Epithelial Precancerous Lesions
20
ACTINIC KERATOSES
AT-A-GLANCE
■ Precursor lesions of cutaneous squamous cell carcinoma (SCC).
■ Long-term and cumulative ultraviolet (UV) radiation exposure is the most important etiologic factor in the development of actinic keratoses.
■ Risk factors include fair skin, age, cumulative UV radiation exposure, immunosuppression, prior history of non-melanoma skin cancer.
■ The overall risk of progression to invasive SCC is estimated as 5% to 10%.
■ Treatment is recommended to reduce the risk of SCC formation and to improve patients’ quality of life.
■ Treatment modalities include cryosurgery, shave excision, curettage, dermabrasion, ablative lasers, topical drugs (diclofenac + hyaluronic acid, 5-fluorouracil ± salicylic acid, imiquimod, ingenol mebutate), chemical peelings, and photodynamic therapy.
Actinic keratoses (AKs, also known as solar keratoses or senile keratoses) are cutaneous lesions that consist of proliferations of atypical epidermal keratinocytes that may progress to invasive squamous cell carcinoma (SCC). The concept of a precancerous keratosis was first presented by Dubreuilh in the late 1800s. AKs were first identified and named keratoma senilis by Freudenthal in 1926. In 1958, Pinkus further characterized these lesions and coined the term actinic keratosis. It literally means a condition (-osis) of excessive horny (kerat-) tissue induced by a ray of light (aktis), presumably ultraviolet (UV) light. AKs have historically been considered precancerous or premalignant lesions with a potential for developing into SCCs. However, there is a debate at what grade of atypia AKs should be considered carcinoma in situ because not all AKs progress to SCCs and some lesions may spontaneously regress. Attempts have been made to coin AK as “keratinocytic intraepidermal neoplasia” grades I to III according to the degree of atypia.1 This concept is analogous to the grading of other precancerous lesions such as the classification of cervical intraepithelial neoplasia or vulvar intraepithelial neoplasia (VIN) as precursor lesions of cervical and vulvar carcinoma, respectively.
Regardless of the clinical course of single lesions, AKs are a strong indicator of chronic exposure to UV radiation with actinic skin damage and identify patients who are at high risk to develop nonmelanoma skin cancer. In an increasingly aging society with generations that poorly used sun protection measures and sunscreen, AKs are nowadays rated among the most common reasons to consult a dermatologist in regions with predominantly white populations such as the United States, Australia, and Europe.2 The high prevalence and the uncertainty of the clinical course of the precancerous lesions make AKs an important challenge for patients and physicians, and an economic burden for health-care providers.
EPIDEMIOLOGY
EPIDEMIOLOGY
In European countries, such as Spain and Austria, the prevalence of AKs in adult dermatology outpatients was reported to be approximately 30% in 2011. In the Netherlands, a total of 23.5% of the general population older than 50 years of age was estimated to be affected in 2011.3 Similar numbers were reported in the United States, where AK is the most common diagnosis among dermatology patients 45 years of age and older. The disease is estimated to account for more than 5 million physician visits in the United States per year. The highest prevalence of AK was shown in Australia, it being up to 59% in the general population older than age 40 years in the 1980s. In contrast, only 0.52% of dermatology patients in China were diagnosed with AK from 2008-2012. The prevalence in other geographical regions is widely unknown. Various risk factors for the development of AKs exist. The most important ones include skin phenotype, cumulative UV exposure, age, and gender. AKs occur most commonly in individuals with fair skin, red or blond hair, and blue eyes (Fitzpatrick type 1). People with darker skin (Fitzpatrick types 2 to 6), brown eyes, and dark hair are less likely to develop AKs.3 The risk of AK is strongly associated with high cumulative UV exposure. Workers with a long history of outdoor occupation, such as farmers, construction workers, or fishermen, have an up to 2.5-fold increased risk compared to indoor workers.4,5 This also accounts for individuals with predominantly outdoor hobbies.4,5
Evidence that sun exposure plays a role in the development of AKs is reflected by their distribution on the body. They typically develop on sun-exposed areas, such as the balding scalp, head, neck, forearms, dorsal hands, and in women, additionally the dorsal legs (Fig. 110-1).
20
Age is another major risk factor. The number of sunburns during childhood is associated with a higher likelihood of developing AKs in the future.5 Therefore, the age at which a person received the greatest amount and intensity of sun exposure appears to be important. The risk of AK steadily increases with lifetime exposure to UV radiation, as seen in the significantly higher prevalence of AK in elderly people.2,3 In Austria, for instance, 1.1% of female and 2.4% of male dermatology outpatients from 30 to 39 years of age are affected by AKs, compared to 68.1% of females and 89.7% of males older than 90 years of age.2 The prevalence increases with age in both sexes. However, men are more likely to develop AK than women. This presumably reflects greater cumulative sun exposure in males than in females, and less protection on the bald scalp.3,5,6
Immunosuppressed patients, such as organ transplant recipients, are at increased risk of developing AKs. In addition, immunosuppression is associated with both developing AKs earlier in life and with a more rapid malignant transformation.7 Furthermore, persons with certain genetic syndromes, namely albinism and xeroderma pigmentosum, are more likely to develop AKs. There are case reports of patients with Rothmund or Kindler syndrome who developed AKs early in life.
CLINICAL FEATURES
CLINICAL FEATURES
The typical patient with AKs is an older, fair-skinned, light-eyed individual, who has a history of significant sun exposure, who burns and freckles rather than tans, and who has significant solar elastosis on examination. AKs can be seen in younger individuals if they had sustained sufficient sun exposure over their lives. Eighty percent of AKs are found on chronically sun-exposed sites of the body, such as the bald scalp, face, ears, neck, forearms, and dorsal hands. They are mostly asymptomatic, but may come along with pruritus, burning or stinging pain, bleeding, and crusting.
1858
CLINICAL SUBTYPES
The typical AK lesion, sometimes called the erythematous AK, presents most commonly as a 2- to 6-mm, erythematous, flat, rough, gritty or scaly papule (Fig. 110-2). It is usually more easily felt than seen. AKs can vary in size and sometimes reach to several centimeters in diameter. They are most often found against a background of photodamaged skin (dermatoheliosis), with solar elastosis, dyspigmentation, yellow discoloration, ephelides and lentigines, telangiectasias, and sagging skin notably prominent. At times, the number and confluence of AKs are so great that the patient appears to have a rash. In some cases, multiple AKs may affect a large area of the sun-exposed skin. In addition, alongside clinically detectable AKs, multiple subclinical lesions may be present (Fig. 110-3). This concept is known as field cancerization and is crucial for the therapeutic approach. Various definitions of field cancerization have been proposed including (a) more than 2 AKs within 1 skin area with signs of solar damage, (b) at least 3 AKs within 25 cm2 of skin, or (c) more than 5 AKs in 1 body region or field and contiguous areas of chronic actinic sun damage and hyperkeratosis.8
In addition to the typical erythematous AK, there are several other clinical subtypes. Some AKs have a pigmented brownish appearance and may be difficult to distinguish from other dermatoses of the elderly, such as seborrheic keratosis. If such lesions are ill defined,
some authors have proposed the term spreading pigmented actinic keratosis. A hypertrophic AK presents as a thicker, scaly, rough papule or plaque that is skincolored, gray-white, or erythematous (Fig. 110-4). It can be found on any chronically sun-exposed body site, but has a propensity for dorsal hands, arms, and scalp. A typical erythematous AK can progress into an hypertrophic AK. It can be difficult to distinguish an hypertrophic AK from an SCC, clinically necessitating a biopsy. Biopsies must be taken to a level deep enough to ensure that the dermal extent of the keratinocytic proliferation can be evaluated in order to obtain an unequivocal histopathologic diagnosis. Induration, inflammation, pain, and ulceration are the main clues to the transition of AK to SCC. Cutaneous horn, also known as cornu cutaneum, refers to a reaction pattern and not a particular lesion. In reference to AKs, a cutaneous horn is a type of hypertrophic AK that presents with a conical hypertrophic protuberance emanating from a skin-colored to erythematous papular base (Fig. 110-5). Classical definitions of a cutaneous horn maintain that the height is at least one-half of the largest diameter. Approximately 21% of all cutaneous horns represent AKs. The pathology underlying a cutaneous horn can be a number of different lesions, such as AK, SCC, seborrheic keratosis, filiform verruca vulgaris, trichilemmoma, and keratoacanthoma.
20
A
B
Actinic cheilitis represents confluent AKs on the lips, most often the lower lip. Persons with this condition have red, scaly, chapped lips, and at times erosions or fissures may be present (Fig. 110-6). The vermilion border of the lip is often indistinct, and focal hyperkeratosis and leukoplakia also may be seen. Individuals with this condition often complain of persistent dryness and cracking of the lips. The diagnosis of actinic cheilitis should always be suspected in patients with photodamaged skin and such complaints. Biopsy is then necessary to confirm the diagnosis. Persistent ulcerations or indurated areas on the lip are suspicious for SCC.
CLASSIFICATION
The widely accepted Olsen classification suggests 3 grades of clinical severity of AK.8,9 It is based on the palpable thickness of AK lesions. According to this classification, grade 1 includes lesions that are mild, slightly palpable, and are better seen than felt. Grade 2 represents lesions that are moderately thick and easily seen and felt. Grade 3 lesions are severe, very thick and/or obvious AKs (Table 110-1).9
On a histologic level, a recommended scheme for grading AK severity is the Roewert-Huber classification.8,10 This scheme distinguishes 3 types of AK based
1859
20
A
B
on the extent of atypical keratinocytes in the epidermis. In type AK I, atypical keratinocytes are restricted to the lower third of the epidermis and are only found within the basal and suprabasal layers. In type AK II, atypical keratinocytes are found within the lower two-thirds of the epidermis, alternating with zones of normal epidermis. In the upper papillary dermis buds of keratinocytes can be found. In type AK III, atypical keratinocytes extend to the lower two-thirds of the full thickness of the epidermis. They can also involve the epithelia of the hair follicle, infundibula, and acrosyringium. As in type AK II, buds of keratinocytes can be found in the upper papillary dermis. If a biopsied AK lesion shows different histologic types, the classification suggests that the highest type defines the
1860
lesion. Histologically, type I and type II AK represent the same severity grade as the former term “early in situ SCC.” Type AK III has been proposed to be equivalent to the previous term “in situ SCC”.10
In daily practice, AK is a clinical diagnosis. However, it was shown that the clinical classification following Olsen and the histologic classification of Roewert- Huber do not match in all cases. In a systematic study of 892 AK lesions, a correlation between both classification systems was found in 480 lesions (54%) only. Whereas 21 out of 259 lesions (8%) that were clinically graded as mild (Olsen grade 1) were histologically severe (Roewert-Huber type AK III), 36 out of 101 lesions (36%) that were clinically severe (Olsen grade 3) were histologically mild (Roewert-Huber type AK I).11
Clinical Classification (Olsen et al.9) Grade 1 (Mild)
■Slight palpability
■AK better felt than seen Grade 2 (Moderate)
■Moderately thick AK
■Easily seen and felt Grade 3 (Severe)
■Very thick or obvious AK
Histologic Classification (Roewert-Huber et al.10) Early in situ SCC (type AK I)
Histologic Classification (Roewert-Huber et al.10) Early in situ SCC (type AK I)
■Involvement of basal and suprabasal layers of the epidermis
■Involvement of basal and suprabasal layers of the epidermis
■Nuclei hyperchromatic and variable in size
■Nuclei hyperchromatic and variable in size
■Loss of nuclear polarity Early in situ SCC (type AK II)
■Loss of nuclear polarity Early in situ SCC (type AK II)
■Involvement of the lower two-thirds of the epidermis
■Involvement of the lower two-thirds of the epidermis
■Alternation with zones of normal epidermis
■Alternation with zones of normal epidermis
■Buds of keratinocytes in the upper papillary dermis In situ SCC (type AK III)
■Buds of keratinocytes in the upper papillary dermis In situ SCC (type AK III)
■Involvement of more than two-thirds of the full epidermal thickness
■Involvement of more than two-thirds of the full epidermal
thickness
■Involvement of hair follicle, infundibula, and acrosyringium
■Involvement of hair follicle, infundibula, and acrosyringium
■Buds of keratinocytes in the upper papillary dermis
■Buds of keratinocytes in the upper papillary dermis
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
ETIOLOGIC FACTORS
Fair skin and exposure to UV radiation are the most important contributing factors for the formation of AKs. The majority of lesions develop in areas with chronic exposure to sunlight, such as the balding scalp, nose, ears, lips, and dorsal hands and forearms. A high extent of cumulative UV exposure, frequent sunburns in patient history, poor use of sun protection, and outdoor activities or occupations have been consistently associated with AK formation. Other risk factors include male sex, advancing age, and immunosuppression. It is currently under debate whether infection with human papillomavirus (HPV; particularly HPV types 5, 8, 21, and 38) contributes to the development of AK. Although HPV was detected in several epithelial tumors of the skin, it is uncertain if there is a causal relationship or only random coincidence as a result of the high prevalence of HPV infection. Rare exogenous risk factors comprise ionizing radiation and radiant heat. Rare endogenous predisposing conditions are genetic disorders with impaired DNA damage repair mechanisms after exposure to UV like xeroderma pigmentosum, Bloom syndrome, and Rothmund-Thompson syndrome.
PATHOGENESIS
Chronic UVB radiation induces genetic alterations of the keratinocytes residing at the basal layer of the epidermis. On a molecular level, UV light induces the formation of cyclobutane pyrimidine dimers which modify the structure of the DNA (photomutagenesis). Inactivating mutations of the tumor-suppressor gene p53 occur as early and common events (Fig. 110-7). p53 has a critical role in cell-cycle progression and DNA damage repair. If the gene is inactivated, p53- mutant keratinocytes show unrestricted cell growth and acquire cellular and morphologic atypia. Somatic UV signature mutations of p53 are present in more than 50% of all AKs and SCCs. In contrast, activating mutations of the oncogene H-ras lead to constitutive activation of the extracellular signal-regulated kinase signaling pathway and uncontrolled proliferation of affected cells. Other UV-induced mutations may affect the genes p16, K-ras, telomerase, CDKN2A, nuclear factor κB, or tumor necrosis factor α.11 Photodamaged transformed keratinocytes escape apoptosis and immunosurveillance and proliferate into clinically and histologically evident premalignant lesions. Notch 1 regulates numerous processes in keratinocytes such as proliferation, differentiation, and apoptosis. Proper expression of Notch 1 within the epidermis appears to be tumor suppressive and to prevent the progression to invasive SCC, which may show decreased levels of the protein. In addition to
20
epidermal tissue alterations, there is growing evidence that mesenchymal factors within the dermis such as the Notch/CSL signaling pathway have a significant role in the establishment of epithelial lesions.12
DIAGNOSIS
DIAGNOSIS
The diagnosis of AK is usually made clinically by touch and visual inspection recognizing the typical clinical features. Some lesions present as visually discreet macules or patches that are diagnosed best by feeling their rough texture. If the diagnosis is uncertain or if SCC cannot be excluded clinically, a histologic examination is obligatory. Common indications for a biopsy are rapidly enlarging lesions, bleeding or ulceration, evidence of inflammation, strong induration, lesions extending beyond 1 cm of size, or resistance to treatment.
HISTOPATHOLOGY
A punch or shave biopsy should be performed to confirm the diagnosis. The depth of the biopsy needs to reach the mid-reticular dermis to allow for the assessment of invasiveness of a given lesion. Initially, a compact packing of basal and suprabasal atypic keratinocytes with hyperchromatic and pleomorphic nuclei can be seen. Atypic mitotic figures, apoptotic cells and dyskeratosis may be present. The architecture is increasingly lost in the basal layers, but not the full thickness of the epidermis (Fig. 110-8). The alternation of hyperorthokeratosis and hyperparakeratosis is common in later stages, a feature that is referred to as “flag sign” or “pink and blue.” Per definition, the lesion is confined to the epidermis. The underlying dermis often shows solar elastosis and a superficial inflammatory infiltrate. Immunohistochemically, AK lesions show increased expression of p53, proliferating cell nuclear antigen, Ki-67 (MiB-1), and cyclin E. Histologic variants comprise lichenoid, bowenoid, and, rarely, acantholytic forms.
DERMOSCOPY
If it is difficult to recognize the clinical features by naked eye, dermoscopic evaluation may help to facilitate the correct diagnosis. Common features of nonpigmented lesions are scales that appear as whitish or yellowish crystalline structures and a reddish pseudonetwork with erythema and wavy configuration of telangiectasias between enlarged hair follicles. The follicles may show a perifollicular halo, resulting in a “strawberry pattern.” Hyperkeratotic AK lesions on the face may have prominent keratotic plugs within the hair follicles (targetoid-like pattern). The rosette sign consists of white dots localized inside the follicular openings, which may reflect alternating orthokeratosis and parakeratosis. Pigmented lesions may show brown dots and globules surrounding the follicular openings.
1861
20
Schematic overview on the etiology and pathogenesis of actinic keratosis development
X-ray
UV
Tar
HPV As
Immunosuppression
p53 loss Ras activation, chromosomal aberrations, defective apoptosis… p16 loss, other mutations
Sequential progression
AK II AK I Normal skin
AK III
Decreased notch/CSL signaling
Direct malignant transformation
SCC
SCC
1862
A
B
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
There are various dermatoses that may be difficult to differentiate from AKs. Spreading pigmented AK may mimic seborrheic keratosis or facial lentigo maligna. In contrast to spreading pigmented AKs, seborrheic keratoses have a velvety to finely verrucous surface that usually feels soft and greasy on palpation. In addition, seborrheic keratoses are also found on the trunk and other body surfaces that are rarely exposed to sunlight. Dermoscopy can help to distinguish pigmented AK from facial lentigo maligna. Dermoscopic findings of pigmented AK are white and evident follicles, scales, and red color. Intense pigmentation and gray rhomboidal lines are diagnostic clues for lentigo maligna.13 In rare cases, disseminated superficial actinic porokeratoses may affect the face and be confused with AK. The flat lesions are normally asymptomatic and surrounded by a ridge-like border. Besides other precancerous (eg, arsenical keratosis) or malignant (eg, SCC) lesions, differential diagnoses include melanocytic nevi, senile lentigo, and cutaneous lupus erythematosus.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
Established AKs usually take a chronic course and lesions may persist, spontaneously regress, or progress to invasive SCCs. The likelihood for these events was investigated in a panel of studies, but revealed inconsistent and varying results. Most investigations show major methodologic limitations with a follow up
20
period of less than 12 months and are of low quality. Thus, reliable estimates for the clinical course and prognosis of AK lesions remain uncertain to date.
PROGRESSION TO INVASIVE SQUAMOUS CELL CARCINOMA
Although atypical keratinocytes may penetrate the basement membrane and become invasive, the annual progression rate of a single lesion to SCC is supposedly below 1%, ranging from 0 to 0.53% in individuals without a history of nonmelanoma skin cancer and without immunosuppression. Currently, there is an intense debate on how the progression from AK to SCC occurs. One model assumes that low-grade AKs successively progress toward high-grade AKs and ultimately invade the epidermal–dermal junction (classic pathway of progression). However, there is evidence that not all SCCs develop from high-grade AKs, but that the majority of invasive carcinomas have their origin from AK type I. These findings suggest that each AK per se bears the potential to progress into SCC regardless of the grade of histologic atypia, and that a direct cancerous invasive transformation of basaloid atypical keratinocytes is the most common mechanism of disease progression (differentiated pathway of progression). Overall, it is estimated that only 5% to 10% of all AKs progress to invasive SCC (see Fig. 110-7). The risk for progression of AK to SCC reported in the literature varies from less than 1% to 20%. The risk for SCC formation increases with the duration of presence, total lesion count (>5), and individual patient characteristics, such as suppressed immune status. Conversely, more than 60% of cutaneous SCCs are believed to develop from preexisting AKs. Several histopathologic studies examined invasive SCC specimens and determined the percentage of associated or contiguous AKs. Premalignant AK-like areas were detected at the periphery or within the invasive parts of SCC in 60% to 100% of cases.14-19 A lesion may become tender or painful and show signs of inflammation prior to progression, requiring a biopsy to rule out SCC formation.
REGRESSION
Spontaneous resolution without treatment may occur. The annual regression rates for single AK lesions identified in cohort studies generally range from 20% to 30% with a large variation, depending on the presence and maintenance of risk factors. For instance, limiting sun exposure and the use of sunscreen may promote regression. The resolution rates of complete fields on face and scalp are lower and have been estimated to be 0 to 7.2%.8 Lesions that have regressed can eventually relapse, with recurrence rates ranging from 15% to 53%.8 However, it is often not entirely clear if these lesions are true local relapses or if they have developed de novo. The presence of AKs indicates long-term sun damage and identifies individuals who are at high risk for developing actinic skin lesions. Thus, AKs are sometimes considered a chronic skin condition where lesions come and go.
1863
20
TREATMENT
TREATMENT
It is not possible to reliably predict which lesions will persist, regress, or become SCCs based on clinical and histologic features. Thus, despite the relatively low risk of transformation and high rates of spontaneous resolution, early and consequent therapy is warranted. Furthermore, treatment can help minimize symptoms like scaling, pain, or pruritus, improve the cosmetic appearance and ultimately improve the quality of lives of the patients. A plethora of treatment options exists and more agents and procedures are constantly being launched and approved by regulatory agencies. Treatment modalities for AKs can be broadly divided into lesion-targeted therapies and field-targeted therapies (Table 110-2).
LESION-TARGETED THERAPIES
The majority of lesion-targeted therapies are mechanically destructive, such as cryosurgery, surgical approaches, or ablative lasers. Other lesion-directed approaches include medical treatment with 5-fluorouracil (5-FU) plus salicylic acid and lesion-directed photodynamic therapy (PDT).
Cryosurgery: Liquid nitrogen cryosurgery is a commonly performed destructive procedure that is typically administered with a spray device, cotton swab, or probe. The freezing procedure leads to the formation of extracellular and intracellular ice crystals. With subsequent thawing, destruction of atypical keratinocytes occurs through cell dehydration and rupture of cell membranes and organelles. Cryosurgery is easy to administer, cheap, and efficient in clearing single lesions. More benefits include the lack of need for local anesthesia and simple posttreatment care. Frequent short-term complications are procedure-related discomfort with pain and hemorrhage, accompanied by, in many cases, the formation of a blister. Further drawbacks include the danger of nerve damage, pigmentary changes resulting from the destruction of adjacent melanocytes, and scarring. The application procedure of cryosurgery for AK is little standardized with varying durations of freeze– thaw cycles, number of freeze–thaw repetitions, or duration of freezing. Cryosurgery is suitable to treat a limited number of clinically perceptible or symptomatic lesions.
Surgical Approaches: Surgical approaches generally have the advantage of obtaining specimens for further histopathologic assessment. Conventional surgical
ADVANTAGES DISADVANTAGES
Lesion-Targeted Therapies
Liquid nitrogen cryosurgery
■Short treatment duration (sec-min)
■No need for local anesthesia
■Histopathologic assessment
Surgical approaches (conventional excision, shave excision with/without electrodessication)
■Low recurrence rates
■Little standardized
■Frequent blister formation
■Hypopigmentation
■Local anesthesia needed
■Surgery-related complications
■Hypopigmentation/hyperpigmentation
■Scarring
Ablative lasers
■Short treatment duration
■Dyspigmentation
■Easy application by the patient
Topical therapy (5-fluorouracil plus salicylic acid)
■No need for local anesthesia
■No need for local anesthesia
Lesion-directed photodynamic therapy (PDT) (“patch” PDT)
■Cosmetic outcome
Field-Targeted Therapies
■Risk of scarring
■High equipment costs
■Long treatment duration (6-12 weeks)
■Local inflammation
■Local pain and adverse events (eg, erythema, edema, erosion)
■Lamp device needed
Topical/Medical
■Application by the patient
5-fluorouracil Imiquimod Diclofenac-Na Ingenol mebutate
■Cosmetic outcome
■Potential of contact hypersensitivity
■Treatment duration (3-90 days)
■Local adverse events (eg, erythema, edema, erosion)
■Rarely systemic adverse events
Procedural
■Cosmetic outcome
■Local adverse events (eg, erythema, edema)
Conventional PDT (with blue light or red light)
■Local pain/burning sensation
■Lamp device needed
Natural daylight PDT
■Cosmetic outcome
■Local adverse events (eg, erythema, edema)
Natural daylight PDT ■Cosmetic outcome ■Local adverse events (eg, erythema, edema)
1864
■Dependent on weather condition (<10°C [50°F], no rain)
■Dependent on weather condition (<10°C [50°F], no rain)
excision is not a routine procedure for AK. It can be considered for clinically atypical lesions that warrant further histologic evaluation or to rule out invasive SCCs. Shave excisions are commonly performed for single hyperkeratotic lesions. However, the pathologic evaluation after shave excision may be problematic if the biopsy is taken too superficially to determine if the lesion is confined to the epidermis or invasive. Curettage takes advantage of a curette to mechanically scrape away the atypical keratinocytes. It may either be applied as single technique or in combination with shave excision, electrodessication, or cryosurgery. It is useful for single, hypertrophic AKs on the extremities, and is technically easy to perform in an office-based setting. Yet, the quality of specimens obtained with curettage is usually poor and histologic evaluation may be equivocal. Some studies suggest that surgical therapies show lower rates of recurrence than other destructive treatments. Nevertheless, disadvantages of all surgical procedures include the need for local anesthesia, potentially prolonged wound healing, infection, bleeding, dyspigmentation, scarring, and rather poor cosmetic outcomes.
Laser Therapies: Laser devices are increasingly used for the treatment of AKs. Most experience and evidence has been collected for ablative resurfacing with the carbon dioxide (CO2) and erbium:yttrium aluminium garnet (Er:YAG)-laser. Both devices ablate the epidermis at varying depths, allowing for reepithelialization with adnexal or lesion-adjacent keratinocytes that are less actinically damaged. The CO2 laser has a higher penetration depth than the Er:YAG laser and may offer advantages when treating thicker and hyperkeratotic lesions. Adverse events comprise hypopigmentation and atrophic scarring. Although lesion clearance rates were promising in a panel of studies, AKs can relapse after laser treatment. Laser resurfacing is probably best reserved for use by specially trained and experienced physicians and for patients with more cosmetic concerns. The efficacy of nonablative fractional photothermolysis is currently unclear and well-designed trials are lacking.
Lesion-Directed Photodynamic Therapy: PDT is increasingly used for the treatment of both single AK lesions and field cancerization with superb cosmetic outcomes. It is based on the topical application of a photosensitizing agent followed by exposure to a specific wavelength of light. 5-Aminolevulinic acid (ALA) and methyl aminolevulinate (MAL) are the 2 substances that are used in PDT for AKs. They are absorbed by the epidermis and preferentially accumulate in atypical cells where they are further processed to protoporphyrin IX. Subsequent exposure to a specific wavelength light source activates protoporphyrin IX, resulting in a phototoxic reaction with release of reactive oxygen species and, ultimately, in destruction of target cells by necrosis and apoptosis. Although PDT is predominantly perceived as field therapy (see section “Field-targeted Therapies”), 5-ALA can be applied with a patch to isolated lesions to spare and protect healthy skin. This targeted application of the photosensitizer can help minimize local adverse events
20
like erythema, crusting, blister formation and is usually well tolerated by patients. The efficacy of the patch PDT is high and results in excellent cosmetic outcomes. In particular, hypopigmentation which is observed in many cases with destructive lesion-directed approaches is not seen with this technique.
FIELD-TARGETED THERAPIES
Field-centered approaches do not target at single lesions, but treat entire actinically damaged areas (“fields”). This strategy is applicable if several illdefined AK lesions exist within 1 field or if subclinical lesions are suspected and field cancerization is present. Field therapies can be further categorized into topical and procedural treatments (see Table 110-2).
Topical Treatment: A variety of topical agents exist for the treatment of AKs such as diclofenac, 5-FU, imiquimod, and ingenol mebutate (Table 110-3). Diclofenac is an inhibitor of cyclooxygenase and belongs to the nonsteroidal antiinflammatory drugs. Topical therapy with 3% diclofenac in 2.5% hyaluronic acid gel is a widely used effective treatment option for patients with multiple AKs or field cancerization.20 It was shown to be protective against the appearance of new AKs, as it also acts against subclinical lesions.21
Diclofenac is well tolerated, but may lead to local adverse events, such as erythema, scaling, burning
DRUG PREPARATION DOSAGE/APPLICATION
Diclofenac-Na 3% gel Twice daily for 90 days
5-Fluorouracil (5-FU) 0.5% cream Once daily for up to 4 weeks
1% cream Twice daily for 2-6 weeks
4% cream Once daily for 4 weeks
5% cream Twice daily for 2-4 weeks
2% solution Twice daily for 2-4 weeks
5% solution Twice daily for 2-4 weeks
5-FU plus salicylic acid (SA) 0.5% (5-FU) and 10% (SA) solution Once daily up to 12 weeks
Imiquimod 5% cream Three times per week for 4 weeks
3.75% cream Once daily for 2 weeks
2.5% cream Once daily for 2 weeks
Ingenol mebutate 0.015% gel Once daily for 3 days
0.05% gel Once daily for
0.05% gel Once daily for 2 days
1865
2 days
20
sensation or pruritus. The recommended treatment duration of 90 days with twice daily application is relatively long. This may have a negative impact on practicability and patient adherence.22
5-FU is a pyrimidine analog and acts as an antimetabolite and via inhibition of the thymidylate synthetase as a cytostatic drug. In a cream formulation, 5-FU is a well-established topical treatment option for AK. 5-FU is available in numerous preparations, most commonly as 0.5% cream once daily or 5% cream twice daily. Both are effective and similarly safe, but patients may prefer the 0.5% preparation as it is applied only once daily.23 Typical adverse events are erythema, erosion and discomfort at the site of application. Treatment duration is usually 2 to 4 weeks. Another formulation is a combination of 0.5% 5-FU with 10% salicylic acid.24,25 It is applied once daily for up to 12 weeks on an area not larger than 25 cm2. It may be more suited for hypertrophic lesions than 5-FU alone because salicylic acid has a keratolytic effect and improves the penetration of 5-FU. Imiquimod is a Toll-like receptor 7 agonist and activates innate immune cells to produce interferon-α and other cytokines. Topical imiquimod is an effective treatment option for AK and available as 2.5%, 3.75%, and 5% cream.26,27 Application frequency depends on which concentration is used. Imiquimod at 2.5% and 3.75% concentration is usually applied once daily for 14 consecutive days. The 5% formulation is applied 3 times per week during a 4-week period. Adverse events are usually limited to the site of application including local irritation, pain, pruritus and swelling. In some cases, systemic events, like cardiovascular disorders, myalgia, arthralgia, and flu-like symptoms, may occur. In the light of long-term experience and better tolerability, 3.75% imiquimod is commonly preferred for the treatment of single AK lesions as well as for field-directed therapy.8 In immunosuppressed patients, 5% imiquimod cream was shown to be safe. Ingenol mebutate is a hydrophobic triterpene ester that is extracted from the sap of the plant Euphorbia peplus. It is effective against AK by chemoablative and immunostimulatory properties.28,29 Ingenol mebutate is available as a 0.015% gel for scalp and face and a 0.05% gel for the trunk and extremities. In contrast to other topical treatments for AK, 0.015% and 0.05% ingenol mebutate are only applied for 3 and 2 consecutive days, respectively. Local adverse events are virtually obligatory and are irritation, pruritus, and inflammatory changes, including erythema, blister, edema, erosion, scaling, and crusting. All these reactions appear early and usually subside within 14 days.30 However, because of the short treatment duration and good efficacy, ingenol mebutate was shown to increase treatment satisfaction and the quality of life of patients.31
Cryopeeling: This procedure refers to the extensive application of liquid nitrogen not only to single lesions, but to a complete field of manifest and subclinical AK. Cryopeeling is relatively easy to apply and was found effective for hypertrophic AK. Compared to conventional cryosurgery, it may help to reduce
1866
recurrence rates, although it bears a higher risk for hypopigmentation of treated areas.
Chemical Peelings: Medium-depth chemical peels using Jessner solution and 35% trichloroacetic acid, 70% glycolic acid, or solid CO2 are moderately effective in treating diffuse nonhypertrophic AKs, especially when a series of such peelings is repeated over time. They cause skin damage in the superficial papillary dermis and induce a wound reaction with exfoliation of the atypical keratinocytes and reepithelialization. Common side effects are stinging, burning sensation, erythema, and scaling. Deep chemical peelings using phenol or higher concentrations of trichloroacetic acid are more effective in treating hyperkeratotic AK or AK with appendageal epithelial atypia. However, they are rarely used because of the potential cardiac and renal toxicity of phenol and a higher risk of scarring, infection, and hypopigmentation.
Dermabrasion: Dermabrasion (also known as surgical skin planing) is an older technique that is nowadays rarely used for AK treatment. It is based on physical ablation of lesions with superficial abrasion of the epidermis at the level of the epidermis. Devices for dermabrasion are either drywall sanding sheets or diamond fraises that are powered or handheld. The procedure is painful and should be performed under sedation or general anesthesia. It may be applied for field therapy for an actinically damaged bald scalp or forehead.
Field-Targeted Photodynamic Therapy: Field-targeted PDT is usually performed with 5-ALA cream or MAL nanoemulsion as photosensitizing substances in combination with visible light (ie, blue, green or red light). Randomized, placebo-controlled studies demonstrated the efficacy of both ALA-PDT and MAL-PDT. They are equally effective, with lesion clearance rates ranging from 70% to 90%. A common adverse event is local discomfort ranging from burning or stinging to intolerable pain during exposure to the light source. Allergic reactions to ALA and MAL have been rarely reported. One to 2 days after treatment, local erythema, edema, blistering, sterile pustule formation, and crusting are commonly observed as clinical correlates for the phototoxic reaction. The cosmetic outcome of PDT is excellent and the term photorejuvenation has been coined. The effect is characterized by collagen remodeling and a decrease of small wrinkles, telangiectasias, and lentigines. An alternative to conventional PDT is the so-called natural daylight PDT, using much shorter incubation times of MAL/ALA and exposing the affected skin to sunlight instead of artificial visible light. Within 30 minutes after topical application of MAL/ALA patients are advised to stay outdoors for 2 hours. Natural daylight PDT is significantly less painful than conventional PDT, while the other local side effects are comparable. For the treatment of mild to moderate AKs, the effectiveness of natural daylight PDT was noninferior to conventional PDT in several trials.
APPROACH TO INDIVIDUAL MANAGEMENT
As described above, there are a number of effective lesion-targeted and field treatments available to choose from to decrease the burden of AKs. The individual patient’s needs and expectations, the physician’s skills, the mechanisms of action of the various treatments and their side-effect profiles, and the costs of the agents and procedures should all be considered when choosing a treatment strategy. To help physicians in their choice several national and international guidelines for the management of AKs have been proposed.8,32
PREVENTION
PREVENTION
Measures of primary prevention are primarily based on the avoidance of exposure to UV, because it is the main risk factor for the development of AKs. Educational and preventive efforts should be directed toward all patients, including children and high-risk populations such as organ transplant recipients or outdoor workers. Minimizing UV radiation is the single most effective means of decreasing the risk of AKs. Because complete avoidance of the sun is impractical, the next best preventive measures are to avoid exposure to intense midday sun; consistently apply and reapply broad-spectrum sunscreens; wear UV-protective clothing, hats, and sunglasses; install UV-protective windows where indicated; and make sure to take an oral vitamin D supplement if necessary to avoid vitamin D insufficiency or deficiency. Tanning beds should be avoided. Newborns should not be exposed to sun.
USE OF SUNSCREENS
Numerous randomized studies show that the use of sunscreen can decrease the incidence and prevalence of AKs, reduce the number of AK lesions, and increase their rate of regression. There is also evidence that sunscreen use can prevent certain types of skin cancer, mostly SCC. Broad-spectrum sunscreen against UVB and UVA radiation with a minimum sun protection factor of 30 should be applied to areas that cannot be protected by physical measures like UV-protective clothes or UV avoidance. It is important to apply sunscreen in sufficient amounts at least 20 minutes before going outside and to reapply it every 2 to 3 hours especially when excessive sweating or swimming.
CHEMOPREVENTION
Some agents or dietary interventions can prevent or delay the development of AKs in high-risk populations. There is limited evidence that adhering to a low-fat diet may decrease the incidence of AKs and nonmelanoma skin cancer. Nutritional supplements, like vitamin A, selenium, and carotenes, are currently
20
not recommended for prevention. Topical imiquimod also has been safely used in organ transplant recipients to prevent development of cutaneous SCC.
Retinoids: There is a debate on whether the application of topical retinoids is effective in the prevention of AKs because prevention trials have yielded discordant results. Unlike the controversy with topical retinoids, there is strong evidence for the use of systemic retinoids in preventing nonmelanoma skin cancer and AKs, especially in high-risk populations, such as organ transplant recipients, patients with xeroderma pigmentosum, and other chronically immunosuppressed patients.33 However, systemic retinoids are only effective while taking them. Their use is also limited by the frequent occurrence of systemic toxicities, including hypercholesterolemia, hypertriglyceridemia, mucocutaneous xerosis, musculoskeletal abnormalities, and alteration in liver function. Thus, when considering the use of systemic retinoids as chemoprevention one must weigh the risks and benefits.
Nicotinamide: Oral nicotinamide (vitamin B3) was reported safe and effective in reducing the rates of new nonmelanoma skin cancer and AK in highrisk patients in a recent phase III trial. Specifically, the number of AKs was reduced by 13% in patients who took 500 mg of nicotinamide twice daily for 12 months compared to placebo.34 However, the beneficial effects disappeared when the treatment was discontinued. Furthermore, it is unclear if nicotinamide is associated with an increased risk for infectious adverse events.
BOWEN DISEASE
AT-A-GLANCE
■ Bowen disease (BD) is squamous cell carcinoma (SCC) in situ.
■ It can progress to Bowen carcinoma (invasive SCC) in up to 5% of cases.
■ Etiologic factors include UV radiation, arsenic, previous therapy with psoralen and UVA radiation, immunosuppression, exposure to ionizing radiation, and infection with human papillomavirus.
■ Clinical variants are pigmented, intertriginous, periungual, and subungual BD.
■ Histopathologic features include full-thickness epidermal atypia with large, round cells and possible adnexal involvement.
■ Therapeutic options include surgical, topical, and ablative interventions.
■ Surgical treatment methods include excision and Mohs micrographic surgery, which permit histopathologic evaluation to exclude invasive SCC.
■ Topical therapy may be used in areas that are difficult to treat with other methods.
1867
20
Bowen disease (BD) is a distinct type of SCC in situ and was originally described in 1912 by John T. Bowen, a Boston dermatologist. It may affect both skin and mucous membranes and has the potential to progress to Bowen carcinoma, that is, an invasive SCC.
EPIDEMIOLOGY
EPIDEMIOLOGY
The exact incidence of BD in the United States is unknown. The incidence was estimated at 142 per 100,000 persons in Hawaii. BD usually occurs in adults, and is typically seen in individuals older than age 60 years. It affects both sexes with a preponderance in men.35 BD mostly affects sun-exposed areas, such as head and neck, as well as the upper and lower limbs. Men are more likely to have BD on the balding scalp, ear, and anterior trunk. In contrast, women commonly have BD on the cheeks and lower legs. Immunocompromised patients are more likely to develop BD at a younger age. It also affects more often the trunk, limbs, and neck, and recurrence rates are higher compared to immunocompetent patients.35
A
1868
C
CLINICAL FEATURES
CLINICAL FEATURES
BD lesions grow slowly and may be accompanied by pruritus, but are usually asymptomatic. Lesions typically present as erythematous plaques with irregular, clearly demarcated borders. The surface may be scaling, crusting, or hyperkeratotic (Fig. 110-9A). Over time, lesions may grow in size and measure up to several centimeters. The flat plaque may transform to a nodular or verrucous form. BD usually appears pink or reddish, whereas crusty or hyperkeratotic lesions may take a gray or brownish color. In very few cases, lesions are pigmented. Lesions of BD are usually solitary, but may be multiple in up to 20% of individuals. Sites of predilection include sun-exposed areas such as the head and neck and lower legs, although any site of the body may be affected. There are a few clinical variants of BD. In the periungual region BD may appear as an erythematous, scaly, thin plaque around the cuticular margin or as a verrucous plaque. It may lead to nail discoloration, onycholysis, or destruction of the nail plate (see Fig. 110-9B). In intertriginous areas, BD can present as an oozing,
B
erythematous, or pigmented patch or plaque. BD of the mucosal surfaces may appear as verrucous or polypoid papules and plaques, erythroplakia, or a velvety erythematous plaque. These variants are discussed in the sections on precancerous lesions of the oral cavity (see section “Potentially Malignant Disorders of the Oral Cavity,”) and the lower anogenital tract (see section “Precancerous Lesions of the Lower Anogenital Tract”), respectively.
ETIOLOGY AND PATHOGENESIS
ETIOLOGY AND
PATHOGENESIS
The most important etiologic factors for the development of BD include a long history of significant UV exposure and infection with HPV. BD has been described with increased frequency in patients undergoing psoralen plus UVA therapy. In contrast, it is rarely seen in stronger-pigmented individuals. Up to 30% of extragenital BD lesions have been found to harbor HPV DNA. Several HPV subtypes, such as HPV types 16, 18, 31, 34, 35, 54, 58, 61, 62, and 73 have been detected in BD lesions.36 Infection with high-risk HPV subtypes such as HPV 16 may be responsible for BD lesions on hands or fingers after anodigital infection in patients that simultaneously have anal and genital lesions. However, the prevalence of HPV-associated BD lesions is higher on sun-protected than on sunexposed body areas.37 Organ transplant recipients, HIV patients and other patients with long-term immunosuppression are at higher risk of developing BD. Other etiologic factors include arsenic exposure and ionizing radiation.
DIAGNOSIS
DIAGNOSIS
The clinical picture together with the typical history of a slowly growing, mostly asymptomatic lesion that remains resistant to topical corticosteroid treatment is highly suspicious for BD. However, final diagnosis requires biopsy and histologic examination. On a histologic level, BD lesions display full-thickness epidermal atypia with loss of the stratified epidermal architecture that is clearly demarcated from the surrounding physiologic structures (see Fig. 110-9C). Abnormal mitoses, acanthosis, and hyperkeratosis are further characteristics. Toward the upper epidermal layers parakeratosis is usually present. The degree of cytologic atypia may be variable. Typical are hyperchromatic, pleomorphic, and enlarged nuclei. The cells show a pale staining and eosinophilic cytoplasm. Vacuoles may be present within the keratinocytes. Atypical cells can be seen throughout the epidermal thickness alongside with mitotic figures and apoptotic cells. Intraepidermal portions of adnexal structures, such as the pilosebaceous units, may be affected
20
as well.14 As the basement membrane remains intact, atypia does not affect subepidermal structures. The upper dermis is usually infiltrated by numerous inflammatory cells, including lymphocytes, plasma cells, and histiocytes. Several histopathologic subtypes, such as psoriasiform, atrophic, acantholytic, and epidermolytic BD can be distinguished. Psoriasiform BD displays parakeratosis and marked acanthosis with broad, sometimes fused, epidermal rete ridges. Atrophic BD is characterized by a thinned epidermis. Acantholytic BD shows acantholysis in the epidermis. Epidermolytic BD has changes of incidental epidermolytic hyperkeratosis present. The phenomenon of intraepidermal epithelioma of Borst-Jadassohn—namely, nesting of the atypical cells within the epidermis, or so-called pagetoid BD—can also be seen. Furthermore, verrucoushyperkeratotic and papillomatous variants have been described.
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Clinically and histologically, BD may be difficult to distinguish from other dermatoses (Tables 110-4 and 110-5).
■Erythematous Bowen disease
■Erythematous Bowen disease
■Superficial basal cell carcinoma
■Superficial basal cell carcinoma
■Dermatitis, eczema
■Dermatitis, eczema
■Psoriasis
■Psoriasis
■Seborrheic dermatitis
■Seborrheic dermatitis
■Lichen planus
■Lichen planus
■Benign lichenoid keratosis
■Benign lichenoid keratosis
■Irritated or inflamed seborrheic keratosis
■Irritated or inflamed seborrheic keratosis
■Actinic keratosis
■Actinic keratosis
■Squamous cell carcinoma
■Squamous cell carcinoma
■Amelanotic melanoma
■Amelanotic melanoma
■Hyperkeratotic Bowen disease
■Hyperkeratotic Bowen disease
■Verruca vulgaris
■Verruca vulgaris
■Seborrheic keratosis
■Seborrheic keratosis
■Discoid lupus erythematosus
■Discoid lupus erythematosus
■Hypertrophic lichen planus
■Hypertrophic lichen planus
■Squamous cell carcinoma
■Squamous cell carcinoma
■Pigmented Bowen disease
■Pigmented Bowen disease
■Melanoma
■Melanoma
■Bowenoid papulosis
■Bowenoid papulosis
■Intertriginous Bowen disease
■Intertriginous Bowen disease
■Inverse psoriasis
■Inverse psoriasis
■Seborrheic dermatitis
■Seborrheic dermatitis
■Candidiasis
■Candidiasis
■Paget disease
■Paget disease
■Hailey-Hailey disease
■Hailey-Hailey disease
■Subungual or periungual Bowen disease
■Subungual or periungual Bowen disease
■Nail dystrophy
■Nail dystrophy
■Onychomycosis
■Onychomycosis
■Squamous cell carcinoma
■Squamous cell carcinoma
1869
■Amelanotic melanoma
■Amelanotic melanoma
20
■Paget disease
■Paget disease
■Pagetoid melanoma in situ
■Pagetoid melanoma in situ
■Intraepidermal eccrine carcinoma
■Intraepidermal eccrine carcinoma
■Intraepidermal Merkel cell carcinoma
■Intraepidermal Merkel cell carcinoma
■Intraepidermal sebaceous carcinoma
■Intraepidermal sebaceous carcinoma
■Bowenoid papulosis
■Bowenoid papulosis
■Hidroacanthoma simplex
■Hidroacanthoma simplex
■Podophyllin-induced changes in a wart
■Podophyllin-induced changes in a wart
CLINICAL DIFFERENTIAL DIAGNOSIS
Superficial basal cell carcinoma may mimic BD but can be distinguished by its elevated, subtle and translucent border. Patches of psoriasis, atopic dermatitis or lichen planus are typically accompanied by itching and located on their sites of predilection together with other lesions. In addition, they usually respond to topical corticosteroid therapy. Hyperkeratotic or verrucous lesions of BD can be misinterpreted as viral warts, seborrheic keratosis, and SCC. For both pigmented and unpigmented BD lesions, it is important to consider melanoma and amelanotic melanoma as differential diagnoses, respectively. Because of their very similar histologic picture, the clinical setting is crucial in differentiating BD from sexually transmitted bowenoid papulosis.
HISTOPATHOLOGIC DIFFERENTIAL DIAGNOSIS
BD may be confused with (extramammary) Paget disease. Both entities show atypical cells with pleomorphic, hyperchromatic nucleus, clear cytoplasm, and mitotic figures. While BD affects the full-thickness of the epidermis, Paget cells typically form nest-like or glandular-like patterns with a central lumen that are most abundant in the basal layers. Immunohistochemistry is essential for diagnosis, as Paget cells stain positive for carcinoembryonic antigen, mucin, Alcian blue, aldehyde fuchsin, and periodic acid-Schiff and are diastase resistant. In addition, unlike BD, Paget disease overexpresses low-weight cytokeratins, such as cytokeratin 7, and gross cystic disease fluid protein 15 (GCDFP-15).38,39
Similar to BD, AK type III (bowenoid AK) displays cell atypia throughout the entire thickness of the epidermis. In contrast to BD, they do not have a clear border, but show a diffuse transition into the surrounding epidermis. In addition, mitotic figures are less prominent. Finally, lumican, a small leucine-rich proteoglycan, is expressed in most BD lesions, but not in AK.40
In hidroacanthoma simplex, Lumican staining is also observed, but atypical mitoses cannot be seen.15
Pagetoid melanoma in situ can be difficult at times to distinguish histopathologically from BD. In BD, the intercellular desmosomal bridges should be identifiable between the atypical keratinocytes. Additionally,
1870
melanocyte-specific immunoperoxidase staining gives positive results in melanoma cells, but negative results in BD and Paget disease cells. The other rare pagetoid neoplasms are usually recognizable, but erroneous diagnoses can be made by the unwary. Bowenoid papulosis may lack the full-thickness epidermal atypia present in BD, but the clinical setting is paramount. Podophyllin applied topically to skin lesions induces metaphase arrest, leading to bizarre keratinocyte formation, architectural disturbance, vacuolation, and sometimes a pattern of pseudoepitheliomatous hyperplasia that can be mistaken for BD. These changes typically resolve after a few days to a week.
CLINICAL COURSE AND PROGNOSIS
CLINICAL COURSE AND
PROGNOSIS
In general, recurrence of BD is rare and estimated to be approximately 6% within 5 years after sufficient treatment. The theory that persistent BD within the deep portion of the follicle is mainly responsible for recurrence could not be confirmed.14 In fact, recurrent BD may be more likely caused by subclinical lateral spread, as excision with narrower lateral margin is associated with a higher risk of recurrence.16
The overall risk that untreated BD will progress to invasive carcinoma is estimated at approximately 5%. Immunocompromised individuals, such as organ transplant recipients, are at particular risk of recurrence, multiple BD lesions and transformation into invasive SCC.7,35
Once BD occurs, the risk of developing subsequent nonmelanoma skin cancer is particularly higher. There is no evidence, however, that BD is associated with a higher risk for internal malignancies. One exception is in cases of BD related to previous arsenic exposure, where the occurrence of an internal malignancy is possible. Also, BD involving the vulvar region in females and the perianal region in males may be associated with an increased risk of uterine, cervical, vaginal, and anal cancer, most likely as a consequence of HPV infection.36
TREATMENT
TREATMENT
There are various treatment approaches for BD. Such therapies can be divided into 3 main categories: surgical or destructive therapies, topical therapies, and radiation therapy (Table 110-6). The evidence on efficacy and safety is strongly limited and mostly restricted to PDT.17 However, this does not necessarily imply that other treatments lack efficacy. The choice on which treatment is best rather depends on several individual aspects, such as availability, patient or clinician’s preference, affected body area, and treatment costs. Surgical and destructive therapies include excision, Mohs micrographic surgery, curettage with or without electrosurgery, chemoablation with trichloroacetic acid, and cryosurgery. These
ADVANTAGE DISADVANTAGE
Surgical and Destructive Therapies
■Excision
■Histopathologic assessment (not for cryosurgery)
■Surgery-related complications
■Mohs micrographic surgery
■Scarring
■Curettage with or without electrosurgery
■Short treatment duration
■Cryosurgery: hypopigmentation, blister formation
■Cryosurgery
Topical Therapies
■5-Fluorouracil
■Application by the patient
■Long treatment duration
■Cosmetic outcome
■Local adverse events (eg, erythema, edema, erosion)
■No need for local anesthesia
■Toxic for eyes
Nonsurgical Ablative Therapies
■Photodynamic therapy (PDT)
■Cosmetic outcome (PDT)
■Local adverse events
■Photodynamic
■Cosmetic
■Local adverse
therapy (PDT)
outcome (PDT)
events
■Laser ablation
■Dyspigmentation
■Laser ablation
■Dyspigmenta-
■Chemoablation (trichloroacetic acid)
■Chemoablation
tion
■Chronic radiation dermatitis
■Chronic radia-
(trichloroacetic acid)
■Radiation therapy
■Radiation therapy
tion dermatitis
interventions are widely available and relatively cheap, and surgical approaches permit histopathologic evaluation. They are simple, rapid, and suitable for small BD lesions on easily accessible body areas. In particular for BD affecting the periungual region, local excision or Mohs micrographic surgery are commonly used. The most preferred topical therapies are 5-FU and 5% imiquimod cream, but others, such as ingenol mebutate, have been tried as well.18 Like surgical interventions, they are effective and widely available and therefore suitable for the outpatient setting. In addition, they can be used in individuals who refuse surgery, have significant comorbidities or impaired healing capability. Nonsurgical ablative therapies include PDT, laser ablation, and radiation therapy. There is good evidence for the use of PDT with MAL and ALA. One major advantage of PDT is an excellent cosmetic outcome. Combination therapies using PDT, CO2-laser, surgery, imiquimod 5% cream, and radiation have been described.19,41,42 If previous nonsurgical therapies have failed, BD warrants surgical intervention to exclude invasiveness and involvement of large surface areas.
VIRAL-ASSOCIATED EPITHELIAL PRECANCEROUS LESIONS
It has been suggested that some epithelial precancerous lesions are associated with HPV infection. HPVs are
20
PRECANCEROUS LESION ASSOCIATED HUMAN PAPILLOMAVIRUS TYPESa
Bowenoid papulosis (BP) 16, 18, 31-35, 39, 42, 48, 51-54
Epidermodysplasia verruciformis (EV) 2, 3, 5, 8, 9, 12, 14, 15, 17, 19, 25, 26, 38, 47, 50
Anal and perianal intraepithelial lesions (AIN, PaIN) 16, 18, 31, 33
Vulvar intraepithelial lesions (VIN) 16, 18, 31, 33
Penile intraepithelial lesions (PIN) 16, 18, 31, 33
Digital/periungual Bowen disease 16
16
Digital/periungual Bowen
disease
aThe most common associations are highlighted in bold.
double-stranded DNA viruses belonging to the Papillomaviridae family. More than 100 different types have been identified so far. According to their oncogenic potential, one distinguishes high-risk types from low-risk types. They can further be subdivided according to their tissue tropism into cutaneous and mucosal categories. Chapter 167 discusses HPV infections and HPV-associated diseases in more detail. The conditions bowenoid papulosis (BP), epidermodysplasia verruciformis (EV), and precancerous lesions of the lower anogenital tract (anal intraepithelial neoplasia [AIN], perianal intraepithelial neoplasia [PaIN], VIN, penile intraepithelial neoplasia [PIN]) are reviewed here (Table 110-7).
BOWENOID PAPULOSIS
BOWENOID PAPULOSIS
AT-A-GLANCE
■ Synonyms: Bowenoid papulosis (BP) of the genitalia, pigmented penile papules with carcinoma in situ changes, genital keratinocytic dysplasia, penile carcinoma in situ associated with human papillomavirus (HPV) infection.
■ BP is a precancerous condition of the genitalia caused by infection with high-risk HPV, most commonly with types 16, 18, and 33.
■ BP most commonly affects young to middle-aged males.
■ BP typically presents with multiple red to brownish flat papules on the penis or vulva.
■ BP rarely transforms into Bowen disease or invasive squamous cell carcinoma.
■ Treatment options include topical imiquimod, curettage, excision, and laser vaporization.
■ Vaccination may help to reduce the prevalence of BP among young adults.
1871
20
Genital lesions that histopathologically resembled SCC in situ were first described by Lloyd in 1970 as multicentric pigmented BD of the groin. In 1977, Kopf and Bart described multiple bowenoid papules of the penis, which were thereafte referred to as BP. Its association with high-risk HPV, most commonly with HPV types 16 and 18, was discovered only later. To date, numerous other mucosal HPV types have been associated with the condition, including types 31 to 35, 39, 42, 48, and 51 to 54. BP typically presents with multiple flat verrucous papules and plaques with a red-to-brownish color (Fig. 110-10). It is most common among young to middle-aged sexually active individuals with a male predominance. Lesions are multiple, pigmented. and typically located on the glans penis, prepuce, and penis shaft in males, and around the labia minora and majora in females. Depending on sexual practices lesions may be found in the perineal and anal area. Involvement of other sites such as oral cavity, neck, and periungual area is rarely seen. BP lesions may be confused with genital warts, lichen planus, condylomata acuminata, erythroplasia, molluscum contagiosum, and seborrheic keratoses. The multiplicity of the lesions is an important distinctive feature of BP compared to BD. Patients often report condylomata acuminata in their history. Histopathologically, BP is characterized by the presence of SCC in situ–like changes. The epidermis is usually hyperplastic and shows acanthosis, hyperorthokeratosis, and focal parakeratosis. Keratinocytes show signs of cellular atypia and disordered maturation. Dyskeratotic and pyknotic keratinocytes with scattered mitotic figures are commonly seen. HPV infection and identification of high-risk types can be achieved with polymerase chain reaction from lesional material. BP is perceived as transitional state between genital warts and in situ SCC. It has a variable, but mostly benign, clinical course, ranging from spontaneous regression to persistence of lesions to, rarely,
1872
transformation into BD and invasive SCC. It is estimated that the risk of malignant transformation is rather low, ranging from less than 1% to 2.6%. BP is highly contagious and patients with BP and their sexual partners should be followed and examined periodically, because of the increased risk of developing SCC or cervical or vulvar neoplasia. Patients with persistent disease should probably undergo testing for altered immune status. Despite the low risk for malignant transformation, treatment of BP is recommended. It typically responds well to local therapy, although recurrences are common. Therapeutic options include local destructive measures such as curettage with or without electrosurgery, CO2-laser, neodymium:YAG laser, cryosurgery, and excision. Topical tretinoin, topical 5-FU, and topical cidofovir have been used in anecdotally reported cases with mixed results. Imiquimod 5% cream 3 times per week for up to 12 weeks showed high lesion clearance rates in several studies and is a valid treatment option in clinical practice. Also, the efficacy of PDT in the treatment of BP has been demonstrated. Whether HPV-specific vaccination for types 6, 11, 16, and 18 can help reduce the prevalence and incidence of BP in which HPV types 16 and 18 have frequently been identified is currently under investigation.
EPIDERMODYSPLASIA VERRUCIFORMIS
EPIDERMODYSPLASIA
VERRUCIFORMIS
AT-A-GLANCE
■ Epidermodysplasia verruciformis (EV) is an inherited skin condition with a high local susceptibility to infection with human papillomavirus (HPV), most commonly with HPV types 5 and 8.
■ Sporadic and familial cases of EV may occur.
■ Loss-of-function mutations of the genes EVER1 and EVER2 are associated with EV.
■ The clinical presentation is with either widespread, flat, wart-like papules and plaques, or hypopigmented scaly patches in childhood.
■ Patients with EV are at high risk to develop actinic keratosis, Bowen disease, or invasive squamous cell carcinoma in the further course of the disease.
■ Late-onset EV may occur in patients with cellular immunodeficiency (HIV, organ transplant recipients).
■ Sun avoidance, sun-protective measures, regular dermatologic follow up, and screening of family members for the disease are recommended.
EV is a rare inherited skin condition that is characterized by a high susceptibility to infection with some types of HPV, in particular types 5 and 8 (termed
A
20
B
EV-HPV). In addition to the host genetic background and HPV infection, UV exposure and immunosuppression contribute to the pathogenesis of the disease.43
The exact prevalence of EV is not known. Sporadic and familial cases of EV have been reported in the literature. It is probably inherited as an autosomal recessive or X-chromosomal recessive disorder with 2 gene loci: EV1 (located on chromosome 17q25.3) and EV2 (located on chromosome 2p21-24). The genes TMC6 (EVER1) and TMC8 (EVER2) have been identified within the locus EV1.44,45 Even though loss-of-function mutations of both genes have been linked with EV, approximately 25% of all patients do not show mutations in either gene. The EVER genes belong to a transmembrane-like channel protein family and are thought to be involved in zinc homeostasis of the endoplasmic reticulum and transcriptional regulation within the nucleus of keratinocytes. Cells deficient for EVER1 or EVER2 are unable to prevent the replication of certain HPV types, mostly beta-HPV. Thus, EV patients develop a selective immunodeficiency for HPV infection. Most commonly, HPV 5 and HPV 8 can be found in EV, but also HPV types 9, 12, 14, 15, 17, 19, 25, 36, 38, 47, and 50 have been reported. Patients with EV develop skin lesions early in life as infection with HPV typically occurs during infancy. Skin findings comprise 2 different morphologies. First, numerous thin, pink, flat-topped papules and plaques that resemble flat warts (verrucae planae) may be seen. Therefore, these papules are sometimes referred to as EV-plane warts. Sites of predilection for these warts are knees, elbows, and trunk. Second, patients can present with widespread scaly, erythematous, or hypopigmented macules and flat papules that appear similar to tinea versicolor (Fig. 110-11). The mucosal membranes are usually not affected. Histopathologically, the EV-plane warts share features with plane warts not associated with EV. Dyskeratosis and pyknosis are observed more commonly in EV. However, the diagnosis is made based on a combination of the clinical image, histopathologic findings, plus viral and genetic testing. The clinical course of EV is not entirely known and variable. It is estimated that more than 60% of patients
affected by EV develop cutaneous malignancies in the wart-like lesions, most often in the fourth to fifth decades of life and usually on sun-exposed or acral areas of the skin. Patients may develop AK, BD, and invasive SCC. Some patients with immunodeficiency, such as organ transplant recipients and HIV-positive patients, can have a late-onset of EV (called acquired EV). Thus, older patients suspected of having EV should also be tested for HIV and other conditions with impaired cell-mediated immunity. No specific or successful treatments exist for EV lesions. Mixed results have been achieved with topical 5% imiquimod cream and retinoids. Patients with EV should undergo a regular and thorough follow up to detect precancerous and invasive lesions as early as possible. UV radiation should be avoided because it increases the risk of malignant transformation. Single EV-plane warts can be treated successfully with excision, curettage, cryosurgery, or ablative lasers.
PRECANCEROUS LESIONS OF THE LOWER ANOGENITAL TRACT
PRECANCEROUS
LESIONS OF THE LOWER
ANOGENITAL TRACT
ANAL INTRAEPITHELIAL NEOPLASIA
AT-A-GLANCE
■ Synonyms: anal squamous intraepithelial neoplasia or anal dysplasia.
■ Anal intraepithelial neoplasia (AIN) is associated with high-grade human papillomavirus (HPV) types, most commonly with types 16, 18, 31, and 33.
■ AIN shows biologic and clinical analogy to cervical intraepithelial neoplasia.
1873
(Continued)
20
AT-A-GLANCE (Continued)
■ Major risk factors for AIN are HPV infection, high-risk sexual behavior (anal intercourse), HIV infection with low levels of CD4+ T cells, smoking, immunosuppression, a history of genital warts, and a history of cervical cancer in females.
■ AIN is commonly localized within the transitional zone of squamous epithelium of the anus and columnar epithelium of the rectum, which is highly susceptible to HPV infection (dentate line).
■ AIN is usually asymptomatic, but may occasionally cause local symptoms like pruritus, pain, bleeding, tenesmus, or rectal discharge.
■ The diagnosis of AIN is made by anal cytology, high-resolution anoscopy, and histopathologic examination of biopsy specimens.
PERIANAL INTRAEPITHELIAL NEOPLASIA
AT-A-GLANCE
■ Synonyms: genital Bowen disease (GBD).
■ Perianal intraepithelial neoplasia (PaIN) is less likely than AIN to be associated with human papillomavirus than anal intraepithelial neoplasia.
■ Only 5% of patients with PaIN may progress to invasive squamous cell carcinoma.
VULVAR INTRAEPITHELIAL NEOPLASIA
AT-A-GLANCE
AT A GLANCE
■ The term vulvar intraepithelial neoplasia (VIN) should be restricted to high-grade precancerous lesions of the vulva (formerly VIN 2 and VIN 3) that may progress to vulvar squamous cell carcinoma.
■ VIN grade 1 (formerly VIN 1) is similar to vulvar condyloma acuminatum with a low oncogenic potential and not considered VIN in the nomenclature of the Vulvar Oncology Subcommittee of the International Society for the Study of Vulvar Diseases (ISSVD).
■ VIN is primarily a disease of younger, sexually active females (75% of all cases) with rising incidence and prevalence.
1874
■ AIN 1 is a low-grade squamous intraepithelial lesion (LSIL) with a low risk of progression to anal cancer.
■ AIN 2 and AIN 3 are precursor high-grade squamous intraepithelial lesions (HSILs) of anal squamous cell carcinoma and histopathologically display moderate and severe dysplasia, respectively.
■ It is currently under debate whether screening for AIN should be performed in high-risk populations.
■ HPV vaccination with a quadruple vaccine against HPV types 6, 11, 16, and 18 may reduce the incidence of AIN.
■ Patients with HSIL (AIN 2 or AIN 3) should receive treatment; treatment is optional for LSIL (AIN 1).
■ Therapy options include topical treatment with trichloroacetic acid, infrared coagulation, 5-FU, intraanal imiquimod, or electrocauterization.
■ PaIN may present with a variety of clinical patterns, including well-demarcated erythematous, or variably pigmented plaques.
■ Dermatologists play a role in high-risk patients by examining the perianal skin and clinically diagnosing PaIN.
■ Treatment options for PaIN include wide local excision, Mohs micrographic surgery, and various topical agents.
■ Three categories of VIN are distinguished: (a) usual type, (b) differentiated (simplex) type, and (c) unclassified type.
■ VIN usual type is associated with high-risk human papillomavirus (HPV) (types 16, 18, 31), occurs in younger premenopausal females, and presents with multifocal and multicentric lesions; in up to 50% of cases associations with cervical intraepithelial neoplasia can be found.
■ VIN differentiated type is less common than usual type and usually not associated with HPV; it affects postmenopausal females with a unifocal presentation and has a significant association with lichen sclerosus.
(Continued)
AT-A-GLANCE (Continued)
■ Risk factors for VIN (usual type) are smoking, sexual promiscuity, HPV infection, and immunosuppression.
■ The clinical presentation of VIN ranges from reddish patches to gray-white plaques and verrucous wartlike papules.
■ The differential diagnosis of VIN includes lichen sclerosus, lichen planus, condyloma acuminatum, and other vulvar neoplasias like SCC and melanoma.
■ VIN is asymptomatic in many cases, but may cause vulvodynia, vulvar pain and burning sensation, dysuria, or pruritus.
PENILE INTRAEPITHELIAL NEOPLASIA
AT-A-GLANCE
■ Penile intraepithelial neoplasia (PIN) is an umbrella term for precursor lesions of the male genital to penile squamous cell carcinoma (SCC).
■ Two clinical variants of PIN are the genital Bowen disease (GBD) and erythroplasia of Queyrat (EQ) (Fig. 110-12).
■ PIN and penile SCC mainly affect older, uncircumcised males.
■ Risk factors for PIN are poor genital hygiene, smegma retention, phimosis, chronic inflammatory and infectious conditions of the penis, lichen sclerosus, lichen planus, immunosuppression (HIV infection, organ transplant recipients), smoking, and preceding psoralen plus ultraviolet A or ultraviolet exposure.
■ Approximately 40% to 45% of PIN cases are associated with HPV, mainly with high-risk types such as types 16, 18, 31, and 33; low-risk types 6 and 11 may be present in low-grade PIN.
■ PIN associated with HPV infection are supposedly more aggressive and may develop to warty and basaloid subtypes of penile SCC.
■ PIN without HPV infection is morphologically associated with the usual or differentiated type of penile SCC.
20
■ The diagnosis of VIN is made by physical examination, biopsy, and optionally colposcopy.
■ Treatment modalities include surgical excision and ablative laser therapy for single lesions, while topical treatment with 5-FU or imiquimod is more suited for multicentric VIN.
■ A diagnosis of VIN mandates referral to a gynecologist to look for synchronous vaginal and cervical intraepithelial neoplasia.
■ Quadrivalent HPV vaccination (HPV types 6, 11, 16,
18) may reduce the risk for VIN usual type in young females.
■ EQ is a common type of PIN usually associated with HPV 8 and HPV 16 infection; it presents as a well-demarcated, glistening, erythematous, velvety plaque or plaques on the mucosal surfaces of the penis (Fig. 110-12A).
■ The GBD variant of PIN is less common than the EQ variant; it presents as a well-demarcated, erythematous to variably pigmented plaque on the shaft of the penis (Fig. 110-12B).
■ Both variants have histopathologic features of SCC in situ; EQ shows prominent epithelial hypoplasia and plasma cells in the dermal infiltrate.
■ The EQ variant of PIN has a higher risk of progression to invasive SCC (∼30%) than the GBD variant (3% to 6%).
■ Treatment options include local excision, cryosurgery, ablative lasers (CO2-laser), imiquimod, or topical cidofovir.
■ Preventive measures comprise circumcision, proper hygiene, stopping smoking, and avoiding genital UV exposure.
■ It is currently under investigation if immunization of young males with HPV vaccines can reduce the risk of PIN; however, HPV-unrelated lesions are not affected by this approach.
1875
20
A
C
B
POTENTIALLY MALIGNANT DISORDERS OF THE ORAL CAVITY
In a World Health Organization (WHO) workshop held in 2005, the terminology, definitions, and classification of oral lesions with a predisposition to malignant transformation were discussed.46 The term potentially malignant was preferred over premalignant or precancerous. In addition, it was recommended that the traditional distinction between potentially malignant lesions and potentially malignant conditions be abandoned and that the term potentially malignant disorders
1876
be used instead. Here, the focus will be on oral leukoplakia and erythroplakia.
LEUKOPLAKIA
LEUKOPLAKIA
Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. Leukoplakia is the most common potential malignant lesion of the oral mucosa, with the potential to become oral SCC. It is in the same clinical spectrum of disease as oral erythroplakia, but
leukoplakia is more common and the likelihood of malignant transformation is lower.
AT-A-GLANCE
■ Leukoplakia is a clinical diagnosis of exclusion for a fixed white lesion in the oral cavity that does not resolve spontaneously.
■ Oral leukoplakia is the most common potentially malignant lesion of the oral mucosa, with the potential to become oral squamous cell carcinoma (SCC).
■ The prevalence is 0.2% to 3.4%.
■ Approximately 50% of oral SCCs are associated with potentially malignant lesions.
■ Leukoplakia and erythroplakia are markers for increased risk for additional oral or upper aerodigestive tract malignancies.
■ Risk factors for leukoplakia are the use of any tobacco product, alcohol abuse, history of previous or premalignant lesions, and infection with certain human papillomavirus subtypes.
■ No consensus exists on how best to treat leukoplakia.
EPIDEMIOLOGY
The prevalence of leukoplakia varies significantly by geographical region and demographic group. Estimates for global prevalence vary from 0.5% to 3.4%. Individuals 40 years of age and older are at higher risk. Males are affected more often than females with an estimated male-to-female ratio of 2:1. This may be explained by a higher exposure to certain risk factors. For instance, leukoplakia is 6 times more common among smokers than among nonsmokers.
CLINICAL FINDINGS
Leukoplakia is clinically divided into a homogeneous and nonhomogeneous form. Homogeneous leukoplakia has been defined as a mostly white, flat, uniform lesion. It may have shallow cracks and a smooth, wrinkled, or corrugated surface (Fig. 110-13). Nonhomogeneous leukoplakia is defined as a mostly white or white-reddish lesion (“erythroleukoplakia”) that may be irregular and flat, nodular, ulcerative, or verrucous. Nonhomogeneous leukoplakia has a significant higher risk of malignancy than does homogeneous leukoplakia. Proliferative verrucous leukoplakia represents a rare form, which is most often found in patients who do not use tobacco products. It has a high rate of malignant transformation and recurrence after treatment.
ETIOLOGY AND PATHOGENESIS
Etiologic factors for leukoplakia include chronic chemotoxic exposure, mechanical trauma, and HPV
20
infection. Tobacco is probably the strongest risk factor for the development of leukoplakia. It was shown that most patients with leukoplakia consumed tobacco, either as smoke or by chewing. In addition, tobacco-related white lesions of the oral mucosa may disappear once the tobacco use has been discontinued. The combination of tobacco use and alcohol consumption has a strong synergistic effect in the development of leukoplakia. However, alcohol consumption was also identified as an independent risk factor, regardless of beverage type or drinking pattern. Typical causes for chronic mechanical trauma of the oral mucosa are ill-fitting prosthesis, chronic cheek biting, and reduced dental status with poor oral hygiene. HPV represents another etiologic factor for leukoplakia. It was detected in up to 22% of leukoplakia lesions and its prevalence compared to normal mucosa is significantly higher. High-risk oncogenic subtypes, such as HPV types 16 and 18, were isolated more frequently than low-risk HPV (type 6 or type 11). For this reason, HPV is widely believed to be an independent risk factor in the development of leukoplakia, or at least an intensifier of other carcinogenic effects. However, the specific role of HPV in carcinogenesis remains controversial, as no correlation between mucosal dysplasia and HPV infection was found. Persons with a previous malignancy or premalignancy of the upper aerodigestive tract are at greater risk for the development of leukoplakia.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Leukoplakia is a clinical diagnosis. Whitish lesions in the oral mucosa that cannot be rubbed off are suspicious for leukoplakia. If causative agents, such as tobacco or mechanical irritation, are detected, it is recommended to eliminate these factors for a period of 2 to 6 weeks. If regression does not occur during this observational period, biopsy and histologic examination should be performed. If upon initial examination
1877
20
■Tobacco-associated lesion
■Tobacco-associated lesion
■Candida-associated lesion
■Candida-associated lesion
■Leukoedema
■Leukoedema
■Lichen planus
■Lichen planus
■Lupus erythematosus
■Lupus erythematosus
■Linea alba
■Linea alba
■Habitual cheek biting
■Habitual cheek biting
■Frictional lesion
■Frictional lesion
■Aspirin burn
■Aspirin burn
■Oral white sponge nevus
■Oral white sponge nevus
■Oral hairy leukoplakia
■Oral hairy leukoplakia
■Verrucous carcinoma
■Verrucous carcinoma
■Squamous cell carcinoma
■Squamous cell carcinoma
no causative agent can be identified, biopsy should be performed directly. This is particularly important for symptomatic leukoplakia. In this case, malignant transformation into invasive SCC should be ruled out.46 Further important differential diagnoses include Epstein-Barr virus–induced hairy leukoplakia in HIV patients, lichen planus, and lupus erythematosus, among others (Table 110-8).
HISTOPATHOLOGY
On a histologic level, characteristic findings are hyperkeratosis, epithelial hyperplasia, and dysplasia. The latter includes atypical mitosis, polymorphic cells, as well as hyperchromatic and polymorphic nuclei. Epithelial hyperplasia and hyperkeratosis give the lesion the characteristic whitish appearance. The degree of dysplasia varies from lesions showing only hyperkeratosis with no dysplasia toward lesions with moderate dysplasia and those with severe dysplasia resembling SCC in situ. There are different growing patterns, which include clinically flat, papillary endophytic and papillary exophytic, verrucous proliferation. Transformation into invasive SCC occurs as dysplastic cells break through the basement membrane.
CLINICAL COURSE AND PROGNOSIS
Once a definitive diagnosis of leukoplakia has been made, the risk of malignant transformation should be evaluated. The rate of all clinical subtypes of leukoplakia is estimated to be approximately 2% to 3% per year.46,47 Table 110-9 lists the numerous identified risk factors for malignant transformation. Of these factors, epithelial dysplasia and nonhomogeneous clinical subtype are the most important indicators for malignant transformation. However, it should be recognized that not all dysplastic lesions progress to malignancy.
1878
Main risk factors
Main risk factors
■Presence of epithelial dysplasia
■Presence of epithelial dysplasia
■Nonhomogeneous clinical subtype
■Nonhomogeneous clinical subtype
■Large size
■Large size
■Location on the tongue or the floor of the mouth Other risk factors
■Location on the tongue or the floor of the mouth Other risk factors
■Female gender
■Female gender
■Long duration of oral leukoplakia
■Long duration of oral leukoplakia
■Leukoplakia in nonsmokers
■Leukoplakia in nonsmokers
Adapted and modified from van der Waal.47,52
Some remain clinically unchanged and others may regress spontaneously or after elimination of the causative agent, such as cessation of smoking. In addition, malignant transformation may also occur in nondysplastic leukoplakia.
TREATMENT AND PREVENTION
There is a chance of spontaneous remission of leukoplakia. However, the risk of malignant transformation warrants treatment if remission does not occur within a short period of observation. In general, any possible causative agent or risk factor such as consumption of tobacco products, alcohol, bethel nuts, or chronic mechanical trauma should be omitted. There are numerous therapeutic approaches for leukoplakia, but evidence remains strongly limited and recurrence rates for all interventions are high. Usually, surgical excision is the first treatment of choice. In contrast to other therapies, surgery allows histologic workup and unexpected carcinomas may be identified.48 However, adequate surgical excision may be limited as field cancerization may be present and normal-appearing surrounding mucosa may harbor clones of cancer stigmatized cells. In the case of recurrence after surgical excision, cryotherapy or CO2-laser represent useful treatment options. Other therapies include PDT, herbal extracts, beta-carotene supplements, antiinflammatory drugs, and vitamin A, among others.49-51
Independent of the treatment, the patient should be followed closely.
ERYTHROPLAKIA
ERYTHROPLAKIA
Erythroplakia (or erythroplasia) is a clinical term used to describe a red macule or patch on a mucosal surface that cannot be categorized as any other known disease entity caused by inflammatory, vascular, or traumatic factors. It is commonly seen in association with leukoplakia, a condition termed erythroleukoplakia.
AT-A-GLANCE
■ Erythroplakia is a clinical diagnosis of exclusion for a persistent fixed red patch in the oral cavity.
■ It is the least common of all oral potentially malignant lesions but has the greatest potential to harbor or become oral squamous cell carcinoma.
■ Risk factors are use of tobacco products and alcohol consumption.
■ Early and effective treatment is important.
EPIDEMIOLOGY
Erythroplakia is rare and the least-frequent potentially malignant lesion in the oral cavity. The prevalence depends on the geographical area and varies between 0.02% and 0.83%. Erythroplakia mainly occurs in middle-aged individuals. Males are affected more often than females, which may be explained by a higher exposure to certain risk factors, such as tobacco consumption. Erythroplakia has been well described in the chutta smokers (reverse cigar smokers) of India.
CLINICAL FINDINGS
Erythroplakia usually presents as an asymptomatic, solitary, subtle, erythematous macule or patch. It is sharply demarcated from the surrounding pink mucosa, and its surface is most often smooth and homogeneous in color. However, some lesions may have a pebbled or stippled surface and feel soft and velvety on palpation. Induration is highly suspicious for transformation into invasive SCC. The most common areas in the oral cavity are the soft palate, the floor of the mouth, and the buccal mucosa. Most often it is less than 1.5 cm in its widest diameter, but lesions up to 4 cm in diameter have been described.
ETIOLOGY AND PATHOGENESIS
The underlying etiology of erythroplakia is unknown. Risk factors are equal to those of other potentially malignant lesions in the oral cavity: consumption of tobacco products, alcohol and chewing nuts that contain carcinogenic substances, such as areca nuts. Genetic analyses have shown a high mutation rate of the tumor-suppressor gene p53 in erythroplakia lesions, reflecting their high potential to malignant transformation.
DIAGNOSIS
Erythroplakia is a diagnosis of exclusion. Table 110-10 outlines differential diagnoses. On a histologic level, erythroplakia typically displays moderate to severe dysplasia. Frequently, SCC in situ and focal areas of invasive SCC are present.
20
■Erythematous candidiasis
■Erythematous candidiasis
■Atrophic lichen planus
■Atrophic lichen planus
■Lupus erythematosus
■Lupus erythematosus
■Pemphigus
■Pemphigus
■Cicatricial pemphigoid
■Cicatricial pemphigoid
■Kaposi sarcoma
■Kaposi sarcoma
■Chronic contact or allergic contact dermatitis
■Chronic contact or allergic contact dermatitis
■Chronic mechanical trauma
■Chronic mechanical trauma
■Thermal or mechanical injury
■Thermal or mechanical injury
■Squamous cell carcinoma
■Squamous cell carcinoma
■Amelanotic melanoma
■Amelanotic melanoma
CLINICAL COURSE AND PROGNOSIS
Of all potentially malignant lesions in the oral cavity, erythroplakia is considered to be the most dangerous and carries the greatest risk of progressing to or harboring invasive carcinoma. In erythroleukoplakia, the red patches are most prone for malignant transformation. After excision, lesions that exceed 80 mm2 have a significant higher risk of recurrence.
TREATMENT
The high potential for malignant transformation warrants early treatment. Surgery or excision with CO2- laser is the treatment of choice. Any risk factors, such as consumption of tobacco or alcohol, should be avoided.
ARSENICAL KERATOSES
AT-A-GLANCE
■ Arsenical keratoses (ArKs) result from chronic exposure to arsenic.
■ ArKs have the potential to become squamous cell carcinoma (SCC), although reliable estimates of progression rates are unknown.
■ Clinical appearance comprises punctuate, keratotic, yellow papules overlying pressure points on palms and soles.
■ Further arsenic-related skin diseases are superficial basal cell carcinoma, SCC, Bowen disease, and diffuse hyperpigmentation.
■ No standard recommendations for treatment exist and most lesions are followed clinically or treated symptomatically.
Arsenical keratoses (ArKs) result from chronic intake or intoxication with arsenic. Arsenic is a ubiquitous element that has no color, taste, or odor. It has the
1879
20
potential to cause characteristic acute and chronic symptoms in persons exposed to it. Arsenic exposures are typically obscure and medicinal, occupational, and environmental sources still exist. ArKs are considered precancerous lesions because they have the potential to progress into invasive SCC. ArKs are localized most commonly on the palms and soles. Clinically, they appear as gray-to-yellow keratotic papules. If lesions are large, they may acquire a verruciform look (Fig. 110-14). Further signs of a chronic exposure to arsenic are diffuse hyperpigmentation and the presence of superficial basal cell carcinoma or BD. Histopathologically, ArKs resemble hypertrophic AKs with a more cellular atypia and prominent vacuolization of keratinocytes. The diagnosis may be difficult. Taking a thorough history is an important clue and the first step toward the correct diagnosis. ArKs may be confused with vulgar warts, hypertrophic lichen planus, keratosis palmaris, and plantaris dissipata or diffusa, or AKs in sun-exposed areas. Although ArKs and arsenic-induced skin disorders tend to persist for many years, progression to invasive SCC is believed to be a relatively rare event. However, reliable estimates for progression rates are lacking as a consequence of the rarity of the disease. Some evidence exists that invasive SCCs that arise from ArKs are more locally aggressive and have a greater chance of metastasis than SCCs arising from AKs. If ArKs are suspected, a thorough skin examination and physical examination are obligatory. The sources of exposure to arsenic should be identified and discontinued. The exact incidence of internal malignancies associated with chronic arsenism is unknown, so there is no standard protocol for the evaluation of potential internal malignancies. Exhaustive evaluations to detect such malignancies have not been recommended. Biannual detailed history taking and physical examination, yearly chest radiography, and selective testing when clinically indicated are probably reasonable recommendations. Single lesions can be treated with surgical excision, cryosurgery, or curettage. Ablative resurfacing with the
1880
CO2-laser and Er:YAG-laser were successfully applied in some cases. If diffuse hyperkeratosis or disseminated ArK lesions are present, topical and systemic retinoids are a valuable option, although lesion clearance is generally lower compared to treatment of AKs. Patients with verified ArKs should be followed-up and monitored regularly, possibly every 6 to 12 months.
THERMAL KERATOSES
AT-A-GLANCE
■ Precancerous lesions that result from long-term exposure to infrared radiation; can progress to squamous cell carcinoma (SCC).
■ Sources of infrared radiation include open fires, railway engines, wood-burning stoves, heating pads and blankets, and laptop computers.
■ Precursor lesion is erythema ab igne; biopsy should be performed on any hyperkeratotic papule or plaque within such a patch.
■ Risk of progression of thermal keratosis to SCC is unknown.
HYDROCARBON KERATOSES
AT-A-GLANCE
■ Synonyms: pitch keratoses, tar keratoses, tar warts.
■ Precancerous lesions resulting from prolonged exposure to tar.
■ Tar contains highly cancerogenic polycyclic aromatic hydrocarbons such as benzpyrene, dibenzanthracene, or methylcholanthrene.
■ May be present in patients with occupational exposure to tar; occupations at risk include tar distiller, shale extractor, roofer, asphalt worker, road paver, highway maintenance worker, brick mason, diesel engineer, and chimney sweep.
■ Ultraviolet exposure is a cofactor in the establishment of tar keratosis.
■ Hydrocarbon keratosis can progress to squamous cell carcinoma (SCC), but the rate of progression and risk are unknown.
■ Latency periods between exposure and development of hydrocarbon keratosis or SCC range from 2.5 years to 45 years.
■ Lesions typically present as hyperkeratotic papules with a verruciform surface; sites of predilection are face, neck, forearms, and scrotal skin.
(Continued)
AT-A-GLANCE (Continued)
Continued
AT A GLANCE (
)
■ Other skin findings include patchy hyperpigmentation, acne, and telangiectasias.
■ Therapeutic options include excision, curettage, and ablative lasers (CO2, Er:YAG).
CHRONIC RADIATION KERATOSES
AT-A-GLANCE
■ Chronic radiation keratoses are precancerous lesions that may arise at irradiated sites years after such exposure and may progress to squamous cell carcinoma.
■ Ionizing radiation sources include X-rays, grenz rays, and contaminated gold rings.
■ Common sites are the palms, soles, and mucosal surfaces.
■ They most commonly present as hyperkeratotic papules or plaques within areas of chronic radiation dermatitis and occasionally on clinically normal skin.
■ Latency for the development of lesions can be up to 50 years after exposure.
■ Patients with ionizing radiation exposure and chronic radiation keratoses are also at risk for internal malignancies.
CHRONIC SCAR KERATOSES
AT-A-GLANCE
AT A GLANCE
■ Synonym: cicatrix keratoses.
■ Chronic scar keratoses are precancerous lesions that arise in longstanding scars from various causes.
■ Common conditions comprise burn scars, chronic wounds, sinuses, and leg ulcers.
■ Approximately 2% of burn scars will undergo malignant changes.
■ Marjolin ulcer is an umbrella term covering malignant changes within a scar from any cause.
■ Acute Marjolin ulcer develops within 1 year of the time of injury; chronic Marjolin ulcer develops more than 1 year after an injury.
20
■ Most invasive carcinomas are squamous cell carcinomas (SCCs), but basal cell carcinomas, melanomas, sarcomas, and malignant fibrous histiocytomas also have been described.
■ SCCs deriving from scar keratoses show an aggressive growth pattern with a high propensity to metastasize.
■ Sites of predilection are the extremities and overlying joints.
■ Any persistent lesion, erosion, or ulceration within a scar requires biopsy.
■ Prevention includes wound care, early skin grafting, avoidance of contractures, and early excision of any tissue showing degenerative changes.
ACKNOWLEDGMENTS
We thank Saskia A. Graf for her support with Fig. 110-1 and Karynne O. Duncan, John K. Geisse, and David J. Leffell who are the authors of the previous version of this chapter.

Figure 110-1 Multiple scaly and erythematous plaques on the dorsal hands of a 71-year-old male patient with a history of significant ultraviolet exposure. The lesions were grade II to grade III actinic keratoses.

Figure 110-2 Mild actinic keratoses on the face of a fairskinned woman (grade I). The lesions appear as erythematous patches with a rough texture on palpation. Note other signs of actinic skin damage such as perioral wrinkling and the presence of solar lentigines.

Figure 110-3 Field cancerization. There are several illdefined erythematous and scaly plaques, crusts, and ulcerations affecting a large area (“field”) of the balding scalp. Further alterations, such as mottled hypopigmentation and hyperpigmentation, are present and indicate actinic damage.

Figure 110-4 A, Multiple well-defined hypertrophic actinic keratoses on the decollete of a middle-aged female. B, A higher magnification reveals the rough and hyperkeratotic texture of some lesions.
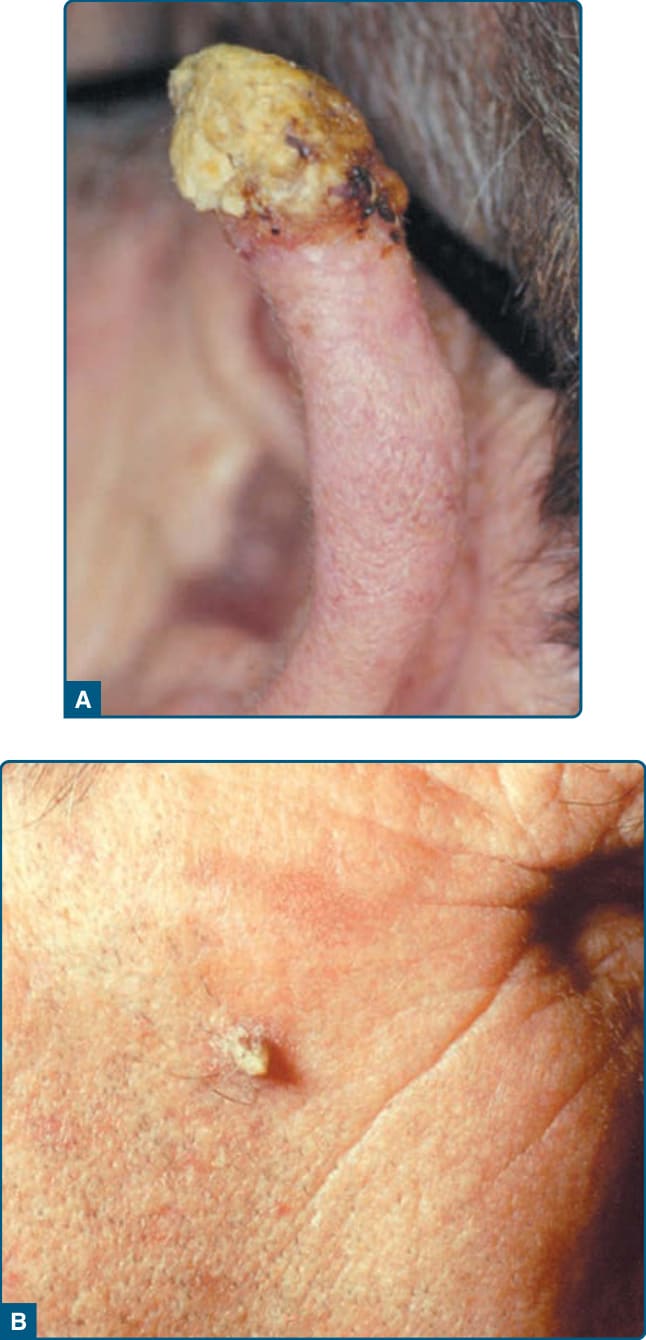
Figure 110-5 A, Cutaneous horn of the ear. Only biopsy will confirm whether this is an actinic keratosis or a squamous cell carcinoma. B, Cutaneous horn of the cheek.

Figure 110-6 Actinic cheilitis. Reddish to yellow crusts and erosions on the lower lip are typical features of actinic damage along the vermilion border. The patient complained of a persistent dryness of the lip.
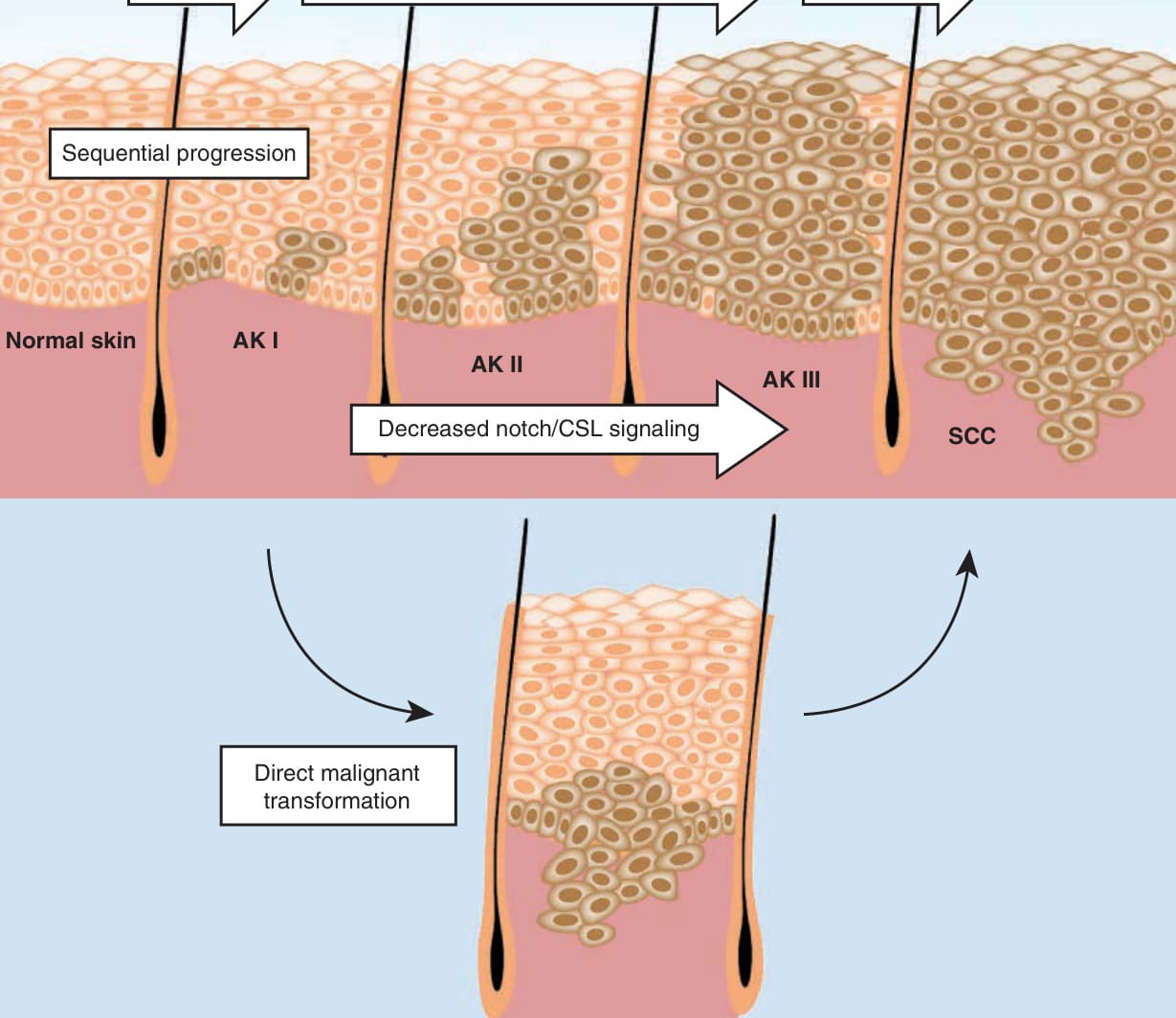
Figure 110-7 Schematic overview on the etiology and pathogenesis of actinic keratosis (AK) development. The most important etiologic factors are fair skin, ultraviolet (UV) radiation, immunosuppression, human papillomavirus (HPV) infection or exposure to tar, arsenic, and X-rays. The classic pathway (upper panel) assumes a stepwise progression from early lesions confined to the basal layers of the epidermis (AK I) toward intermediate (AK II) and late AK lesions (AK III), which may progress to invasive squamous cell carcinoma (SCC). A common and early molecular event is loss or inactivation of the tumor-suppressor gene p53. Recent evidence suggests decreased Notch signaling in underlying dermis may contribute to the formation and progression of AK. The alternative pathway (lower panel) assumes that any AK, including low-grade lesions, bears the potential to directly progress to invasive SCC. Abbreviation: As, arsenic; HPV, human papillomavirus.
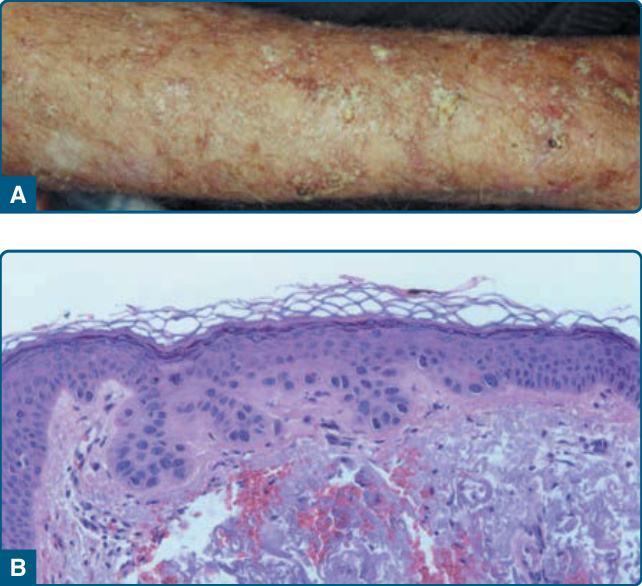
Figure 110-8 A, Severe solar damage of the dorsal arm demonstrating hypertrophic actinic keratoses. B, Histopathologic preparation of actinic keratosis demonstrates atypical cells along the basal layer with sparing of adnexal epithelium and a sparse lymphocytic infiltrate with marked actinic elastosis in the upper dermis underlying the lesion.
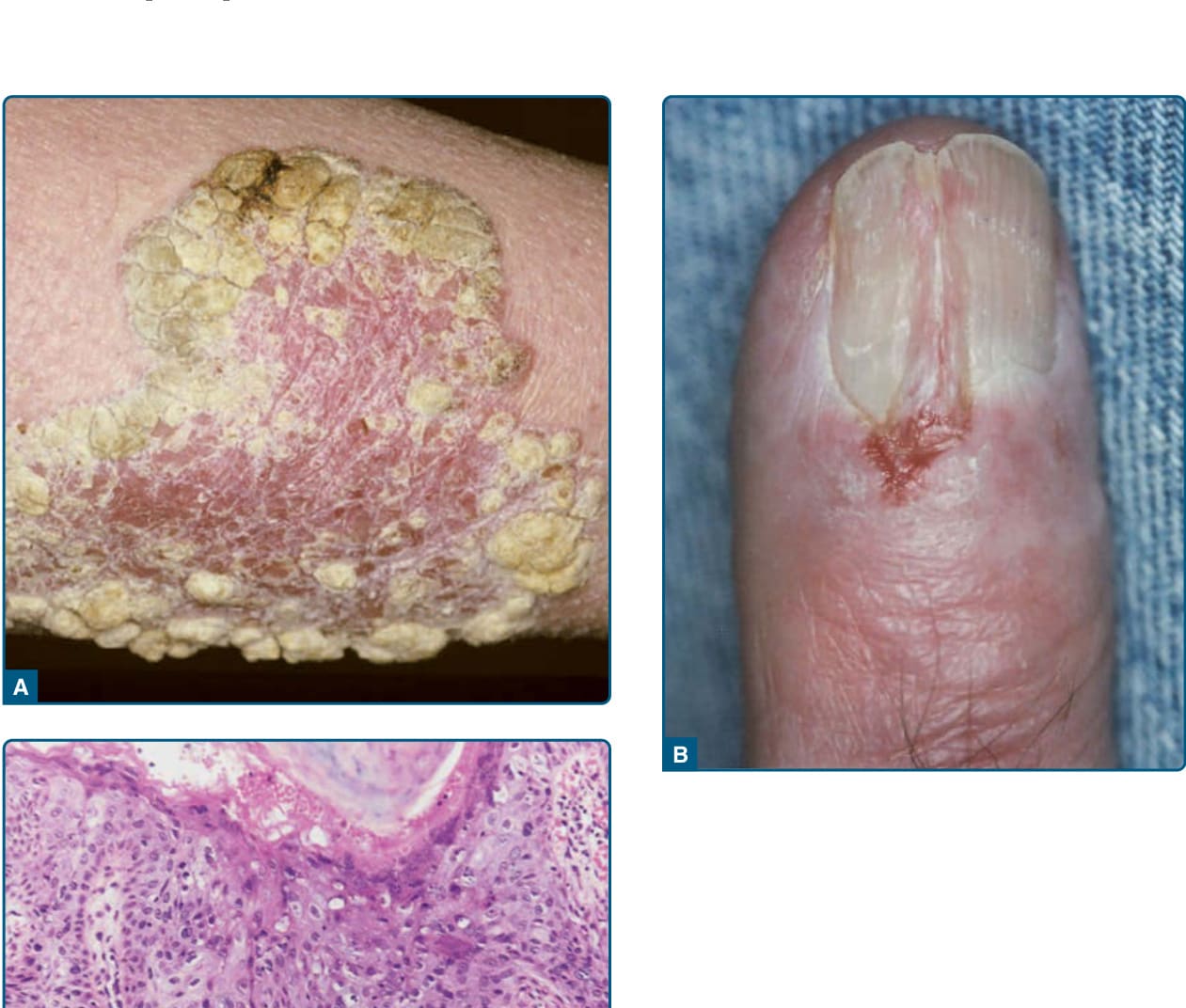
Figure 110-9 A, Large plaque of Bowen disease of the leg. B, Bowen disease of the nail unit resulting in onycholysis. C, Typical histopathologic features of Bowen disease include full-thickness epidermal atypia with loss of the stratified architecture. Involvement of adnexal structures is commonly seen.
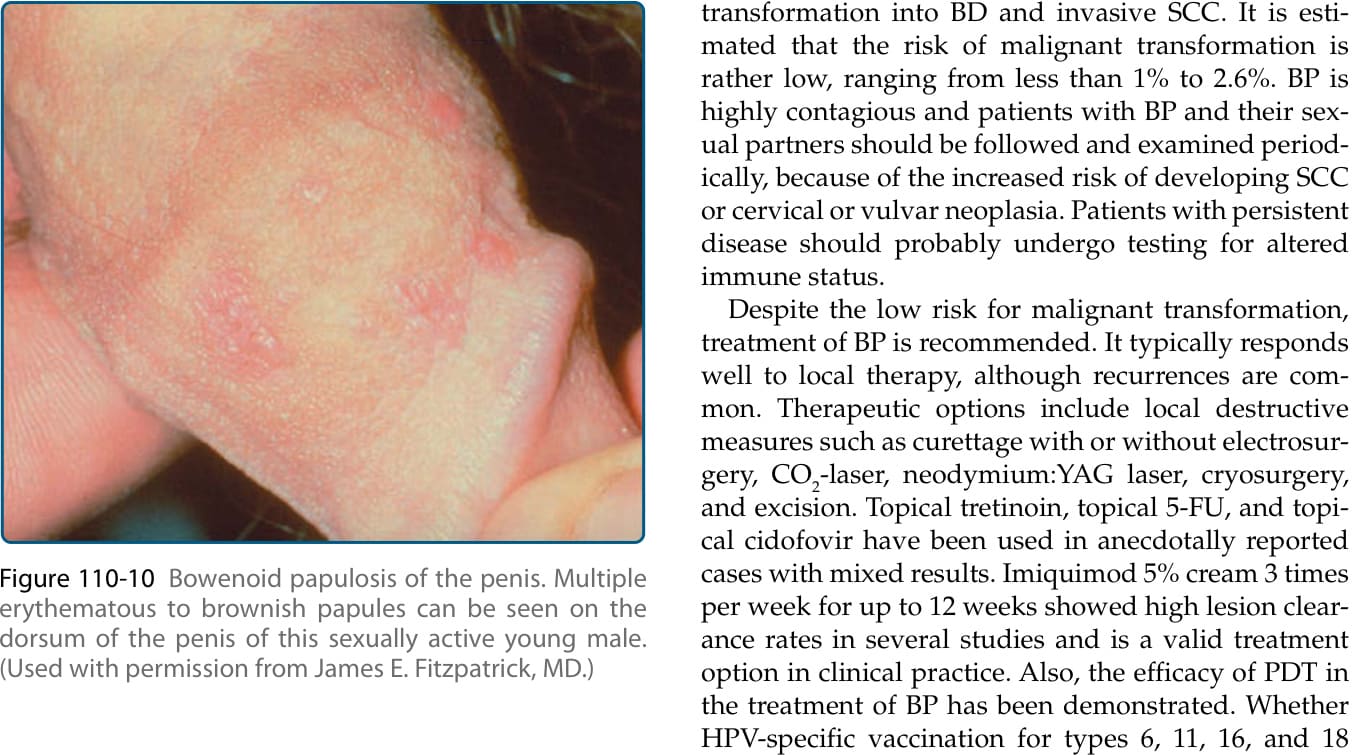
Figure 110-10 Bowenoid papulosis of the penis. Multiple erythematous to brownish papules can be seen on the dorsum of the penis of this sexually active young male. (Used with permission from James E. Fitzpatrick, MD.)
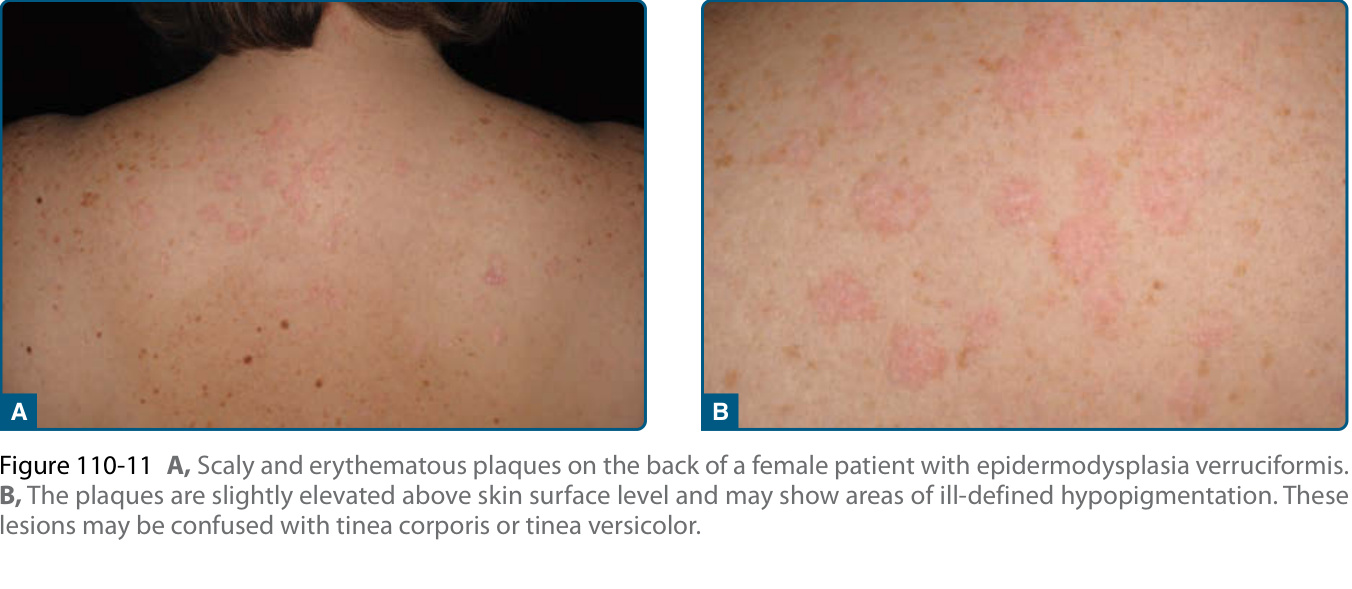
Figure 110-11 A, Scaly and erythematous plaques on the back of a female patient with epidermodysplasia verruciformis. B, The plaques are slightly elevated above skin surface level and may show areas of ill-defined hypopigmentation. These lesions may be confused with tinea corporis or tinea versicolor.

Figure 110-12 Penile intraepithelial neoplasia (PIN) in a male patient. A, The erythroplasia of Queyrat (EQ) variant clinically presents with well-demarcated, erythematous plaques on the mucosal surface of the penis. B, In contrast, the genital Bowen disease (GBD) variant shows variably pigmented and erythematous papules, mainly located on the shaft of the penis. This condition is at times difficult to distinguish from typical condylomata acuminata (C).

Figure 110-13 Oral leukoplakia of the left cheek in a 65-year-old male with chronic HIV infection and a history of smoking. Note the irregular and verrucous surface (nonhomogeneous variant).

Figure 110-14 Disseminated arsenic keratoses in a male patient who had been exposed to arsenic therapeutically for many years in the past to treat his psoriasis. The lesions were found on the entire skin including trunk, arms, and legs. Keratoses of the chest are shown.
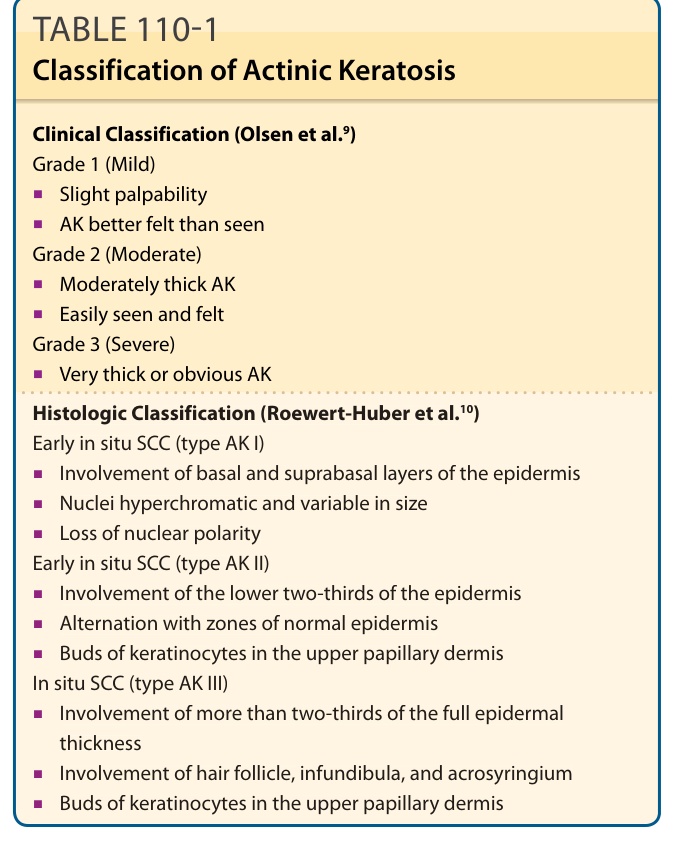
TABLE 110-1 Classification of Actinic Keratosis
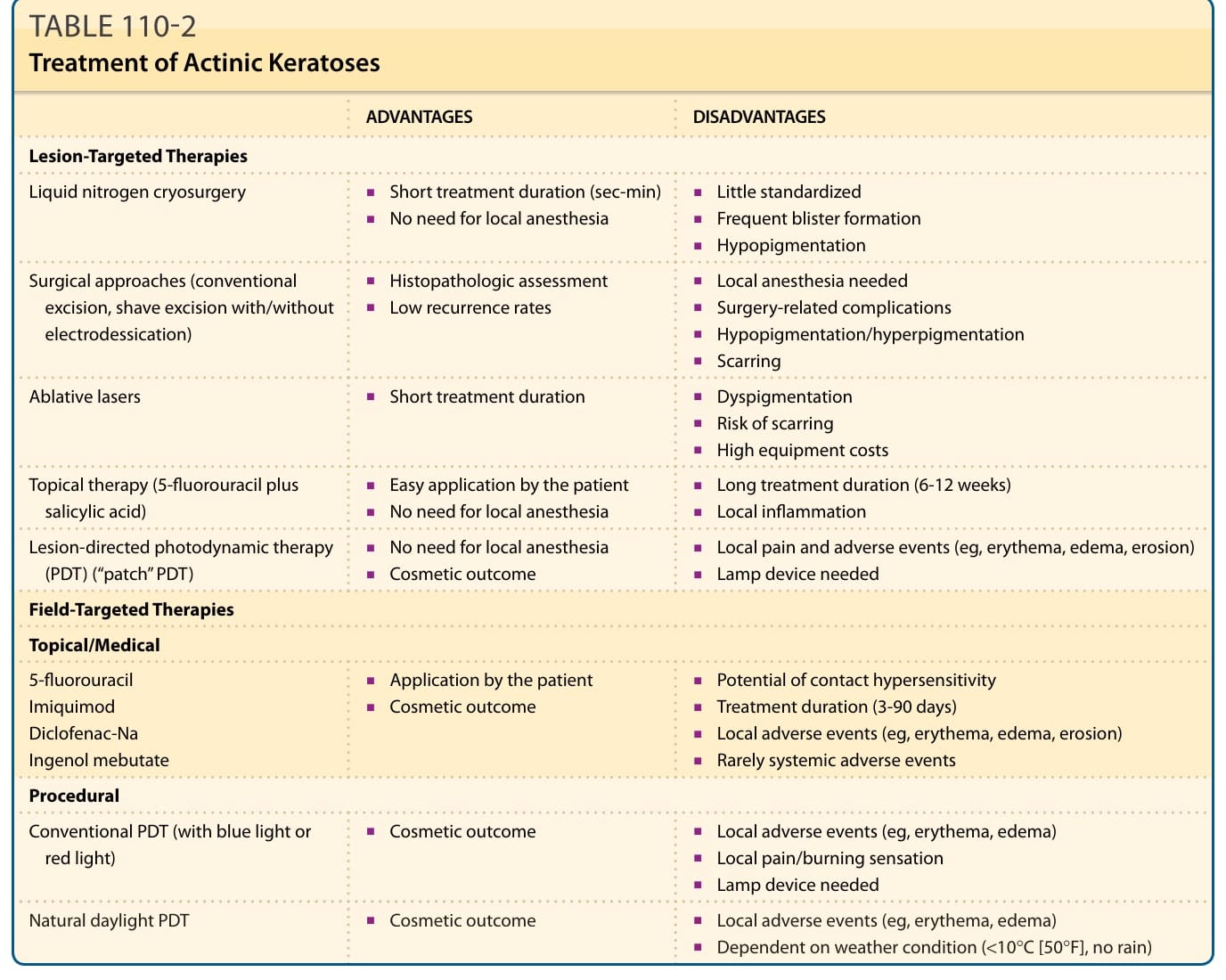
TABLE 110-2 Treatment of Actinic Keratoses
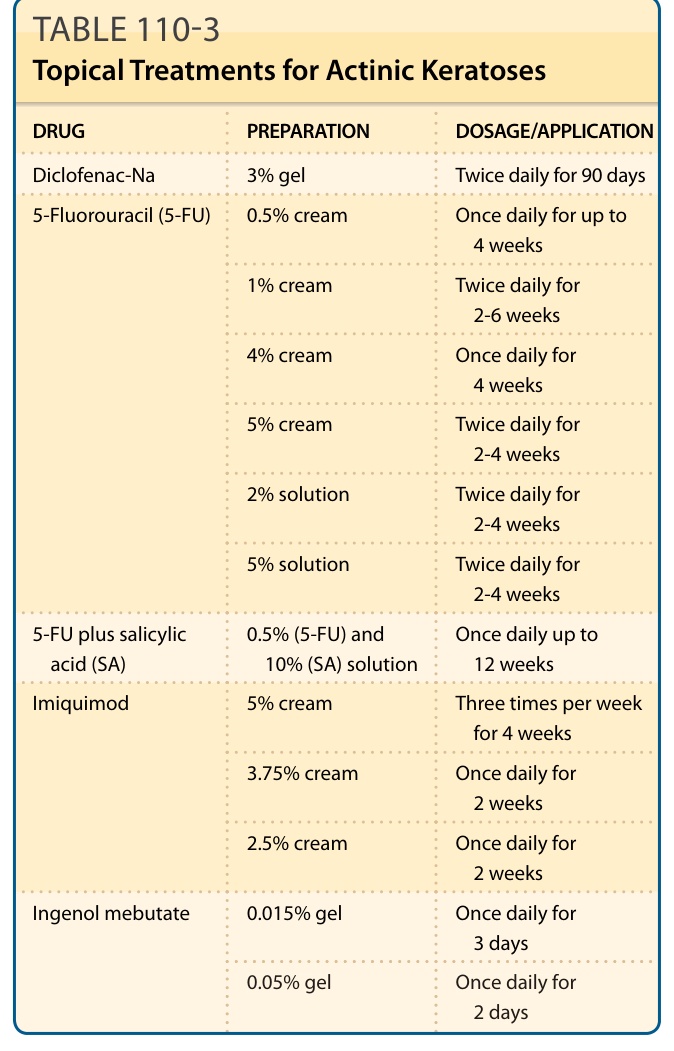
TABLE 110-3 Topical Treatments for Actinic Keratoses
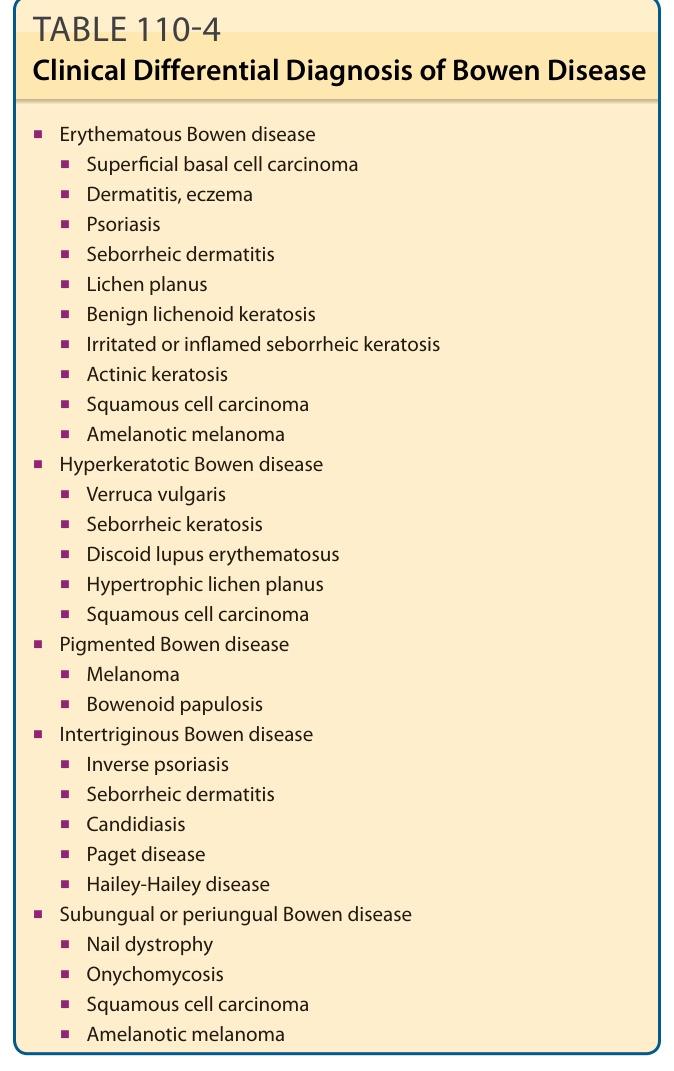
TABLE 110-4 Clinical Differential Diagnosis of Bowen Disease
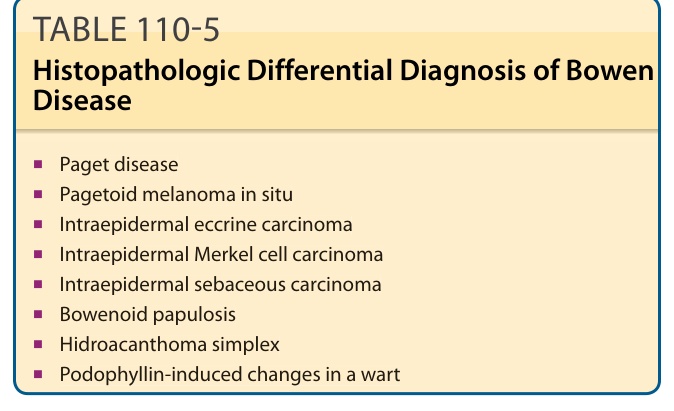
TABLE 110-5 Histopathologic Differential Diagnosis of Bowen Disease
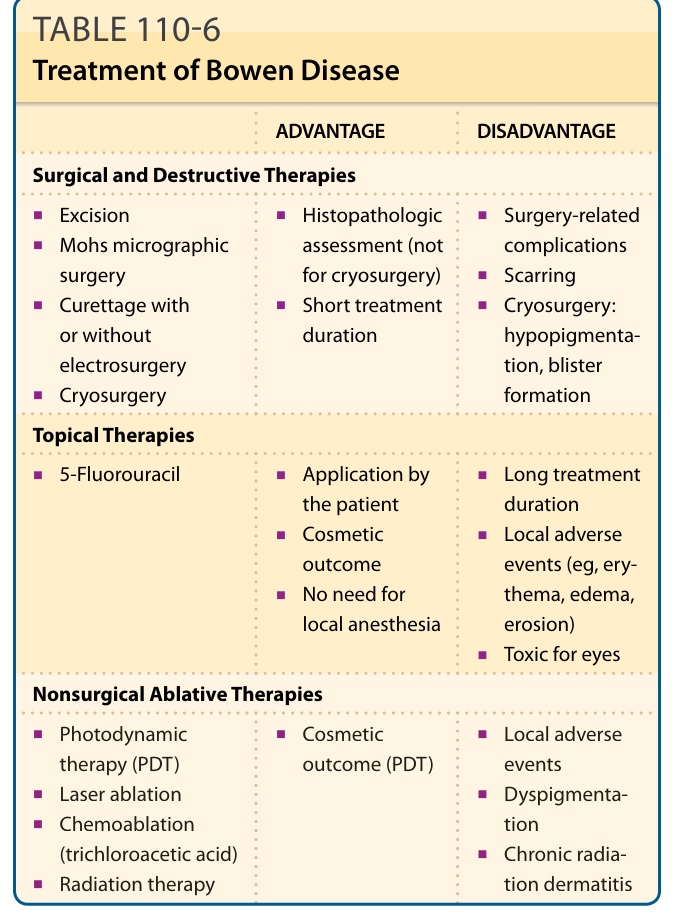
TABLE 110-6 Treatment of Bowen Disease
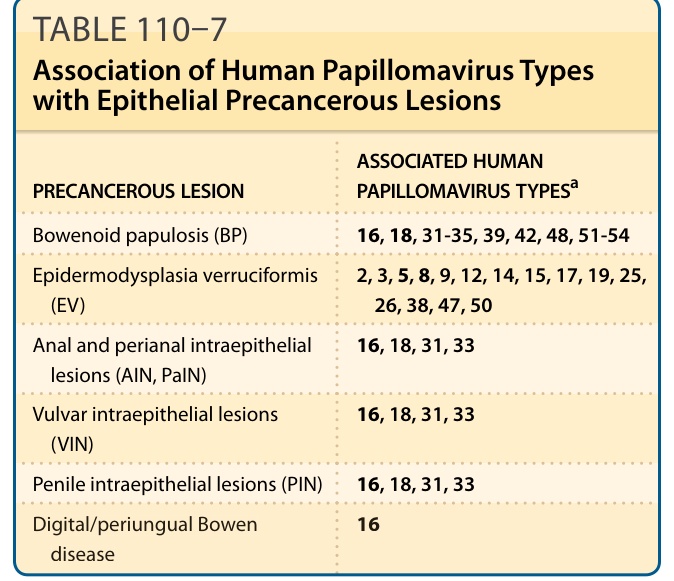
TABLE 110–7 Association of Human Papillomavirus Types with Epithelial Precancerous Lesions
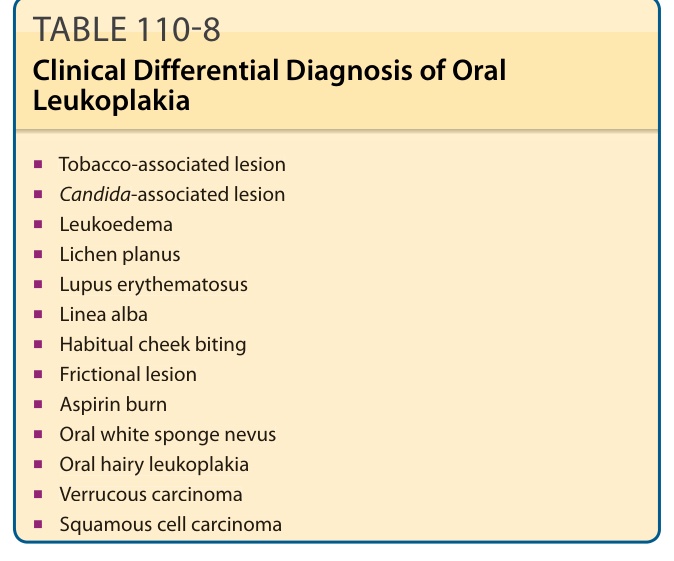
TABLE 110-8 Clinical Differential Diagnosis of Oral Leukoplakia
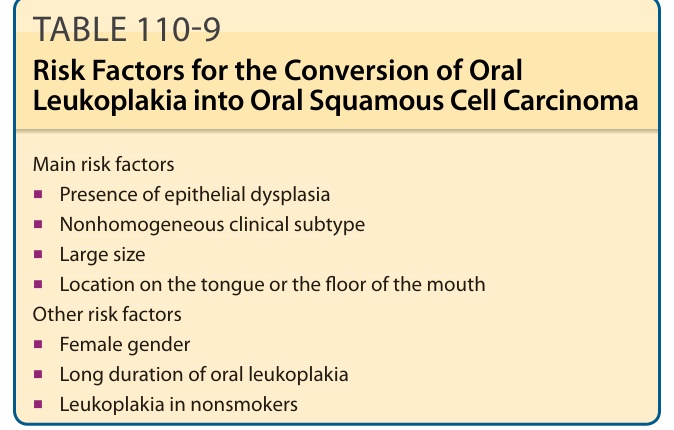
TABLE 110-9 Risk Factors for the Conversion of Oral Leukoplakia into Oral Squamous Cell Carcinoma
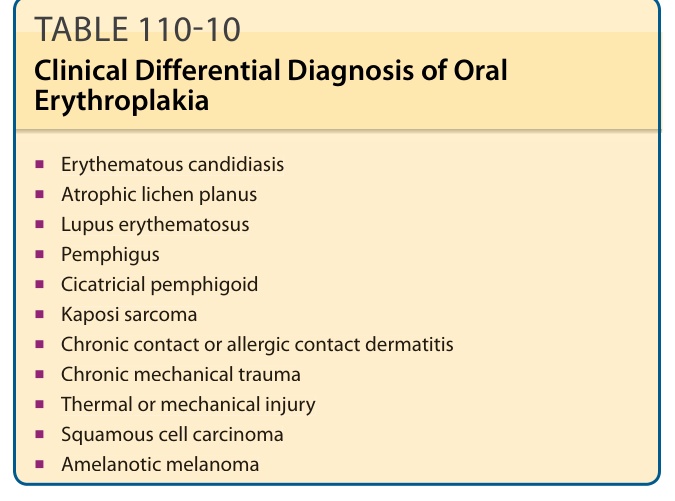
TABLE 110-10 Clinical Differential Diagnosis of Oral Erythroplakia