Skin Aging
19
AT-A-GLANCE
■ Intrinsic skin aging includes the inevitable physiologic changes of the skin that occur with time and are influenced by genetic and hormonal factors.
■ Extrinsic skin aging is the preventable structural and functional changes of the skin that occur with exposure to environmental factors, the most important source being ultraviolet radiation.
■ Intrinsic and extrinsic aging of the skin have distinct histologic and clinical manifestations.
■ Oxidative damage is a common component of the multiple mechanisms of aging.
■ Geriatric dermatoses include solar lentigines, seborrheic keratoses, senile angiomas, xerosis, asteatotic eczema, and pruritus.
■ There is increased incidence of benign and malignant skin growths in the elderly population.
■ Infections in the elderly often have distinctive causative organisms and increased morbidity and mortality relative to younger patients.
In Westernized countries, the chronologic age of older than 65 years is accepted as the definition of an elderly individual. By 2050, the elderly population is estimated to more than double in developing countries (World Health Organization. Global Health and Aging. 2011; http://www.who.int/ageing/publications/global_ health/en/). This demographic transformation will present unique challenges to physicians across the medical specialties, including dermatology. Aging is an inevitable and dynamic biologic process that is characterized by the progressive deterioration of many body systems and decline in physiologic reserve capacity. Given its location at the body’s environmental interface, human skin undergoes 2 distinct types of aging: intrinsic and extrinsic. Intrinsically aged skin appears dry and pale with fine wrinkles and increased laxity; whereas, photoaged skin is darker, coarser, and often has mottled pigmentation (Fig. 106-1). Intrinsic aging encompasses a set of gradual physiologic changes that are a consequence of time and under genetic and hormonal control. Conversely, extrinsic aging, also termed photoaging, includes dramatic structural and functional changes that are caused by exogenous factors, the primary one being unprotected sun exposure.
OXIDATIVE STRESS AND AGING
One theory of aging involves cellular senescence or apoptosis secondary to oxidative damage.1 The generation of reactive oxygen species is a normal consequence of aerobic metabolism. Accordingly, a complex antioxidant system of enzymatic and nonenzymatic effectors has evolved to counteract the endogenously and exogenously produced free radicals in the skin (Table 106-1). However, the skin’s antioxidant defenses tend to weaken with age,2 and the resultant oxidative stress contributes to intrinsic aging. Oxidative damage leads to the upregulation of stress-related factors, which can then trigger downstream events enabling the aging process. For example, stress-induced factors, such as hypoxia-inducible factors and nuclear factor κB, induce the expression of cytokines. Some of these cytokines, like interleukin-1, interleukin-6, vascular endothelial growth factor and tumor necrosis factor-α, have been shown to be proinflammatory regulators of cell survival and modulators of matrix-degrading metalloproteins.3-5 Additionally, oxidative damage to cellular proteins combined with the age-related deterioration of proteasome activity results in the accumulation of damaged proteins that interfere with normal cellular function. Oxidative stress also modifies telomeres, the terminal portions of linear chromosomes that defend against degradation or fusion. Telomeres consist of hundreds of tandem DNA sequence repeats that are shortened with each somatic cell division. The shortening of telomeres is a result of the inability of DNA polymerase to replicate the final base pairs of a chromosome. When the telomeres reach a “critically short” threshold, the cell undergoes proliferative senescence or apoptosis, depending on the cell type. In addition to shortened telomeres secondary to serial cellular division, oxidative insult appears to trigger telomere signaling. Kosmadaki and Gilchrest have proposed a common final pathway for intrinsic and photoaging leading to the disruption of the normal loop structure at the end of telomeres. The exposure of the normally buried TTAGGG tandem repeat of the 3′ overhang strand then activates p53 signaling leading to downstream events that include proliferative senescence and apoptosis (Fig. 106-2).6
It has been suggested that cellular senescence is the cellular basis for aging.7 After a finite number of cellular divisions, the cell cycle of a mammalian cell is irreversibly arrested and the cell has entered a state
19
known as replicative senescence.8 Cellular senescence has been described as a possible tumor-suppressor mechanism, which precludes the unregulated growth of cells that have acquired multiple genetic mutations over time. This apparent biologic trade off of increased life span and increased risk of malignant transformation is further underscored by the observation that improved DNA repair mechanisms correlate with longer life spans in mammalian species.9
INTRINSIC SKIN AGING
Intrinsic or chronologic skin aging refers to the seemingly unavoidable physiologic changes of the skin that occur with time and are influenced by genetic and hormonal factors. These alterations include decreased collagen production, reduced blood flow, lowered amounts of lipids, and the loss of rete ridges.10 The result is dry, pale skin with fine wrinkles, less elasticity, and impaired reparative capacity (Fig. 106-3). Intrinsically aged skin is also characterized by the development of a range of benign neoplasms, resulting from impaired regulation of cellular proliferation.11
EXTRINSIC SKIN AGING
Extrinsic skin aging entails the physiologic and histologic changes caused by environmental factors. The most powerful source of extrinsic aging is ultraviolet radiation. The ultraviolet radiation–mediated
ENZYMATIC NONENZYMATIC
Glutathione peroxidase Vitamin C (ascorbic acid)
Catalase Vitamin E
Superoxide dismutase Glutathione Thioredoxin system Carotenoids Flavonoids
Superoxide dismutase
Glutathione Thioredoxin system Carotenoids Flavonoids
1780
Telomeres in loop configuration
Telomere overhang concealed
5’ 3’ 5’
3’
Telomere overhang exposed
Acute DNA damage Critical telomere shortening
5’
3’
5’ 3’
5’ 3’ 5’
3’
Apoptosis Proliferative senescence
p53
structural and functional changes of the skin are known as photoaging, which is described in “Photoaging” section in more detail below. Other exogenous factors that contribute to extrinsic skin aging include cigarette
smoking, diet, chemical exposure, trauma, and air pollutants (eg, particulate matter, CO2, CO, SO2, NO, and NO2). In fact, an intense interest in the effects of air pollution on skin physiology has developed in recent years, giving rise to several mechanistic and epidemiologic studies.12 The initial link between airborne particle exposure and extrinsic skin aging was established by a cross-sectional study in Germany that found an association between exposure to chronic trafficrelated particulate matter and premature skin aging with pigment spot formation.13 Indoor air pollution, such as cooking with fossil fuels, also has been associated with accelerated aging in Chinese populations.14
Activation of the aryl hydrocarbon receptor by exogenous factors like tobacco smoke extract and airborne particulate matter has been identified as a potential contributor to extrinsic aging.15,16 Ozone also causes skin inflammation and disrupts barrier function by inducing lipid peroxidation and protein oxidation in the stratum corneum.16
Unlike intrinsic aging, extrinsic aging is more amenable to intervention and preventive measures. Typical clinical features of extrinsically aged skin, which are mostly ultraviolet radiation–mediated, include deep wrinkles, laxity, coarseness, increased fragility, and multiple telangiectases. Moreover, photodamaged skin may appear darker and have mottled pigmentation (Fig. 106-4). Extrinsically aged skin has an increased tendency to develop benign and malignant growths.11
19
INTRINSIC AGING EXTRINSIC AGING
Histologic features Epidermal thinning Loss of rete ridges Decreased number of collagen and elastin fibers
Solar elastosis Reduced number of fibroblasts Reduced amount of extracellular matrix
Clinical
Xerosis Pallor Fine wrinkles Decreased elasticity Fragility
Xerosis Multiple telangiectases Deep wrinkles Decreased elasticity Fragility Dyspigmentation
Clinical features Xerosis Pallor Fine wrinkles Decreased elasticity Fragility
Xerosis Multiple telangiectases Deep wrinkles Decreased elasticity Fragility Dyspigmentation
features
PHOTOAGING
PHOTOAGING
At the earth’s surface, sunlight is composed of infrared, visible, and ultraviolet (UV) light, with most of the UV blocked by the earth’s atmosphere. Of the UV radiation that reaches the earth’s surface, more than 95% is UVA (320 to 400 nm) and approximately 5% is UVB (280 to 320 nm). Both UVA and UVB contribute to skin aging. UVB, which only penetrates into the epidermis and upper dermis, is a chief source of direct DNA damage, inflammation, and immunosuppression.17 Conversely, UVA deeply penetrates the skin down to the lower dermis. UVA is considered a larger contributor to skin aging than UVB because of its greater depth of penetration and its higher percentage of surface sunlight. In addition to the mechanisms of aging discussed before, photodamage contributes to extrinsic aging through other mechanisms. UV damage impacts collagen degradation and synthesis, as well as causes the production of elastotic material in the skin, both of which are further described in section “Dermis”. Photodamaged skin is also associated with a higher frequency of mitochondrial DNA mutations that result in decreased mitochondrial function and the generation of reactive oxygen species.16 The basement membrane at the dermal–epidermal junction is also damaged in sun-exposed skin. Following UV radiation exposure, the basement membrane becomes multilayered and partially disrupted. Additionally, matrix metalloproteinases (MMPs) and urinary plasminogen activator are increased in photodamaged skin.18
Recently, there has been a growing interest in the impact of non-UV solar radiation on skin physiology and aging. Approximately 50% of the total solar spectrum is visible light (400 to 700 nm), which is able to penetrate down to the hypodermis.19 Visible light generates reactive oxygen species in human skin20 and induces the formation of oxidized DNA bases.21 Additionally, irradiation of human skin equivalents with visible light results in increased production of proinflammatory cytokines and MMP-1.22 Nearly 45% of the
1781
19
solar spectrum reaching human skin is infrared, which is composed of infrared A (700 to 1400 nm), infrared B (1400 to 3000 nm), and infrared C (3000 nm to 1 mm). Infrared B and infrared C do not penetrate the skin well, but infrared A can reach down to the hypodermis, increase reactive oxygen species production, and impact mitochondrial integrity.19
ESTROGEN AND SKIN AGING
ESTROGEN AND
SKIN AGING
In addition to their reproductive roles, estrogens are important regulators of skin physiology and wound healing (Table 106-3). Estrogens exert their effects through specific estrogen receptors, which can act as ligand-activated transcription factors. Estrogen receptor signaling is a critical modulator of redox (reduction–oxidation) balance and oxidative stress, which is central to many of the mechanisms of skin aging. Recently, estrogens have been shown to have nongenomic effects that occur through estrogen receptor–independent mechanisms, including interactions with membrane-associated G-coupled protein receptors and subsequent activation of signal transduction pathways.23 Both genomic and nongenomic effects of estrogen appear to be critical mediators of skin physiology and may impact skin aging. As the population of menopausal women increases, the profound impact of changes in estrogen levels on aging grows in clinical relevance. In premenopausal women, the predominant form of estrogen is estradiol, which is produced by the ovaries. After menopause, the levels of estradiol drop dramatically and women may experience a rapid onset of skin aging. Postmenopausal changes that have been reported include decreased collagen content, thinner skin, reduced elasticity, dryness, and increased wrinkling. These changes reflect the loss of the protective effects of estrogen and can be ameliorated with estrogen replacement.24
SKIN COMPONENT EFFECT OF ESTROGENS
Epidermis Increase in mitotic activity of epidermal cells Stimulation of epidermal melanocytes
Dermis Increase in collagen synthesis, maturation, and turnover Morphologic improvement of collagen and elastic fibers
Glands Reduction in activity of sebaceous and apocrine glands
Hair follicle Influences hair follicle cycle May inhibit activity of follicular melanocytes
Hair follicle Influences hair follicle cycle May inhibit activity of follicular melanocytes
1782
Data from Thornton MJ. The biological actions of estrogens on skin. Exp Dermatol. 2002;11(6):487-502.
Several studies have examined the effect of topical estrogens on human skin. Treatment of photoaged facial skin with a conjugated estrogen cream increased skin thickness and decreased fine wrinkles.25 Several studies have found that topical administration of estradiol induces procollagen in sun-protected skin of postmenopausal women and age-matched men.26,27 Despite the similar expression of estrogen receptors in photoaged and intrinsically aged skin, topical estradiol did not alter procollagen production in photoaged skin, suggesting that changes that result from long-term sun exposure impede the ability of topical estrogen to stimulate collagen synthesis. Furthermore, these findings indicate that the estradiol-mediated effect on collagen production is indirect, that is, independent of estrogen receptor signaling.
EPIDERMIS
The human epidermis undergoes several structural and functional age-related alterations. Between the third and eighth decades of life, the epidermal turnover rate decreases by 30% to 50%,28 coinciding with a deterioration of wound repair capacity. During this time period, there is also an overall thinning of unexposed epidermis by 10% to 50%. The spinous cell layer appears to be the most greatly impacted by epidermal atrophy, whereas the stratum corneum and stratum granulosum are largely unaffected.29 The most pronounced and consistent histologic change of aged skin is flattening of the dermal–epidermal junction and loss of rete ridges, resulting in decreased surface contact area and presumably less nutritional support of the avascular epidermis by the vascularized dermis.11
These alterations account for the increased fragility of aged skin to minor trauma as well as propensity to blister. Although the average thickness of the stratum corneum does not change with age, older skin has a greater susceptibility to irritant contact dermatitis and severe xerosis. Aged skin also has altered drug permeability with reduced absorption of hydrophilic substances observed in older skin relative to younger controls.30
Taken together, these observations suggest a compromise of the aged epidermal permeability barrier. Indeed, intrinsically aged skin has impaired barrier recovery following challenge. This may be partly because of a global decline of stratum corneum lipids, leading to diminished lamellar bilayers in the stratum corneum interstices.31 Moreover, between the ages of 50 and 80 years, abnormal stratum corneum acidification results in impaired lipid-processing enzymatic activity,32 as well as abnormal permeability barrier homeostasis and stratum corneum integrity.33 An agerelated decrease in epidermal filaggrin also has been proposed to impact barrier function and to account for the increased dryness and scaliness of older skin.34
At the cellular level, a number of important agerelated changes occur in epidermal keratinocytes. Cellular heterogeneity—for example, differences in cellular shape, size, and staining characteristics—results
CELL TYPE STRUCTURAL CHANGES FUNCTIONAL CHANGES
Epidermal keratinocytes Epidermal dyscrasia Reduced mitotic activity Increased migration time Increased senescence
Melanocytes Atypia Decreased number of functional melanocytes Increased number in photodamaged skin
Decreased melanin production
Langerhans
Decreased number Fewer and shorter
Decreased antigen
Langerhans cells Decreased number Fewer and shorter dendrites
Decreased antigen presentation capability
cells
presentation capability
dendrites
in epidermal dyscrasia, a mild actinic keratosis that is particularly accentuated in photoaged skin. Epidermal dyscrasia is associated with reduced mitotic activity, lengthened cell cycle, and increased migration time from the basal cell layer to the stratum corneum.35 It has been shown in vitro that human keratinocytes approach replicative senescence after 50 to 100 doublings and arrest in G1 phase.36 Because senescent cells are resistant to apoptosis, they may accumulate DNA mutations and protein damage over time. The buildup of senescent keratinocytes over time may provide the mechanistic link between aging and epidermal carcinogenesis.35
In addition to keratinocytes, the other resident cells of the epidermis—melanocytes and Langerhans cells— experience age-associated changes. Although the density of melanocytes doubles in photodamaged skin, the number of functional melanocytes in the basal layer declines by up to 20% per decade.37 This decrease of melanocytes is associated with a decrease in protective melanin, which in addition to the age-related impairment of DNA repair mechanisms, contributes to an elevated risk of skin cancer in the elderly. The incidence of melanocytic nevi also declines with age.38 In aged epidermis, there is also a reduction of the number and the responsiveness of Langerhans cells,39 the dendritic cells of the skin. Langerhans cells of older skin undergo structural changes, for example, fewer and shorter dendrites, and have diminished antigen presenting capacity,40 which likely contributes to weakened cutaneous immunity in the elderly. Table 106-4 summarizes the age-related changes in the various epidermal cell types.
DERMIS
Age-related biochemical changes in collagen, the main component of the dermis and the structural scaffold of the skin, may account for many of the characteristics of older skin, including increased rigidity and impaired wound healing.41 There is a reduction of collagen types I and III in intrinsically aged skin that
19
is enhanced by photodamage.42 There is a significant downregulation of collagen synthesis in the skin with age43 and photodamage.44 An age-dependent difference in the collagen-synthetic capacity of aging fibroblasts partially accounts for the lower collagen synthesis in intrinsically aged skin.45 Collagen fragmentation also contributes to the downregulation of collagen synthesis in both intrinsically aged and photoaged skin. Collagen-degrading MMPs gradually increase with age.43 Acute UV irradiation transiently upregulates 3 MMPs (MMP-1, MMP-3, and MMP-9) in the skin, with the epidermis being the major source.46,47
In contrast, chronically photodamaged skin has been shown to constitutively express higher levels of 7 MMPs (MMP-1, MMP-2, MMP-3, MMP-9, MMP-11, MMP-17, and MMP-27), which are primarily derived from dermal fibroblasts.48 The resulting fragmentation of collagen is unable to produce an amount of mechanical tension on the fibroblasts to stimulate collagen synthesis.45 Thus, elevated MMP activity in the dermis of photodamaged skin creates a microenvironment of fragmented collagen that impairs fibroblast function leading to abnormal collagen homeostasis with increased degradation and decreased production of collagen. Elastin, the dermal element that provides elasticity and resilience, is also altered with aging. Solar elastosis, the most striking histologic alteration of photodamaged dermis, is characterized by the replacement of normal elastic fibers with a disordered mass of elastotic material (ie, degraded elastic fibers, tropoelastin, and fibrillin) that is localized near the dermal–epidermal junction.49 Even in sun-protected chronologically older (>70 years old) skin, elastin fibers are reduced in number and diameter, appear fragmented, and exhibit increased crosslinkage and calcification.50,51 These structural abnormalities in elastin translate into impaired function, namely a fall off of elastic recovery and resilience in aged skin. Aging also affects the ground substance of the skin, which is composed of proteoglycans and glycosaminoglycans leading to decreased interaction of proteins with water. Although glycosaminoglycans are increased in photoaged skin, their deposition in the abnormal elastotic material prevents the normal attraction of water molecules, resulting in tetrahedron water.52,53 In contrast, in intrinsically aged skin there is a progressive decline of hyaluronic acid, possibly secondary to decreased secretion or extractability.54,55 All of these changes in the ground substance of the skin may contribute to age-related declines in skin hydration and turgor. Table 106-5 summarizes the consequences of the age-dependent alterations of the dermal components.
SKIN APPENDAGES
HAIR
HAIR
With aging, there are striking spatially dependent and hormonally influenced changes in overall hair density and texture. Elderly men commonly have a drop in the density of chest, axillary, and pubic hair, but an
1783
19
DERMAL COMPONENT STRUCTURAL CHANGES FUNCTIONAL CHANGES
Collagen Increased rigidity Reduction of types I and III collagen Increased fragmentation
Impaired wound healing Decreased mechanical stress on fibroblasts (→ decreased collagen synthesis)
Elastin Reduced number and diameter of elastin fibers Solar elastosis (photodamage)
Decreased elasticity
Ground
Abnormal deposition of
Decreased skin
Ground substance Abnormal deposition of glycosaminoglycans preventing normal interaction with water Reduced hyaluronic acid
Decreased skin hydration
substance
glycosaminoglycans preventing normal interaction with water Reduced hyaluronic acid
hydration
increase of hair in other body sites, especially the nostrils, external auditory meatus, and eyebrows. Elderly women typically experience a new growth of coarse hair on the chin and upper lip, likely resulting from the unopposed influence of testosterone secondary to falling estrogen levels.11
Both men and women are affected by age-related alopecia. Senescent alopecia is the age-related thinning of hair, whereas androgenetic alopecia (or male pattern hair loss) is a distinct entity that can occur at an earlier age and results from the effect of dihydrotestosterone on hair follicles.56 Conversely, only a small portion of female pattern hair loss may actually be androgenic.57
By the age of 60 years, nearly half of the population has at least 50% gray scalp hair, with everyone experiencing some amount of graying.58 Hair graying is a result of the progressive depletion of melanocytes specifically in the hair bulb. The reasons for the vulnerability of this specific melanocyte stem cell population is not completely understood, but may be related to the high lifetime proliferative rate and relative sensitivity to oxidative stressors.59,60 Recently, a sublineage of hair shaft progenitors in the hair matrix that are differentiated from follicular epithelial cells expressing the transcription factor KROX2 have been identified and shown to be a source of stem cell factor, which is critical for the maintenance of differentiated follicular melanocytes and hair pigmentation.61 Whether this stem cell factor–dependent niche for follicular melanocytes is impaired in aging remains to be seen.
NAILS
NAILS
Until approximately the age of 25 years, the rate of linear nail growth steadily increases, then drops off.62 The texture of the nails also changes with age. In elderly
1784
individuals, nails are typically more brittle. Older nails may also exhibit ridging as a consequence of variation in lipid composition.63
CUTANEOUS GLANDS AND NERVES
There are striking age-related alterations in all of the glands of the skin. Both the number and output of eccrine glands decline with age.64 The resulting decrease in spontaneous sweating renders the elderly more vulnerable to heat stroke. There is also a reduction in the size and function of apocrine glands in older skin.65 Although the size and number of sebaceous glands appear constant, there is a drop of sebum production that is likely associated with hormonal changes.66
With aging, tactile thresholds are increased.67 The decrease in the size and density of Pacinian and Meissner corpuscles may account for this finding.68,69
There is also an increase in thermal pain thresholds in the elderly.70 An age-associated decline in the spatial acuity (ability to discriminate between 2 points, light touch, and vibration) of the skin also occurs.71,72
GERIATRIC DERMATOSES
BENIGN SKIN LESIONS
BENIGN SKIN LESIONS
Benign proliferative growths commonly occur in aging skin. Solar lentigines, also known as senile lentigines and liver spots, are well-defined patches of hyperpigmentation that are associated with UV exposure and especially common in fair-skinned individuals (Fig. 106-5). The reported average prevalence of solar lentigines ranges from 10% to 90% in older subjects.73 Solar lentigines do not require any treatment; however, lentigo maligna and lentigo maligna melanoma, which are more serious malignant conditions, should be excluded. The role of repeated UV exposure in the pathogenesis of solar lentigines is not completely
understood, but appears to involve increased melanin production and abnormal proliferation and differentiation of keratinocytes.74
Another common skin disorder in the elderly are seborrheic keratoses (Fig. 106-6A), which are benign papules or plaques that are highly variable in color, may have a waxy or wart-like appearance, and can arise as a single lesion or as multiple growths. Reported prevalences of seborrheic keratoses have ranged between 8% and 54% in elderly subjects.73 Similar to senile lentigines, seborrheic keratoses have no malignant potential and do not require therapy beyond cosmetic reasons. Unlike senile lentigines, the development of seborrheic keratoses is independent of UV exposure and is likely a result of impaired focal epidermal homeostasis resulting in the clonal expansion of melanocytes and keratinocytes.75 The pathogenesis of seborrheic keratoses is currently under investigation (see Chap. 108). Interestingly, keratinocyte-derived endothelin-1, which is a regulator of melanocyte function, has been implicated.76
Senile angiomas (Fig. 106-6B), also known as cherry angiomas, are another skin disorder that afflicts elderly subjects. They are small circular or oval red papules resulting from the proliferation of blood vessels that tend to increase in size and number with age and may bleed with minor trauma. The prevalence of senile angiomas has been reported as 50% to 75% in older individuals.73 Treatment for senile angiomas
A
B
19
is not needed unless for cosmetic reasons or repeated bleeding.
MALIGNANT SKIN LESIONS
MALIGNANT SKIN LESIONS
The incidence of skin cancer, both melanoma and nonmelanoma skin cancers increases exponentially over a lifetime. In elderly populations, skin cancers represent approximately 40% of diagnosed malignant neoplasms. Older individuals with skin cancer are also at increased risk for poor outcomes. In particular, elderly males present with thicker melanomas and have increased mortality when compared to age-matched women and younger men.77 The vast majority of skin cancer cases is basal cell cancer; however, squamous cell cancers are associated with greater nonmelanoma skin cancer–related morbidity and mortality.78
As one ages, the constant exposure to carcinogens, especially UV irradiation, leads to an accumulation of mutations. Compounding this risk is an age-related impairment of DNA repair capacity in response to UV exposure and decline in immune function.79 There is a relationship between the risk of the type of skin cancer and the nature of the UV exposure. Squamous cell cancer and its precursor lesion, actinic keratosis, are associated with habitual sun exposure, whereas basal cell cancer and malignant melanoma correlate with a history of habitual or intense intermittent sun exposure.80
Merkel cell carcinoma (MCC, see Chap. 113) is a rare and aggressive type of cutaneous cancer that presents as a painless rapidly growing nodule that may be flesh-colored or bluish-red and typically occurs in sunexposed areas of the body. Ninety percent of all cases of Merkel cell carcinoma occur in patients older than 50.81 It is also associated with immunosuppression.82
Merkel cell carcinoma is considered a neuroendocrine tumor of the skin that arises from a 2-step process: the integration of the Merkel polyomavirus genome into the host genome and development of T-antigen mutations that prevent autonomous replication of the viral genome. The result is an avoidance of DNA damage responses or recognition of the viral T-antigen by the immune system leading to tumor growth.83 The clinical characteristics of Merkel cell carcinoma have been summarized in an acronym: AEIOU (asymptomatic/ lack of tenderness, expanding rapidly, immune compromised, older than 50 years, and UV-exposed site on a person of fair skin).84 These characteristics have been shown to be highly sensitive for Merkel cell carcinoma and can aid in the decision to biopsy and improve early detection of this aggressive cancer. Angiosarcoma, a cancer of the inner lining of blood vessels, most commonly occurs in the elderly. It can affect any area of the body, but the majority present on the head and neck (Fig. 106-7). Rapidly proliferating and invasive anaplastic cells are characteristic of angiosarcoma. This aggressive and highly metastatic cancer is associated with a high mortality and often leads to death within 2 years of initial diagnosis.85
1785
These vascular tumors have been shown to express
19
high levels of vascular endothelial growth factor and vascular endothelial growth factor receptor-2, which have emerged as potential therapeutic targets.86
Kaposi sarcoma (KS) is a lymphoangioproliferative disease that is associated with human herpesvirus-8. There are 4 variants of KS: classic KS (CKS), AIDSassociated KS, iatrogenic posttransplantation KS, and endemic African KS. Only CKS is reviewed here. CKS primarily affects individuals of Eastern European Jewish or Mediterranean descent, and males more than females. CKS lesions are purple, red, or brown macules, plaques, and nodules that typically affect the face or lower extremities, often producing pain and debilitation. CKS lesions can also occur in the lungs, liver, and digestive tract, potentially causing life-threatening obstruction and bleeding. CKS is a rare disorder and its risk factors include increasing age, corticosteroid use, and diabetes. Treatment for localized disease entails observation, radiotherapy, surgery, or intralesional injections of vincristine or interferon alfa-2. However, the efficacy of the various therapies for CKS has not been validated, and standardized treatment guidelines are still needed.87
XEROSIS
XEROSIS
Xerosis, or dry skin, is an extremely common skin disorder in the elderly and frequently affects the legs. The causes of xerosis are multifactorial. The age-associated reduction in the activity of sebaceous and sweat glands may contribute to its development. Alterations in lipid composition,31 impaired filaggrin production,34 and intrinsic changes in keratinization88 are also potential etiologic factors. Xerosis is also associated with chronic renal failure, liver disorders, lower-leg atherosclerosis, autoimmune diseases, and hepatitis C virus infections.73 Treatment options involve environmental changes and application of emollients.88
An associated skin condition is asteatotic eczema (Fig. 106-8), also known as winter itch, eczema craquelé,
1786
and desiccation dermatitis. Asteatotic eczema is xerosis complicated by dermatitis and is characterized by dry, extremely pruritic, fissured skin with scales. It typically presents in the elderly during the winter seasons and is often associated with low humidity in heated environments. Therapies are similar to those for xerosis, for example, behavior and environmental adaptions and topical emollients.89
PRURITUS
PRURITUS
Pruritus, or itchy skin, is a common complaint of elderly patients that has a significant adverse effect on quality of life.90 Pruritus can be caused by xerosis, but also can be a sign of an underlying systemic disease or malignancy. Pruritus has been associated with diabetes mellitus, thyroid disorders, and renal and liver failure. Malignant neoplasms, such as lymphoma or leukemia, can also present as pruritus. Pruritus is also a defining characteristic of the myeloproliferative neoplasm polycythemia vera. Infections such as scabies and tinea pedis are also typical causes of pruritus. Symptomatic treatment and addressing any underlying conditions are the mainstays of pruritus therapy.
INFECTIONS
There are many infections of medical significance that can produce both skin lesions and systemic disease in the elderly. Older individuals may be susceptible to aggressive and life-threatening infections that are rare in younger populations. In devising the appropriate medical intervention, it is important to be aware of the types of bacterial, parasitic, fungal, and viral pathogens that more frequently occur in the elderly. Given the increased likelihood of comorbidities and polypharmacy, differences in drug metabolism, atypical symptomology, and elevated risk of a poor outcome, the geriatric patient with an infection may present unique challenges relative to their younger counterparts.
BACTERIAL
BACTERIAL
Bacterial infections in elderly populations often have distinctive causative organisms and increased morbidity and mortality relative to younger patients. In elderly patients, infection with staphylococci is frequently the cause of impetigo (infection of the superficial layers of the epidermis) and folliculitis (inflammation of the hair follicles).91 Cellulitis, an infection of the dermis and subcutaneous fat, is usually caused by streptococci or staphylococci and may present more subtly in elderly individuals. Risk factors for cellulitis, such as diabetes mellitus, immunodeficiency, lymphedema, and chronic venous insufficiency, are also more prevalent in the elderly. Older patients are particularly vulnerable to certain rare and aggressive forms of cellulitis. Orbital cellulitis can be caused by the contiguous spread of infections of the paranasal sinuses or metastatic spread from a systemic focus. In contrast to preseptal orbital cellulitis, orbital cellulitis involves the soft tissues posterior to the orbital septum. In the absence of adequate treatment, orbital cellulitis can lead to blindness and death from intracranial spread. In older individuals, the cause of orbital cellulitis is typically polymicrobial and may be a mix of aerobic and anaerobic bacteria. Elderly persons with diabetes are more likely to develop Pseudomonas cellulitis of the ear than are other populations.91
In addition to cellulitis, other rare cutaneous infections occur more frequently in the elderly. Erysipelas, a β-hemolytic streptococcal infection of the upper dermis that spreads to the lymphatics, is more common in older individuals and more likely to result in sepsis and other life-threatening complications. It can be distinguished from cellulitis by its demarcated borders. Necrotizing fasciitis, which is often caused by Streptococcus, is associated with increased morbidity and mortality in the elderly. Risk factors for necrotizing fasciitis, such as immunosuppression, diabetes, chronic systemic illnesses, and malignancies, are more prevalent in older individuals. The elderly population also has been identified as being at risk for carriage for methicillin-resistant Staphylococcus aureus,92 which is often implicated in cases of necrotizing fasciitis.
PARASITIC93
PARASITIC
93
Scabies is one of the most clinically significant parasitic infections in the geriatric population. Residents of nursing homes, like other communal living arrangements, are at increased risk for this highly contagious infestation. To complicate the clinical picture, the elderly, similar to other immunosuppressed groups, may present with less-severe pruritus and inflammation. Furthermore, given the common occurrence of xerosis in the elderly, pruritus in an older patient may fail to raise any alarm in the practitioner. Early detection and treatment with topical scabicides and oral ivermectin will help to limit the spread of the infestation. Another
19
parasitic cause of pruritus in the elderly is pediculosis, or infestation with lice. Pediculosis can be treated with malathion, lindane, or permethrin. Less-frequent parasitic infections in the geriatric population include cutaneous larva migrans and cutaneous leishmaniasis.
FUNGAL94
FUNGAL
94
There are several risk factors that predispose the geriatric population to cutaneous fungal infections, including age-associated decrease in immunity, vitamin deficiency, peripheral vascular disease, broad-spectrum antibiotic use for other infections, lymphoproliferative disorders, and malignancies. Dermatophytes, a type of fungi that requires keratin for growth, can cause superficial infections such as tinea capitis, tinea corporis, tinea pedis, and tinea unguium. Tinea pedis affects approximately 80% of patients older than 60 years age and in elderly persons with diabetes, it is often complicated by ulceration and cellulitis.95 Candida albicans, a type of yeast that is part of the body’s normal flora, is another frequent source of cutaneous infections in the elderly. Pityrosporum ovale may cause seborrheic dermatitis, tinea versicolor, and Pityrosporum folliculitis, conditions that frequently affect older patients. Antifungals are effective for the geriatric population, but have to be used with caution because of possible drug interactions and underlying disorders.
VIRAL96
VIRAL
96
Herpes zoster, commonly known as shingles, is a cutaneous viral disease that primarily affects elderly patients. It is characterized by painful vesicular rash in a dermatomal distribution and is often preceded by pain in the affected area. Herpes zoster is caused by the reactivation in adults of the varicella-zoster virus (VZV), which is the virus that causes chickenpox in children. Age-related changes in immunity may be responsible for the failed suppression of VZV in the elderly. Current treatment includes antivirals like acyclovir, famciclovir, and valacyclovir. There is also a live, attenuated VZV vaccine and a recently approved recombinant zoster vaccine available.97 Pain can persist following an acute attack of herpes zoster. This is known as postherpetic neuralgia and is treated with topical anesthetics, analgesics, tricyclic antidepressants, and anticonvulsants. The VZV vaccine provides protection against herpes zoster for at least 3 years and reduce the incidence of postherpetic neuralgia by 66.5%.98
Infections caused by herpes simplex virus, which are characterized by vesicular eruptions in the genital and perioral regions, are also of clinical importance for the geriatric population. The vermilion border of the lip is the most frequent site of herpes simplex virus infection in older individuals. Recurrent herpes labialis in the geriatric patient can result in autoinoculation of the eye and genital area and subsequent spread of
1787
19
the disease. Similar to VZV infections, herpes simplex virus infections can be treated with antivirals including acyclovir, famciclovir, and valacyclovir.
ULCERS
Compromised wound repair capacity and comorbidities like diabetes mellitus and atherosclerotic peripheral vascular disease predispose the geriatric population to the development of chronic ulcers, particularly leg ulcers. Chronic venous insufficiency can lead to venous hypertension, resulting in the leakage of fibrinogen and other macromolecules into the dermis that can block the normal flow of oxygen, nutrients, growth factors, and cytokines, all of which are vital to tissue health and wound healing. Lipodermatosclerosis, a type of lower-extremity panniculitis, can develop and further impede wound repair. It is characterized by indurated skin with brownish-red pigmentation and is associated with tissue hypoxia, cytokine activation, and interstitial protein exudates.99 The elderly are also more prone to develop decubitus ulcers than younger patients. This is because of age-related skin atrophy from constitutive elevation in MMPs and concomitant decline in collagen synthesis by dermal fibroblasts.48 Furthermore, decline in physical mobility, urinary and fecal incontinence, and malnutrition all contribute to the ulcer formation in the elderly.100
SENILE PURPURA (BATEMAN PURPURA)
Senile purpura is the recurrent formation of ecchymoses on the sun-exposed extensor surfaces of the arms or hands of elderly patients. Age-related skin thinning and sun-induced damage of the connective tissue of the dermis results in inadequate support and increased fragility of the microvasculature. As a result, minor trauma of aged photodamaged skin can lead to vessel rupture and extravasation of blood into the dermal tissues.38 This condition can be exacerbated with the use of aspirin and other anticoagulants, medications that are common in the elderly population. Blood is typically resorbed within 2 weeks, but postinflammatory hyperpigmentation may occur. Although benign and self-resolving, senile purpura is of great cosmetic concern with a significant impact on patient well-being.
BULLOUS PEMPHIGOID
Bullous pemphigoid is an autoimmune blistering disorder that primarily affects patients older than 60 years of age. The initial manifestation can be urticarial papules and plaques with significant pruritus that subsequently progress into large tense bullae. The formation of autoantibodies that target the basement membrane leads to the separation of the dermal–epidermal junction. Certain risk factors for bullous pemphigoid have been identified and include
1788
neurologic disorders (eg, dementia and Parkinson disease), psychiatric disorders, bedridden condition, and chronic polypharmacy.101 Mortality in bullous pemphigoid cases is associated with increased disease severity and can occur as a result of therapies.102
DRUG ERUPTIONS
Adverse cutaneous drug reactions, such as morbilliform and urticarial eruptions, are frequent in the elderly and can have a significant impact on quality of life. Furthermore, older patients are more likely to develop drug-induced autoimmune reactions, like bullous pemphigoid (described before), lupus erythematosus, and pemphigus. One reason for increased risk of drug eruptions is polypharmacy. Additionally, renal, cardiac, and liver functions decline with age, which negatively impact drug metabolism and excretion. Thus, appropriate consideration and follow up when prescribing new medications, as well as frequent evaluation of existing medications is advised for the geriatric population.103

Figure 106-1 Difference between photoprotected and photoexposed skin.
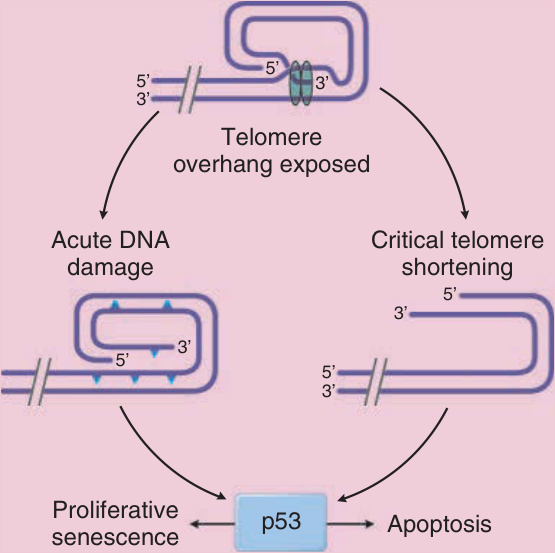
Figure 106-2 Schematic of cellular responses induced by exposure of the telomere repeat sequence. (From Yaar M. Clinical and histological features of intrinsic versus extrinsic skin aging. In: Gilchrest BA, Krutmann J, eds. Skin Aging. New York, NY: Springer; 2006:9-21, with permission. Copyright © 2006.)
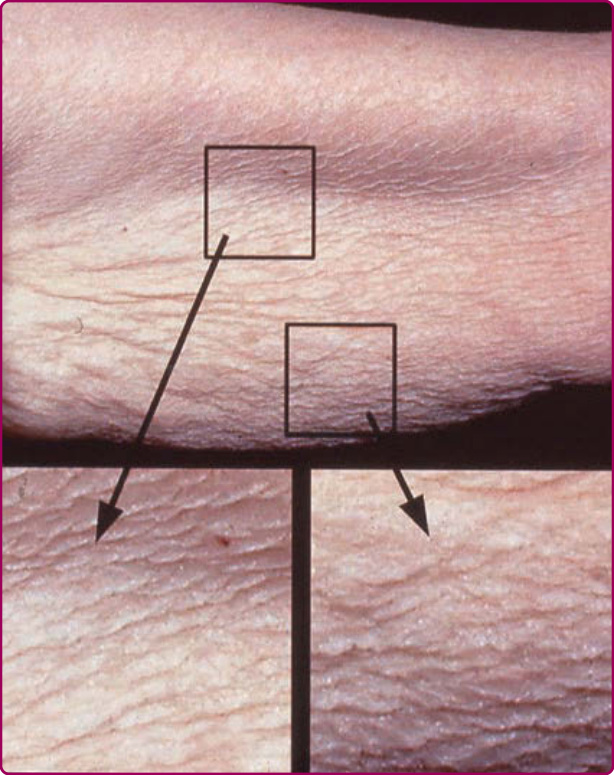
Figure 106-3 Intrinsic aging (upper inner arm): Intrinsic aging is characterized by fine wrinkling, increased skin laxity, and sagging.

Figure 106-4 Photoaging aging (face): The photograph highlights salient features of photoaging including fine and coarse wrinkles, discrete tan-brown macules, mottled pigmentation, telangiectasias, loss of translucency and elasticity, xerosis, and sallow color.

Figure 106-5 Solar lentigo: discrete tan, brown macules on photoexposed site. (Image from the Graham Library of Wake Forest Department of Dermatology, with permission.)
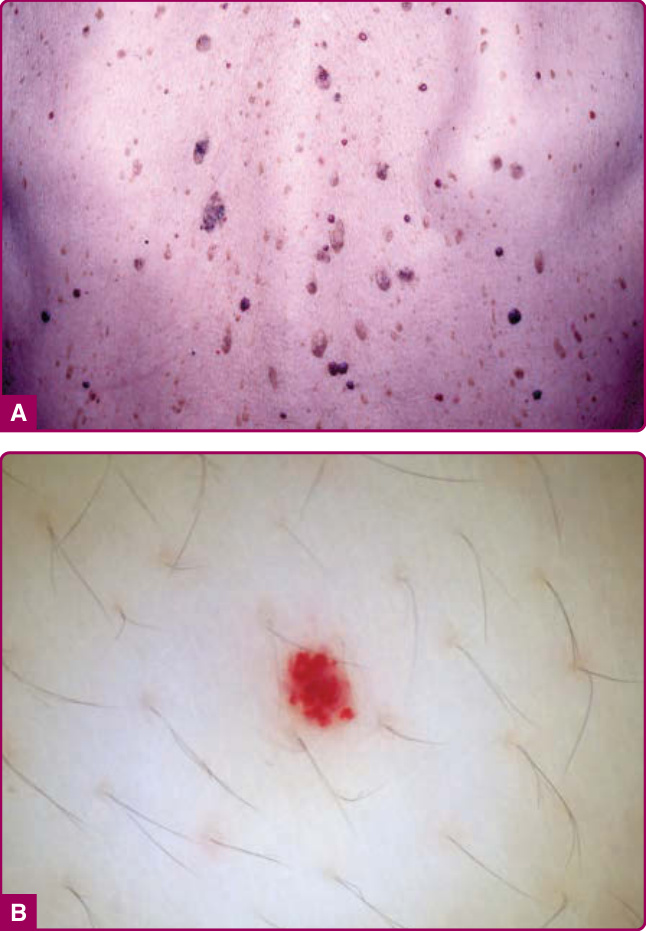
Figure 106-6 A, Seborrheic keratoses: brown, waxy, stuckon papules and plaques and B, Senile angioma: erythematous to violaceous lobulated papules. (Image B, used with permission from Dr. Willy Huang.)

Figure 106-7 Angiosarcoma: Angiosarcomas in the elderly typically occur on head and neck, characterized by enlarging nonblanching violaceous patch or deeply violaceous nodule with ulceration and tenderness.

Figure 106-8 Asteatotic eczema (“eczema craquelé”): minimally erythematous scaly plaques with fissures on background of xerosis. (Image from the Graham Library of Wake Forest Department of Dermatology, with permission.)
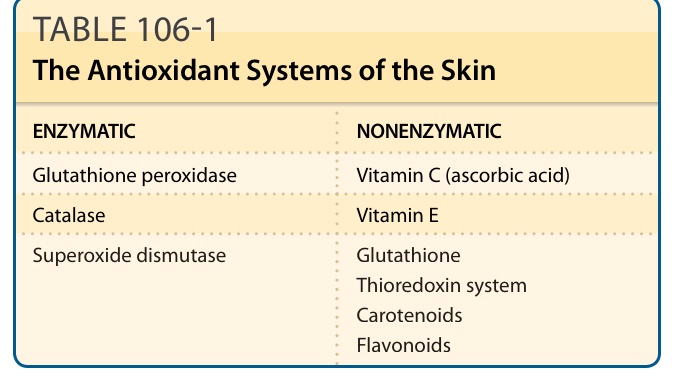
TABLE 106-1 The Antioxidant Systems of the Skin
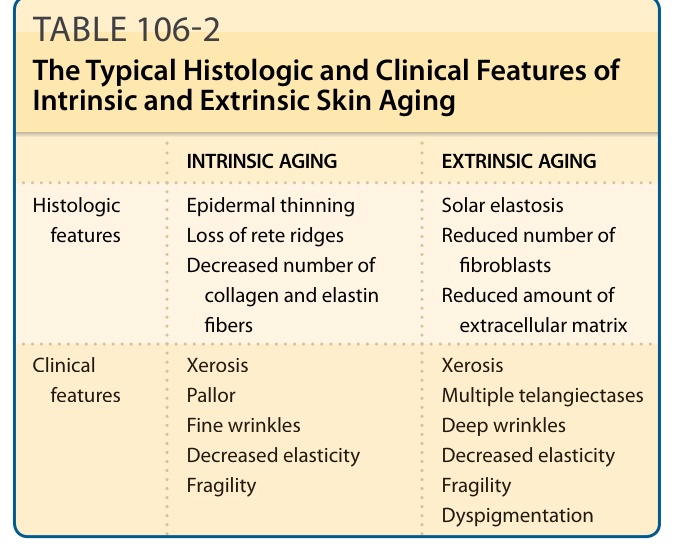
Table 106-2 summarizes the histologic and clinical features that are typical of intrinsically and extrinsically aged skin.
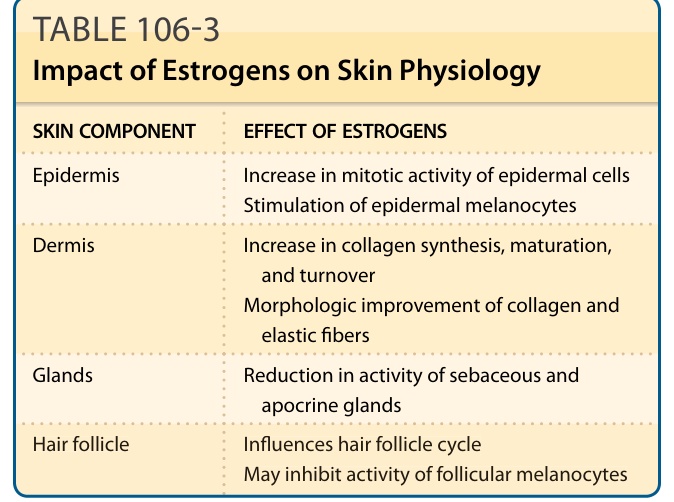
TABLE 106-3 Impact of Estrogens on Skin Physiology
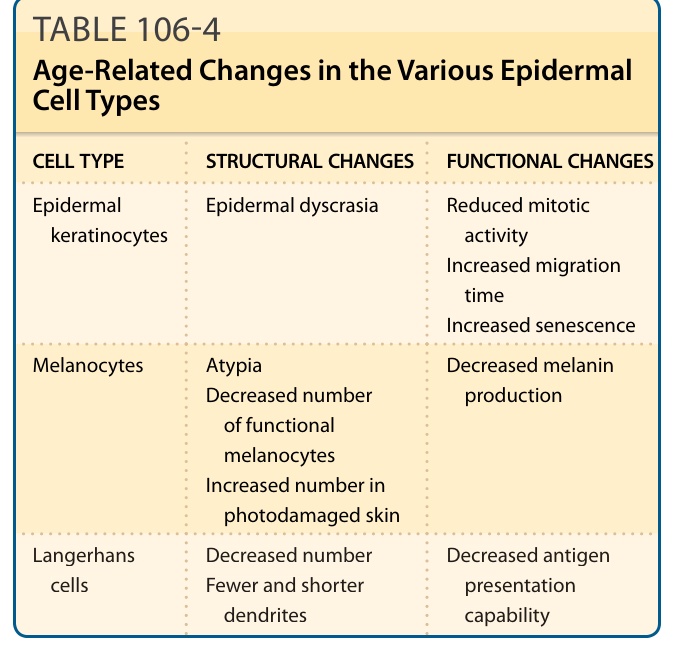
TABLE 106-4 Age-Related Changes in the Various Epidermal Cell Types
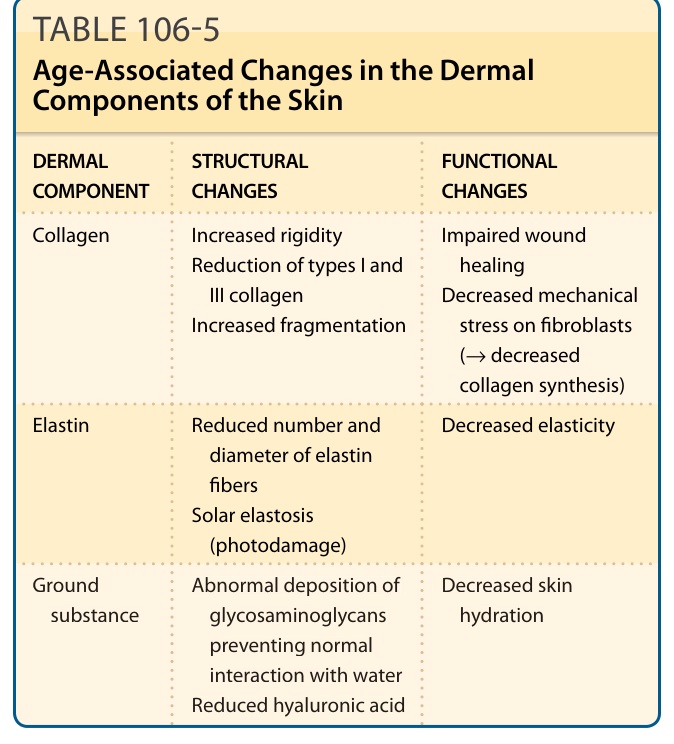
TABLE 106-5 Age-Associated Changes in the Dermal Components of the Skin