Paget’s Disease
20
AT-A-GLANCE
■ Uncommon intraepithelial adenocarcinoma occurring in apocrine gland-bearing skin in patients older than age 50 years.
■ Erythematous, scaly plaque frequently misdiagnosed as inflammatory or infectious dermatitis.
■ Most commonly affected sites: unilateral nipple/ areola (mammary Paget’s disease [MPD]); vulva, perianal skin, scrotum, and penis (extramammary Paget’s disease [EMPD]).
■ Nearly all cases of MPD are associated with underlying breast carcinoma; EMPD is associated with underlying cancer in a minority (20% to 30%) of cases.
DEFINITIONS
Mammary Paget’s disease (MPD; also called Paget’s disease of the breast) is an intraepidermal adenocarcinoma of the nipple and/or areola, typically associated with underlying breast carcinoma. Extramammary Paget’s disease (EMPD) is a clinically distinct condition that affects extramammary sites, such as the vulva, penis, scrotum, perineum, and anus. Even though both MPD and EMPD may appear similar clinically and histologically, they differ in their pathogenesis and frequency of associations with underlying malignancies.
HISTORICAL PERSPECTIVE
In 1874, Sir James Paget first reported MPD in a series of 15 women with chronic dermatitis of the nipple and areola who were subsequently diagnosed with underlying breast carcinoma.1 In 1889, English dermatologist Henry Racliffe Crocker first described EMPD as a condition on the scrotum and penis with histopathology similar to MPD.2
EPIDEMIOLOGY
MPD represents approximately 1% to 3% of breast cancers.3 The peak incidence is between 50 and 60 years of age, with most reported cases occurring in women. In various studies, between 82% and 100% of MPD cases are associated with an underlying in situ or invasive ductal carcinoma.3
EMPD is a rare malignancy of the anogenital region, with various studies citing incidence rates
ranging from 0.6 per 1,000,000 person-years to 0.11 per 100,000 person-years.4,5 The majority of cases occur in the sixth through eighth decades of life, with women more commonly affected than men.6-8
In contrast to MPD, most cases of EMPD are not associated with an underlying adnexal carcinoma or visceral malignancy, with most studies reporting approximately a 20% to 30% risk.7
CLINICAL FEATURES
HISTORY
HISTORY
Both MPD and EMPD present with a longstanding history of erythematous, scaly, or velvety patches or plaques on the breast and anogenital skin, respectively. The most commonly reported symptom is pruritus. Other symptoms may include pain, bleeding, a burning sensation, and serosanguinous discharge. Because of the rather nondescript appearance, there is often a several-month delay in diagnosis as initial treatment frequently involves topical steroids (for presumed inflammatory dermatitis) or antifungal agents (for presumed infectious dermatitis).
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
MPD frequently presents as a unilateral, erythematous, scaly plaque involving the nipple and/or the areola (Fig. 114-1). The associated pruritus may lead to lichenification and excoriations. Ulceration, weeping, and crusting are often present. Nipple erosion and discharge may occur. Retraction of the nipple and areola may be seen in advanced disease. Lesions of EMPD are clinically similar to MPD and often present as well-defined, moist, erythematous, scaly plaques, usually involving apocrine glandbearing skin (eg, in the genitoperineal region and axilla). Hypopigmentation and hyperpigmentation may occur. Lichenification and excoriations of the involved area are commonly found because of pruritus. The vulva is the most commonly affected area, representing 65% of EMPD cases but less than 2% of all vulvar neoplasms.3,9 EMPD in other sites, such as the perineum, scrotum (Fig. 114-2), perianal skin (Fig. 114-3), and penis, is less common. In rare cases, ectopic EMPD has been reported in areas that are relatively free of apocrine glands, such as the chest, abdomen, thigh, eyelids, face, and external auditory canal.10-14
20
NONCUTANEOUS FINDINGS
NONCUTANEOUS FINDINGS
Patients may present with symptoms and physical findings of an underlying carcinoma or metastatic disease. Complete physical examination including thorough full-body skin examination is required in all cases of MPD and EMPD, as approximately one-half of patients presenting with MPD are found concurrently to have a palpable underlying breast mass.15,16 Of these patients, one-half to two-thirds have axillary lymph node metastases.16
Given the less-established association with underlying carcinoma in EMPD as compared to MPD, a palpable mass or lymph node is much less frequently found on physical examination in EMPD. EMPD of the external male and female genitalia may be associated with tumors of the bladder and urethra and of the prostate in men.17 Perianal EMPD may be associated with colorectal cancer.17
Failure to identify and adequately treat MPD and EMPD can lead to progression and metastasis, with a poor prognosis.
ETIOLOGY AND PATHOGENESIS
MAMMARY PAGET’S DISEASE
MAMMARY PAGET’S
DISEASE
Historically, 2 contrasting theories, known as the epidermotropic and transformation theories, attempted to explain the pathogenesis of MPD. In the epidermotropic theory, malignant Paget cells arise from an underlying breast adenocarcinoma and directly extend into the epidermis via the lactiferous ducts and ductules (epidermotropism).9 These malignant cells then invade the epidermis of the nipple and areola, leading to the clinical manifestations detailed above. In multiple reports, immunohistochemical studies showed significant similarities between the Paget cells and the underlying breast carcinoma in a majority of cases, further suggesting that MPD arose from intraepidermal extension of the ductal carcinoma.9,18,19
In contrast, epidermal keratinocytes expressed a different immunohistochemical staining pattern. In one study, overexpression of the heregulin receptor HER2/neu (also known as cluster of differentiation 340 [CD340], c-erbB-2, and human epidermal growth factor receptor 2) was identified in 80% of MPD cases. In all these cases, there was complete concordance between HER2/neu overexpression in both the Paget cells and the underlying ductal carcinoma.20 Normal epidermis does not show overexpression of HER2/ neu. Another study suggested that movement of Paget
1935
20
MOST COMMON CONSIDER ALWAYS RULE OUT
Mammary Paget’s disease
Nipple dermatitis Hailey-Hailey disease Bowen disease
Erosive adenomatosis Pemphigus Melanoma
Contact dermatitis Lichen simplex chronicus
Dermatophyte infection
Extramammary Paget’s disease
Candidiasis Lichen sclerosus et atrophicus Bowen disease
Tinea cruris Pemphigus Erythroplasia of Queyrat
Inverse psoriasis Lichen simplex chronicus Melanoma
Contact dermatitis Lichen planus
Intertrigo Symmetrical drug-related intertriginous and
Intertrigo Symmetrical drug-related intertriginous and flexural exanthema
cells is induced by the action of the heregulin-alpha motility factor, which is produced by normal epidermal keratinocytes, on HER2/neu receptors on the Paget cells, leading to chemotaxis to the overlying nipple epidermis.21 These studies suggest that a common mutation or progenitor cell leads to the development of both MPD and the underlying breast carcinoma. The transformation theory suggests that epidermal keratinocytes on the nipple transform or degenerate into malignant Paget cells that are distinct from any underlying breast carcinoma.15,22 Therefore, MPD originates as an in situ carcinoma that may subsequently progress. The epidermotropic theory is supported by the presence of an underlying breast carcinoma in nearly all cases of MPD, but the transformation theory is supported by the small fraction of cases without an underlying ductal carcinoma.15 Although both theories are possible, the literature currently favors the epidermotropic theory for the very reason that almost all cases of MPD are associated with underlying breast carcinoma.
EXTRAMAMMARY PAGET’S DISEASE
EXTRAMAMMARY PAGET’S
DISEASE
Unlike MPD, which, in most cases, has a documented underlying carcinoma, EMPD more commonly occurs in the absence of underlying malignancy and accounts for the majority of EMPD cases. Known as primary EMPD, this form of EMPD represents malignant cells that are believed to originate from the intraepidermal parts of apocrine glands or from pluripotent cells in the epidermis.7 Primary EMPD is thought to start as an in situ carcinoma that can progress by invading the dermis and subsequently metastasizing via lymphatic spread.7 In contrast, secondary EMPD arises from an underlying adnexal carcinoma or internal malignancy in approximately 20% to 30% of cases. These cases are caused by epidermotropic spread of malignant cells from the underlying tumor.7 Common visceral malignancies associated with EMPD are
1936
flexural exanthema
carcinomas of the colon, rectum, bladder, urethra, cervix, and prostate.9
DIAGNOSIS
Diagnosis of MPD and EMPD requires a high index of suspicion, with full-thickness punch, wedge, or excisional biopsy of the skin for histopathologic confirmation. A complete review of systems and fullbody skin examination, including palpation of lymph nodes, should be performed in all patients. A complete workup for both MPD and EMPD should also include a thorough search for underlying malignancy.
MAMMARY PAGET’S DISEASE
MAMMARY PAGET’S DISEASE
Punch, wedge, or excisional biopsy of lesional skin is necessary to confirm the diagnosis by histopathology. A few studies in the past suggested a role for nipple scrapings for cytologic evaluation, but this method has not gained widespread acceptance because of the potential for false-positives and false-negatives results that occur from processing artifact.23,24
Bilateral mammography is required in all cases, with biopsy of any detectable breast mass. Various studies have shown approximately 35% to 65% of patients with biopsy-proven MPD show findings on mammography that are concerning for underlying breast carcinoma.25,26 However, because nearly all patients with MPD have underlying breast carcinoma, a negative mammogram does rule out this possibility. Although the likelihood of an invasive breast carcinoma is low (∼5%) in patients without a clinically palpable breast mass and with a negative mammogram, ductal carcinoma in situ may be present and not detected by mammography.27 In one particular study, 68% of patients without a palpable breast mass and with negative mammography were found to have ductal carcinoma in situ.27
Because of the limitations of mammography, a few newer studies have suggested use of MRI in patients
with biopsy-proven MPD and negative mammogram to help identify occult breast malignancy.25,28 However, despite the increased sensitivity of MRI compared to mammography, this imaging modality has limitations because there remains a small possibility of an underlying cancer that was not visualized with MRI (potential for a false negative). In addition, because MRI is very sensitive but not very specific, it may detect findings that lead to unnecessary diagnostic testing, so patients should be counseled to the possibility of a false-positive result.
EXTRAMAMMARY PAGET’S DISEASE
EXTRAMAMMARY PAGET’S
DISEASE
As in MPD, histopathologic confirmation from a punch or excisional biopsy of lesional skin is necessary. As a consequence of the low incidence of EMPD, there is currently no standardized diagnostic algorithm once EMPD is diagnosed, but workup (Table 114-2) is directed to the possibility of an underlying GI or genitourinary neoplasm. Colonoscopy, cystoscopy, and, in female patients, pelvic examination with Papanicolaou test and colposcopy should all be considered as firstline studies to evaluate underlying malignancy. Further imaging studies should be guided by the results of the initial studies, sex of the patient, and anatomic areas of involvement. Other imaging studies to consider, as clinically indicated, include pelvic ultrasound, positron emission tomography, chest radiography, MRI, mammography, and intravenous pyelogram. The clinical utility of other laboratory tests and imaging remain unclear. In 2 reports, patients with significantly elevated serum carcinoembryonic antigen (CEA) levels had a greater risk of death from EMPD compared to patients with normal serum CEA, and the level of CEA paralleled disease course.8,29 Other studies suggest that positron emission tomography (PET)-CT scans may be useful for cases of invasive
■Sigmoidoscopy
■Sigmoidoscopy
■Cystoscopy
■Cystoscopy
■Papanicolaou test
■Papanicolaou test
■Colposcopy
■Colposcopy
■Pelvic ultrasound
■Pelvic ultrasound
■Positron emission tomography
■Positron emission tomography
■Chest radiography
■Chest radiography
■MRI
■MRI
■Mammogram
■Mammogram
■Intravenous pyelogram
■Intravenous pyelogram
■Serum carcinoembryonic antigen
■Serum carcinoembryonic antigen
■Positron emission tomography–CT scans
■Positron emission tomography–CT scans
aThese should be guided by the results of the initial studies, sex of the patient, and anatomic areas involved.
20
EMPD to evaluate for lymph node involvement and metastases.29-31 However, even PET-CT scans may not detect microscopic metastases. The role of sentinel lymph node biopsy (SLNB) for patients with EMPD is discussed in section “Management Extramammary Paget’s Disease”.
PATHOLOGY
PATHOLOGY
The intraepidermal adenocarcinoma of EMPD and MPD has a similar histologic appearance. There are groups, clusters, or single cells within the epidermis that show nuclear enlargement with atypia, prominent nucleoli, and well-defined ample cytoplasm (Fig. 114-4).32 Intercellular bridges are absent. The cells may be in all levels of the epidermis, and compress, but preserve, the basal layer without junctional nest formation. The cells may extend into the contiguous epithelium of hair follicles and sweat gland ducts. Acanthosis, hyperkeratosis, and parakeratosis are often present. These cells have a “pagetoid” appearance and simulate other intraepidermal malignancies, such as melanoma, pagetoid squamous cell carcinoma, mycosis fungoides, cutaneous adnexal carcinomas (eg, sebaceous carcinoma, porocarcinoma, and others), Merkel cell carcinoma, Langerhans cell histiocytosis, and other epidermotropic cutaneous metastases. The cells of MPD and EMPD can be pigmented, which does not necessarily indicate that they are melanocytic. Paget cells have intracellular mucopolysaccharides, with EMPD having a greater amount of mucin compared to MPD. As a result, cells stain positive for periodic acid-Schiff, mucicarmine, Alcian blue, and colloidal iron, and are diastase resistant. There may be focal “skip areas” that are devoid of mucin, resulting in sections of negative staining. Immunohistochemistry is invaluable in confirming the diagnosis (Table 114-3). Low-molecular-weight cytokeratin stains cytokeratin 7 (CK7) and anticytokeratin (CAM 5.2) are sensitive markers for both MPD and EMPD (Fig. 114-5), as they stain Paget cells but do
1937
20
S100 CK7 CAM 5.2 CEA CK20 EMA GCDFP-15 MUC1 MUC2 HER2/NEU
MPD − + + + − +
1° EMPD − + + + − + + + − +/−
2° EMPD − +
−
+a
2° EMPD − + + − +a
aPositivity in underlying colorectal adenocarcinoma. 1°, primary; 2°, secondary; CAM 5.2, anticytokeratin; CEA, carcinoembryonic antigen; CK, cytokeratin; EMA, epithelial membrane antigen; EMPD, extramammary Paget’s disease; GCDFP-15, gross cystic disease fluid protein-15; HER2, human epidermal growth factor receptor 2 (also known as cluster of differentiation 340 [CD340], c-erbB-2, and neu); MPD, mammary Paget’s disease; MUC, mucin core protein.
not typically react with epidermal or mucosal keratinocytes, helping to distinguish MPD and EMPD from pagetoid squamous cell carcinoma.33 These cytokeratin stains are not completely specific, however; for example, both Toker and Merkel cells also exhibit CK7 positivity. The cells of MPD and EMPD also commonly stain with CEA and epithelial membrane antigen, but these stains also are not specific for these entities.33 HER2/ neu has been used in select studies and is more often positive in MPD than in EMPD.34 S100, Melan-A (also known as MART-1), and HMB-45 are useful markers to exclude melanoma and are typically negative in MPD and EMPD. Cytokeratin 20 (CK20) positivity has been found more frequently in cases of secondary EMPD with underlying carcinoma as compared to cases of primary EMPD (CK7+/CK20−).35 Gross cystic disease fluid protein-15 (GCDFP-15) is a marker for apocrine epithelium and is more commonly positive in primary EMPD and negative in cases of secondary EMPD with an associated malignancy.36
Mucin core protein (MUC) expression is useful in the diagnosis of MPD and EMPD.37 MUC1 positivity is noted in both MPD and EMPD. MUC2 expression is generally negative in primary EMPD but may be expressed in cases of secondary EMPD with an associated underlying colorectal adenocarcinoma.38
MUC5AC is more frequently positive in invasive and metastatic EMPD than in noninvasive EMPD.39
1938
A study investigating a relationship between expression of androgen receptor on Paget cells in EMPD and 5α-reductase levels showed an elevated 5α-reductase level more frequently in invasive (81%) compared with purely intraepidermal (45%) cases of EMPD.40
For invasive cases, men had a significantly higher level of androgen receptor and 5α-reductase positivity than women (70% vs 17%), suggesting the possibility of autocrine synthesis of androgens in EMPD and gender-specific microenvironments that may contribute to invasiveness of the disease.40 In a related study, Ki-67 and cyclin D1 were expressed more frequently in cases of invasive EMPD than in intraepidermal EMPD. When both Ki-67 and cyclin D1 were expressed, the likelihood of invasive disease was higher than when either was expressed alone.41 This study raised the question of whether androgens may be associated with cell-cycle regulation and invasiveness of EMPD.41
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE AND PROGNOSIS
The prognosis in patients with MPD depends on the presence or absence of a clinically palpable breast mass and nodal metastases. Patients with MPD who present with a palpable breast mass tend to have more advanced disease than patients without a palpable breast mass. In these 2 groups, the rates of metastases to the lymph nodes were 57% to 63% (with a palpable breast mass) versus 11% to 21% (without a palpable breast mass).42-44 In addition, patients with MPD who also present with a palpable mass were more likely to have invasive, rather than in situ, and multifocal ductal carcinoma.44 The median survival of patients with a palpable breast mass was 42 months compared to 126 months for patients without a palpable breast mass, and the 5-year overall survival rates of patients with a palpable breast mass were 35% to 43% versus 75% to 93% for patients without a palpable breast mass.43,45
As a result of the limited number of longitudinal studies, heterogeneity in disease stage, and variability in management of MPD, recurrence rates are extremely variable across studies. One study found about one-third of the underlying breast carcinomas were located more than 2 cm beyond the areolar margin. Thus, with limited excision of the MPD and the underlying breast carcinoma, rather than mastectomy, a significant number of underlying breast carcinomas may be inadequately treated, which may help explain why some studies show higher recurrence rates.43 See “Management: Mammary Paget’s Disease” below for a full discussion of treatment of MPD. The prognosis for primary EMPD is excellent with appropriate treatment, with 5-year overall survival rates ranging between 72% and 91% across several studies.4,5,8 Risk factors that appear to carry a worse prognosis include lymphovascular invasion and increasing depth of tumor invasion, with one study suggesting that a dermal invasion greater than 1 mm confers a worse prognosis.7 The presence of lymph node metastases markedly reduces overall survival and indicates a very poor prognosis, with 5-year survival rates ranging from 0 to approximately 20% in case series.8,17 Two studies noted that patients with elevated serum CEA levels were more likely to have a worse prognosis, with 1 study noting that all the patients with elevated CEA levels had metastatic disease, but not all patients with metastatic disease had elevated CEA levels.8,29 The usefulness of measuring CEA levels in the serum at this time is unclear; however, this particular study suggested that, for the subset of patients with a history of metastatic disease and elevated serum CEA, trending the serum CEA values over time may be useful in surveillance of the disease.29 Nevertheless, regular surveillance for early
20
detection of local recurrence is critical given the multifocal pattern often present in EMPD. The prognosis for secondary EMPD caused by an underlying adnexal carcinoma or visceral malignancy is generally worse than for primary EMPD and depends on the prognosis of the underlying cancer.17
MANAGEMENT
MAMMARY PAGET’S DISEASE
MAMMARY PAGET’S DISEASE
However, standardized, evidence-based treatment recommendations for MPD are not available because of the lack of studies directly comparing outcomes for mastectomy versus BCT plus radiotherapy. Most of the current treatment recommendations are based on small studies with variable treatment techniques and followup periods, making comparisons among different studies difficult. For patients with MPD with a clinically palpable breast mass, most studies recommend mastectomy versus BCT (resection of the nipple and areola with wide local excision of the breast mass) followed by wholebreast radiotherapy.43,45-47 In patients with an underlying invasive ductal carcinoma, SLNB is typically recommended at the time of excision if no clinically palpable pathologic nodes are identified. However, for patients with underlying invasive ductal carcinoma
Approach to the patient with mammary Paget’s disease
Mammogram
Longstanding
New onset
Biopsy
Underlying breast cancer Short trial of steroids or antifungals
Special stains (eg, CK7; CAM 5.2; mucin)
No improvement
Mastectomy vs breast conserving therapy PLUS lymph node evaluation
Confirmation of MPD
Adjuvant therapy
• Radiotherapy
• Chemotherapy
• Hormonal therapy
1939
20
and clinically pathologic lymph nodes, biopsy of the lymph nodes should be performed prior to surgery. If lymph node biopsy confirms metastatic disease, axillary lymph node dissection should be considered. If pathology is negative for metastatic disease on lymph node biopsy, SLNB should be considered at the time of wide local excision. In patients with MPD with negative mammography and without a palpable breast mass, most studies recommend mastectomy versus BCT followed by wholebreast radiotherapy.43,45-47 Most of these patients have ductal carcinoma in situ, rather than invasive ductal carcinoma, so many studies do not routinely recommend SLNB in these patients. However, 1 study found that approximately 20% of patients without an associated breast mass had metastases to the axillary lymph nodes and suggested consideration of SLNB even in cases of ductal carcinoma in situ.43 Another study in patients with MPD without any identified underlying breast carcinoma found that 11% had metastases to the axilla and, thus, recommended SLNB for all patients.48
Because all diagnoses of MPD require management by a surgical oncologist with expertise in breast cancer, a thorough discussion regarding the pros and cons of these various surgical approaches is warranted before proceeding with treatment.
EXTRAMAMMARY PAGET’S DISEASE
EXTRAMAMMARY
PAGET’S DISEASE
SURGERY
Surgery is generally considered the standard treatment for EMPD. However, local recurrences are common, even when wide excision margins are used, with studies reporting rates ranging from approximately 30% to 60%.7,49 Invasive disease has a higher recurrence rate than in situ disease, with one study reporting rates of 67% and 35%, respectively.7,49 The high recurrence rates are likely the result of the clinical characteristics of EMPD: the ill-defined clinical margins, multifocal nature of the tumor, and involvement of clinically normal-appearing adjacent skin.6 More extensive procedures are associated with lower rates of recurrence, but also may be more technically difficult and
Approach to a patient with extramammary Paget’s disease
Perianal, perineal, inguinal, axillary red patch/plaque
Recent
Longstanding
Biopsy Trial of steroids or antifungals
No improvement
Surgical treatment (Mohs surgery vs wide-local excision)
Consider nonsurgical treatment modalities if not a surgical candidate (eg, radiation, PDT, etc)
Special stains (eg, CK7; CAM 5.2; mucin)
Confirmation of EMPD
Internal malignancy workup
• Abdomen/pelvis imaging
• CXR
• Mammogram
• Consider PET-CT scan to r/o lymph node involvement and metastasis
• Colonoscopy
• Cystoscopy
• Pelvic exam
1940
disfiguring for patients. In one study, patients with primary vulvar EMPD treated with radical vulvectomy, radical hemivulvectomy, and wide local excision had recurrence rates of 15%, 20%, and 43%, respectively.7
A few studies have attempted to decrease recurrences of EMPD using adjuvant techniques for surgery. Intraoperative frozen-section analysis reduced recurrences in some studies but not in others.50,51 Multiple scouting biopsies performed prior to surgery have been reported to be helpful in delineating the extent of disease and surgical planning.52,53 Intraoperative CK7 immunostaining during Mohs micrographic surgery also has been reported to be helpful in delineating tumor margins.53
SLNB has been described in the treatment of EMPD.54
This technique has been limited to a small number of reported patients, and most cases of EMPD have in situ disease. However, SLNB may prove beneficial for the prognosis and management of patients with increased risk of metastatic disease, such as those with invasive disease or elevated serum CEA levels.55 A study involving patients with in situ, microinvasive (to the papillary dermis), or deeply invasive (to the reticular dermis or deeper) EMPD found that the incidence of sentinel lymph node metastasis was 16.9%. Stratified by depth of invasion, the rates were 0% for intraepidermal lesions, 4.1% for microinvasive disease, and 42.8% for deeply invasive disease.56 Thus, some advocate the use of SLNB and/or regional lymph node dissection in all high-risk EMPD cases, despite negative findings on PET-CT, as micrometastases are undetectable with this form of imaging.29
With the high rates of local recurrence and the significant morbidity associated with radical and repeated surgical procedures, Mohs micrographic surgery has been used to improve cure rates and for tissue sparing of critical genitourinary anatomic structures.6,7,57
The recurrence rate with Mohs micrographic surgery has ranged from 16% to 28% for primary EMPD in recent studies, and 50% for recurrent EMPD.6,57 It was also reported that 97% of the cases treated with Mohs micrographic surgery required margins of 5 cm from the clinical margin for tumor clearance.57 The same study found that surgical margins of 2 cm would clear only 59% of the cases, which is consistent with reported recurrence rates of approximately 40% with wide local excision. This further suggests a potential benefit of frozen horizontal sectioning for complete peripheral and deep margin mapping to reduce the possibility of residual tumor.
RADIOTHERAPY
Radiotherapy may be indicated in patients who are poor surgical candidates or are concerned with the risk of compromising genitourinary function as a consequence of the extensive surgery required for curative treatment.7 Although initial studies indicated poor success with radiotherapy as a primary treatment modality, subsequent case series reported acceptable outcomes, with recurrence rates of less than 35%.58-60 Even though these results may appear more favorable than some of the surgical modalities, it is important to note that the
20
sample sizes in these reports were several patients, making generalizations difficult. In addition, one of the studies reported no recurrences in a subset of 7 patients with intraepidermal disease but had a recurrence in 1 of 2 patients with invasive disease.59
Moreover, radiotherapy is beneficial for local recurrences after surgery or as an adjuvant therapy in those patients with a high risk of recurrence.61,62 No randomized controlled studies comparing surgery to radiotherapy have been performed as of this writing.
TOPICAL CHEMOTHERAPY AND IMMUNOMODULATOR
Topical 5-fluorouracil (5-FU) and imiquimod have been used to treat EMPD with varying degrees of success. 5-FU has been used as a neoadjuvant modality prior to surgery to delineate clinical margins and for early postoperative detection of recurrence.63,64 However, topical 5-FU has not proven to be a reliably curative agent in the treatment of EMPD because of the limited penetration of the drug and the inability to reach the deeper epidermal layers and adnexal structures that are frequently involved in EMPD.7,64
Imiquimod has been reported to result in clinical and histologic clearance in a few case series involving primary and recurrent EMPD.65,66 In one study of 8 patients with recurrent primary intraepidermal EMPD, 6 patients initially experienced complete clinical and histologic response, but 4 patients subsequently developed recurrences during the followup period (median: 35 months).67 All the patients with recurrences did not have progression to invasive disease, declined further surgery for their recurrences, and chose to retreat with imiquimod.67
As a result of the limited number of patients treated with these topical agents, the ideal duration and frequency of application is unknown. Further studies and long-term followup in a larger cohort are necessary.
PHOTODYNAMIC THERAPY
Photodynamic therapy has been used as an adjuvant to chemoradiotherapy, neoadjuvant prior to surgery, and as a primary modality with reasonable success.7 However, as in the case of other topical treatment modalities, the ideal duration and frequency of application is unknown. Further studies and long-term followup in a larger cohort are necessary.
SYSTEMIC CHEMOTHERAPY
Systemic chemotherapy has been used to treat patients with invasive and metastatic disease and may be considered in rare cases in which surgery and radiotherapy are contraindicated. Limited reports of systemic chemotherapy for the treatment of EMPD have been described, including a combination of low-dose 5-FU and cisplatin68; a combination of 5-FU, carboplatin/cisplatin, mitomycin C, epirubicin, and vincristine69,70; docetaxel71-73; and combination trastuzumab, docetaxel, and carboplatin followed by lapatinib.74
1941
20

Figure 114-1 Paget’s disease of the nipple. Erythematous and scaly plaque involving the nipple and areola.

Figure 114-2 Scrotal extramammary Paget’s disease. Moist, eroded, oozing plaque on the scrotum of an older man.

Figure 114-3 Perianal extramammary Paget’s disease presenting as moist, superficially eroded plaque.
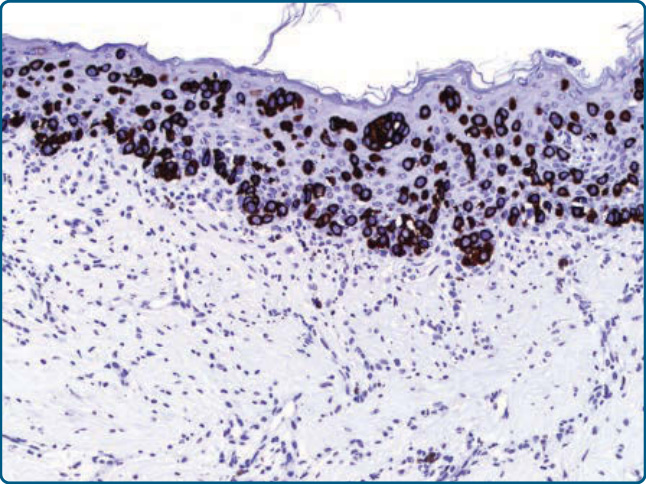
Figure 114-5 Anticytokeratin (CAM 5.2) is a sensitive marker for both mammary and extramammary Paget’s disease on histopathology. (Image used with permission from Thaddeus Mully, MD, UCSF.)
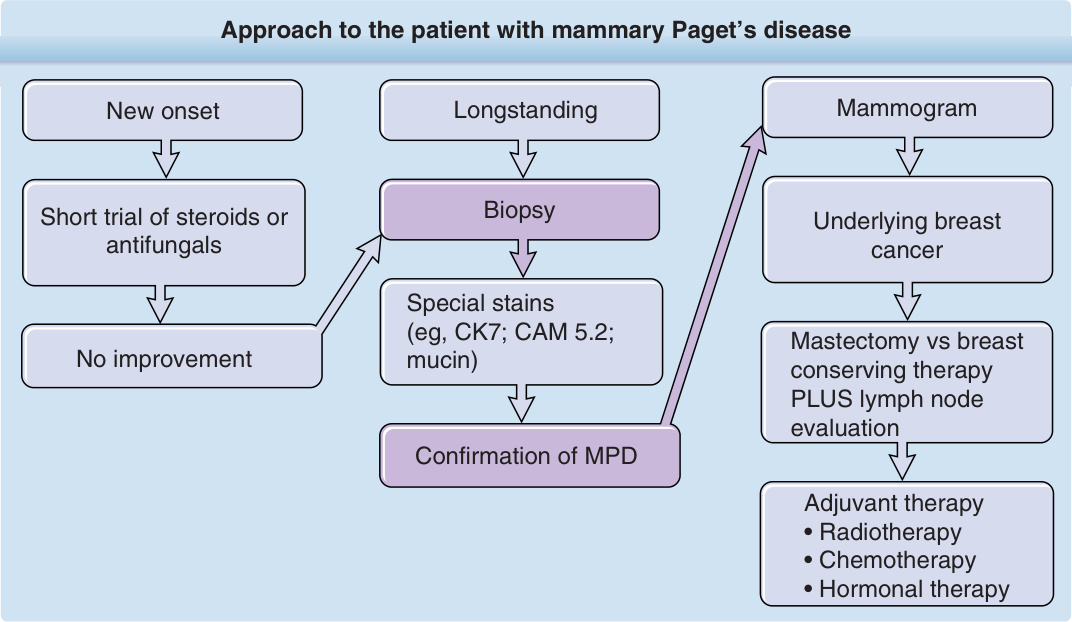
Figure 114-6 outlines an approach to treatment of MPD. Historically, the standard of care for MPD has been mastectomy, but emerging evidence suggests that select cases of MPD may be treated with breastconserving therapy (BCT) plus radiotherapy with excellent results and low rates of recurrences.45-47
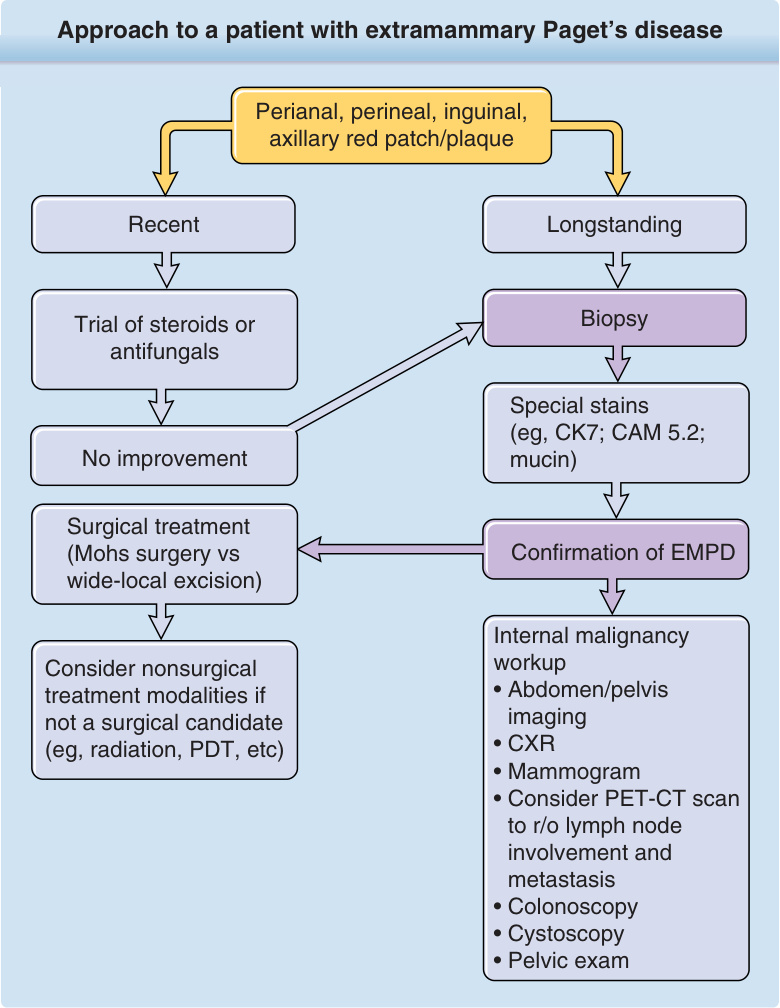
Figure 114-7 outlines an approach to treatment of EMPD. EMPD has been treated with a variety of modalities. The condition is most frequently managed with surgery, but other treatments have a role for poor surgical candidates and as adjuvant therapy.
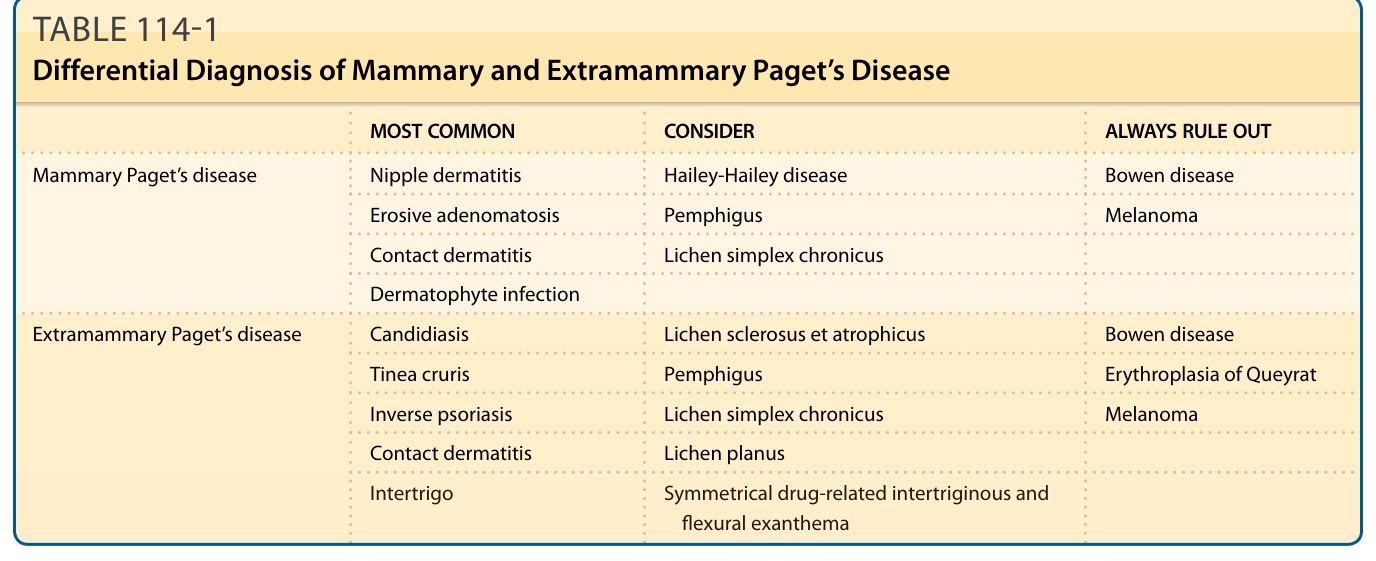
Table 114-1 outlines the differential diagnoses of MPD and EMPD.
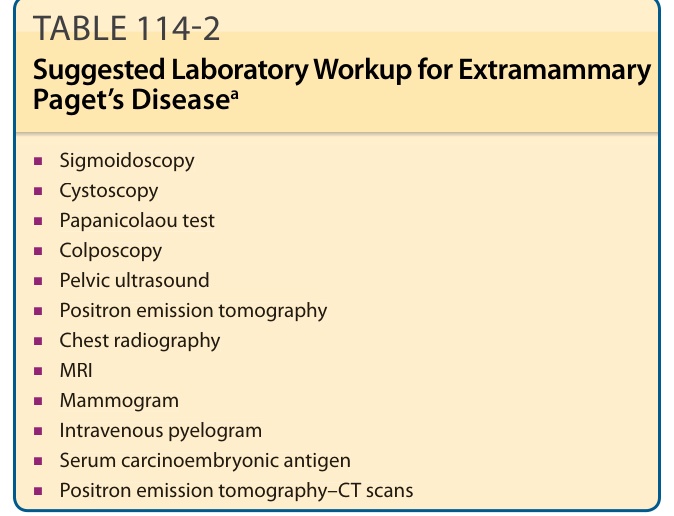
TABLE 114-2 Suggested Laboratory Workup for Extramammary Paget’s Diseasea
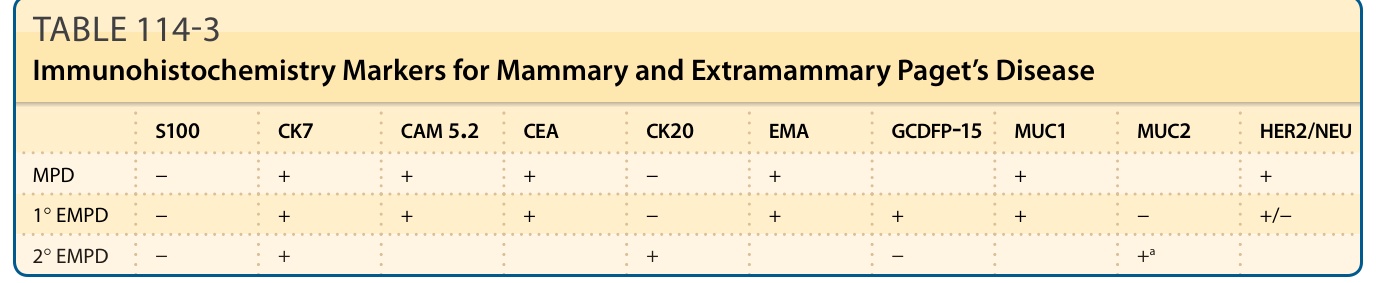
TABLE 114-3 Immunohistochemistry Markers for Mammary and Extramammary Paget’s Disease