially excised nevus, regardless of the initial pathology, is fraught with potentially concerning consequences of repigmentation, regrowth, or both (see recurrent melanocytic nevus). Incisional biopsy is necessary at times, particularly for lesions that cannot be excised easily but require histopathologic diagnosis. Destructive modes of therapy (electrodesiccation, cryotherapy, dermabrasion, and laser) should be avoided. These destructive modes of therapy preclude histopathologic assessment of the treated nevi. They have the disadvantage of not providing tissue for histopathology. Although dermabrasion may eliminate pigmentation of nevi, residual nevomelanocytes in the dermis are to be expected, cosmetic outcome is often unpredictable, and recurrence with worrisome clinical features may complicate future management.
PREVENTION AND COUNSELING
There appears to be a direct relationship between the number of acquired nevi and sun exposure and a decrease with sunscreen use. Patients should be encouraged to minimize UVR overexposure without impeding day-to-day activities. Sensible UVR exposure includes confining outdoor activities to the early morning or late afternoon or evening and avoiding
20
the most intense UVR exposure occurring 2 hours on either side of noon. Cover-up clothing that blocks light transmission should be worn during intense UVR exposure. Clothing is often easier to put on than sunscreen and does not rapidly wear off with swimming or sweating. Effective sunscreens should be used as part of a comprehensive sun-protection program. Vitamin D supplementation should be recommended for patients who diligently practice UVR avoidance and protection.
BLUE NEVUS
AT-A-GLANCE
■ A group of lesions composed of deeply pigmented spindle or epithelioid melanocytes in the dermis; includes common blue, cellular blue, combined blue, and atypical cellular blue lesions
■ Lesions appear as blue, blue-gray, or blue-black papules, nodules, or plaques.
■ Lesions are generally acquired but may be congenital.
■ Cellular blue nevi may have an elevated risk for development of melanoma.
■ Related lesions include nevus of Ota/Ito, Mongolian spot, dermal dendritic hamartoma.
■ Initiating mutations in GNAQ or GNA11 are present in most blue nevi.
EPIDEMIOLOGY
EPIDEMIOLOGY
Blue nevi are present in approximately 1% to 2% of white adults and in 3% to 5% of Japanese adults. Women are more often affected than men. The vast majority of blue nevi present in the second decade of life and are single, small, deep-blue macules or papules less than 1 cm in diameter. Common blue nevi arise most often in adolescence and cellular blue nevi before age 40 years. Congenital onset or those that appear in the first few years of life are less common.
CLINICAL FEATURES
CLINICAL FEATURES
The most frequent sites for blue nevi are on the dorsal hands and feet, scalp, and buttocks or sacral skin. The blue hue seen in many lesions comes from the Tyndall effect, the result of the refraction of light reflected from the nevus by the overlying dermis. Blue nevi have been reported to rarely occur in the oral mucosa, uterine cervix, vagina, spermatic cord, prostate, and lymph nodes, and several clinical variants have been described: eruptive, plaquelike,
1957
20
linear, agminate, disseminated, satellite, familial, and targetoid.49
CUTANEOUS FINDINGS
Most blue nevi are blue, blue-gray, or blue-black smooth surfaced papules or nodules (Fig. 115-10). Common blue nevi are deeply pigmented small lesions, usually less than 1 cm in diameter. Cellular blue nevi have a similar color but are often larger plaques or nodules greater than 1 cm. Blue nevi tend to be firm, reflecting their dermal location and often fibrotic stroma. Hypomelanotic blue nevus is a rare variant in which not much melanin
A B
C D
pigment is produced. The resultant lesions are flattish skin-colored firm papules or plaques. Many group the dermal melanocytoses, conditions in which there are pigmented dendritic melanocytes, in the blue nevus family. Nevus of Ota and Ito share similar underlying defects to blue nevi and are also commonly acquired (in early childhood, often before age 1 year or around puberty) but are far more extensive, encompassing a portion of the trigeminal (ophthalmic and maxillary) and brachial (posterior supraclavicular and lateral cutaneous) nerve distributions, respectively. Dermal melanocyte hamartoma presents at birth as coalescing macules, resulting in diffuse blue-gray pigmentation. Mongolian spot is usually present at birth or within the first few weeks of life
1958
and centered over the lumbosacral area. Mongolian spots typically regress in early childhood but may persist in approximately 10% of cases. Nevus of Ota/Ito typically persist into adulthood. Acquired adult variants of dermal melanocytosis rarely occur.
RELATED PHYSICAL CONDITIONS
Multiple blue nevi and epithelioid blue nevi may be associated with lentigines, cardiac myxoma, and mucocutaneous myxomas (Carney complex/LAMB syndrome [lentigines, atrial myxomas, mucocutaneous myxomas, and blue nevi]). Extensive dermal melanocytosis may be associated with phakomatosis pigmentovascularis.
COMPLICATIONS
Malignant blue nevus (melanoma) may arise de novo but more often arises in contiguity with a cellular blue nevus. Rarely, there is malignant transformation of a dermal melanocytosis.50 This event may present as an expanding dermal or subcutaneous nodule with or without ulceration.
RISK FACTORS
RISK FACTORS
Other than Carney complex/LAMB syndrome and phakomatosis pigmentovascularis, there are no known risk factors for blue nevi. The risk of UVR in the development of blue nevi is unknown.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Most blue nevi have initiating mutations in GNAQ and to a lesser extent GNA11. These mutations result in loss of GTPase activity and constitutive activation of the MAPK pathway, resulting in increased cellular proliferation. Although the frequency of these mutations varies among studies, mutation in the GNAQ gene has been identified in up to 87% of blue nevi, almost all of them in codon 209.51
The distribution of blue nevi is thought to parallel sites of colonization by active non-neoplastic pigmented bipolar dermal melanocytes during embryogenesis.19 These cells typically migrate and disappear during embryonic life, but occasionally incidental pigmented dendritic cells can be seen in biopsies from the scalp, upper face, dorsal hands or feet, and sacrum. GNAQ mutations have been reported in nevus of Ota,52 and more recently mosaic activating mutations in GNA11 and GNAQ were discovered in the pigmented lesions of phakomatosis pigmentovascularis with extensive dermal melanocytosis.53 Thus, the molecular mutational profile of dermal melanocytoses appears to parallel that of blue nevi.
20
In contrast, neither GNAQ nor GNA11 mutations have been documented in deep penetrating nevi; rather, HRAS mutations were seen in 6% of lesions in one study, implicating that these lesions may be more related to Spitz nevi.51 Recently, deep penetrating nevi have been found to harbor activating mutations in both the MAPK and β-catenin pathways.54 There is also a subgroup of lesions with mixed morphologic features of blue nevus and Spitz nevus. Evidence mounts that such “Blitz” nevi are best classified as blue melanocytic neoplasms because of their high frequency (57%) of GNAQ and GNA11 mutations.55
Pigmented epithelioid melanocytoma is indistinguishable from epithelioid blue nevus of Carney complex. In the sporadic setting, it is considered an intermediate-grade melanocytic tumor that demonstrates a propensity to spread to regional lymph nodes but has a favorable long-term clinical course.56 Those that occur in the setting of Carney complex behave in an entirely benign fashion. In both settings, such lesions are linked to mutations of protein kinase A regulatory subunit type 1 α (PRKAR1α) gene.57 Protein kinase C alpha isoform (PRKCA) fusion genes have also been recently reported in pigmented epithelioid melanocytoma.58
DIAGNOSIS
DIAGNOSIS
The diagnosis of blue nevus is sometimes made clinically when a small, very dark or blue lesion is found in a typical location for a common blue nevus. For larger lesions and those in less typical locations, it is customary to confirm the diagnosis by biopsy.
PATHOLOGY
All types of blue nevus have components that include some of the following: deeply pigmented dendritic melanocytes, spindled and less pigmented melanocytes, oval melanocytes, melanophages, and fibrotic stroma (Fig. 115-11). Nevus cells may show perivascular or periadnexal accentuation. Almost all blue nevi lack a junctional component. Very occasionally, one can see single dendritic melanocytes in increased number along the DEJ (so-called compound blue nevus). Another exception is combined blue nevus, in which another form of nevus is contiguous and a junctional component occurs (eg, common or congenital nevus). The stereotypic common blue nevus is an inverted dermal wedge-shaped mass in which pigmented dendritic melanocytes are admixed with melanophages within a fibrotic stroma. The prototypical cellular blue nevus has vertically oriented dumbbell-shaped masses of melanocytes that protrude into the subcutis. The superficial dermis often contains a fibrotic stroma in which there are dendritic melanocytes and melanophages, but the definitional component is the presence of larger streaming aggregates of oval melanocytes. These cells usually have only scant melanin. Multinucleated melanocytes
1959
20
A B
C D
are sometimes present within aggregates. The presence of cells with large central nucleoli, more than a few mitotic figures per section, atypical mitotic figures, necrosis, or lymphocytic infiltrates evokes concern for melanoma. Sparsely scattered mid and deep dermal dendritic melanocytes oriented parallel to the skin surface typify the dermal melanocytoses. The cells of blue nevus are usually positive with S100 immunohistochemistry, stain strongly with Melan-A/ Mart-1, and are positive for HMB-45. They have a low proliferation rate.
1960
Deep penetrating nevi may clinically simulate a blue nevus but can be distinguished histopathologically. They are named for their tendency to extend through most of the thickness of the dermis, and some lesions reach the superficial subcutis. They are usually wedge shaped, with the apex sometimes surrounding a folliculosebaceous unit. They are composed of nests of large, oval melanocytes with abundant, pale vacuolated cytoplasm with dusty melanin and moderately enlarged nuclei. Mitoses are few, although two or three can occur in a single section. Combined deep penetrating nevi have a component of common
nevus or congenital-like nevus to the side, above, or both. The criteria for distinguishing deep penetrating nevi from intermediate-grade lesions, in which metastases are rare, and higher grade lesions are still being developed. Benign epithelioid blue nevi of Carney complex are histologically indistinguishable from pigmented epithelioid melanocytoma, which occurs in the sporadic setting.56 It is characterized by a mostly dermal nodular and sheetlike proliferation of enlarged epithelioid melanocytes with round nuclei, conspicuous nucleoli, and heavily pigmented cytoplasm. Numerous admixed melanophages are present. Some melanocytes show a spindled morphology, particularly at the periphery of the lesion. Occasional mitotic figures may be evident in some lesions. No morphologic criteria have been determined to reliably predict metastatic potential in sporadically occurring pigmented epithelioid melanocytoma.
SPECIAL TESTS
Imaging tests of the heart may be required if there is concern for Carney complex/myxoma syndrome/ LAMB syndrome. Mutation analysis can be helpful diagnostically for distinguishing cellular blue nevi or atypical blue nevi from blue nevus–like melanoma.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-4.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Blue nevi are benign lesions, and their only adverse prognostic event is the development of melanoma within one. This more frequently occurs in cellular blue nevi. Melanomas associated with or mimicking cellular blue nevi have been demonstrated to have a propensity for the scalp and a high frequency of GNA11 mutations with loss of BAP1 expression.59
■Pigmented spindle cell nevus
■Pigmented spindle cell nevus
■Tattoo (traumatic, radiation port marker)
■Tattoo (traumatic, radiation port marker)
■Primary or metastatic melanoma
■Primary or metastatic melanoma
■Glomus tumor
■Glomus tumor
■Pyogenic granuloma
■Pyogenic granuloma
■Sclerosing hemangioma
■Sclerosing hemangioma
■Dermatofibroma
■Dermatofibroma
■Ochronosis
■Ochronosis
20
MANAGEMENT
MANAGEMENT
TREATMENT
Stable common blue nevi usually do not require therapy. However, clinical change of a blue nevus, such as sudden appearance of a new nodule, enlargement of an existing nevus, or a large or atypical clinical appearance should prompt histopathologic examination. Cellular blue nevi, particularly in adults, should be evaluated for excision because of the small risk of malignant transformation. Excision should include subcutaneous fat to ensure removal of the deeper melanocytic components that are often present in cellular blue nevi. The prognosis for deep penetrating nevi is excellent, although there may be a very low conversion rate to deep penetrating-like melanoma for lesions that are not completely removed. What this rate is and how much higher it is than for other forms of nevus are unknown. Some dermatopathologists advocate complete removal of deep penetrating nevi, but others regard clinical removal as sufficient. Pigmented epithelioid melanocytoma occurring in the sporadic setting are typically treated similar to melanoma, with wide excision and sentinel lymph node biopsy.
PREVENTION AND COUNSELING
There are no known preventative measures. As with other nevi, it is reasonable to minimize excessive UVR exposure.
PIGMENTED SPINDLE CELL NEVUS
AT-A-GLANCE
■ Synonym: Reed nevus
■ Acquired, benign melanocytic tumor composed of heavily pigmented spindle-shaped melanocytes in nests confined primarily to the epidermis
■ Lesions are jet black often with “starburst” appearance on dermoscopy.
■ They may develop quickly and then stabilize.
■ Malignant degeneration is thought to be rare.
EPIDEMIOLOGY
EPIDEMIOLOGY
The pigmented spindle cell nevus (PSCN) presents most commonly in the third decade of life. The mean age at presentation has been reported to be 25.3 years,
1961
20
ranging from 2.5 to 56.0 years of age.60 Similar age ranges have been reported in other studies.61 Female patients outnumber male patients with reported ratios of up to 2:1.60,62 The majority of these lesions are found on the extremities with reported frequencies of 67.0%,60
69.6%,62 and 75.0%.61 There is a preference for the lower extremity, particularly the thigh.61
CLINICAL FEATURES
CLINICAL FEATURES
PSCN was first described by Reed in 1975.63 Many authors consider it a variant of Spitz nevus, but others define it as a distinct entity. At presentation, patients often note that the lesion has increased in size, prompting biopsy.61,62 If allowed to fully develop, they are thought to generally remain stable over time.
CUTANEOUS FINDINGS
PSCN classically presents as a sharply circumscribed darkly pigmented papule, usually less than 7 mm in diameter. They are jet-black but may have shades of blue, gray, or brown (Fig. 115-12). Dermoscopically, most have streaks or pseudopods, giving the lesion a starburst appearance; others may have a globular pattern with reticular depigmentation.64
RELATED PHYSICAL CONDITIONS
There are no known associations.
B A
1962
COMPLICATIONS
There are no reported complications, but misinterpretation as a melanoma may result in overtreatment.
RISK FACTORS
RISK FACTORS
There are no known risk factors.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Although BRAF mutation and gene fusions have been detected, these changes are also present in other types of acquired and Spitz nevi, respectively. No known specific mutation has been identified for PSCN.
DIAGNOSIS
DIAGNOSIS
The diagnosis may be suspected given the clinical scenario and supportive dermoscopic features. However, the diagnosis should be confirmed by biopsy.
PATHOLOGY
The PSCN is a sharply circumscribed lesion composed of fascicles of uniform pigment-synthesizing melanocytes with spindled appearance along the junction and to a lesser extent the superficial dermis (Fig. 115-13). Melanocytes have uniform nuclei and small nucleoli. Occasionally, there is an admixture of epithelioid appearing cells. Pagetoid cells may be seen but are usually limited to the central portion of the nevus. Extension of the spindle cells along skin adnexal structures is relatively common. There are invariably pigment-laden macrophages in the papillary dermis with a mild perivascular infiltrate of lymphocytes. Atypical variants of PSCN exist in which there are architectural alterations and striking cellular atypia, raising a differential diagnosis of melanoma.62
SPECIAL TESTS
In cases with atypical histologic features, immunohistochemical markers (Ki-67, cyclin-D1, survivin) and FISH have shown utility in distinguishing PSCN from melanoma.65
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-5.
A B
20
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
PSCN is considered benign. No local recurrence or distant spread was noted for 38 patients followed for an average of 14 months.60 In another study, 57 patients were followed for an average of 6 years, and again no local recurrence or metastasis was noted.61
MANAGEMENT
MANAGEMENT
TREATMENT
Given the difficulties in the histopathologic differentiation from melanoma in some cases, these lesions should be considered for excision to attain histologically free margins.
■Spitz tumor
■Spitz tumor
■Blue nevus
■Blue nevus
■Hematoma
■Hematoma
■Dysplastic junctional nevus
■Dysplastic junctional nevus
■Hypermelanotic nevomelanocytic nevus
■Hypermelanotic nevomelanocytic nevus
■Combined nevomelanocytic/blue nevus
■Combined nevomelanocytic/blue nevus
■Melanoma
■Melanoma
PREVENTION AND COUNSELING
There are no known preventative measures. The role of UVR exposure in the development of PSCN is unknown.
SPITZ NEVUS
AT-A-GLANCE
■ Spitz nevi represent a spectrum of unique, usually acquired lesions, exhibiting epithelioid and often spindle-shaped melanocytic cells with abundant eosinophilic cytoplasm, large nuclei, and often prominent nucleoli. The often develop in the epidermis and dermis or may be purely intradermal and even desmoplastic. Atypical variants exist.
■ Clinically, they often present as red, domeshaped papules. Some have varying degrees of pigmentation.
■ Spitz nevi are thought to develop quickly and then stabilize. Their clinical presentation and histopathology can cause diagnostic confusion for melanoma.
■ Synonyms: spindle and epithelioid cell nevus
EPIDEMIOLOGY
EPIDEMIOLOGY
The annual incidence rate of Spitz nevi is approximately 1.4 to 1.6 cases per 100,000 individuals.66 In a
1963
20
series reported by Weedon and Little, 70% of 211 Spitz nevi occurred in patients younger than 20 years of age.67 This higher pediatric prevalence of Spitz nevi is confirmed in most large epidemiologic studies. There appears to be no gender predilection for Spitz nevi in children. Whites are more commonly affected than other ethnicities.
CLINICAL FEATURES
CLINICAL FEATURES
Spitz nevi typically begin with an initial phase of growth, with either gradual or relatively rapid enlargement followed by a stable quiescent period. The presence of a new or growing lesion in the pediatric population often prompts tissue biopsy.
CUTANEOUS FINDINGS
The most common variety of Spitz nevus is solitary, asymptomatic, pink or red, hairless, firm, and dome shaped (Fig. 115-14). Some Spitz nevi may resemble a keloid or pyogenic granuloma when eroded. The surface is commonly smooth, and the borders may fade into surrounding skin. Verrucous, scaly, stippled, and crusted lesions may occur. Spitz nevi are usually asymptomatic, but pruritus, tenderness, or bleeding is sometimes noted. The halo phenomenon may occur in Spitz nevi as they do in common acquired nevi. Spitz nevi can also present as widespread eruptive lesions or in a grouped manner as multiple agminated lesions consisting of red, red-brown, brown, or dark-brown papules or nodules, with a fine stippled surface. Agminated Spitz nevi often occur in the early years of life within a background of congenital (sometimes acquired) macular pigmentation (nevus spilus) or occasionally within a hypopigmented plaque. Spitz nevi may also develop as single or multiple lesions in a large CMN.
B A
The diameter of Spitz nevi ranges from several millimeters to several centimeters. They have a predilection for the head and neck and extremities, although truncal lesions are not uncommon. Spitz nevi tend to spare the palms, soles, and mucous membranes.
RELATED PHYSICAL FINDINGS
Multiple epithelioid Spitz nevi with loss of BAP-1 expression may occur as part of a familial cancer syndrome.68,69
COMPLICATIONS
Misinterpretation of benign or malignant behavior of the lesion could result in unnecessary or insufficient treatment, respectively. Spitz nevi rarely acquire more mutational aberrations over time and thus may attain metastatic (atypical Spitz tumor) or malignant potential (Spitzoid melanoma).
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Unlike common acquired nevi, congenital nevi, and melanoma, which frequently harbor BRAF or NRAS mutations, Spitz tumors often either harbor HRAS mutations or demonstrate genomic rearrangements involving kinase genes (ALK, ROS1, NTRK1, BRAF, RET, MET).70 The combination of BAP1 loss and BRAF mutation has been shown to be characteristic of a subset of atypical Spitz tumors that display distinct histopathologic features.69 Such lesions often occur sporadically via somatic mutation, although a subset of BAP1-deficient melanocytic neoplasms arises in the setting of a familial germline mutation, resulting in BAP1-associated cancer susceptibility syndrome. Affected individuals are at increased risk for cutaneous and uveal melanoma, mesothelioma,
C
1964
A B
20
renal cell carcinoma, cholangiocarcinoma, and other malignancies.71
DIAGNOSIS
DIAGNOSIS
PATHOLOGY
Spitz nevi are characterized by melanocytic cells with large epithelioid nuclei, often with prominent nucleoli and surrounded by a rim of eosinophilic cytoplasm with “ground-glass” appearance (Fig. 115-15). These lesions are well-circumscribed and symmetric from side to side and from top to bottom. In contrast to melanoma, the melanocytic cells in Spitz nevi show progressive maturation with increasing depth, becoming smaller with the overall distribution of cells in the dermis being wedge shaped, with narrowing of the wedge toward the subcutaneous fat. Purely junctional and dermal lesions also occur. When there is a junctional component, there is often epidermal hyperplasia. Small intraepidermal eosinophilic globules (Kamino bodies), which are positive for periodic acid–Schiff and diastase resistant (resembling colloid bodies), may be seen. Melanocytic elements are usually well nested, although there may be permeation of the epidermis by single cells or small groups of cells. Pagetoid cells are more commonly encountered in the center of the lesion. There are often artifactual clefts between melanocytic nests and the epidermis. Ovoid junctional nests often show vertical streaming of the constituent cells.
In most cases, dermal inflammation is mild and confined to a sparse perivascular lymphocytic infiltrate. However, more intense infiltrates including a halo may occur. Atypical features including nuclear pleomorphism, increased or atypical or deep mitoses, asymmetry, and lack of maturation should raise concern for an atypical Spitz tumor or melanoma.
SPECIAL TESTING
Immunohistochemical studies may be helpful when the differential diagnosis includes Spitzoid melanoma. In most Spitz nevi, there is full or partial retention of p16 staining, but Spitzoid melanomas tend to lose p16 expression. Ki-67 proliferation marker is low in nevi but elevated in melanoma. In difficult cases, CGH or FISH studies may help better define the biologic potential of a given lesion.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-6.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
The natural history of the Spitz nevus is that most have an initial growth phase and then remain stable over time. However, a small subset may show atypical
1965
20
Nonpigmented or Red
■Amelanotic melanoma
■Juvenile xanthogranuloma
■Hemangioma
■Pyogenic granuloma
■Molluscum contagiosum
■Intradermal nevus
■Solitary mastocytoma
■Granuloma
■Clear cell acanthoma
■Insect bite reaction
■Dermatofibroma
■Appendageal tumor
■Keloid
Pigmented
■Blue nevus
■Deep penetrating nevus
■Hypermelanotic intradermal nevus
■Melanoma
■Hematoma
Warty Variants
Warty Variants
■Verruca vulgaris
■Verruca vulgaris
■Seborrheic keratoses
■Seborrheic keratoses
■Epidermal nevus
■Epidermal nevus
■Epidermolytic acanthoma
■Epidermolytic acanthoma
histopathologic features corresponding with accrual of additional genomic aberrations (atypical Spitz tumor or Spitzoid melanoma). Spitz tumors in the adult population should be viewed with suspicion, particularly if they are new or changing.
MANAGEMENT
MANAGEMENT
TREATMENT
Complete excision with histologically clear margins is generally sufficient treatment for benign Spitz nevi. Given the difficulty of confidently excluding the possibility of melanoma in certain cases, such as those with atypical histopathologic features, an even wider margin of normal skin may be prudent for worrisome lesions. The role of sentinel lymph node biopsies for atypical Spitz tumors is controversial because tumor cells may be present in the regional lymph nodes but not have the biologic significance or poor prognosis associated with metastatic melanoma. Management of patients who have numerous Spitz nevi requires individual judgment and periodic surveillance for new or unstable lesions.
PREVENTION
There are no known preventative measures for the development of Spitz nevus.
1966
NODAL NEVI
AT-A-GLANCE
■ Benign melanocytic neoplasia present in a lymph node. Nevomelanocytes are characteristically located in the capsule.
■ They are generally asymptomatic and found incidentally as a result of lymph node removal.
■ Cells may be deposited passively into the node from a cutaneous melanocytic lesion. It is also possible that abnormal migration pathways result in the nevomelanocytes taking up residence in lymph nodes during embryonic development.
■ The presence of melanocytic cells in nodal tissue may create difficulties for pathologists evaluating sentinel node biopsies in patients with cutaneous melanoma.
EPIDEMIOLOGY
EPIDEMIOLOGY
Nevomelanocytes can be identified in lymph nodes with a frequency ranging from 0.3% to 7.3% in lymphadenectomies not related to melanoma and up to 22% in regional nodes removed because of melanoma.72 A significant association has also been noted for the presence of cutaneous nevomelanocytic nevi in the zones of skin drained by lymph nodes that were found to include nevomelanocytes.73 This association was strongest with congenital nevi. In most cases, nodal nevomelanocytes phenotypically resemble common acquired nevomelanocytic nevi, but nevi with congenital features, blue nevi, cellular blue, and Spitz nevi have all also been reported to involve regional lymph nodes.74
CLINICAL FEATURES
CLINICAL FEATURES
HISTORY
Generally, nodal nevi are identified in lymph nodes that are removed for other reasons, usually melanoma or breast cancer, but these benign cells are also identified in nodes removed for other reasons. Patients do not note symptoms related to nodal nevi.
CUTANEOUS FINDINGS
Melanocytic neoplasia in the form of melanoma or melanocytic nevi may be present at the cutaneous site corresponding to the draining lymph node basin.
RELATED PHYSICAL FINDINGS
Lymph nodes harboring benign nodal nevi are most commonly seen in patients undergoing lymphadenectomy for melanoma but are also seen in lymphadenectomy specimens for breast carcinoma and other causes.
COMPLICATIONS
Complications, such as scarring or lymphedema, may be the consequence of lymphadenectomy. Misinterpretation of benign nodal deposits as malignant could result in unnecessary regional lymph node dissection and treatment with systemic agents. Misinterpretation of malignant melanocytes as benign in lymph nodes may lead to under treatment.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
There are two prevailing theories as to the mechanism by which nevomelanocytes appear in regional lymph nodes. The first theory is that during development, melanoblasts get trapped in developing nodal tissues. Some support for this theory could be based on the fact that nodal nevi can be found in association with CMN. This observation suggests that there is an opportunity for nevomelanocytes to be deposited during development. Furthermore, blue nevus cells can be found in tissues such as prostate, cervix, vagina, spermatic cord, and seminal vesicles.74 Thus, aberrant migration and differentiation of melanocytic cells does occur. The second theory suggests that there may be passive transfer from the cutaneous lesion to the lymph node. Substances such as carbon, tattoo ink, and radioactive colloid are readily transferred to the draining lymph node. It is reasonable to assume that loosely adherent nevomelanocytes could also traverse the same path. In fact, nevomelanocytes have been noted in lymph channels.74 In the lymph node, nevomelanocytes are generally identified in the capsule, but they can also be found in the parenchyma.72
It is not known how nevomelanocytes get into the capsule, but it is reasonable to assume that these cells migrate from the parenchyma into the capsule. It is important to note that melanoma cells can also be found in the capsule, so it is rational to assume that entry into the capsule is not limited to a developmental event. The fact that nevomelanocytes in regional lymph nodes are highly correlated with the presence of nevomelanocytic nevi in the skin supports the concept that these cells may arrive in lymph nodes via dissemination from benign cutaneous lesions.75
20
■Melanoma
■Melanoma
■Cells from another neoplastic source
■Cells from another neoplastic source
■Foreign body deposit (tattoo ink, carbon)
■Foreign body deposit (tattoo ink, carbon)
DIAGNOSIS
DIAGNOSIS
PATHOLOGY
Pathology often reveals nevomelanocytes largely confined to the nodal capsule or trabeculae. However, cells may also be noted in the parenchyma. Nodal nevi should lack cellular atypia and mitotic activity.
SPECIAL TESTING
The use of standard immunohistochemical tests may help identify the location and cellular features of nevomelanocytes in lymph node tissue sections. Weak or negative staining for HMB-45, lack of proliferative markers (Ki67), and strong p16 expression support a benign diagnosis.76,77 A recent study determined that fatty acid synthase and acetyl-CoA carboxylase are not expressed in intracapular nodal nevi but are expressed in metastatic melanoma.78
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-7.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
If the lymph node deposits are determined to be benign, no further treatment is warranted.
TREATMENT
None required for benign nodal nevi.
LENTIGO SIMPLEX
AT-A-GLANCE
■ Clinically, lesions are hyperpigmented macules, occurring alone, in focal clusters (agminated), or have a generalized distribution. They occur on the skin, conjunctivae and mucous membranes.
1967
(Continued)
20
AT-A-GLANCE (Continued)
Continued
AT A GLANCE (
)
■ They commonly develop in early childhood.
■ Multiple lentigines may be associated with somatic abnormalities.
■ Synonyms: simple lentigo, melanotic macule, lentiginosis. Other names for agminated lentigines include unilateral lentigines, partial unilateral lentiginosis, lentiginous mosaicism, and segmental lentiginosis.
■ Other lesions in which epidermal melanocytic hyperplasia may be noted, where overlap may exist with simple lentigines, include café-au-lait macules, melanoacanthoma, labial melanotic macule, melasma, and inflammatory/cytokineinduced proliferation.
EPIDEMIOLOGY
EPIDEMIOLOGY
Lentigo simplex is a very common melanocytic lesion, present either at birth or developing later in childhood or adulthood. Although acral lentigo is more prevalent in blacks, lentigo simplex does not have a racial or gender predilection. The incidence of agminated and generalized lentiginosis is rare.
CLINICAL FEATURES
CLINICAL FEATURES
Lentigo simplex occurs on the skin, conjunctivae, and mucocutaneous surfaces. They may develop as early as the first decade of life (juvenile lentigo) and arise on both sun-exposed and sun-protected sites. Lentigines may develop in a unilateral, agminated (partial or segmental lentigines), or generalized distribution (lentigines profuse) and may occur as an isolated phenomenon or in associated with a number of inherited disorders,
B A
including LEOPARD (lentigines, electrocardiographic conduction abnormalities, ocular hypertelorism, pulmonary valve stenosis, abnormalities of genitalia, growth retardation, and sensorineural deafness) syndrome, Carney syndrome, Peutz-Jeghers syndrome, Laugier- Hunziker syndrome (idiopathic lenticular mucocutaneous pigmentation), and centrofacial lentiginosis.
CUTANEOUS FINDINGS
Lentigo simplex are usually sharply circumscribed macules, measuring 1 to 5 mm in size, with uniform light brown to black pigmentation. If partial or generalized lentiginosis is present, the specific pattern and clinical course of lesions may be suggestive of a specific inherited syndrome. In LEOPARD syndrome, lentigines are often absent during the first years of life; patients subsequently may develop hundreds of lentigines during childhood, including on the genitalia, conjunctiva, oral cavity, palms, and soles. In Peutz-Jeghers syndrome, lentigines are commonly present on the buccal mucosa, lips, perioral skin, and ventral surfaces of the hands and feet. Although cutaneous lesions may fade at puberty, oral lentigines usually persist into adulthood. In centrofacial lentiginosis, lentigines are characteristically distributed in a horizontal band across the face. In Laugier-Hunziker syndrome, lentigines predominantly occur on the lips, hard and soft palates, fingers, nail matrix and palms, and infrequently at other sites, including conjunctivae and genitalia. In LAMB (lentigines, atrial myxoma, mucocutaneous myxomas and blue nevi) syndrome, lentigines mainly occur on the face, trunk, and genitalia as tan to black macules (Fig. 115-16). Agminated lentigines are congenital or develop shortly after birth and often are confined to a localized area of the skin, often in a segmental distribution and frequently demonstrate a curvilinear or swirled pattern (Fig. 115-17).
1968
20
B A C
RELATED PHYSICAL FINDINGS
In addition to several inherited syndromes, lentigines may be associated with Addison disease; topical immunosuppressive calcineurin inhibitors, such as tacrolimus; and type 1 hereditary punctate palmoplantar keratoderma.79,80 Eruptive acral lentigines have been reported with synchronous malignancies, including gastric adenocarcinoma, mammary carcinoma, large-cell lymphoma, non-Hogkin lymphoma, melanoma, and AIDS.81-84
COMPLICATIONS
Complications may arise from associated syndromes; however, lentigines are benign without any direct complications.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The mechanisms underlying lentigo simplex formation are not well understood. An increased density of melanocytes suggests that melanocyte homeostasis is disrupted in lentigo simplex. Additionally, the presence of melanin macroglobules in melanocytes suggests that melanization is dysregulated and may contribute to the formation of lentigines. The presence of lentigines in association with various inherited syndromes underscores the likelihood that lentigo development may be influenced by a variety of different genetic and developmental factors. Interestingly, lentigo simplex does not harbor characteristic mutations found in solar lentigo, psoralen UVA (PUVA) lentigines, and common acquired nevi. In a study by Hafner and coworkers, lentiginous
junctional nevi, compound, and intradermal nevi harbored BRAFV600E mutations in 17%, 55%, and 78% of cases, respectively, but lentigo simplex was shown to lack BRAFV600E mutation.85 Likewise, lentigo simplex lacks FGFR3 and PIK3CA mutations, which are frequently present in solar lentigo and PUVA lentigines.85,86
DIAGNOSIS
DIAGNOSIS
PATHOLOGY
Histologic sections of lentigo simplex show slight to moderate elongation of rete ridges, basilar melanocytic hyperplasia, and increased pigmentation within the epidermis and melanophages in the papillary dermis. Melanocytes lack atypia. Rarely, giant pigment granules (melanin macroglobules) may be present. Frequently, a lymphohistiocytic infiltrate is present within the superficial dermis. Commonly, a junctional nevus and lentigo may coexist (lentiginous junctional nevus). Solar lentigo characteristically shows greater elongation of rete ridges and prominent solar elastosis with the papillary dermis.
LABORATORY TESTING
Immunohistochemistry to highlight melanocyte density with the epidermis (MITF, Mart-1, Sox10) is typically not necessary for histologic diagnosis.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
1969
See Table 115-8.
20
Solitary
■Solar lentigo
■Ephelis
■Junctional nevomelanocytic nevus
■Dysplastic (atypical) melanocytic nevus
■Café-au-lait macule
■Melanoma (lentigo maligna)
Grouped
Grouped
■Agminated nevomelanocytic nevi or lentigines
■Agminated nevomelanocytic nevi or lentigines
■Nevus spilus
■Nevus spilus
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Generally, when present, lentigo simplex are relatively stable. During pregnancy, lentigines may become more conspicuous. There is not an association with progression to nevomelanocytic nevus or increased risk of malignant transformation to melanoma.
MANAGEMENT
MANAGEMENT
TREATMENT
Treatment is not necessary for lentigo simplex. Cosmetic removal has been completed with cryotherapy or other approaches, including Q-switched laser.
PREVENTION
There are no known preventive measures for lentigo simplex. Avoidance of sun exposure and UVR does not reduce the risk of development of lentigo simplex.
SOLAR LENTIGO
AT-A-GLANCE
■ Solar lentigines are hyperpigmented macules that occur on photodamaged skin, singly or as multiple lesions.
■ They predominantly develop in older individuals. Children with xeroderma pigmentosum develop solar lentigines during the first year of life because of increased susceptibility to UV radiation.
■ Histology shows elongation of rete ridges with budlike processes, hyperpigmentation, normal or slightly increased melanocytes, and dermal solar elastosis.
1970
■ Solar lentigines are benign. Development is associated with increased risk of UV-related cutaneous malignancies, including squamous cell carcinoma, basal cell carcinoma, and melanoma.
■ Synonyms: actinic lentigo, sun-induced freckle, liver spot, lentigo senilis, senile lentigo
EPIDEMIOLOGY
EPIDEMIOLOGY
The prevalence of solar lentigines is strongly associated with older age and photodamage. They mainly arise on sun-exposed skin of those with white skin and Asians. More than 90% of those with white skin develop a solar lentigo by the age of 50 years.87 Multiple lentigines on the face appear to be associated with dark skin (types III and IV).88,89 In addition to age and sun exposure, they are associated with history of facial ephelides (freckles), tanning capacity, and concurrent use of oral contraceptive therapy.88
Chronic psoralen photochemotherapy may induce lentigines, termed PUVA lentigines. A study of 1380 adults undergoing PUVA treatment for psoriasis observed buttock lentigines in 53% of patients, arising an average of 5.7 years after initiating treatment (Fig. 115-18).90 PUVA lentigines are associated with total number of treatments, male gender, fair-skin, and older age.90 Additionally, lentigines are associated with UVA exposure from artificial sunbed use.91
CLINICAL FEATURES
CLINICAL FEATURES
Solar lentigines are acquired hyperpigmented lesions that generally arise on sun-exposed sites on lightskinned individuals. They most commonly occur on the face and dorsal surfaces of the forearm and hand.
CUTANEOUS FINDINGS
Solar lentigines arise on skin exposed to natural sunlight or artificial sources of UV radiation. They have well-defined, irregular borders, with a tendency to coalesce at sites of severe sun damage where multiple lesions may be present (Fig. 115-19). They range in size from less than 1 mm to several centimeters in greatest dimension. Lesions are light to dark brown in color. Ink spot lentigo (reticulated black solar lentigo) is a variant with black pigmentation. Unlike solar lentigo, PUVA lentigines commonly develop on sun-protected sites, including the buttocks and genitalia (see Fig. 115-18), in addition to sunexposed areas. They often have brown-black pigmentation and are irregular. An ephelis (freckle) is a small, uniformly pigmented macule that may be clinically distinct from a solar lentigo. Freckles are most common on the central face. Typically, they develop in early childhood, increase
20
A B
in adulthood, and may regress in the elderly or in the absence of continued sun-exposure.
RELATED PHYSICAL FINDINGS
Given that solar lentigines occur on photodamaged skin, they are associated with actinic keratosis, squamous cell carcinoma, basal cell carcinoma, and melanoma. Type 2 diabetes has been shown to be independently associated with solar lentigo.92
COMPLICATIONS
Although solar lentigines may sometimes show melanocytic atypia on sun-damaged skin, they are benign. However, in lesions where significant atypia is present, distinction between atypical solar lentigo and melanoma in situ, lentigo maligna type may be challenging.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
Solar lentigines arise from proliferation of basal melanocytes and increased melanin production. The relationship between UVR and development of lentigines is well-recognized. The cumulative effects of photodamage produce genetic and epigenetic changes in gene expression within both keratinocytes and melanocytes. Interestingly, keratinocytes are more sensitive to UVR than melanocytes.93,94
In response to UVR exposure, keratinocytes upregulate multiple ligands and produce reactive oxygen species (ROS), ultimately leading to MC1R and subsequently MITF activation in melanocytes through direct cell-to-cell communication and paracrine signaling.95
MITF is a key transcription factor for melanin production in melanocytes. Studies have reported the association of solar lentigo with loss of function MC1R alleles, MC1R promoter polymorphisms, and SLC45A2 allele variants.96-98
Hafner and coworkers observed FGFR3 and PIK3CA mutations in 17% and 7% of solar lentigos, respectively. Kadono and coworkers demonstrated increased expression of endothelin B receptor and endothelin 1 in solar lentigo, which are key factors for melanocyte development and melanogenesis.99 Additionally, fibroblast-derived growth factors, including keratinocyte growth factor, hepatocyte growth factor, and stem cell factor, may contribute to formation of solar lentigo.100,101 T1799A BRAF mutation are detected in 33% of PUVA lentigines.102
DIAGNOSIS
DIAGNOSIS
PATHOLOGY
Histologic sections of solar lentigo show elongated rete ridges, extending into the papillary dermis with clubshaped or budlike endings. The epidermis between the rete ridges may be atrophic and have minimal overlying hyperkeratosis. The rete ridges may branch and become fused, creating a reticular pattern, caused by
1971
20
A
C
epidermal proliferation. Within the lesion, melanocytes may be normal in number or slightly increased and are hyperactive with markedly increased melanin production. Both within the lesion and background adjacent skin, melanocytes may have mild nuclear atypia, likely because of actinic changes. Occasionally, small horn cysts form, resulting in histologic overlap with seborrheic keratosis. The dermis characteristically shows solar elastosis. A scant to moderate perivascular chronic inflammatory infiltrate is usually present within the dermis, along with melanin-laden macrophages. PUVA lentigines show a variety of histologic features, ranging from predominantly basal cell hyperpigmentation with normal melanocyte count to markedly elongated rete ridges with melanocyte hyperplasia. In a subset of cases, melanocytes show cellular atypia, including nuclear pleomorphism, pseudoinclusions,
1972
B
multinucleation, irregular nuclear contours and melanin macroglobules.103
In electron microscopy studies of solar lentigo, melanosome complexes were greatly enlarged within keratinocytes compared with background adjacent skin.104
PUVA lentigines had more dendrites and more active melanogenesis.103
LABORATORY TESTING
Immunohistochemistry to highlight melanocyte density is generally not required for histologic diagnosis.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-9.
■Reticulated seborrheic keratoses
■Reticulated seborrheic keratoses
■Lentigo simplex
■Lentigo simplex
■Ephelis
■Ephelis
■Junctional nevomelanocytic nevus
■Junctional nevomelanocytic nevus
■Pigmented actinic keratoses
■Pigmented actinic keratoses
■Large cell acanthoma
■Large cell acanthoma
■Lentigo maligna
■Lentigo maligna
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Over time, solar lentigines may enlarge or darken, persist as a stable lesion, or regress. They may evolve into lichenoid keratoses.105 Subsequent resolution of the lichenoid keratosis ultimately may cause complete resolution of the prior lentigo. Recent molecular studies support this pathway of solar lentigo regression. Benign lichenoid keratoses have been shown to harbor FGFR3, PIK3CA, and RAS mutations, which are known to be involved in the pathogenesis of solar lentigo.106
Some authors have suggested that solar lentigo may evolve into large cell acanthoma or that large cell acanthoma is a variant with cellular hypertrophy.107
Although the lesions share similar morphological features, differences in immunophenotype, including keratin 10 and BCL-2 expression, have been observed. Higher expression of keratin 10 and lower expression of BCL-2 suggests large cell acanthoma to have advanced maturation compared with solar lentigo.107
PUVA lentigines may persist years after treatment discontinuation.90 Long-term follow-up of a large cohort of patients treated with PUVA demonstrated increased risk of melanoma, which emerged 15 years after initial therapy and continued to increase as time progressed.108 Solar lentigines are similarly associated with increased risk of cutaneous malignancies.
MANAGEMENT
MANAGEMENT
TREATMENT
Solar lentigines are benign lesions that do not require therapy. If desired, cosmetic removal may be completed with cryotherapy or other techniques, including Q-switched laser.
PREVENTION
Avoidance of UVR exposure may decrease the risk of developing additional solar lentigines.
20
DYSPLASTIC MELANOCYTIC NEVI
AT-A-GLANCE
■ Commonly occur in Caucasians; prevalence varies by population
■ Flat or raised with smooth or “pebbly” surface, irregular shape, indistinct borders, variable pigmentation, and measure at least 5 mm in diameter
■ Identify population at risk for melanoma
■ Most frequent on sun-exposed areas, especially intermittently exposed, including the upper back
■ Associated with large numbers of common acquired nevi
■ May persist or involute; subset undergoes malignant transformation to melanoma
■ Histologic features include lentiginous melanocytic hyperplasia with architectural and cytologic atypia and stromal response.
EPIDEMIOLOGY
EPIDEMIOLOGY
Dysplastic nevi are common melanocytic lesions, predominantly occurring in Caucasians. The prevalence of dysplastic nevi varies by population. Individuals from melanoma-prone families have the highest incidence of dysplastic nevi. In a study by Rhodes and coworkers, dysplastic nevi were present in 30.4% of patients with melanoma compared with 1.8% of the control group.109
Studies involving populations of northern European descent have reported variable ranges for clinically atypical nevi from 7% to 18%, with histologic-proven dysplastic nevi estimated near 10%.6 Some support a more accurate frequency to be between 2% to 8% in this population. Dysplastic nevi are uncommon in Japanese.110 Individuals with dysplastic nevus syndrome (DNS) may develop more than 100 clinically atypical nevi by adolescence.
CLINICAL FINDINGS
CLINICAL FINDINGS
CUTANEOUS FINDINGS
Clinically, dysplastic nevi often measure at least 5 mm in diameter and characteristically have irregular, indistinct borders and variable pigmentation (Fig. 115-20). Color is typically a mixture of tan and brown, with some lesions showing pink-red coloration.
1973
20
A B C
D E F
Black pigmentation is more commonly associated with melanoma.111 Rarely, nonpigmented dysplastic nevi may develop. Additionally, dysplastic nevi frequently have a flat macular component, which corresponds to a ‘shoulder’ or junctional component of a compound lesion. Absence of a macular component and lesional symmetry are clinically suggestive of benignity. A study by Barnhill and Roush found that nevus size and irregular borders are the most significant clinical features that had the highest correlation to histologically proven dysplastic nevi.112 Notably, nevi that are clinically atypical may be recognized on microscopy as benign. Moreover, site-specific changes should be well-known to dermatopathologists. For instance, acral and flexural site nevi may display atypia both clinically and histologically but lack diagnostic criteria for frank dysplasia on histologic examination. Dysplastic nevi are often slightly raised and have a “pebbly” or smooth texture. They predominate on intermediate sun-exposed skin sites, such as the trunk and especially the upper back (Fig. 115-21). To a lesser extent, they occur on sun-protected sites, such as the chest and buttocks, and less commonly the scalp. Skin creases are usually unaffected. Patients may have solitary or numerous dysplastic nevi. Agminated lesions are rarely described. In DNS, more than 100 nevi may develop. In affected individuals, large numbers of common acquired nevi develop during childhood and subsequently acquire dysplastic features at or around puberty. Patients tend to develop melanoma at an earlier age, often in the mid-30s, and may have multiple sites of malignancy.
1974
The trunk is the most common site of malignant transformation in DNS.
RELATED PHYSICAL FINDINGS
Patients with DN may develop melanoma. A subset of melanoma cases directly progress from dysplastic nevi, and histologic evidence of an associated nevus may be apparent on microscopy. However, the majority of melanomas arise from normal skin. Several physical and environmental factors, independent of dysplastic nevi, are known to increase the risk of melanoma, including cutaneous phenotype, solar injury, and presence of ephelides (freckles). Cases of eruptive dysplastic nevi have been described in patients with AIDS, renal transplantation, chronic myeloid leukemia, and after chemotherapy for pre–B-cell acute leukemia.113-115
Individuals with dysplastic nevi have higher numbers of common acquired nevi.
COMPLICATIONS
Melanoma is the most clinically concerning complication, associated with dysplastic nevi. Its relative risk increases with the number of dysplastic nevi on an individual and the presence of personal or family history of melanoma. A large meta-analysis found that sporadic dysplastic nevi are associated with a 10-fold increased risk for melanoma.39 If family history of melanoma is present in at least two relatives, there is an associated 200-fold increased risk of melanoma.116
A B
20
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The pathogenesis of dysplastic nevi is not well understood. DNS can be sporadic or inherited as an autosomal-dominant trait with variable expressivity and incomplete penetrance.117 Recently, genetic variants in CDK6 and XRCC1 were found to be associated with dysplastic nevi in melanoma-prone families, independent of melanoma status. Mutations on 9p21-22 (CDKN2A) are present in approximately 40% of cases of DNS and are associated with melanoma; however, they are not frequently detected in dysplastic nevi.118,119 CDKN2A encodes tumor suppressor gene products p16INK4a and p14ARK. Microsatellite instability at chromosome 1p and 9p is frequently identified in dysplastic nevi and melanoma.120 Similar to common acquired nevi, dysplastic nevi have a similar rate of BRAF mutation and can show loss of PTEN expression and altered p53 expression.121,122
Studies have demonstrated that dysplastic nevi may have higher levels of reactive oxidative species and a higher proliferative rate than common nevi, but less than melanoma.123
Additionally, UVR exposure is important for the development of dysplastic nevi. Dysplastic nevi are more likely to develop on sun-exposed sites compared with doubly covered locations such as the buttocks. Sun exposure and sunburns, especially before the age of 20 years, have been shown to be associated with dysplastic nevi.124 In melanoma-prone families, sunprotective measures in childhood reduce the number of nevi that occur. Additionally, the dysplastic and
common nevi are more likely to involute in this population with adherence to sun-protective measures.118
DIAGNOSIS
DIAGNOSIS
PATHOLOGY
The histological features of dysplastic nevi characteristically show an intraepidermal lentiginous melanocytic hyperplasia with cytologic and architectural atypia and dermal stromal response (Fig. 115-22). Melanocytes are irregular in shape and distribution. In a common acquired nevus, nests of melanocytes are confined to the tips of the rete ridges. Dysplastic nevi show melanocytes distributed singly and in nests located at the tips and sides and between rete ridges. Pagetoid spread, especially atypical melanocytes at the level of the granular layer, are more commonly seen in severely dysplastic nevi and melanoma. Additional features of architectural atypia include bridging of melanocytic nests at the tips of the rete ridges, and a “shouldering” junctional component of atypical melanocytes, extending at least three rete ridges beyond a dermal nevomelanocytic component. Confluence of atypical melanocytes along the epidermis is suggestive of melanoma in situ. The epidermis usually shows elongated rete ridges and a normal epidermal thickness. Although effacement of the rete ridges and attenuation of the epidermis, may occur, regressive features are more common in melanoma. A range of cytologic atypia is present in melanocytes, including dusty cytoplasm,
1975
20
A
B
nuclear enlargement, nuclear membrane irregularity, prominent nucleoli, and nuclear pleomorphism. If present, the dermal nevomelanocytic component is usually bland. Dermal fibroplasia is commonly seen directly under the epidermal component in the papillary dermis. A superficial lymphocytic infiltrate and melanin-laden macrophages may be present in the papillary dermis. The overall degree of dysplasia should be scored by a dermatopathologist. Studies examining diagnostic accuracy and reproducibility for melanocytic lesions, including dysplastic nevi, have demonstrated variable results. Multiple studies have moderate to good interobserver agreement, but others have yielded limited to fair concordance.125-128 A recent well-designed study demonstrated poor interobserver accuracy and reproducibility.129 It should be noted that although grading systems have been proposed by multiple groups, consensus amongst dermatopathologists is lacking. Site- and gender-specific differences in DN are well described.111 Additionally, margin status should be noted, particularly in cases of moderate and severe dysplasia.
SPECIAL TESTING
Dermoscopy (dermatoscopy or epiluminescence microscopy) is recommended during the evaluation of melanocytic neoplasia. Dermoscopy increases the diagnostic accuracy of melanoma detection.130
Digital imaging may be beneficial for clinical and histologic evaluation of pigmented lesions. Total-body photography, or mole mapping, is recommended for patients with multiple pigmented lesions or DNS. Total body photography has been shown to detect melanomas at earlier stages and reduce biopsies of benign lesions.131 Other noninvasive and objective imaging techniques are being developing and include Raman spectroscopy, confocal microscopy, and multispectral imaging.
1976
Recent work has focused on the development of a clinically validated molecular test to classify challenging melanocytic lesions as benign or malignant. Several panels have shown some promise differentiating benign nevi from melanoma with respectable sensitivity and specificity. Gene expression profiling may have additional utility in predicting responses to specific treatments or understanding treatment resistance. Further validation of gene-expression signatures in diagnostically challenging melanocytic lesions is critical.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
See Table 115-10.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
The majority of dysplastic nevi do not progress to melanoma. Most studies support that only about 20% of melanoma arise from dysplastic nevi.132,133 The risk of developing melanoma is dependent on a combination of factors, including number of dysplastic
■Common acquired nevus
■Common acquired nevus
■Congenital or congenital-type nevus
■Congenital or congenital-type nevus
■Combined nevus
■Combined nevus
■Spitz nevus or /Spitz variant
■Spitz nevus or /Spitz variant
■Pigmented spindle cell nevus
■Pigmented spindle cell nevus
■Recurrent nevus
■Recurrent nevus
■Melanoma
■Melanoma
nevi, personal history of melanoma or nonmelanoma skin cancer, family history of melanoma, and UVR exposure. Given that early diagnosis of melanoma improves prognosis, periodic dermatologic follow-up is recommended and should be based on the perceived risk of malignancy and competency in self-examination. For high-risk patients, intensive surveillance is initially recommended at 4- to 6-month intervals. For patients with a family history of melanoma and multiple dysplastic nevi, annual surveillance may be appropriate. Surveillance should be initiated at 10 years of age for high-risk individuals with a family history of melanoma in at least two family members and a history of dysplastic nevi in the patient or a family member. Of patients who subsequently develop melanoma, those followed in pigmented lesion clinics usually are diagnosed and treated at earlier stages.131 If performed, the patient should receive a copy of his or her total-body photography. Sun-protective measures, self-examination, and family screening are recommended.
MANAGEMENT
MANAGEMENT
TREATMENT
Biopsy should be performed of clinically suspicious, changing, or symptomatic lesions. If melanoma is of significant concern, excision is appropriate. For patients with DNS, wholesale removal of dysplastic nevi does not significantly reduce the lifetime risk of melanoma. Lesions suspicious for melanoma should be identified as early as possible and completely excised. Reexcision may be necessary to obtain a 5-mm margin if a dysplastic nevi with severe atypia is identified on histology. Patients should be educated on the warning signs of melanoma, including changing pigmented lesions and the ABCD rule (asymmetry, border irregularity, color variation, diameter >6 mm). Sun-protective measures, such as use of sun-protective clothing, sunglasses, sunscreens, and avoidance of overexposure, should be recommended.
PREVENTION
Sun-protective measures reduce the incidence of dysplastic and common acquired nevi.
ACKNOWLEDGMENTS
We acknowledge and extend our thanks to the contributions contained herein by Dr. Philip LeBoit as well as the prior authors of the corresponding chapters in the eighth edition. The former authors are James M. Grichnik, Arthur R. Rhodes, and Arthur J. Sober (“Benign Neoplasias and Hyperplasias of Melanocytes”) and James M. Grichnik and Margaret A. Tucker (“Atypical [Dysplastic] Melanocytic Nevi”).
20

Figure 115-2 Familial aggregation of small congenital nevomelanocytic nevi. Note the small congenital nevus on the thigh of a 3-year-old Caucasian boy and on the back of his 5-year-old brother.

Figure 115-3 Congenital divided nevomelanocytic nevus of the eyelid. The nevus is contiguous when the eyelids are closed, suggesting that the lesion was formed in the developing fetus before the eyelids split (ie, before 24 weeks).
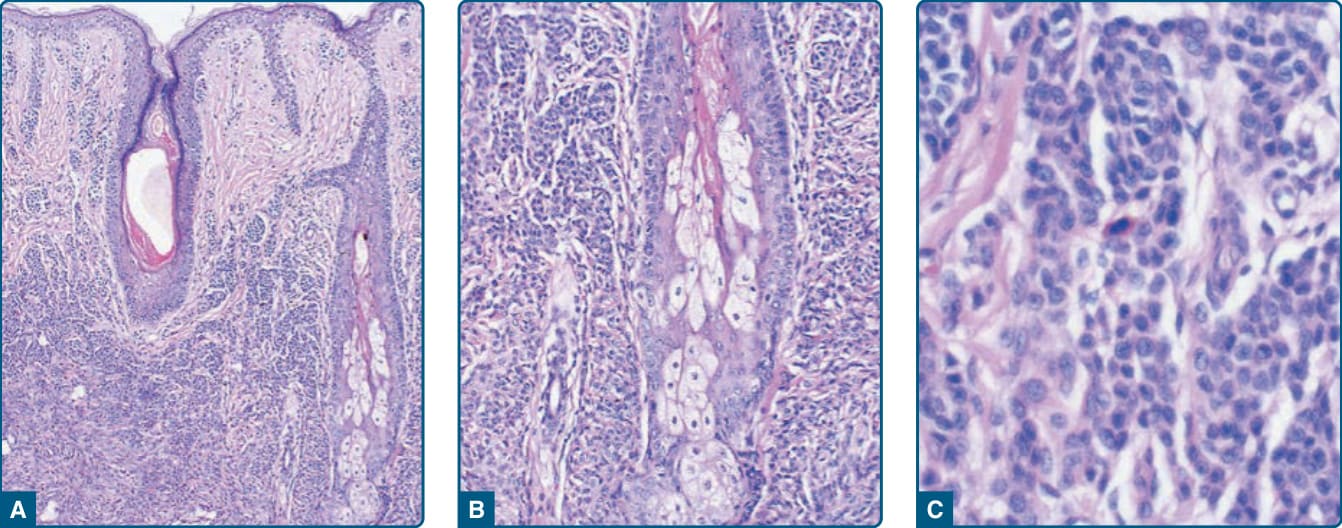
Figure 115-4 Histopathologic features of congenital nevomelanocytic nevus. Nevomelanocytes in the low-magnification image (A) reveal dense accumulation in the lower two-thirds of the dermis; at medium magnification (B), these cells encroach on dermal adnexal structures (follicular, sebaceous, and eccrine); and higher magnification (C) reveals dense collections of small nevomelanocytic cells.

Figure 115-5 Nevus spilus. A, Nevus spilus appearing first at age 3 years on the ankle and foot of a 25-year-old white woman. B, Congenital nevus spilus on the arm of a 10-year-old white boy.
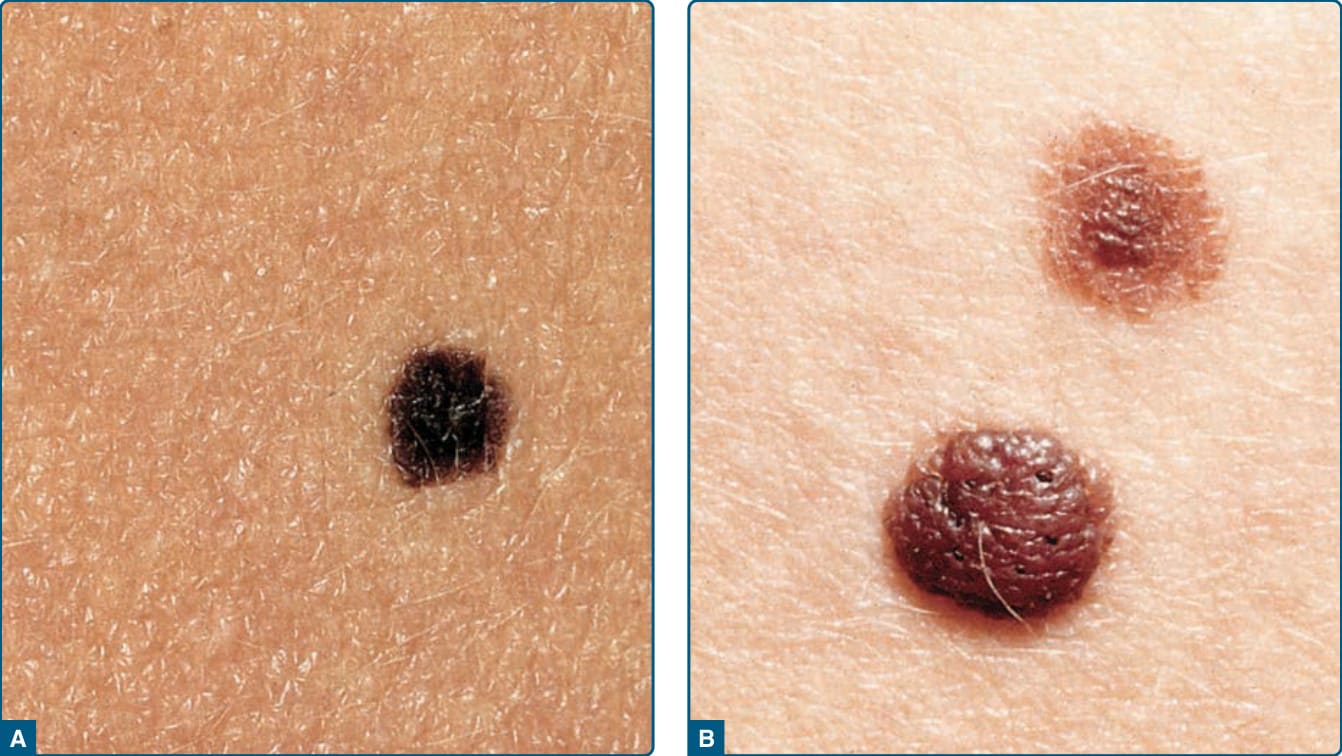
Figure 115-6 Typical acquired nevomelanocytic nevi. A, Junctional nevus. A uniformly dark brown macule, round in shape, with a smooth, regular border. B, Two compound nevi. A uniformly pigmented papule and domed nodule. The upper lesion is flatter and tan with slight central elevation. The lower lesion is older and is uniformly elevated because of an increased intradermal component.

Figure 115-7 Halo nevomelanocytic nevus. A, Acquired halo nevus on the chest of a 16-year-old Caucasian boy whose maternal grandmother had melanoma. B, Acquired halo nevi on the back of a 6-year-old Caucasian boy. Scale in millimeters. C, Halo congenital nevomelanocytic nevus on the neck of a 4-year-old girl. This child also had scattered areas of vitiligo-like depigmentation in other sites. A 3-year follow-up after excision of the nevus revealed almost total repigmentation of the widely scattered previously depigmented areas.
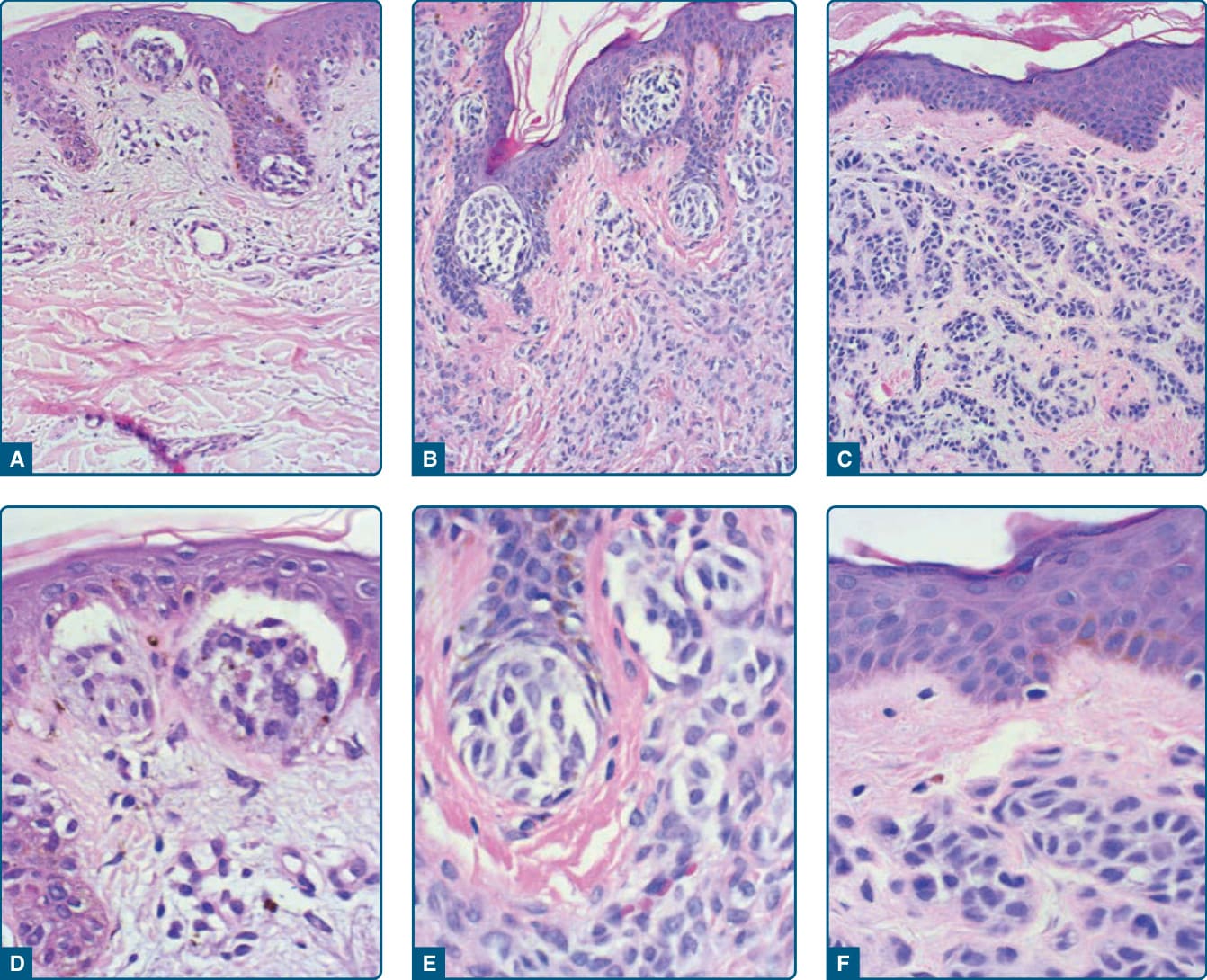
Figure 115-8 Histopathologic features of acquired nevi. Junctional nevus (A) and higher magnification (D). Compound nevus (B) and higher magnification (E). Intradermal nevus (C) and higher magnification (F). Well-formed nests of nevomelanocytes are present in the junctional and compound nevi. Sheets and cords of nevocytes are present in the dermis of the compound and intradermal nevi. A grenz zone free of nevomelanocytes is present just below the epidermis in the intradermal nevus (C and F).
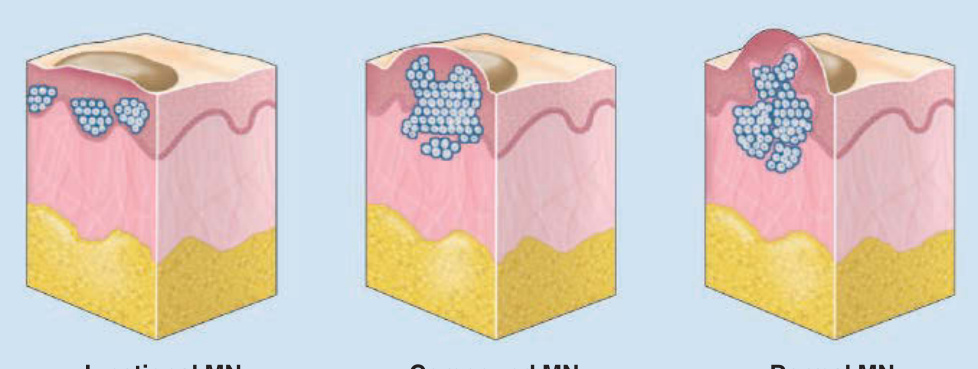
Figure 115-9 Types of nevi. MN, melanocytic nevi.
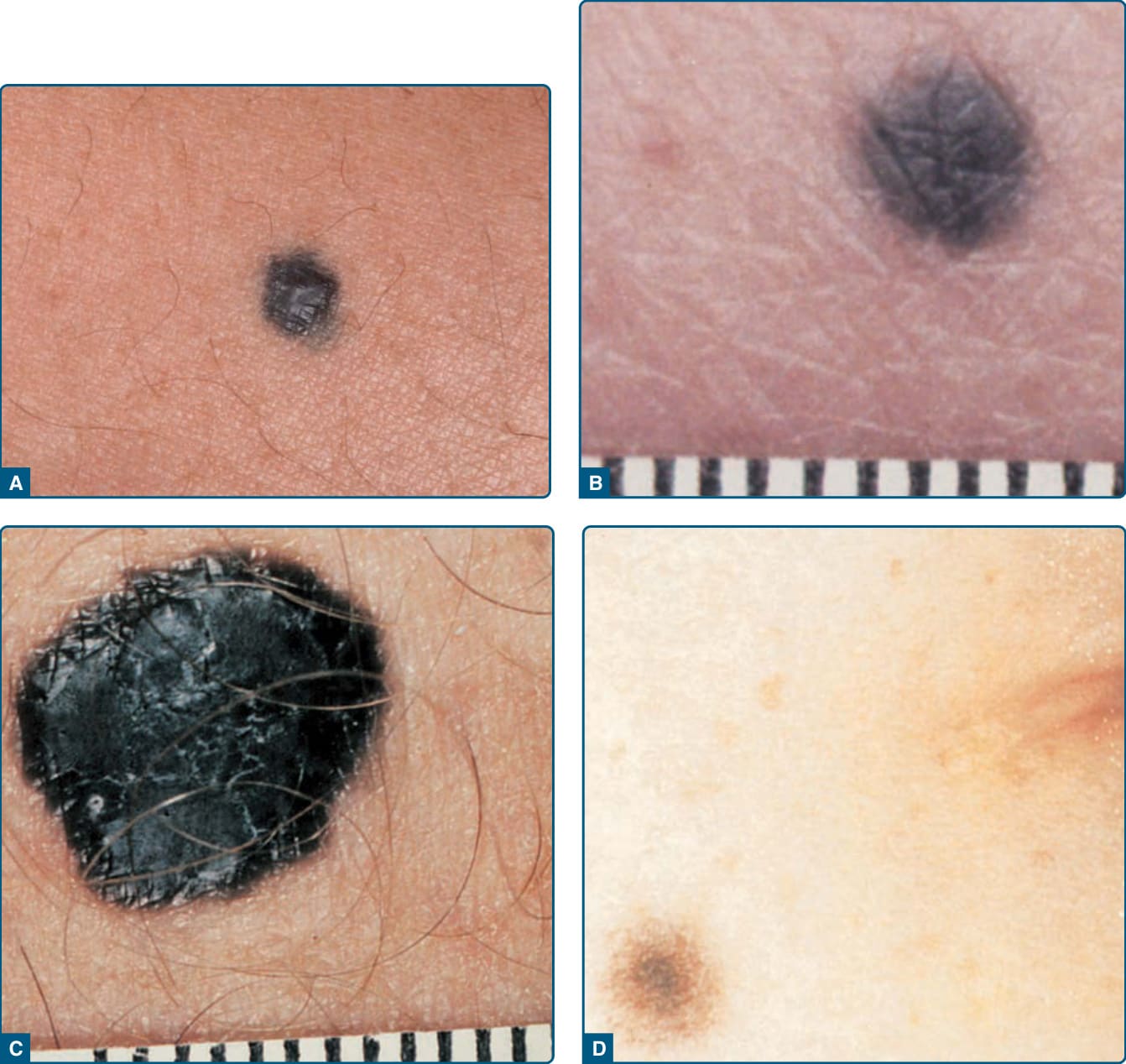
Figure 115-10 Blue nevus. A, Common blue nevus appearing as an acquired blue–gray papule on an adult male. B, Common blue nevus appearing as an acquired blue-gray papule on the buttock of a 62-year-old white man. C, Cellular blue nevus appearing as a congenital blue papule on the low back of a 30-year-old white man. D, Combined common blue nevus–nevomelanocytic nevus appearing as a brown papule with a blue-gray center on the cheek of a 12-year-old white boy, beginning as a pinpoint dot at age 1 year and enlarging slowly over time. Scale in millimeters. (Part A used with permission from Logical Images, Inc., Rochester, NY.)
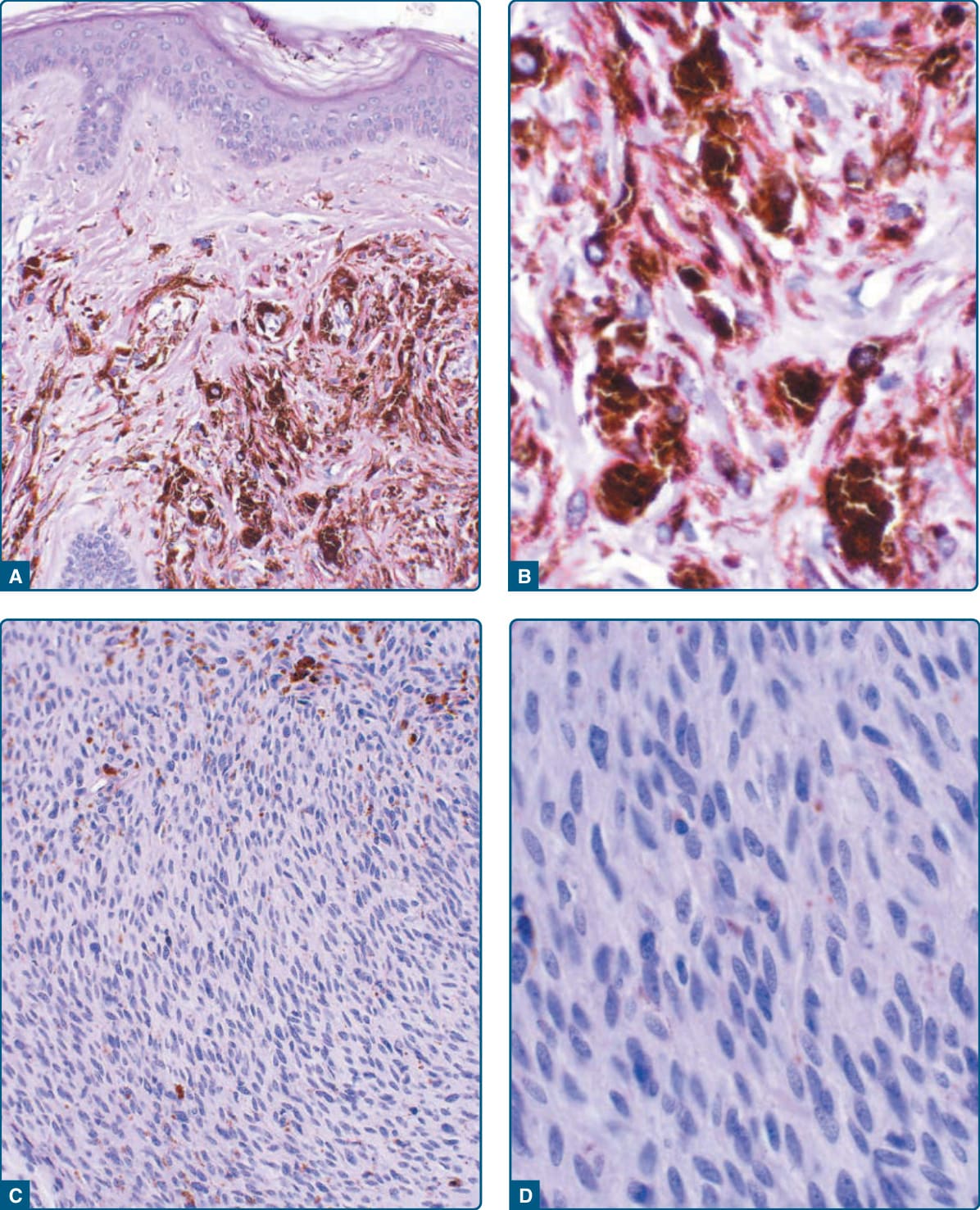
Figure 115-11 Histopathologic features of common and cellular blue nevi. Common blue nevus (A) and higher magnification of the dermal component (B) revealing heavily pigmented, elongated melanocytes. Cellular blue nevus (C) and higher magnification (D) revealing sheets of melanocytes with ovoid nuclei.
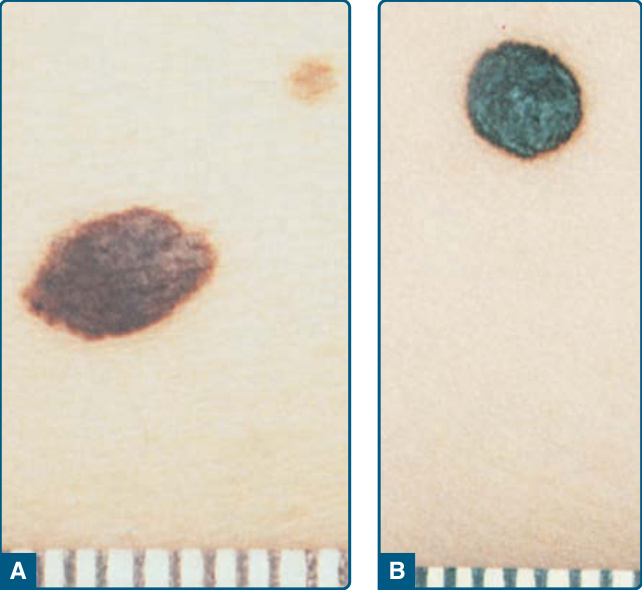
Figure 115-12 Pigmented spindle cell nevus. A, Very dark brown plaque appearing over several weeks on the posterior thigh of a 22-year-old white woman. B, Very darkbluish plaque appearing de novo 3 months previously on the back of an 8-month-old white (Hispanic) boy. Scale in millimeters.
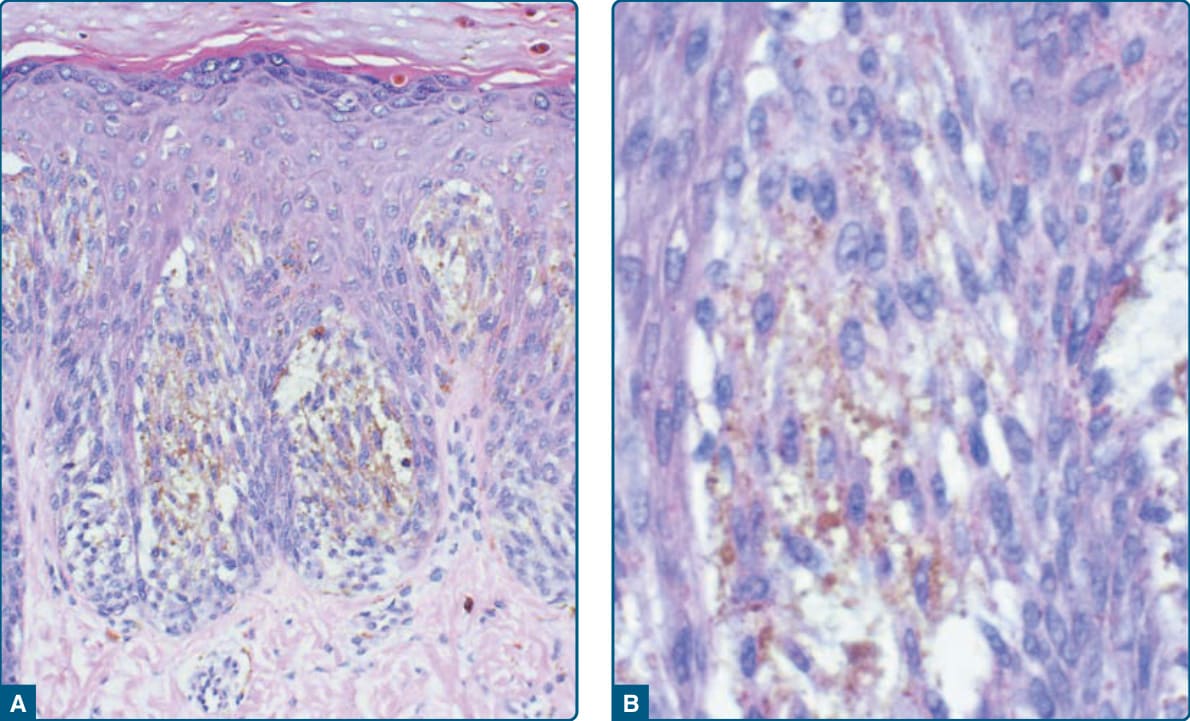
Figure 115-13 Histopathologic features of pigmented spindle cell nevus (A) and higher magnification of the intraepidermal component (B) revealing pigmented spindle-shaped cells.

Figure 115-14 Spitz nevi. A, Pink plaque, which appeared de novo over an 8-week period, becoming more elevated with time, in the preauricular area of a 4-year-old white boy. B, Dome-shaped pink papule, which appeared de novo over a 2-week interval 4 months before, on the forehead of a 5-year-old white boy. C, Agminated Spitz tumors. Numerous grouped pink papules and plaques, appearing at age 6 months, on the face of a 4-year-old white boy.
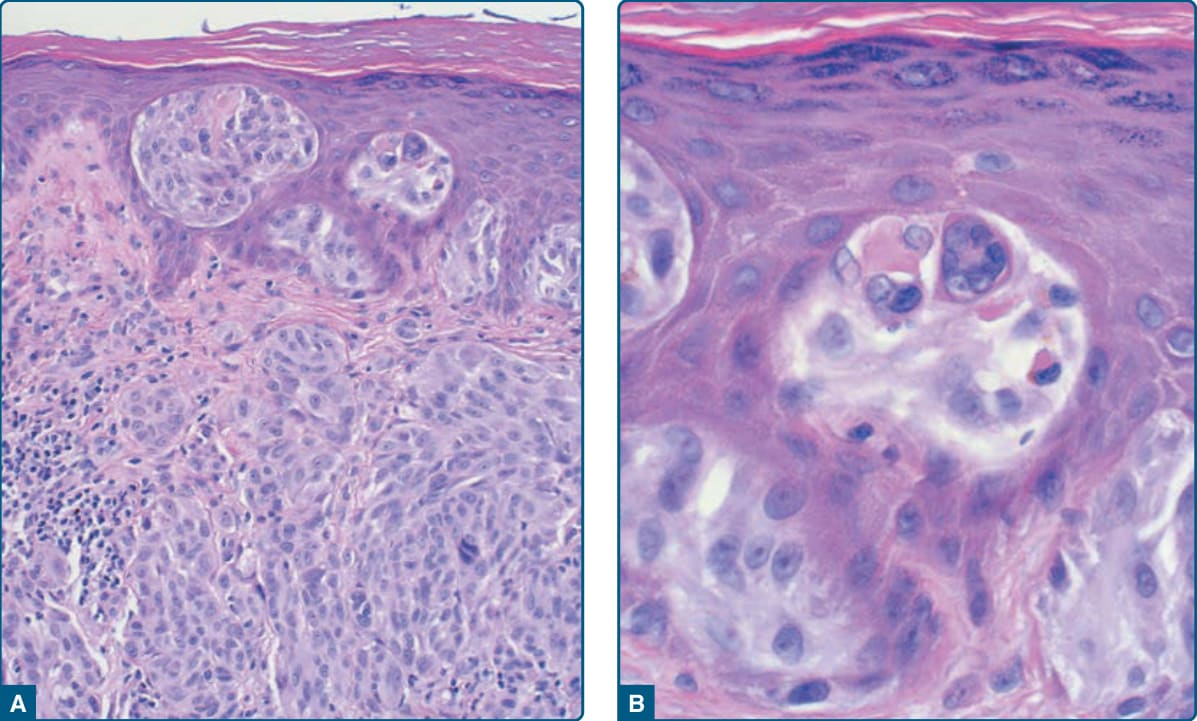
Figure 115-15 Histopathologic features of Spitz tumor (A) and higher magnification of the intraepidermal component revealing eosinophilic globules (Kamino bodies) adjacent to junctional nests (B).
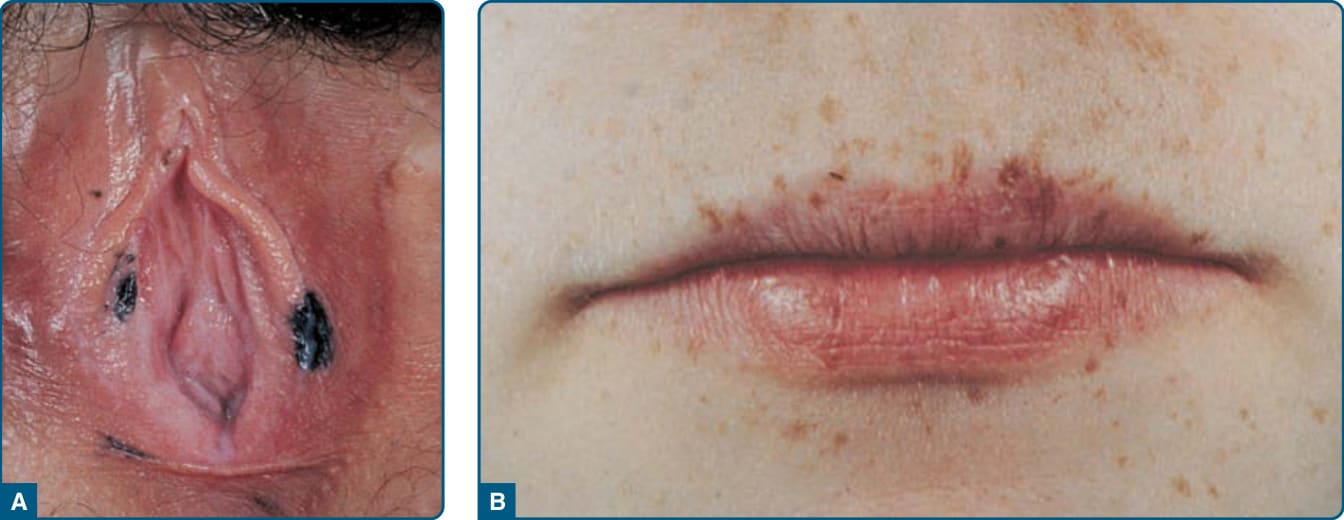
Figure 115-16 Lentigo simplex. A, Acquired darkly pigmented lentigines on the vulva of a 13-year-old white girl who has lentigines, atrial myxomas, mucocutaneous myxomas, and blue nevi (LAMB, myxoma syndrome, Carney complex). B, Multiple lentigines on the lips of the same patient. This patient died in her mid-20s of a malignant schwannoma.
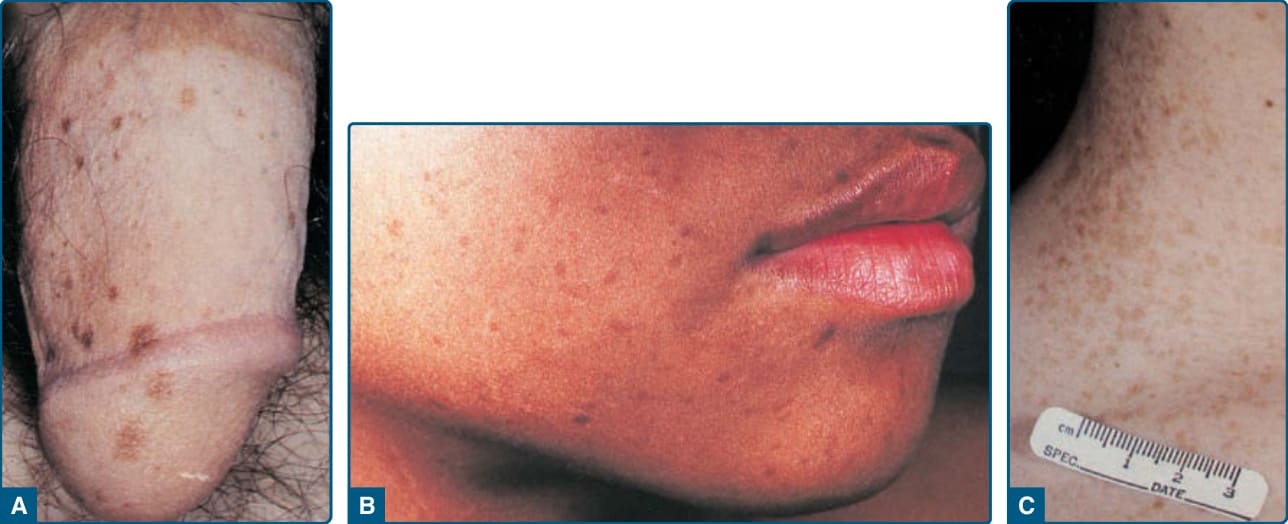
Figure 115-17 Agminated lentigines. A, Grouping of small light brown macules, present since age 14 years, on the right side of the shaft and glans penis of a 17-year-old healthy white male patient. B, Grouping of small, light brown macules, present for at least 6 years, on the right cheek of a healthy 10-year-old African American male patient. C, Grouping of small, light-brown macules, present since age 2 years, on the right neck and supraclavicular area of a 13-year-old healthy white female patient.
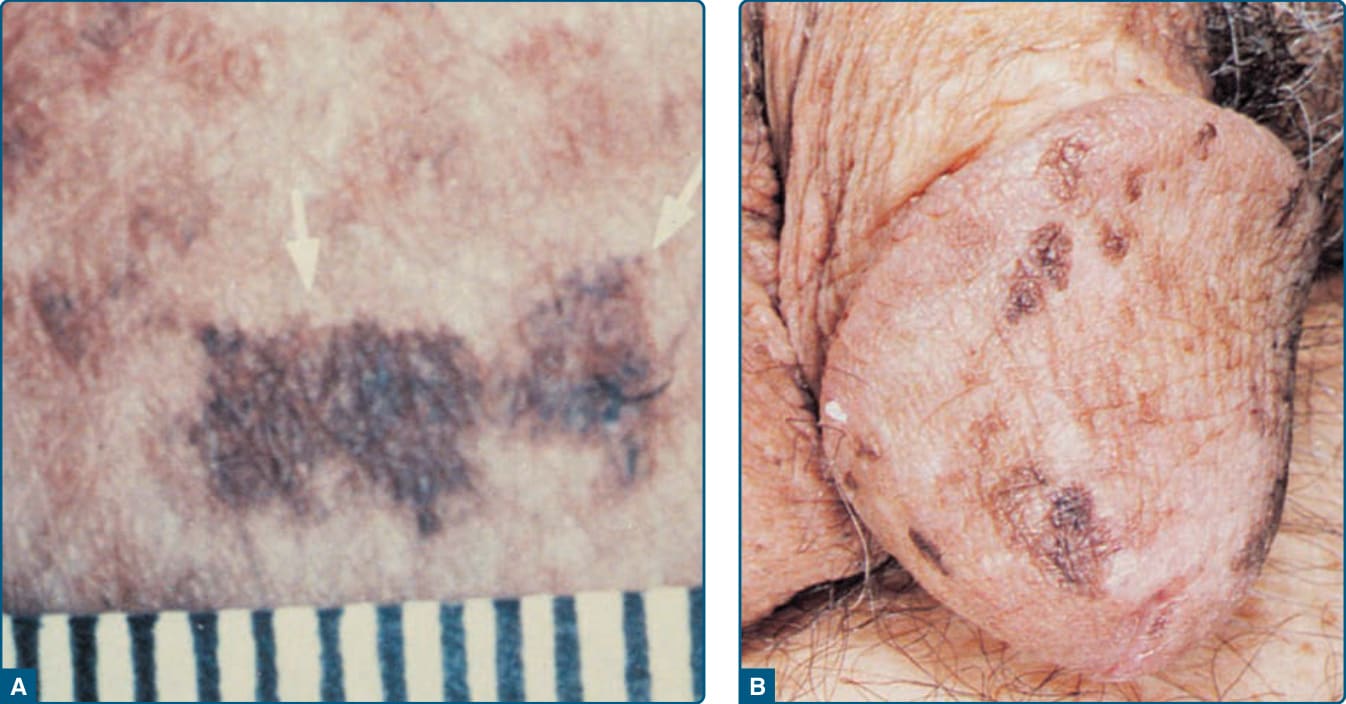
Figure 115-18 Photochemotherapy (psoralen and ultraviolet A light [PUVA])-induced lentigines (arrow) on the buttock (A) and penis (B) of a 57-year-old white man who had received PUVA for psoriasis several times per week for 5 years. The PUVA lentigines appeared between 1 and 2 years after PUVA therapy was begun. The current recommendation is to shield the male genitalia during PUVA therapy to prevent squamous cell carcinoma of the penis and scrotum.
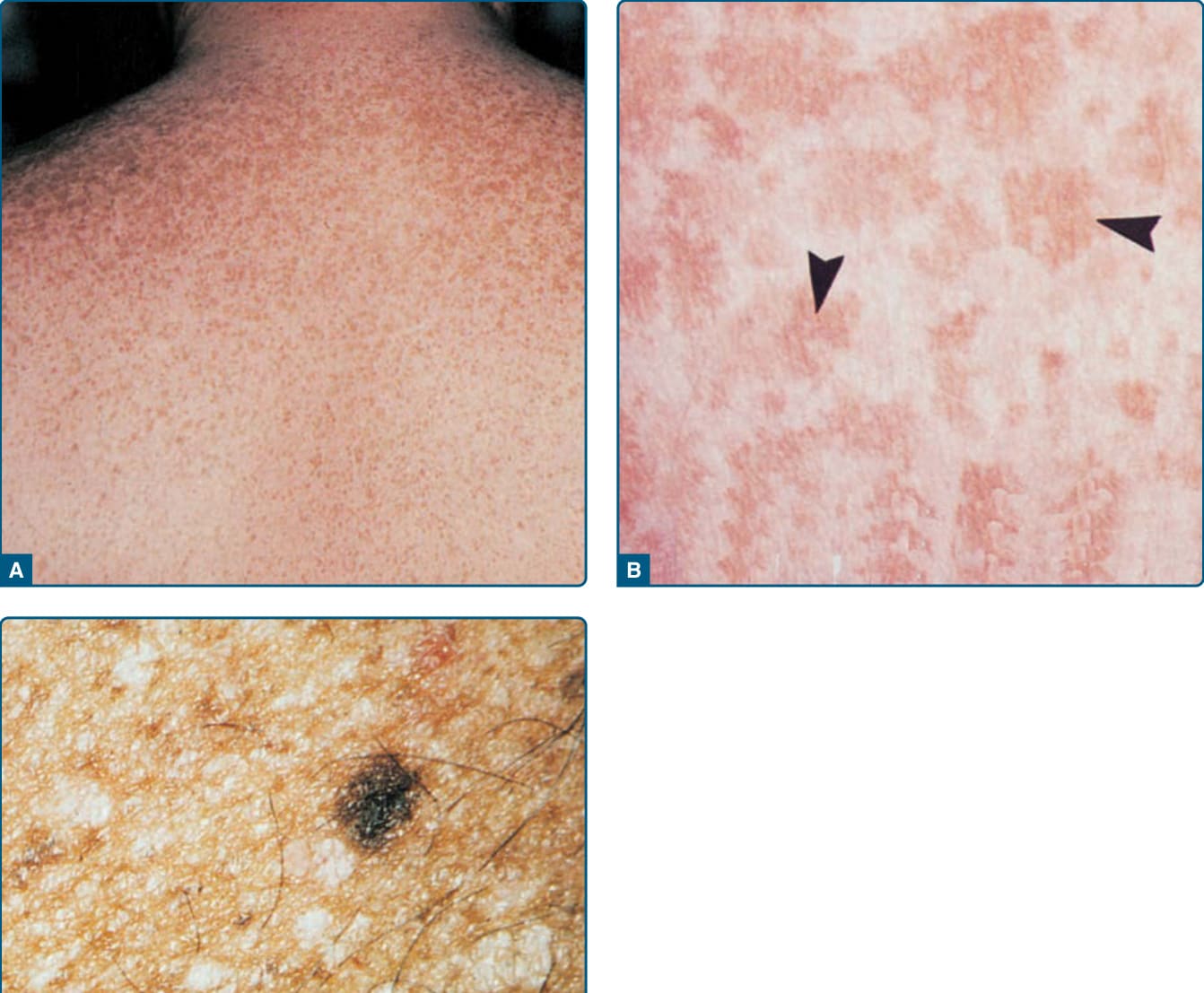
Figure 115-19 Solar lentigo. A, Uncountable solar lentigines on the back of a 30-year-old white man, appearing initially during early childhood after multiple sunburns. B, High magnification of lentigines in (A) showing lightbrown macules with markedly irregular outlines (arrowheads). C, Solar lentigines on sun-damaged dorsal hand skin (hypopigmentation, wrinkling, and telangiectasia) of an older white man.
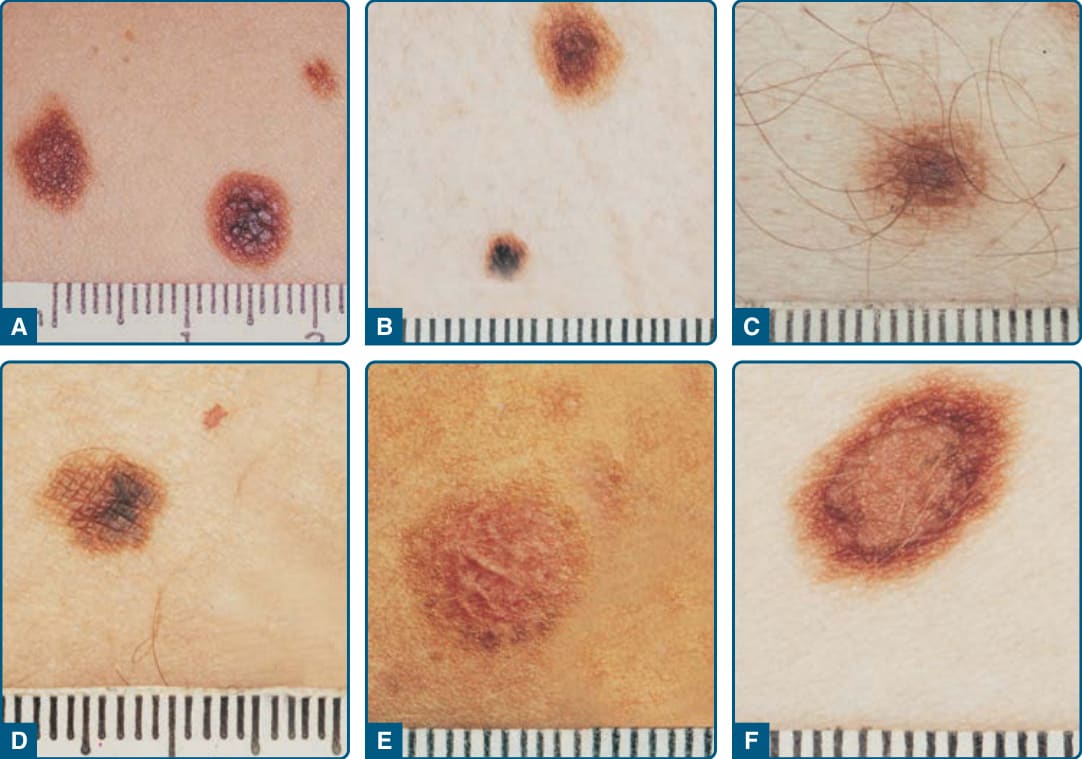
Figure 115-20 A–F, Atypical nevi typically have a diameter (diameter in one dimension at least 5 mm and a prominent flat component) and two of three other features (irregular asymmetric outline, indistinct borders, and variable pigmentation).
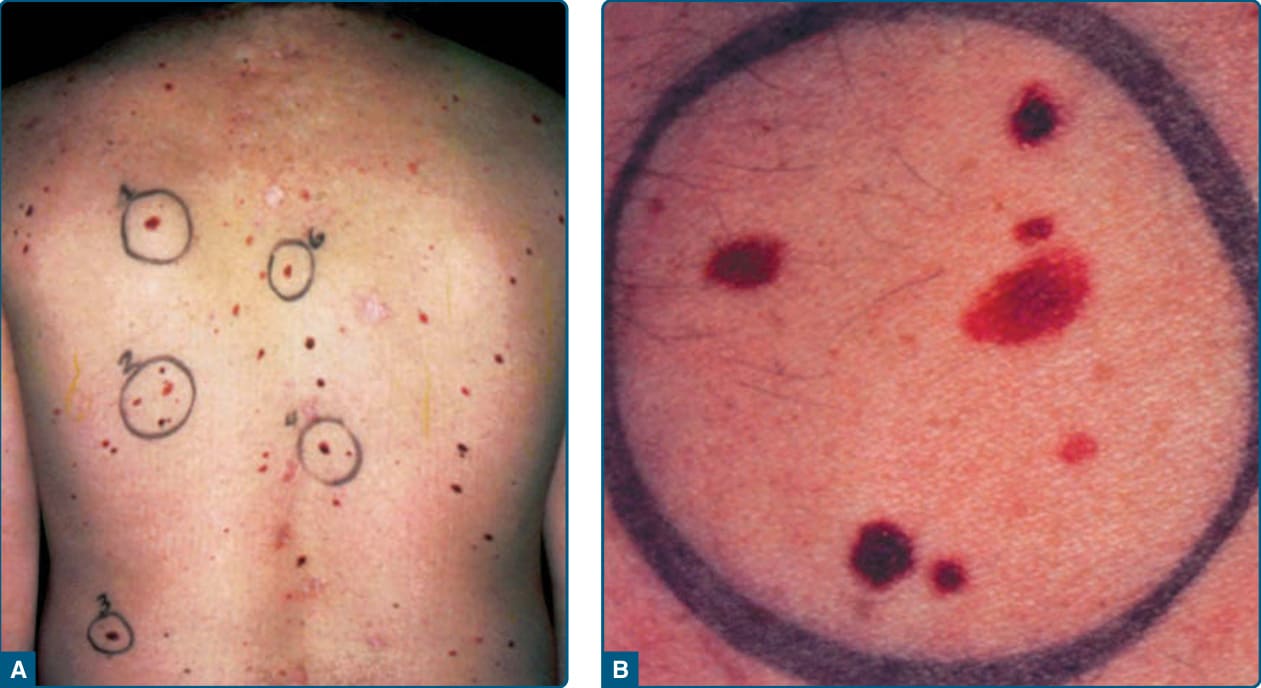
Figure 115-21 A, A back view showing the distribution of dysplastic nevus (DN) and lesion-to-lesion variability, with an increased number of common acquired nevi also. B, A closer view of a cluster of lesions marked as #2 on the back. The lesions are of different sizes, colors, and shapes with differing amounts of asymmetry and indistinct borders. The largest lesion meets all of the criteria for a clinical DN.
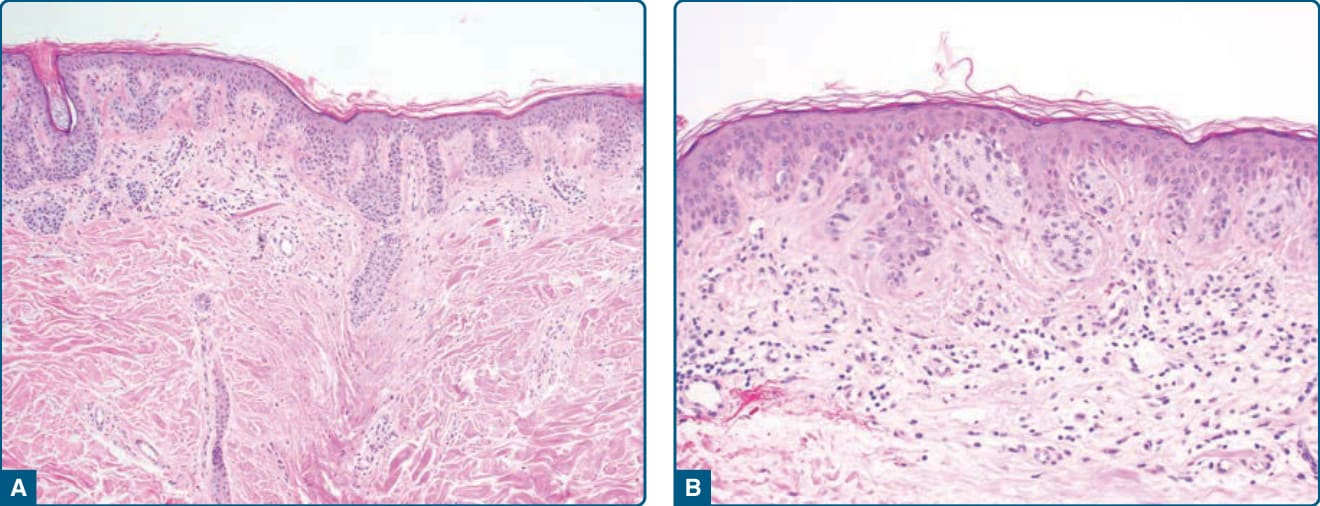
Figure 115-22 Dysplastic nevus. A, Compound dysplastic nevus with architecturally disordered junctional nests extending well beyond the dermal component (100× magnification). B, Junctional melanocytic nests are situated along the tips and sides of rete and display random cytologic atypia. There is underlying papillary dermal fibroplasia, lymphocytic infiltrate, and pigment incontinence (200× magnification).
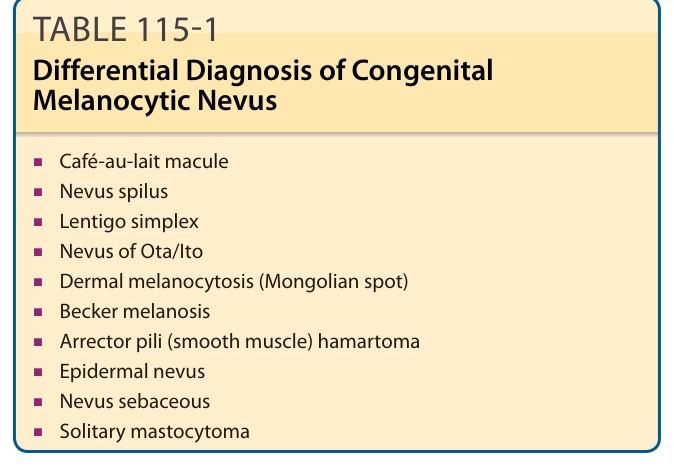
TABLE 115-1 Differential Diagnosis of Congenital Melanocytic Nevus
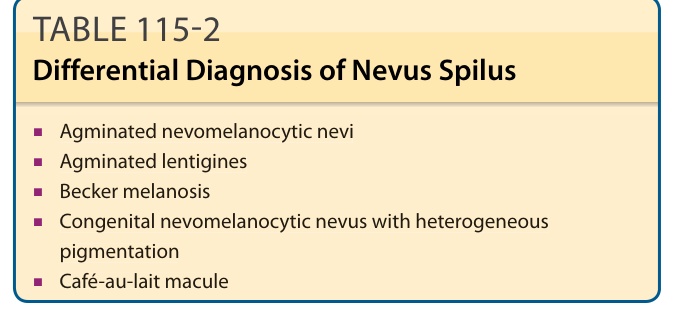
TABLE 115-2 Differential Diagnosis of Nevus Spilus
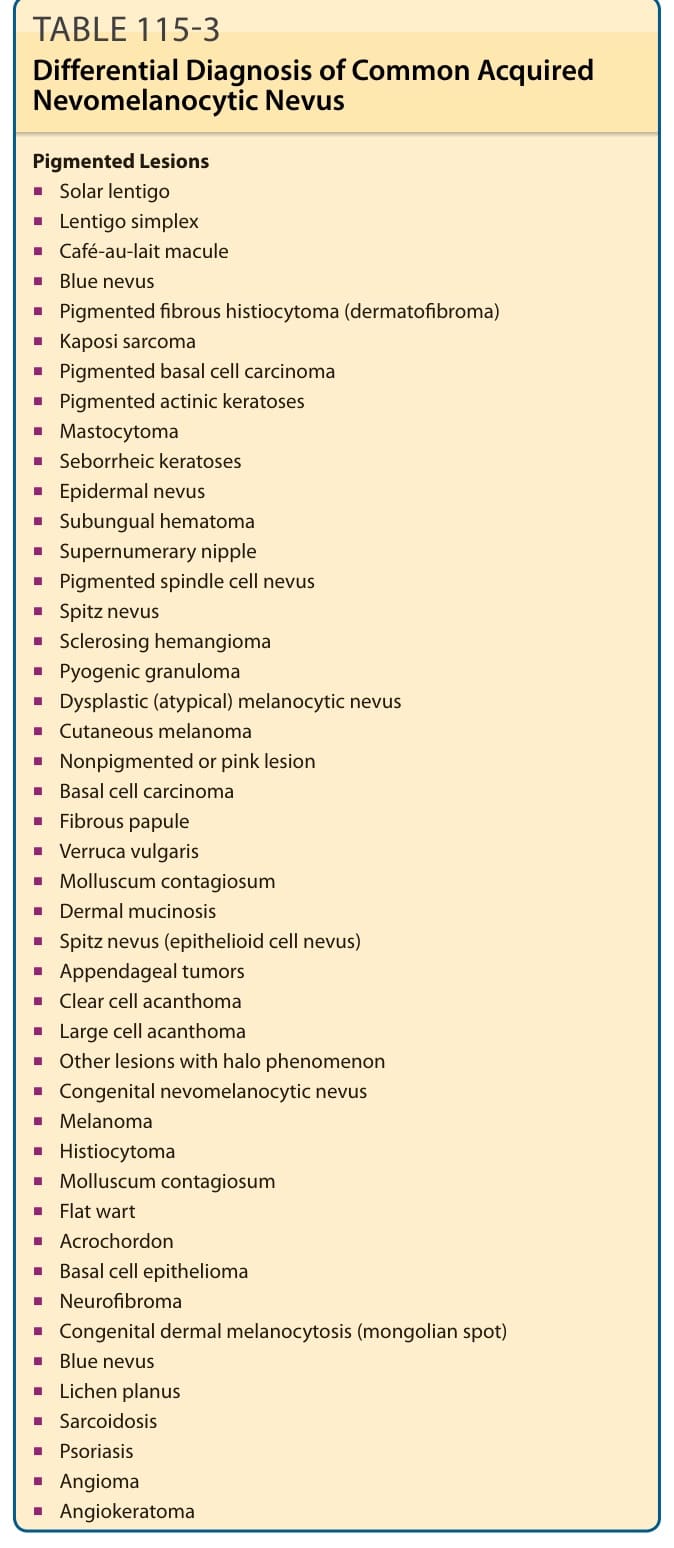
TABLE 115-3 Differential Diagnosis of Common Acquired Nevomelanocytic Nevus
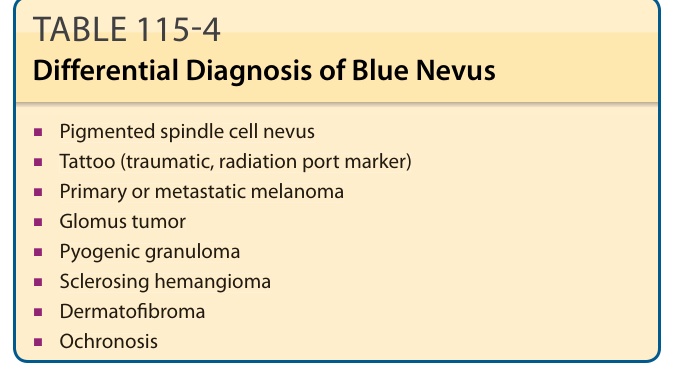
TABLE 115-4 Differential Diagnosis of Blue Nevus
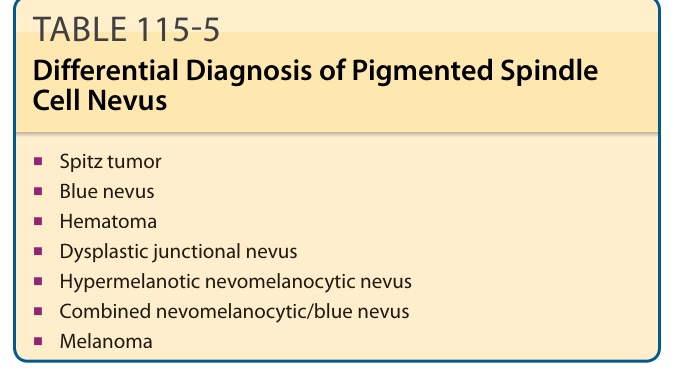
TABLE 115-5 Differential Diagnosis of Pigmented Spindle Cell Nevus
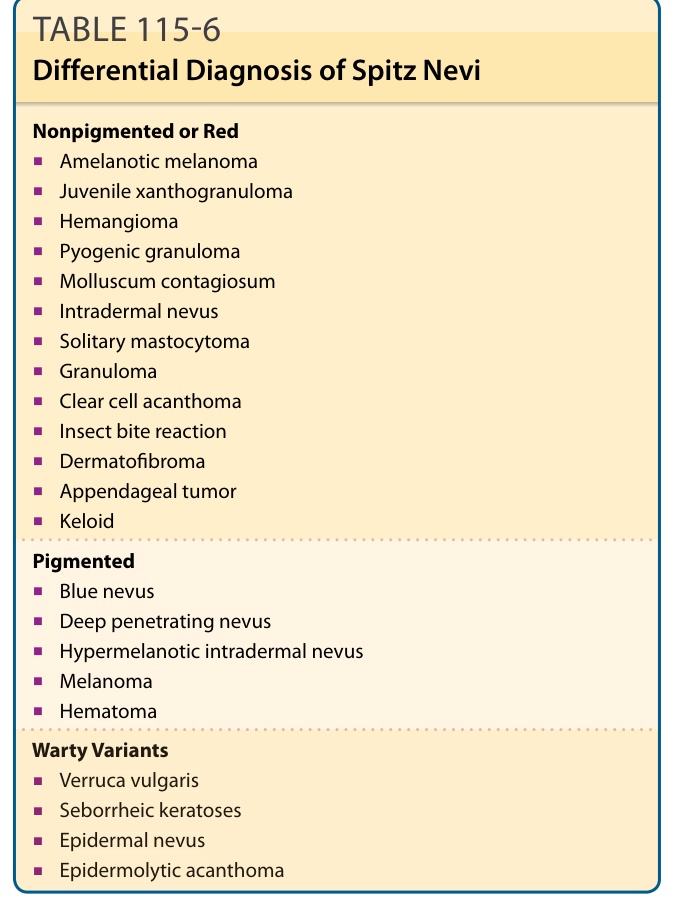
TABLE 115-6 Differential Diagnosis of Spitz Nevi
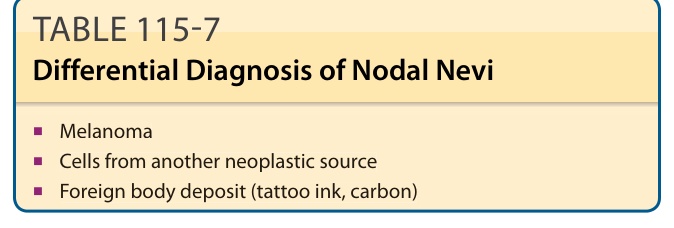
TABLE 115-7 Differential Diagnosis of Nodal Nevi
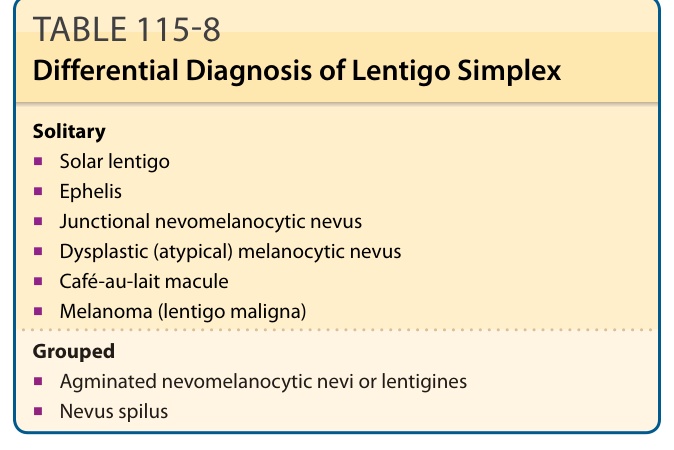
TABLE 115-8 Differential Diagnosis of Lentigo Simplex
TABLE 115-9 Differential Diagnosis of Solar Lentigo
TABLE 115-10 Differential Diagnosis of Dysplastic Nevi