Neonatal Dermatology
PART19
Skin Changes Across the Span of Life
AT-A-GLANCE
■ Many dermatologic diseases exhibit different manifestations in newborns, infants, and children, and a subset of skin conditions are only encountered in neonates.
■ Certain neonatal skin conditions require special attention as they may be a sign of a serious health condition.
■ The medical history and methods of clinical examination in neonates differ from the approaches used with older children and adults. It is very important to elicit a thorough maternal and obstetric history with an emphasis on maternal health and any complications during pregnancy or delivery.
■ The neonate has increased risk for systemic toxicity from topically applied substances; the risk is even greater in premature infants.
Neonatal skin diseases are a fascinating and unique spectrum of dermatologic conditions. They encompass a broad range of diagnoses, including manifestations of neonatal or maternal infection, developmental defects, cutaneous features of genetic disorders, birthmarks, malignancy, complications of prematurity, and benign transient clinical findings. An understanding of benign cutaneous conditions of newborns and an ability to identify more worrisome presentations are essential to the care of the neonate. Appropriate care of the neonatal patient requires a thorough understanding of the maternal health history, including maternal disease as well as pregnancy complications.
NEONATES
The neonatal period is defined as the first 30 days of life. Infancy is defined as beginning after the first 30 days of life. Although this chapter focuses on conditions presenting in the neonatal period, some conditions may occur in infancy as well. Even though many neonatal skin diseases are benign and self-limiting, serious disease may occur, and cutaneous manifestations of systemic disease or an associated genetic syndrome should not be overlooked. Full-term infants are born between 37 and 42 weeks of gestation. Preterm or premature infants are born before 37 weeks of gestation.
NEONATAL SKIN
NEONATAL SKIN PHYSIOLOGY
NEONATAL SKIN
PHYSIOLOGY
The skin with its associated appendages provides several important functions. It serves as a barrier against microbes and environmental and other external toxins, provides thermoregulation, prevents transepidermal water loss, and aids in sensory perception. Knowledge of normal embryologic development and the physiology of neonatal skin is helpful for understanding the adaptive changes that occur after birth and for guiding appropriate skin care in both full-term and preterm neonates. The epidermis begins to develop around 6 weeks of gestational age as a basal cell layer and a superficial periderm layer; the periderm does not contribute to the formation of the stratified squamous epithelium and is shed during the end of the second trimester.1 Stratification of the fetal epidermis begins in the eighth week of gestation; terminal differentiation commences first in
19
the skin appendages between the 11th and 15th weeks of gestation and then in the interfollicular epidermis; by 22 to 24 weeks of gestation the epidermis consists of 4 to 5 cell layers.2,3 The dermal–epidermal junction is evident by 8 weeks of gestational age, and collagen fiber formation and organization of the papillary and reticular dermis occurs by 15 weeks of gestation; elastic fibers are noted at 22 to 24 weeks of gestation.4,5
Hair follicles begin to develop around the 14th week of gestation; lanugo hair production begins around the 18th week of gestation and is complete by the 28th week of gestation.6,7 Eccrine gland development is completed during the second trimester, although the eccrine glands are not functional until after birth. Apocrine gland formation occurs somewhat later in fetal development, and the apocrine glands are transiently functional during the third trimester of pregnancy. Sebaceous gland formation begins around the 16th week of gestation, and the sebaceous glands are functional shortly after formation; sebaceous gland products contribute significantly to the lipid composition of vernix caseosa.8,9
In utero, the skin of the fetus is protected by the vernix caseosa and is immersed in amniotic fluid. Vernix production correlates with epidermal maturation and the formation of the stratum corneum; production begins around the 36th week of gestation. Vernix caseosa is composed of water-containing corneocytes in a lipid matrix composed predominantly of nonpolar lipid such as sterol esters and triglycerides.9,10 It provides antimicrobial, antioxidant, and barrier functions, and contains multiple antimicrobial peptides, including LL-37, cystatin A, and calgranulins.11,12 After birth, the vernix is often manually removed and the skin exposed to room air, although some experts question the validity of this practice. Of particular interest is the development of the epidermal barrier, including postnatal development of barrier function in term and preterm neonates.13 After birth, the skin of the neonate undergoes a series of changes in adaptation to the extrauterine terrestrial environment. Additional maturation of the stratum corneum in neonates occurs in response to air, which contributes to the development of a functional epidermal barrier. It is generally accepted that full barrier function is achieved within 2 to 4 weeks of life in term neonates, and some experts believe that the barrier is fully developed at birth in this population.14 In preterm infants, the epidermal barrier in immature. Barrier stabilization is a dynamic process dependent upon a balance between several biologic and environmental factors. Evaluation of parameters such as skin thickness, skin pH, transepidermal water loss (TEWL), and stratum corneum hydration indicate that neonatal skin undergoes continuous adjustment to the extrauterine environment. In full-term neonates, after drying of the skin in the first few hours after birth, TEWL is equivalent to that seen in adults, with the exception of some variability because for site and ambient temperature and/or humidity, including the diaper area, where TEWL vales are higher and contribute to impaired barrier function and risk for diaper dermatitis.15,16
1728
One of the most visible early manifestations of the adaptive process is desquamation of the upper layers of the stratum corneum, which occurs in all infants. Postterm infants born after 40 weeks of gestation have decreased amounts of vernix caseosa on the skin and more notable desquamation (Fig. 103-1). During the first 3 months of life, the thickness of the stratum corneum decreases, and epidermal thickness increases, along with the formation of dermal papillae and epidermal ridges.17
Normal skin pH is acidic; the acidic pH of the stratum corneum results from multiple factors, including the production of free fatty acids from phospholipids and the presence of sweat and sebum.18 In the term and preterm neonate, skin pH is more alkaline than that of older infants and adults, and it decreases gradually over the first few weeks of life.19-21
Sebum production is high in the neonate, and decreases over the first few months of life.22 Eccrine sweating is present in term neonates, but delayed in preterm neonates.23,24
PREMATURITY
PREMATURITY
Premature neonates, particularly those born before 34 weeks of gestation, have markedly decreased epidermal barrier function. The functional maturation of the stratum corneum begins around 24 weeks of gestational age, and in preterm neonates born before 26 weeks of gestation, functional maturation of the epidermal barrier may take longer than 4 weeks.25,26 TEWL is significantly increased in preterm and
low-birthweight neonates, reflecting epidermal barrier immaturity, and TEWL increases with decreasing gestational age.27 Use of radiant warmers and phototherapy also contribute to increased TEWL.28,29 Impaired epidermal barrier function places the preterm infant at risk for electrolyte imbalances, poor thermoregulation, dehydration, increased absorption of topical agents, and infection. Increased skin fragility is also noted in preterm infants. Epidermal and dermal injury may lead to significant cutaneous pain even with routine handling and nursing care. The premature infant is at risk for infection and sepsis from skin-associated organisms entering through breaks in the thin and fragile skin and via iatrogenic portals of entry such as indwelling venous catheters. Thermal regulation is dysfunctional because of a thin subcutaneous fat layer, decreased ability to sweat, poor autonomic control of cutaneous blood vessels, and a large surface-area-to-body-mass ratio. In the nursery, the premature infant is usually placed in a temperature- and humidity-controlled isolette until temperature and fluid regulation stabilize. In the 1990s, researchers reported that application of petrolatum-based emollient therapy appeared to be beneficial by decreasing TEWL in hospitalized preterm infants.30 Subsequently, many neonatal intensive care units began to implement the use of various emollients and skin-care regimens. However, while skin integrity consistently improved, a threefold increase in the incidence of systemic candidiasis was reported after emollient therapy was implemented in extremely low-birthweight (≤1000 g) premature infants in one neonatal intensive care unit.31 Similarly, an outbreak of systemic candidiasis occurred in very-low-birthweight neonates (≤1500 g) using emollient therapy in a different neonatal intensive care unit.32 A 2004 Cochrane review concluded that prophylactic application of topical ointments increased the risk for nosocomial infection and advised against their routine use in preterm infants. In contrast, randomized, controlled studies in a population of impoverished Bangladeshi preterm neonates have demonstrated decreased mortality rates when sunflower seed oil or Aquaphor ointment was applied by massage, compared to premature infants not receiving massage or emollients, suggesting that in certain populations, such as those without access to sophisticated neonatal intensive care practices, use of emollients may be beneficial in high-risk preterm infants.33 A 2016 Cochrane review concluded that the use of topical emollients in preterm infants did not prevent invasive infection or death.34 Until prospective, controlled trials are performed, neonates receiving petrolatum-based emollient therapy should be carefully monitored for infections, particularly those infants with birthweights less than 1500 g.
SKIN CARE IN THE NEONATE
SKIN CARE IN THE NEONATE
Recommendations for routine skin care in the neonate, as provided by a panel of European experts, include
19
bathing in water 2 to 3 times per week for no more than 5 to 10 minutes with use of a gentle soap-free liquid skin cleanser as opposed to a washcloth; application of an emollient after bathing is also recommended.35
An appropriate skin-care regimen serves to minimize overbathing, maintain the epidermal barrier, minimize exposure to potential irritants or allergens, and remove fecal material. Well-meaning parents often bathe their infants too frequently and use a multitude of products on their infant’s skin. In addition to irritation and asteatosis, these practices may increase the risk of allergic contact dermatitis in infants. It has been estimated that the average newborn is exposed to approximately 10 skin care products in the first month of life, leading to exposure to more than 50 different chemicals, ranging from mildly toxic to toxic.36 Parents should be taught that “less is best.”37 Use of a skin cleanser in healthy, term infants has been shown to have no effect on TEWL, skin surface pH, and stratum corneum hydration, as compared to bathing with water alone.38 Skin care in full-term neonates from birth to 8 weeks of age with cleansing gel, gel plus cream, water alone, or water plus cream showed no significant differences in skin condition, microbial colonization, and sebum level.39,40
Neonates have an increased risk for systemic toxicity from topically applied substances. This is largely a result of the greater surface-area-to-body-mass ratio in the newborn. Preterm neonates have an even greater surface-area-to-body-mass ratio than term neonates. In addition, the metabolism, excretion, distribution, and protein binding of substances can differ significantly in neonates as compared to adults, which increases the risk of toxicity; these adverse effects may be magnified in the preterm neonate. Local or systemic toxicity can occur in the term or preterm neonate not only from topical medications, but also from soaps, lotions, and other cleansing solutions. Neonates with disorders of skin-barrier function, such as congenital ichthyosis, are at increased risk for systemic absorption of topical medications and chemicals.41
EXAMINATION TECHNIQUES
For the neonate, a complete medical history includes gestational and birth history as well as family history. Exposures during pregnancy, including medications, illicit drugs, and infectious diseases, such as varicella, rubella, or sexually transmitted diseases, are important to review in detail. Additionally, other complications of pregnancy and parturition and the appearance of the placenta offer useful clinical information. Comprehensive examination of the skin of a neonate in good lighting is valuable, particularly as some skin findings are initially subtle. For example, a vasoconstricted macule or an erosion can be the presenting sign of an infantile hemangioma.42 All congenital lesions (eg, pigmented lesions, vascular birthmarks, aplasia cutis, cutaneous nodules) warrant thorough
1729
19
evaluation to help exclude associated syndromes or internal disease. Biopsy should be considered when the diagnosis is unclear and the outcome will impact management. Midline face, scalp, or spine lesions may be associated with CNS connections and should be imaged to rule out CNS communication prior to performing a skin biopsy. The newborn is completely dependent on caretakers, and the family structure and social support network should be considered when developing treatment plans. Some new parents may feel overwhelmed or unprepared to deal with a skin condition in their infant. At times, the treatment priorities of the parents may not seem to coincide with the best interests of the newborn at this early stage in their development. Medical and surgical decision making for affected infants is typically aimed at improving function in favor of cosmesis.
DISEASES OF NEONATES
TRANSIENT DERMATOSES OF THE NEONATE
TRANSIENT DERMATOSES OF
THE NEONATE
Benign skin conditions encountered in newborns that tend to resolve by 30 days of age are considered to be transient. They are very common, and the majority do not require intervention. These conditions are discussed below, and Table 103-1 lists a selected differential diagnosis based on broad categories of skin lesions encountered in neonates and infants.
CAPUT SUCCEDANEUM AND CEPHALOHEMATOMA
Trauma during delivery may induce one of several injuries to the scalp of the neonate.43 These range from common and usually benign conditions such as caput succedaneum and cephalohematoma to subgaleal hemorrhage, which is a serious, potentially lifethreatening condition. Caput succedaneum results from subcutaneous edema over the presenting part of the head owing to pressure against the cervix and is a common occurrence in newborns. Caput succedaneum is soft to palpation with ill-defined borders. Petechiae and ecchymosis also may be noted. The edema resolves spontaneously over 7 to 10 days. Cephalohematoma results from rupture of the diploic and/or emissary veins and subsequent subperiosteal collection of blood. It is associated with birth trauma or the use of vacuum extraction vaginal delivery. Areas of hemorrhage respect the suture lines, are well-delimited, usually unilateral, and feel firm to palpation. An underlying skull fracture may be present. Cephalohematomas usually resolve without sequelae over several weeks, but calcification may occur. Subgaleal hemorrhage is also associated with birth trauma and occurs when there is bleeding between
1730
■Pustules
■Pustules
■Erythema toxicum neonatorum
■Erythema toxicum neonatorum
■Transient neonatal pustular melanosis
■Transient neonatal pustular melanosis
■Congenital candidiasis
■Congenital candidiasis
■Pustular psoriasis
■Pustular psoriasis
■Langerhans cell histiocytosis
■Langerhans cell histiocytosis
■Neonatal cephalic pustulosis
■Neonatal cephalic pustulosis
■Bacterial sepsis
■Bacterial sepsis
■Herpes simplex infection
■Herpes simplex infection
■Blisters
■Blisters
■Sucking blisters
■Sucking blisters
■Herpes simplex virus
■Herpes simplex virus
■Aplasia cutis congenita
■Aplasia cutis congenita
■Cutaneous mastocytosis
■Cutaneous mastocytosis
■Epidermolysis bullosa
■Epidermolysis bullosa
■Neonatal pemphigus
■Neonatal pemphigus
■Varicella
■Varicella
■Impetigo
■Impetigo
■Incontinentia pigmenti
■Incontinentia pigmenti
■Epidermolytic ichthyosis
■Epidermolytic ichthyosis
■The red scaly baby
■The red scaly baby
■Physiologic scaling and redness (postdates) infant
■Physiologic scaling and redness (postdates) infant
■Psoriasis
■Psoriasis
■Atopic dermatitis
■Atopic dermatitis
■Scabies
■Scabies
■Seborrheic dermatitis
■Seborrheic dermatitis
■Immunodeficiency
■Immunodeficiency
■Hypohidrotic ectodermal dysplasia
■Hypohidrotic ectodermal dysplasia
■Netherton syndrome
■Netherton syndrome
■Acrodermatitis enteropathica
■Acrodermatitis enteropathica
■The collodion baby
■The collodion baby
■Lamellar ichthyosis
■Lamellar ichthyosis
■Congenital ichthyosiform erythroderma
■Congenital ichthyosiform erythroderma
■Gaucher syndrome
■Gaucher syndrome
■Trichothiodystrophy
■Trichothiodystrophy
■Neutral lipid storage disorder
■Neutral lipid storage disorder
■The “blueberry muffin” baby
■The “blueberry muffin” baby
■TORCH infections
■TORCH infections
■Congenital leukemia
■Congenital leukemia
■Congenital self-healing reticulohistiocytosis
■Congenital self-healing reticulohistiocytosis
■Blue rubber bleb nevus syndrome
■Blue rubber bleb nevus syndrome
■Twin–twin transfusion
■Twin–twin transfusion
TORCH, toxoplasmosis, other agents, especially syphilis, but also hepatitis B, coxsackievirus, Epstein-Barr virus, varicella-zoster virus, and human parvovirus, rubella, cytomegalovirus, herpes simplex virus.
the periosteum of the skull and the galea as a result of damage to the emissary veins. Extensive hemorrhage may occur with either subgaleal hemorrhage or cephalohematoma, and may lead to anemia and neonatal hyperbilirubinemia. With a subgaleal hemorrhage, bleeding can be catastrophic and result in hypovolemic shock or disseminated intravascular coagulation.
MILIA
Milia are pinpoint to 2-mm papules representing benign, superficial epidermal inclusion cysts. Usually few in number, they are seen most commonly on the
face in newborns and may be present in the oral cavity as well, where they are called Epstein pearls. Congenital milia en plaque also has been reported.44 Milia generally resolve spontaneously within a few weeks of life. When persistent and/or numerous, they may be seen in association with several rare genetic disorders, including oral-facial-digital syndrome, Bazex-Dupré- Christol syndrome, and Basan syndrome.
SEBACEOUS GLAND HYPERPLASIA
At least 50% of normal newborns have sebaceous gland hyperplasia (Fig. 103-2). Minute (<1 mm) yellow macules or papules are commonly seen at the opening of pilosebaceous follicles over the nose and central forehead of term newborns. This is a benign condition thought to occur secondary to maternal androgen stimulation of the sebaceous glands; it typically resolves spontaneously by 4 to 6 months of age.
ERYTHEMA TOXICUM NEONATORUM
Erythema toxicum neonatorum is an idiopathic, common skin condition seen in up to 75% of term newborns. It is rarely seen in premature infants. Blotchy erythematous patches 1 to 3 cm in diameter with a 1- to 4-mm central vesicle or pustule are characteristic of erythema toxicum neonatorum (Fig. 103-3). The eruption usually begins at 24 to 48 hours of age, but delayed eruption as late as 10 days of age has been documented.45 These follicular-based lesions can be located anywhere but tend to spare the palms and soles. A smear of the central vesicle or pustule contents will reveal numerous eosinophils on Wright-stained preparations. A peripheral blood eosinophilia of up to 20% may be associated, particularly in infants, with
19
numerous lesions. Erythema toxicum neonatorum is benign and clears spontaneously by 2 to 3 weeks of age without residua.
TRANSIENT NEONATAL PUSTULAR MELANOSIS
Transient neonatal pustular melanosis is an idiopathic pustular eruption of the newborn that resolves with hyperpigmented macules (Fig. 103-4). It is less common than erythema toxicum neonatorum and is more prevalent among newborns with darkly pigmented skin. Lesions are usually present at birth or shortly thereafter, but may appear as late as 3 weeks of age. The eruption is characterized by multiple superficial vesicles and pustules, with ruptured lesions evident as collarettes of scale. Hyperpigmented macules are also often present at birth or develop at the sites of resolving pustules or vesicles within several hours of birth or during the first days of life. Lesions can occur anywhere but are common on the forehead and mandibular area. The palms and soles may be involved. Smear of the vesicle or pustule contents will reveal a predominance of neutrophils with occasional eosinophils on Wright-stained preparations. The pustules usually disappear within 5 to 7 days; residual pigmented macules resolve over several weeks.
MILIARIA RUBRA AND CRYSTALLINA
Miliaria or “heat rash” is a common disorder of the eccrine glands that typically results from fever or overheating such as may occur when neonates are swaddled. Eccrine gland occlusion by sweat and possibly by the extracellular polysaccharides of Staphylococcus
1731
19
A
B
epidermidis leads to the development of minute superficial subcorneal vesicles (miliaria crystallina). A deeper level of occlusion within the epidermis with associated inflammation leads to miliaria rubra, which manifests as 1- to 3-mm erythematous papules and/or papulopustules. The condition resolves spontaneously once the inciting factors are addressed.
MOTTLING AND CUTIS MARMORATA
Mottling is a blotchy or lace-like pattern of dusky erythema over the extremities and trunk of neonates that occurs with exposure to cold environments. Virtually all babies demonstrate mottling at some time during the newborn period as a consequence of immature
1732
autonomic control of the cutaneous vascular plexus. This physiologic mottling disappears on rewarming, differentiating it from cutis marmorata telangiectatica congenita and livedo reticularis. Physiologic mottling resolves spontaneously by 6 months of age.
HARLEQUIN COLOR CHANGE
Harlequin color change is a rare vascular phenomenon that occurs in in full-term newborns, as well as in low-birthweight and premature infants, and in infants exposed to hypoxia or systemic treatment with prostaglandins. In harlequin color change, when the neonate is placed on one side, an erythematous flush with a sharp demarcation at the midline develops on the dependent side, and the upper half of the body becomes pale. The color change usually subsides within a few seconds of placing the baby in the supine position but may persist for as long as 20 minutes. Presentation may be localized to a single body area or may be more generalized. The exact mechanism of this unusual phenomenon is not known, but it may be a result of immaturity of autonomic vasomotor control.46 Harlequin color change is seldom seen after 10 days of age, and if noted to be persistent or to develop at an older age, may be a manifestation of an underlying neurologic disorder.
SUCKING BLISTERS
Sucking blisters may be present at birth as the result of intrauterine sucking, but are more commonly seen during the first weeks of life. Sucking blisters are usually solitary, intact, oval or linear blisters, superficial erosions, or crusts, arising on noninflamed skin on the dorsal aspect of the forearms, wrists, or fingers; a callus may be noted on the upper lip. They resolve within a few days. If the affected extremity is brought up to the infant’s mouth, the infant will often commence sucking at the site, confirming the diagnosis.
BENIGN NEONATAL CEPHALIC PUSTULOSIS
Neonatal acneiform facial eruptions usually develop within the first 30 days of life and are estimated to occur in 50% of newborns (Fig. 103-5). Neonatal cephalic pustulosis is most common, and has been attributed to overgrowth of Malassezia spp.47,48 Most cases resolve spontaneously, but the eruption can be treated topically with ketoconazole. True infantile acne is less common and can be distinguished by later age of onset and the presence of comedones, acneiform cysts, and scars (Fig. 103-6).
BIRTHMARKS
BIRTHMARKS
Birthmarks are common in newborns, and range from common, benign conditions such as nevus simplex
and dermal melanocytosis to more worrisome conditions such as large segmental hemangiomas and giant congenital melanocytic nevi. Although most birthmarks are of little medical or psychosocial consequence, the social and cultural impact of a disfiguring birthmark on both the patient and the parents should not be underestimated.49 Table 103-2 lists common birthmarks.
PIGMENTARY BIRTHMARKS Dermal Melanocytosis: Dermal melanocytosis (commonly called “Mongolian spots”) is characterized by blue-gray patches typically located on the lumbosacral or buttock skin of infants. Collections of dermal melanocytes cause these common birthmarks, which are seen in 80% to 90% of infants of color and only 5% of white infants.50,51
Café-au-Lait Macules: Café-au-lait macules are well-demarcated tan macules or patches. Solitary café-au-lait macules are very common, however, the presence of multiple café-au-lait macules raises the possibility of neurofibromatosis type 1 (see Chap. 135). It is important to remember that findings of neurofibromatosis type 1 are progressive, so a potential
19
■Dermal melanocytosis (commonly called “Mongolian spots”)
■Dermal melanocytosis (commonly called “Mongolian spots”)
■Nevus simplex (salmon patch, “stork bite,” “angel’s kiss”)
■Nevus simplex (salmon patch, “stork bite,” “angel’s kiss”)
■Port-wine stain (capillary malformation)
■Port-wine stain (capillary malformation)
■Infantile hemangioma
■Infantile hemangioma
■Epidermal nevus and nevus sebaceus
■Epidermal nevus and nevus sebaceus
■Congenital melanocytic nevi
■Congenital melanocytic nevi
■Nevus depigmentosus
■Nevus depigmentosus
■Café-au-lait spots
■Café-au-lait spots
neurofibromatosis type 1 diagnosis cannot be excluded based on neonatal examination of an infant with 1 or a few café-au-lait macules. Less-common genetic disorders are also associated with multiple café-au-lait macules. A large, geographic café-au-lait macule with a “coast-of-Maine” appearance is most likely to be an isolated skin finding but may be a marker for McCune- Albright syndrome.
Congenital Melanocytic Nevi: Melanocytic nevi that are present at birth or that appear within the first few months of life are “classic” congenital melanocytic nevi (CMN). Additionally, “late-onset” or “tardive” CMN may appear any time before age 2 years, and both are considered to be programmed from birth. CMN are typically barely elevated melanocytic papules or plaques that range in color from light brown to very dark brown or black. Some CMN have well-demarcated, geographic borders, and internal speckled patterns may be seen. CMN enlarge proportionately as children grow. It is estimated that the size of CMN between infancy and adulthood will increase 1.7-fold on the head, whereas CMN on the lower extremities will increase 3.3-fold, and CMN of other sites will increase 2.8-fold. CMN are classified based on projected adult size into the following categories: small (<1.5 cm); medium (M1 1.5 to 10 cm, M2 >10 to 20 cm); large (L1 >20 to 30 cm, L2 >30 to 40 cm); and giant (G1 >40 to 60 cm, G2 >60 cm).52
Large and giant CMN are associated with an increased risk of melanoma. Additionally, individuals with large or giant CMN may be at risk for complications of neurocutaneous melanocytosis, particularly if the large or giant CMN has a posterior axial location or if more than 20 satellite nevi are present. Newborns with more than 2 medium-sized CMN are also at increased risk of neurocutaneous melanocytosis. Neurocutaneous melanocytosis results from abnormal melanocytic proliferations in the CNS, and can be complicated by obstructive hydrocephalus and primary CNS melanoma.
Pigmentary Mosaicism: Pigmentary mosaicism (patterned dyschromatosis) refers to areas of skin hypopigmentation or hyperpigmentation that are genetically determined by late somatic mosaic genetic mutations in skin cell progenitors. The dyschromia in pigmentary mosaicism tends not to cross the midline
1733
19
of the body. Altered pigmentation may be curvilinear along Blaschko lines, or may manifest with checkerboard, phylloid, or patchy patterns.53 In most cases, pigmentary mosaicism is an isolated finding, but the practitioner should maintain high suspicion for associated disease in children with widespread skin dyschromia, associated neurologic, cardiac, or musculoskeletal disease, or in children who are delayed in accomplishing expected developmental milestones.54
Nevus Depigmentosus: Nevus depigmentosus is a well-demarcated hypopigmented patch present from birth, which may sometimes become more visible in the first year of life as the background skin pigmentation of the newborn gradually increases. Three or more nevus depigmentosus/hypomelanotic patches in a newborn should prompt evaluation for possible tuberous sclerosis complex.55
Nevus Anemicus: Nevus anemicus describes a hypopigmented patch that results from focal vasoconstriction. It is attributed to skin vessel hypersensitivity to catecholamines in the affected areas. Application of pressure with a glass slide (diascopy) across the edge of a nevus depigmentosus will blanch the normal skin surrounding the nevus depigmentosus by compressing local vessels and thus blur the border. Diascopy is helpful in distinguishing nevus anemicus from nevus depigmentosus (Table 103-3), as the border of a nevus depigmentosus remains crisp despite diascopy.
VASCULAR BIRTHMARKS
Vascular tumors and malformations may present during the neonatal period, and prompt diagnosis and differentiation of those that may be associated with systemic manifestations or complications allows for early intervention when needed.
Nevus Simplex: Nevus simplex represents a superficial vascular ectasia of the capillaries. It occurs most commonly on the glabella, upper eyelids, and nuchal area, and is colloquially termed “salmon patch,” “stork bite,” or “angel kiss.” Less-common areas include the lower back and scalp. Nevus simplex appears with high frequency in all races, occurring in 70% of white infants and in 59% of black infants. Although the majority of nevus simplex birthmarks fade over the first 2 years of life, those on the occipital
NEVUS ANEMICUS NEVUS DEPIGMENTOSUS
Pathology Focal vasoconstriction; skin vessel hypersensitivity to catecholamines
Hypomelanosis in affected site
Diascopy Borders of lesion disappear as a
Borders of lesion
Diascopy Borders of lesion disappear as a result of the blanching effect Borders of lesion remain crisp
1734
result of the blanching effect
remain crisp
scalp tend to persist. Nevus simplex should be differentiated from other capillary malformations and their associations, including nevus flammeus (port-wine stain).56,57 Vascular malformations are discussed in detail in Chap. 147.
Infantile Hemangiomas: Infantile hemangiomas are the most common tumors of infancy. They must be differentiated from vascular malformations and other vascular anomalies. Hemangiomas are discussed in detail in Chap. 118.
Vascular Malformations: Vascular malformations are a heterogeneous group of vascular dysplasias that encompass slow-flow malformations (eg, capillary, venous, and lymphatic malformations) and fastflow malformations (eg, arteriovenous malformations and complex combined malformations). Vascular malformations are discussed in detail in Chap. 147.
OTHER BIRTHMARKS Nevus Sebaceus: Nevus sebaceus is a benign skin hamartoma comprised of numerous sebaceous glands that most often appear as yellow-hued hairless plaque on the head of newborns. Around puberty, a nevus sebaceus may thicken and develop hyperkeratotic, verrucous features. Secondary benign neoplasms, including trichoblastoma or syringocystadenoma papilliferum, sometimes develop within a nevus sebaceus, and, uncommonly, basal cell carcinoma has been reported to arise within a nevus sebaceus.58,59 Lesions can be monitored or excised if they are symptomatic or cause disfigurement. Widespread nevus sebaceous skin lesions may be associated with increased risk of abnormalities in the central nervous, eye, or skeletal systems (Schimmelpenning or nevus sebaceus syndrome).60
Epidermal Nevus: Epidermal nevi appear as curvilinear arrays of tan-brown hyperkeratotic papules and/or thin, elongated rough plaques that follow the lines of Blaschko. Epidermal nevi are difficult to treat. Surgical excision may result in large scars which, in some locations, can restrict range of motion. Laser treatment and local dermal shave excision are associated with focal scarring and a high recurrence risk. Infants with widespread epidermal nevi may be at risk for epidermal nevus syndrome, and should be evaluated for associated disease of the central nervous, ocular, and skeletal systems.60
DEVELOPMENTAL ABNORMALITIES
Developmental anomalies of the skin and subcutaneous tissues and structures range from common, benign, minor findings, such as the supernumerary nipple, to major anomalies, such as aplasia cutis congenita, which can be markers for potentially serious underlying anomalies.
MINOR ANOMALIES
MINOR ANOMALIES
The supernumerary digit (Fig. 103-7), supernumerary nipple, and accessory tragus are common examples of minor anomalies of the skin and associated subcutaneous structures. Overall, single, minor congenital anomalies occur in approximately 15% of all newborns and have no functional significance. The occurrence of 2 minor congenital anomalies is less common; however, 3 or more minor congenital anomalies is unusual and warrants a complete thorough physical examination to rule out other congenital abnormalities.61,62
OTHER ANOMALIES
OTHER ANOMALIES
Other anomalies less frequently encountered in the neonate include dermoid cysts, aplasia cutis congenita, and branchial cleft cysts. Understanding which of these lesions imply possible risk of additional associated malformations is important for diagnosis and management. The skin and the nervous system are both derived from the embryonic ectoderm. The neural ectoderm separates from the epithelial ectoderm during the third to fifth week of gestation, occurring simultaneously with the formation and closure of the neural tube. Hence, errors in neural tube development (ie, dysraphism [incomplete fusion]) can be associated with cutaneous anomalies. Midline facial lesions, such as dermoid cysts can be markers of cranial dysraphism, whereas cutaneous anomalies involving the lumbosacral midline may indicate underlying spinal dysraphism. For midline nasal and facial lesions, radiologic evaluation is indicated to rule out intracranial connections before a skin biopsy is performed.63 Radiologic imaging should also be performed in the
19
presence of high-risk lumbosacral anomalies. The highest risk of occult spinal dysraphism occurs with the presence of 2 or more congenital midline lumbosacral skin lesions or if spinal cord dysfunction exists in the presence of 1 lumbar skin lesion.64,65 In addition, lumbosacral lipoma, human tail, and dermal sinus (as isolated findings) are highly associated with occult spinal dysraphism, and MRI is indicated when these high-risk congenital lesions are present. An intermediate risk of occult spinal dysraphism is associated with atypical sacral dimple (≥5 mm diameter, or location ≥2.5 cm away from the anus), aplasia cutis congenita, overlying hamartoma, or deviated gluteal cleft. In the presence of any of these lesions, ultrasonography can be used to screen for occult spinal dysraphism if the infant is younger than 4 months of age. If the infant is older, MRI is needed to rule out dysraphism. Low-risk lesions that do not require imaging include small, focal infantile hemangioma, capillary malformation, mild focal hypertrichosis, congenital melanocytic nevus, dermal melanocytosis, or simple sacral dimple with a visible base (≤5 mm diameter and location ≤2.5 cm from the anus). Figure 103-8 summarizes these findings. Neurosurgical consultation is advised for infants with an intracranial or spinal anomaly.
DERMOID CYSTS
Dermoid cysts are congenital anomalies that typically arise along planes of embryonic fusion of the face and scalp. Dermoid cysts are not always apparent at birth; when appreciated, they present as a firm nodule that may adhere to the underlying periosteum. Nasal dermoid cysts may be associated with a dermal pit or sinus and carry a significant risk for intracranial extension.66 Surgical excision is generally recommended; preoperative MRI should be considered to evaluate for deeper extension of midline dermoid cysts.67
NASAL GLIOMA
Nasal gliomas are composed of heterotopic neural tissue and present as firm, skin-colored to erythematous nodules on the nose (Fig. 103-9). They may distort the central facial structures. Referral to neurosurgery is indicated for surgical excision.
MENINGOCELE AND MYELOMENINGOCELE
A meningocele is formed when the meninges and cerebrospinal fluid herniate through a defect in the calvarium or vertebrae. A meningocele is a midline anomaly that may be associated with a persistent intracranial defect; as such, preoperative imaging is recommended prior to surgical excision and reconstruction. When neural tissue of the spinal cord is also present, the term myelomeningocele is used. Myelomeningocele is the most common presentation of spina bifida.
1735
19
Congenital lumbosacral midline skin lesions, required assessment, and risk of occult spinal dysraphism
Risk of Occult Spinal Dysraphism
Group 1
Group 2
Group 3
• Atypical sacral dimple (deep, farther than 2.5 cm from the anus, size ≥5 mm)
• Unclassified hamartoma
• Aplasia cutis congenital
• Deviation of gluteal crease
• Two or more lesions of any kind
• One lesion + spinal cord dysfunction
• Lipoma
• Tail
• Dermal sinus
• Port-wine stain
• Hypertrichosis (unless large and/or unusual)
• Pigmented nevus
• Simple sacral dimple (<5 mm diameter, 2.5 cm or closer to the anus)
• Mongolian spot
Ultrasonography if younger than age 4 months (then MRI if ultrasonography is abnormal), MRI indicated for age older than 4 months, or if sonographic expertise unavailable
MRI indicated No imaging needed
ENCEPHALOCELE
An encephalocele results from herniation of neural tissue along with the meninges and cerebrospinal fluid through a calvarial defect. As with meningoceles, preoperative imaging is recommended prior to surgical excision and reconstruction. Encephaloceles are often seen in association with other craniofacial defects, and neurodevelopmental sequelae may occur.
HUMAN TAIL
Human tails, pseudotails, and acrochordons are rare developmental anomalies. Human tails are vestigial appendages that may be composed of adipose tissue, blood vessels, muscle fibers, and nerves. Pseudotails resemble true human tails but are not related to the embryonic human tail; examples include sacrococcygeal teratomas and myelomeningoceles. True human tails, but not pseudotails, are associated with spinal dysraphism, and MRI is recommended.68
HYPERTRICHOSIS
Localized hypertrichosis overlying the lumbosacral, cervical, or thoracic spine may be associated with spinal dysraphism (Fig. 103-10), in particular when
1736
prominent (“faun tail”).69 Although there are only a few reported cases in the literature, the presence of a faun tail may be underestimated and mild presentations overlooked.
BRANCHIAL CLEFT ANOMALIES
Branchial cysts, clefts, and sinuses are common developmental remnants involving the neck. Presentation involves either a mass, a draining sinus, or recurrent infection.70 Branchial cysts are the most common branchial cleft anomaly; the majority arise from the second branchial arch and present along the sternocleidomastoid muscle on the lateral aspect of the neck. The definitive treatment for branchial cleft anomalies is surgical excision.
THYROGLOSSAL DUCT CYST
Thyroglossal duct cysts are congenital neck anomalies that present as a midline mass arising anywhere from the suprasternal notch to the posterior tongue.71 They arise from the developmental remnant of the migrational tract of the thyroid gland and, as such, may be associated with ectopic thyroid tissue. Surgical excision is the definitive treatment; preoperative verification of a normal thyroid gland is mandatory.
A
B
C
19
URACHAL CYSTS AND POLYPS (OMPHALOMESENTERIC DUCT CYST)
Developmental anomalies of the umbilical cord represent failure of regression of the urachus (urachal cyst or fistula between the bladder and the umbilicus) or the omphalomesenteric duct (umbilical polyp or fistula between the ileum and the umbilicus). Urachal and omphalomesenteric remnants usually present with persistent drainage from the umbilicus or with an umbilical mass.72 Surgical repair is indicated. In contrast, umbilical granulomas are common abnormalities of the umbilicus that present with persistent friable granulation tissue involving the umbilicus noted after separation of the umbilical cord. Treatment with silver nitrate chemical cautery is typically effective.
APLASIA CUTIS CONGENITA
Aplasia cutis congenita (ACC) describes localized areas of absence of the skin and sometimes the underlying subcutaneous tissues and bone. It most often involves the scalp, but may be noted elsewhere (Fig. 103-11). ACC is often an isolated finding, but a multitude of associated conditions have been described.73 ACC has no single underlying cause and appears to be the end result of a number of distinct pathologic processes, including a forme fruste of a neural tube defect. In the most common form of ACC, oval, sharply marginated atrophic macules are seen on the midline of the posterior scalp; they may be ulcerated or crusted or have a thin, shiny membranous covering (membranous aplasia cutis). They are usually solitary, but may be multiple. Aplasia cutis is always hairless, and when healed, lesions are usually atrophic scars, although keloidal scarring has been observed. Superficial lesions may involve only the epidermis and superficial dermis; in more-severe cases, a full-thickness tissue defect may be present, including involvement of the calvarium. Lesions may range from a few millimeters to many centimeters in diameter. Midline lesions should not be biopsied unless cranial imaging has been performed to exclude the possibility of an intracranial connection. After a careful examination
1737
19
A B
to rule out associated anomalies, ACC is treated conservatively with local wound care. Surgical revision of the scar later in childhood or adolescence can be done electively to improve cosmesis. The “hair collar sign” is a ring of darker and/or coarser terminal hairs on the scalp, typically surrounding ACC, dermoid cyst, encephalocele, meningocele, or heterotopic brain tissue.74 The hair collar sign itself is a marker of cranial dysraphism and its presence, like aplasia cutis, mandates careful examination of the infant.
INFECTIONS OF THE NEONATE
Infants younger than 2 months of age have immature immune systems. Life-threatening sepsis can develop quickly and insidiously. Subtle clues, such as a decrease in body temperature, poor feeding, poor muscular tone, or other nonspecific signs, are taken seriously by the pediatrician, and a “rule out sepsis” admission is initiated when clinical suspicion is high. In general, blood, cerebrospinal fluid, and urine cultures are obtained, and IV antibiotic therapy is started while culture results are pending. Table 103-4 lists cutaneous infections of the
■Staphylococcal infections
■Staphylococcal infections
■Impetigo
■Impetigo
■Staphylococcal scalded-skin syndrome
■Staphylococcal scalded-skin syndrome
■Omphalitis
■Omphalitis
■Breast abscess (usually caused by Staphylococcus aureus and Gram-negative organisms)
■Breast abscess (usually caused by Staphylococcus aureus and
Gram-negative organisms)
■Viral infections
■Viral infections
■Varicella
■Varicella
■Herpes simplex virus
■Herpes simplex virus
■Fungal/candidal infections
■Fungal/candidal infections
1738
■Scabies
■Scabies
neonate. Bacterial skin infections that affect neonates, including staphylococcal scalded-skin syndrome, are further discussed in Chaps. 151 and 152, and viral infections that affect neonates, such as varicella and herpes simplex virus, are discussed in Chaps. 164 and 165.
CONGENITAL VIRAL INFECTION
CONGENITAL VIRAL
INFECTION
Petechiae, purpura, jaundice, hepatomegaly, splenomegaly, microcephaly, encephalopathy, ocular abnormalities, anemia, thrombocytopenia, conjugated hyperbilirubinemia, or elevated serum hepatic transaminases prompt consideration of congenital viral infection, particularly if they arise in combination with “blueberry muffin” violaceous to purpuric nodules. These findings are concerning for possible congenital TORCH (toxoplasmosis; other which includes syphilis, enterovirus. and HIV; rubella; cytomegalovirus; herpes) infection.
NEONATAL HERPES SIMPLEX VIRUS INFECTION
NEONATAL HERPES
SIMPLEX VIRUS INFECTION
It is estimated that untreated neonatal herpes simplex virus (HSV) infection has a 50% mortality rate, with 75% of survivors suffering neurologic sequelae. The greatest risk of neonatal herpes occurs when the delivery is vaginal and the mother has active, primary genital herpes (in contrast to recurrent herpes, in which the mother provides transplacental antibodies that offer some protection to the neonate). Chapter 164 discusses HSV in detail. The vast majority of neonatal HSV cases are caused by HSV type 2. Herpes involves the skin, eye, or mouth in most infected neonates, but some patients with CNS
A B
19
or disseminated disease never have skin lesions.75 Herpetic skin lesions manifest as clusters of vesicles on an erythematous base (Fig 103-12). Vesicles that appear during the first 24 hours of life suggest in utero acquisition of HSV, but onset during the first week to 10 days of life is more common, representing exposure to the virus during the delivery.75
A high index of suspicion should be maintained even in the absence of maternal infection or history of genital herpes. Specimens should be obtained for direct fluorescent antibody assay and/or viral culture to detect HSV. A Tzanck smear prepared from a vesicle may provide supportive diagnostic information quickly. If available, a polymerase chain reaction test can be very helpful in rapid diagnosis. IV acyclovir should be instituted as soon as possible after specimens are collected to minimize the chance of virus replication in the CNS and systemic dissemination of HSV. Prompt recognition and early therapeutic intervention result in improved outcomes in HSV-infected infants.75
FUNGAL INFECTION
FUNGAL INFECTION
In full-term neonates, congenital cutaneous candidiasis typically presents with widespread erythematous macules, papules, and pustules associated with superficial desquamation, whereas preterm neonates with congenital cutaneous candidiasis may develop large, weeping erosions.76 Angioinvasive fungal disease in the premature neonate often manifests as ulcerations or necrotic foci with eschar and surrounding erythema.
ERYTHRODERMA
Although uncommon in the neonate, erythroderma may signal a serious underlying condition. A number of genetic, infectious, inflammatory, metabolic, and immunologic disorders can present with
erythroderma, and some are associated with possible death in the neonatal period. In addition, erythroderma predisposes to potentially life-threatening complications such as sepsis, dehydration, and electrolyte imbalance. In 1 retrospective case series of neonatal and infantile erythroderma, diagnostic prevalence was approximated as follows: immunodeficiency (30%), congenital ichthyosis (24%), Netherton syndrome (18%), eczematous or papulosquamous dermatitis (20%), and unknown (unspecified).77
Inflammatory dermatoses that may present in the first few weeks of life with generalized erythema and scaling include seborrheic dermatitis, infantile psoriasis, juvenile pityriasis rubra pilaris, and atopic or nonatopic eczema. Although seborrheic dermatitis typically presents with localized greasy scalp scaling, a more widespread inflammatory dermatitis is seen in some affected infants, typically with an onset in the first few weeks of life. Infantile psoriasis may present in the first few weeks of life as either a localized or a more widespread psoriasiform dermatitis; however, the characteristic clinical features of psoriasis may be lacking (see Chap. 28). Congenital psoriasis is an uncommon presentation that may not be associated with a family history of psoriasis.78 In contrast, the presentation of atopic dermatitis is uncommon in the first few weeks of life, and onset of disease is usually delayed until after the first month of life (see Chap. 22). However, infantile eczema and psoriasis may coexist.79
A family history of atopy or psoriasis and an assessment of areas of predilection and primary morphology may help to differentiate these disorders, although in some cases definitive diagnosis is only possible by observing over time. Several inborn errors of metabolism, including holocarboxylase synthetase deficiency and biotinidase deficiency, both of which result in deficiency of the 4 biotin-dependent carboxylases (multiple carboxylase deficiency), can present with a desquamative dermatitis.80 A collodion presentation with features of ichthyosis also has been reported.81 Affected neonates
1739
19
typically also experience lethargy, seizures, and apnea; delayed presentation may be seen in those affected with late-onset biotinidase deficiency or late-onset multiple carboxylase deficiency in which symptoms may not develop until later in infancy or childhood.82
In the United States, depending on the state where the infant was born, these disorders may be detected through the newborn screening program before significant symptoms arise. Essential fatty acid deficiency is an uncommon acquired nutritional deficiency that may present with an exfoliative dermatitis.83 Risk factors for essential fatty acid deficiency include malnutrition, which may result from the implementation of specialized infant formulas, improper infant feeding or fad diets, hyperalimentation, or disorders such as cystic fibrosis that result in malabsorption. Essential fatty acid deficiency may occur in association with other nutrient deficiencies, including zinc deficiency, in which case signs of acrodermatitis also may be noted. Several neonatal infections may result in diffuse erythema with or without scaling or other primary lesions. In term and premature neonates, staphylococcal scalded skin syndrome may present with variable erythema, erosions, scaling, and desquamation; congenital presentation has rarely been reported because of presumed intrauterine infection.84-87 Early congenital syphilis may present as a desquamative dermatitis or a more generalized vesiculobullous dermatitis.88-90
The congenital ichthyoses that may present with neonatal erythroderma include Netherton syndrome, autosomal recessive congenital ichthyosis (which commonly presents with a collodion membrane), Sjögren-Larsson syndrome, keratitis-ichthyosis-deafness syndrome, and neutral lipid storage disease (Chanarin- Dorfman syndrome).91 Other genetic disorders that may sometimes present with erythroderma or a collodion membrane include X-linked hypohidrotic ectodermal dysplasia and type 2 Gaucher disease.92,93
Several primary immunodeficiency syndromes are associated with neonatal erythroderma, including Omenn syndrome, severe combined immunodeficiency syndrome (SCID), hyperimmunoglobulin E syndrome, and DiGeorge syndrome. SCID is a heterogeneous group of immunodeficiency disorders characterized by combined T-cell and B-cell dysfunction; there are at least 13 different genes associated with this phenotype.94 The presence of a diffuse eczematous dermatitis is associated with SCID, and in at least a proportion of affected infants dermatitis results from maternal engraftment and cutaneous graft-versus-host disease; diagnosis can be facilitated by skin biopsy with appropriate ancillary genetic studies.95,96 The prognosis for affected patients is poor because of the risk for severe infection, failure to thrive, immune dysregulation, and other complications; bone marrow transplantation before 3 to 4 months of age is generally recommended and ideally is performed before infectious complications arise. Many states include screening for SCID by the T-cell receptor excision circle (TREC) assay on the newborn screen.97 Omenn syndrome is a rare form of SCID that results from autosomal recessive mutations
1740
in the RAG-1 or RAG-2 gene. In addition to an exfoliative erythroderma, the characteristic features include failure to thrive, chronic diarrhea, lymphadenopathy, and hepatosplenomegaly. In the absence of bone marrow transplantation, the prognosis is poor. Hyperimmunoglobulin E syndrome associated with mutations in the STAT3 gene may present with a diffuse eczematous dermatitis in infancy; atopy, mucocutaneous candidiasis, and recurrent staphylococcal skin infections are typical features.98 A characteristic clinical finding of hyperimmunoglobulin E syndrome in infancy is the development of a papulopustular dermatitis of the face and scalp.99 DiGeorge syndrome results from a deletion of chromosome 22q11.21; the key features are thymic aplasia, cardiac anomalies involving the aortic arch, hypoparathyroidism, cleft palate, and dysmorphic features. An eczematous dermatitis has been reported in some infants with DiGeorge syndrome.100,101
Skin biopsy may be helpful in selected diagnoses, in particular Netherton syndrome and SCID.102
SEBORRHEIC DERMATITIS
Seborrheic dermatitis is a common and benign inflammatory dermatosis in infancy, and may be noted as early as the first few weeks of life. The most common presentation is the development of greasy yellow scale with mild underlying erythema on the scalp (“cradle cap”). In the diaper and intertriginous areas, scaling is less prominent and erythema more well-defined, and there is clinical overlap with infantile psoriasis (“sebopsoriasis”). Less-common areas of involvement include the face, in particular the eyebrows and nasolabial folds, and the torso, where the eruption manifests as variable erythema and greasy scaling; in darkerskinned infants, postinflammatory hypopigmentation may predominate. Impetiginization or secondary candidal infection may occur. The pathophysiology of seborrheic dermatitis is hypothesized by some experts to involve an exaggerated immune response to skin colonization with Malassezia species.103 Seborrheic dermatitis typically remits spontaneously within the first 1 to 2 years of life, although there may be an association with the development of adult seborrheic dermatitis and atopic dermatitis.104,105
For mild cases, application of baby oil or mineral oil to the affected areas of the scalp, followed by gentle combing and shampooing to remove scales, is sufficient. For more severe involvement, use of a topical antifungal shampoo or cream or a low-potency topical corticosteroid may be necessary. Seborrheic dermatitis must be differentiated from other inflammatory skin disorders of infancy, including infantile psoriasis, atopic and nonatopic eczema, and Langerhans cell histiocytosis. Additionally, seborrheic dermatitis-like eruptions have been reported to occur in association with immunodeficiency, and nutritional and metabolic disease. Any history of failure to thrive, developmental delay, unexplained symptoms, or recurrent infection raises concern for possible associated systemic disease.
DIAPER DERMATITIS
Diaper dermatitis (Table 103-5) is a common skin problem in infants. Multiple factors contribute to the development of diaper dermatitis. Prolonged exposure to moisture results in increased frictional damage, decreased barrier function, and increased reactivity to irritants. Interrelated etiologic factors include contact with urine and feces, fecal proteolytic and lipolytic digestive enzymes, increased skin pH, and superinfection with Candida.106 Less commonly, bacterial superinfection may complicate diaper dermatitis.
IRRITANT DIAPER DERMATITIS
IRRITANT DIAPER
DERMATITIS
Irritant contact dermatitis is the most common cause of diaper dermatitis. It is characterized by erythematous, moist, and sometimes scaly patches favoring the convex surfaces of the genitalia and buttocks. The skin folds are classically spared. Barrier diaper creams and frequent diaper changes are very helpful to treat this condition.
ALLERGIC CONTACT DIAPER DERMATITIS
ALLERGIC CONTACT
DIAPER DERMATITIS
Allergic contact dermatitis occurs in the diaper area as well. Common contact allergens for the diaper region include preservatives, fragrances, rubber additives, and disperse dyes in diapers or baby wipes.107
19
CANDIDAL DIAPER DERMATITIS
CANDIDAL DIAPER
DERMATITIS
Candidiasis (see Chap. 161) is the second most common cause of diaper dermatitis and is characterized by bright red erythematous, moist papules, patches, and plaques that tend to involve body folds as well as convex surfaces. Satellite papules and pustules are frequently observed, and oral thrush may be present. Candida from intestinal flora may contaminate and exacerbate any type of diaper dermatitis present for longer than 3 days.108
PSEUDOVERRUCOUS PAPULES AND NODULES
PSEUDOVERRUCOUS
PAPULES AND NODULES
Pseudoverrucous papules and nodules (Fig. 103-13) are flat-topped, skin-colored papules that develop in the diaper and perianal areas in patients of any age whose skin is chronically exposed to moisture, including children with prolonged urinary or fecal incontinence.109
JACQUET EROSIVE DERMATITIS
JACQUET EROSIVE
DERMATITIS
Jacquet erosive dermatitis is an uncommon, severe diaper dermatitis that is characterized by welldemarcated, punched-out ulcers and erosions.
DIAPER DERMATITIS CANDIDIASIS (CANDIDAL INTERTRIGO) LANGERHANS CELL HISTIOCYTOSIS PSORIASIS (NAPKIN PSORIASIS)a SEBORRHEIC DERMATITISa
Age Any age Any age 1 to 3 years Usually 3 to 6 months First few weeks to 3 months
Affected sites Convexities of the genitalia affected, skin folds spared
Skin folds and convexities affected Scalp, intertriginous skin folds Trunk, limbs, face, skin folds, and diaper area may be affected
Appearance Scaly erythematous patches Bright red, erythematous, moist papules, patches, and plaques with satellite papules and pustules
Scalp, intertriginous skin folds, face, torso
Tan-to-pink papulovesicles, nodules, ulcerations, and petechiae
Well-defined erythema, white scales over trunk and body, but scaling usually absent in skin folds
Greasy yellow scales with mild erythema; in diaper areas, well-defined erythema, glistening appearance, scaling not prominent
Etiology May be irritant or allergic in origin Candida sp. Reactive vs neoplastic (see Chap. 117)
Treatment Barrier creams,
Keep intertriginous
Treatment Barrier creams, frequent diaper changes (see Table 103-6)
Keep intertriginous areas dry, topical antifungal agents
frequent diaper changes (see Table 103-6)
areas dry, topical antifungal agents
aInfantile psoriasis and seborrheic dermatitis may overlap (“sebopsoriasis”).
Inflammatory disease, T-cell mediated Exaggerated immune response to Malassezia sp.
(See Chap. 117) Topical steroids, topical
Mineral or baby oil; anti-
(See Chap. 117) Topical steroids, topical calcineurin inhibitors Mineral or baby oil; antifungal shampoo; lowpotency topical steroid
calcineurin inhibitors
fungal shampoo; lowpotency topical steroid
1741
19
Prolonged contact with urine and feces under occlusion leads to this condition.110 The availability of superabsorbent disposable diapers has made this diagnosis less common.
GRANULOMA GLUTEALE INFANTUM
GRANULOMA GLUTEALE
INFANTUM
Granuloma gluteale infantum is an uncommon diaper rash characterized by reddish purplish nodules of different sizes (0.5 to 3 cm) occurring on the convexities of the diaper area in 2- to 9-month-old infants. It arises within preexisting diaper dermatitis. Biopsy shows dense dermal infiltrates of lymphocytes, plasma cells, neutrophils, and eosinophils, but no true granulomas. It appears to be an unusual reaction to the usual irritant factors, Candida infection, and, in some cases, topical corticosteroid use in the diaper region.110 Treatment consists of avoidance of irritants, use of a barrier ointment, and avoidance of topical corticosteroids. Resolution occurs over several months.
DERMATOSES NOT ETIOLOGICALLY RELATED TO DIAPER WEARING
DERMATOSES NOT
ETIOLOGICALLY RELATED
TO DIAPER WEARING
Infantile seborrheic dermatitis, napkin psoriasis (Fig. 103-14), bullous impetigo, acrodermatitis enteropathica, scabies, herpes simplex infections, and Langerhans cell histiocytosis are conditions that may occur in the diaper region but are not primarily caused by the wearing of diapers. They should be considered in the differential diagnosis when evaluating diaper eruptions. Skin biopsy is indicated to rule out Langerhans cell histiocytosis (see Chap. 117) if nonhealing erosions or petechiae are seen in the diaper area (Fig. 103-15).
1742
A
B
TREATMENT OF DIAPER DERMATITIS
TREATMENT OF DIAPER
DERMATITIS
HAMARTOMAS AND BENIGN TUMORS
INFANTILE MYOFIBROMATOSIS
INFANTILE
MYOFIBROMATOSIS
Infantile myofibromas typically present as rubbery dermal and subcutaneous nodules. There can be a
A B
19
solitary myofibroma or multiple myofibromas (myofibromatosis). In addition to skin, infantile myofibromatosis can involve bone, the GI tract, heart, lungs, and kidneys.112 Myofibromas limited to soft tissue typically resolve spontaneously within 1 to 2 years. Thus, clinical observation is warranted.
FIBROUS HAMARTOMA OF INFANCY
FIBROUS HAMARTOMA OF
INFANCY
Fibrous hamartoma of infancy is an uncommon infantile mass. Most cases appear as a solitary, painless, 0.5- to 10-cm skin nodule in the deep dermis or subcutis.
A = Air. The diaper should be left open as much as possible when the infant sleeps to allow drying of the skin. B = Barrier ointments. Zinc oxide pastes, petrolatum, and other bland, unmedicated barrier preparations are mainstays of therapy. A continuous layer of barrier paste or ointment should be maintained, reapplying with every diaper change, if necessary. Baby powder on the diaper area offers no antimicrobial benefit to the infant and adds a risk of aspiration. C = Cleansing and anticandidal treatment. Gentle cleansing with plain water, mineral oil, or unscented gentle cleanser is recommended. Avoidance of friction or rubbing is important. A topical anticandidal agent should be added for any signs of candidiasis. Oral nystatin is indicated if oral thrush is present. D = Diapers. Diapers should be changed as frequently and as soon after soiling as possible, especially if cloth diapers are used. E = Education of parents and caregivers.
A = Air. The diaper should be left open as much as possible when the
infant sleeps to allow drying of the skin. B = Barrier ointments. Zinc oxide pastes, petrolatum, and other bland,
unmedicated barrier preparations are mainstays of therapy. A continuous layer of barrier paste or ointment should be maintained, reapplying with every diaper change, if necessary. Baby powder on the diaper area offers no antimicrobial benefit to the infant and adds a risk of aspiration. C = Cleansing and anticandidal treatment. Gentle cleansing with plain
water, mineral oil, or unscented gentle cleanser is recommended. Avoidance of friction or rubbing is important. A topical anticandidal agent should be added for any signs of candidiasis. Oral nystatin is indicated if oral thrush is present. D = Diapers. Diapers should be changed as frequently and as soon
after soiling as possible, especially if cloth diapers are used. E = Education of parents and caregivers.
Modified from Boiko S. Making rash decisions in the diaper area. Pediatr Ann. 2000;29(1):50-56.
Excision is the mainstay of treatment, and recurrence rates are low.113,114
INFANTILE DIGITAL FIBROMA
INFANTILE DIGITAL
FIBROMA
Infantile digital fibromas are smooth pink nodules that appear on the phalanges of infants. Most commonly the fingers are involved, and the thumbs and great toes are classically spared. Approximately one-third of infantile digital fibromas are present at birth. Skin biopsy is diagnostic and shows bundles of myofibroblasts with round cytoplasmic inclusions that are highlighted by the Masson trichrome or phosphotungstic acid–hematoxylin stains. Infantile digital fibromas have a high recurrence rate after surgical excision and tend to resolve spontaneously over years. Conservative observation is typically recommended.115
CONGENITAL SMOOTH MUSCLE HAMARTOMA
CONGENITAL SMOOTH
MUSCLE HAMARTOMA
Congenital smooth muscle hamartomas (CSMHs) are benign dermal proliferations of hyperplastic smooth muscle. CSMHs most often appear as a solitary irregular dermal plaque on the trunk or proximal extremities. The overlying skin tends to be skin-toned to slightly hyperpigmented and may have associated hypertrichosis. Brisk rubbing of a CSMH results in transient piloerection and induration, which is termed the pseudo-Darier sign. The pseudo-Darier sign is elicited in approximately 80% of CSMHs and supports clinical diagnosis. CSMHs are benign and can be observed
1743
19
with consideration of surgical excision for symptomatic or cosmetically concerning lesions.
NEOPLASTIC AND PROLIFERATIVE DISORDERS
NEUROBLASTOMA
NEUROBLASTOMA
Neuroblastoma is the second most common solid tumor of childhood, and approximately 25% of cases are congenital. Cutaneous metastatic neuroblastoma is included in the “blueberry muffin” baby differential diagnosis, owing to its purple-hued papules and nodules. Skin lesions of neuroblastoma may exhibit blanching, attributed to release of locally active catecholamines from the malignant cells, for up to 1 hour after stroking.116 Skin biopsy is needed to determine the diagnosis of neuroblastoma and shows small, round cells with large atypical nuclei. The malignant cells may form pseudorosette structures. Immunohistochemistry for neuronal markers, particularly neuron-specific enolase, is helpful.
CONGENITAL LEUKEMIA
CONGENITAL LEUKEMIA
Congenital leukemia represents a small subset (<1%) of childhood leukemia. In the newborn, acute myeloid leukemia is more common than acute lymphocytic leukemia.117 Signs of leukemia in newborn skin include ecchymoses, petechiae, and skin nodules. Multiple blue-to-purple skin nodules are found in approximately 60% of newborns with congenital leukemia, thus congenital leukemia is included in the differential diagnosis of the “blueberry muffin” baby. Skin biopsy shows sheets of atypical mononuclear cells infiltrating the dermis or subcutaneous fat. Complete blood counts and bone marrow biopsy help confirm the diagnosis.
LANGERHANS CELL HISTIOCYTOSIS
LANGERHANS CELL
HISTIOCYTOSIS
Langerhans cell histiocytosis (LCH) is an uncommon proliferative disorder of childhood. Approximately 5% of LCH cases are diagnosed in the newborn period. Cutaneous findings of LCH in the newborn include tan-to-pink papulovesicles, nodules, ulcerations, and petechiae that preferentially develop on the scalp and intertriginous skin folds. Cutaneous LCH may also manifest as a “blueberry muffin” baby, with blue-hued skin nodules. Red-brown skin nodules with or without ulceration are another possible presentation.
1744
The skin lesions of congenital LCH may resolve spontaneously, which is likely responsible for the past nomenclature of congenital “self-healing” LCH. However, because of a risk for disease recurrence, even into childhood, continued monitoring for possible complications in other organ systems is required for all patients with LCH.118 Skin biopsy of cutaneous lesions shows a histiocytic infiltrate that stains positive for CD1a and CD107 (Langerin).
CUTANEOUS MASTOCYTOSIS
CUTANEOUS
MASTOCYTOSIS
Cutaneous mastocytosis refers to a spectrum of mast cell proliferative disorders that affect the skin. Infants with cutaneous mastocytosis may have a single tanto-light brown ovoid plaque (solitary mastocytoma), many small red-brown macules and papules (urticaria pigmentosa, maculopapular cutaneous mast cell disease), or diffusely indurated, peau-de-orange textured skin (diffuse cutaneous mastocytosis). Telangiectasia macularis eruptive perstans, which manifests as small telangiectatic patches in older individuals, is an exceptionally rare form of mast cell disease in infants or children. Of the mast cell disease spectrum entities, solitary mastocytoma and urticaria pigmentosa frequently appear in the first few months of life. Brisk stroking of affected skin will result in mast cell degranulation with a wheal and flare reaction. This useful clinical examination finding is termed Darier sign. Diagnosis can be made clinically in many cases, but if needed, skin biopsy demonstrates large numbers of mast cells in the dermis. Special stains, including toluidine blue, Giemsa, and c-kit (CD117), can highlight mast cell populations. History of flushing, wheezing, vomiting, diarrhea, abdominal pain, bone pain, or shock should be elicited from patients with widespread cutaneous mast cell disease. In cases with extensive skin disease or a concerning review of symptoms, serum tryptase may be a useful clinical indicator. Based on extrapolation from adult systemic mastocytosis literature, some recommend bone marrow biopsy to rule out systemic mastocytosis in children with tryptase levels greater than 20 ng/mL, whereas others reserve bone marrow biopsy only with levels greater than 100 ng/mL. Recent work suggests that enlargement of the liver and/or spleen is a more sensitive indicator of systemic mast cell disease in children when compared to serum tryptase or history of severe mediator symptoms, and that serum tryptase levels tend to decrease over time in children.119 In general, cutaneous mastocytosis is managed with oral antihistamines (H1 and H2). Parents should be counseled to avoid exposing affected children to common triggers of mast cell degranulation, which include anesthetics, other medications, and physical stimuli.
GENODERMATOSES PRESENTING IN THE NEONATAL PERIOD
Several genetic skin diseases may have the onset of characteristic cutaneous features in the neonatal period. The most common diagnoses include epidermolysis bullosa, congenital ichthyoses, and ectodermal dysplasia.
EPIDERMOLYSIS BULLOSA
EPIDERMOLYSIS BULLOSA
Epidermolysis bullosa (EB) is a mechanobullous disease with variable presentation and prognosis (see Chap. 60). There are 4 main types: EB simplex, junctional EB, dystrophic EB, and Kindler syndrome; they are distinguished on the basis of the localization of the cleavage plane within the skin. EB should be suspected in the neonate with a bullous eruption; however, other etiologies, including infection, should also be considered.120 Diagnosis relies on clinical examination and history, skin biopsy for transmission electron microscopy and immunoepitope mapping, and genetic testing. Prognosis for the milder forms of EB is excellent, whereas the more-severe forms (junctional EB and recessive dystrophic) are associated with significant morbidity and mortality.
CONGENITAL ICHTHYOSIS
CONGENITAL ICHTHYOSIS
The congenital ichthyoses or disorders of cornification are a heterogeneous group of inherited disorders which involve abnormal epidermal differentiation (see Chap. 47). The genetic basis for many of the congenital ichthyoses is known, and the current classification system differentiates syndromic from nonsyndromic forms of congenital ichthyosis.121 Presentation in the neonatal period may include a collodion membrane, which is most commonly seen with the autosomal recessive congenital ichthyoses, such as lamellar ichthyosis and nonbullous congenital ichthyosiform erythroderma. The most extreme presentation of autosomal recessive congenital ichthyosis is harlequin ichthyosis, in which thick, plate-like hyperkeratotic scales cover the face, scalp and body, and ectropion and eclabium are present. Infants with harlequin ichthyosis may develop respiratory insufficiency and are at risk for dehydration, metabolic abnormalities, and sepsis.
ECTODERMAL DYSPLASIA
ECTODERMAL DYSPLASIA
The ectodermal dysplasias are a large group of related disorders characterized by abnormalities in 1 or more
19
ectodermal structures: the skin, hair, nails, teeth, and eccrine glands (see Chap. 131). As of this writing, there are more than 200 defined disorders, only a small proportion of which have a known genetic etiology.122
Diagnosis of many of the forms of ectodermal dysplasia is not generally possible in the neonatal period and is delayed until features such as delayed dentition, alopecia, and nail dystrophy become more pronounced. The astute clinician, however, may suspect X-linked hypohidrotic ectodermal dysplasia, one of the more common forms of ectodermal dysplasias, by noting the characteristic facies, alopecia, and unexplained hyperpyrexia in a neonate or young infant. Other forms of ectodermal dysplasias that may present in the neonatal period include the spectrum of p63- related ectodermal dysplasias termed ankyloblepharon-ectrodactyly-clefting syndrome, which encompass the entities previously known as Hay-Wells syndrome, Rapp-Hodgkin syndrome, and ectodermal dysplasiaectrodactyly-clefting syndrome.
INCONTINENTIA PIGMENTI
INCONTINENTIA PIGMENTI
Incontinentia pigmenti is an X-linked disorder classified as a type of ectodermal dysplasia (see Chap. 131). Incontinentia pigmenti results from mutations in the nuclear factor κB essential modulator (NEMO) gene.123
It is characterized by cutaneous manifestations, abnormalities of the hair, teeth and nails, ocular anomalies, and neurologic abnormalities.124 The earliest clinical manifestations include a characteristic Blaschkoid vesicular eruption. Although more common in girls as a consequence of prenatal lethality in the majority of affected male fetuses, males may present with incontinentia pigmenti in a number of circumstances, including the presence of an XXY karyotype (Klinefelter syndrome), somatic mosaicism, or hypomorphic mutation.125
OTHER DERMATOSES OF THE NEONATE
SUBCUTANEOUS FAT NECROSIS OF THE NEWBORN
SUBCUTANEOUS FAT
NECROSIS OF THE NEWBORN
Subcutaneous fat necrosis of the newborn is characterized by firm, red to purple subcutaneous nodules or plaques on the back, cheeks, buttocks, arms, and thighs (Fig. 103-16; see Chap. 73). The lesions usually appear within the first 2 weeks of life and resolve spontaneously over several weeks.126 Skin biopsy demonstrates lobular fat necrosis with needleshaped clefts in lipocytes and mixed inflammation with lymphocytes, macrophages, and giant cells. Infants affected by subcutaneous fat necrosis of the newborn are at risk for hypercalcemia and should be monitored.
1745
19
SCLEREMA NEONATORUM
SCLEREMA NEONATORUM
Sclerema neonatorum describes diffuse skin hardening in a sick, premature newborn. It is thought to be exceedingly uncommon with modern neonatal care. The onset is characteristically after 24 hours of age. Critically ill premature neonates with sepsis, hypoglycemia, acidosis, or other severe metabolic abnormalities are at most risk. The skin becomes hard and appears shiny. Biopsy shows needle-like crystals within lipocytes but no associated inflammatory infiltrate or fat necrosis, differentiating it from subcutaneous fat necrosis of the newborn. The etiology of sclerema neonatorum is unknown, and infant mortality is high.
ANETODERMA OF PREMATURITY
ANETODERMA OF
PREMATURITY
A specific form of iatrogenic anetoderma (see Chap.
70) has been described in premature infants (born at 24 to 30 weeks of gestation) with very-low birthweights and prolonged neonatal intensive care hospitalization.127 A retrospective review of 11 cases noted the appearance of round, flat atrophic patches on the chest and abdomen (including the periumbilical region), developing between 6 weeks and 5 months of age. Among them, eight patients had lesions at sites where adhesive monitoring leads had been removed, and 5 patients had circular ecchymotic patches from removal of adhesive monitoring leads prior to the occurrence
1746
of the anetoderma. The anetoderma did not improve with time. Given the presumed relationship of the development of anetoderma and skin trauma from adhesive leads, avoidance of pressure (placing leads on the ventral chest when the infant slept on the back, for instance) may help reduce risk.128
CUTIS MARMORATA TELANGIECTATICA CONGENITA
CUTIS MARMORATA
TELANGIECTATICA
CONGENITA
Cutis marmorata telangiectatica congenita is characterized by persistent, reticulated atrophic violaceous vascular patches. It is sometimes associated with telangiectasias and ulceration (Fig. 103-17). It is a sporadic condition, and its etiology remains unknown. Theories of vascular malformation are currently favored. Diagnosis is usually evident on clinical examination. Most frequently, a lower extremity is involved, but location on the trunk or upper extremity is not uncommon. Limb asymmetry may be present. However, the majority of patients have a good prognosis, with half demonstrating improvement of the mottled appearance over the first 2 years.129
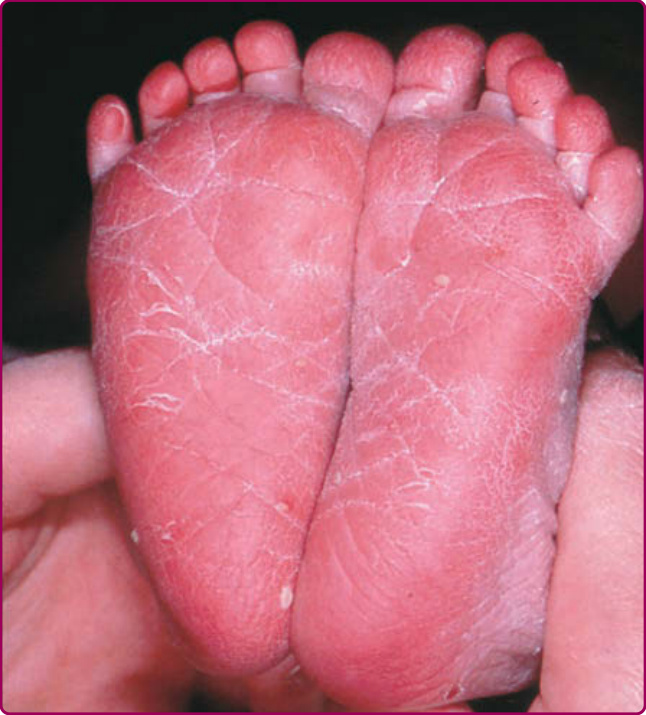
Figure 103-1 The feet of a postterm newborn. The dry, hyperlinear, and scaly skin is typical of babies born after 40 weeks of gestation. Incidentally, pustules of transient neonatal pustular melanosis are also seen.
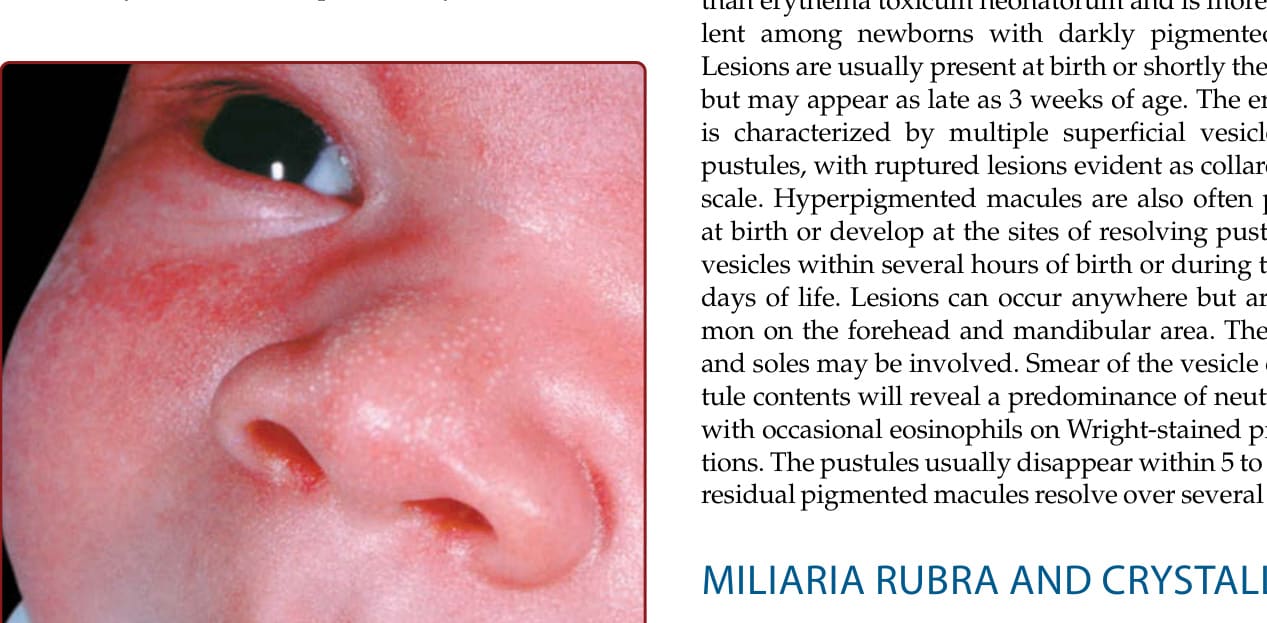
Figure 103-3 Erythema toxicum neonatorum. Erythematous macules, some with a tiny central papule or pustule, on the arm of a 1-day-old newborn.

Figure 103-4 Transient neonatal pustular melanosis. A, A newborn with congenital, thin-walled pustules that rupture easily. B, Hyperpigmented macules appeared by 10 hours of age.

Figure 103-5 Benign neonatal cephalic pustulosis. Tiny papulopustules on the cheeks of a 3-week-old infant.

Figure 103-6 Infantile acne. True comedones and inflammatory papules are noted on the cheeks of a healthy 10-month-old girl.

Figure 103-7 Supernumerary digit, a common minor malformation.
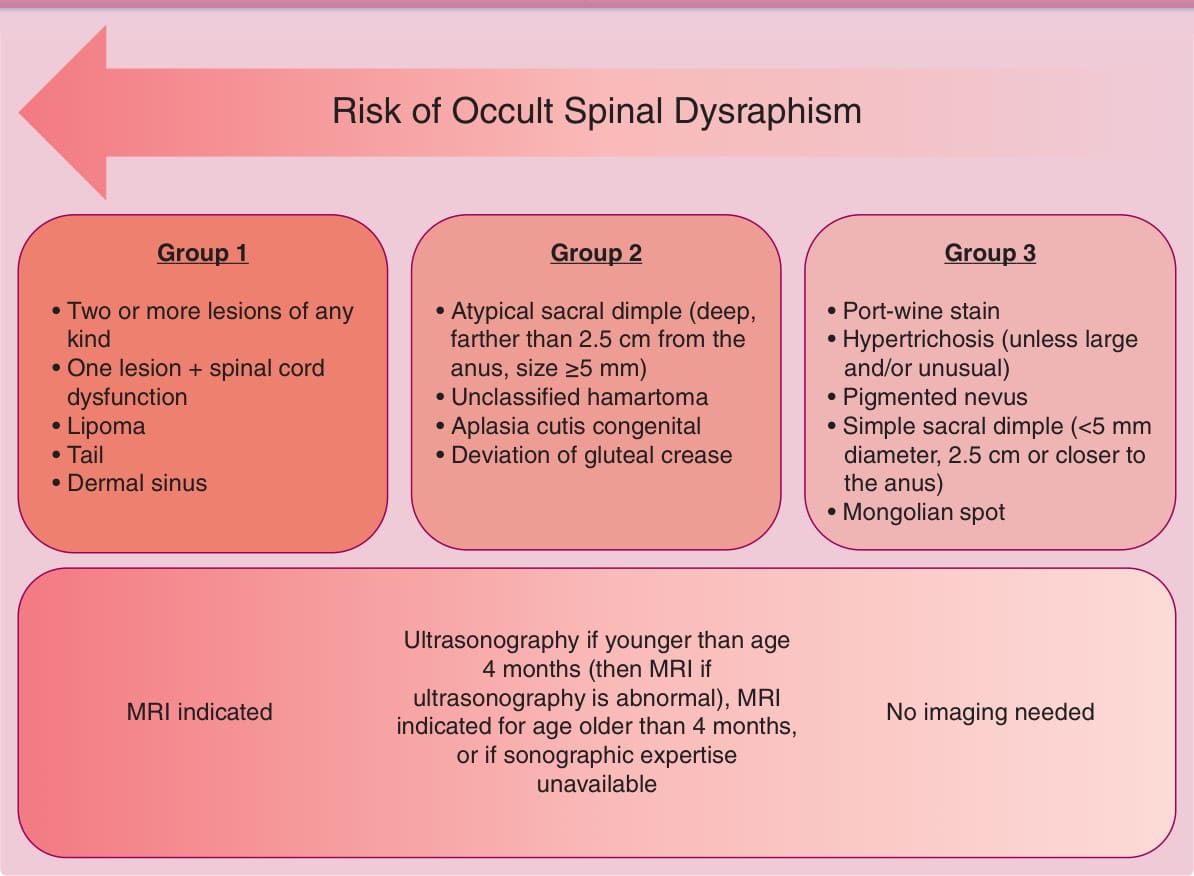
Figure 103-8 Congenital lumbosacral midline skin lesions, required assessment, and risk of occult spinal dysraphism. (Data from Guggisberg D, Hadj-Rabia S, Viney C, et al. Skin markers of occult spinal dysraphism in children: a review of 54 cases. Arch Dermatol. 2004;140(9):1109-1115.)

Figure 103-9 A and B, Nasal glioma initially thought to be a hemangioma of infancy. A firm, reddish, slightly pedunculated tumor was noted off of the midline of the nasal root. MRI showed no intracranial connection. C, Nasal glioma. Firm subcutaneous mass noted at birth.

Figure 103-10 A large, wide tuft of thick terminal hair on the lumbosacral spine noted at birth. This infant had an underlying tethered cord (note midline scar from surgical repair).
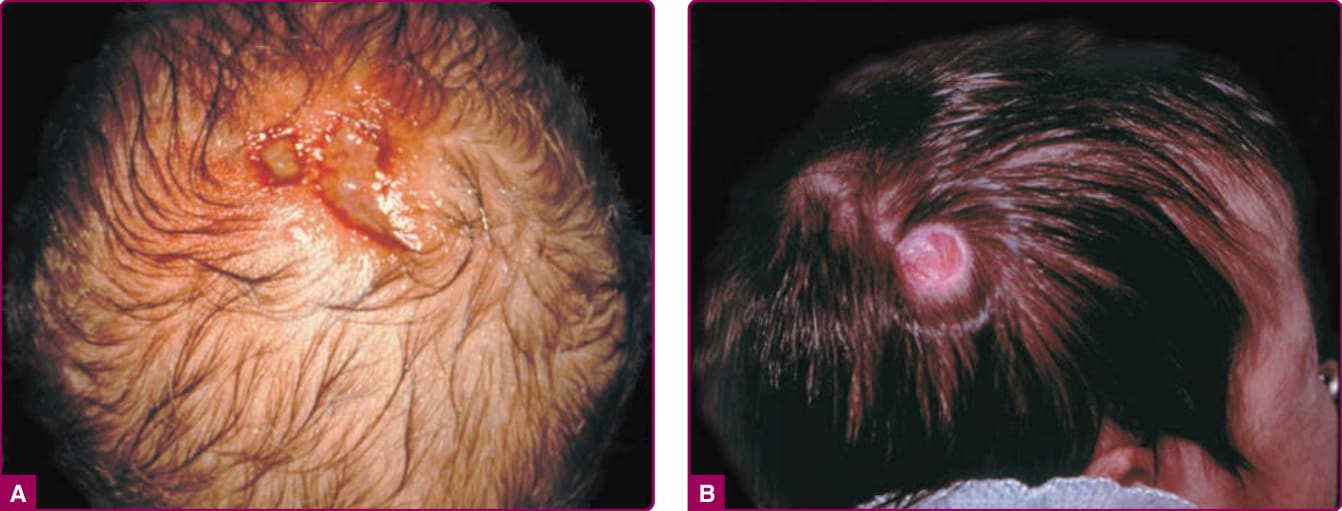
Figure 103-11 Two infants with aplasia cutis congenita. A, Scalp erosions grouped at the vertex scalp. Scraping or biopsy is contraindicated. B, An atrophic, well-circumscribed round patch with visible capillaries on the scalp of an infant. (Image A is from Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. New York: Mosby Elsevier; 2008, with permission. Copyright © Elsevier.)
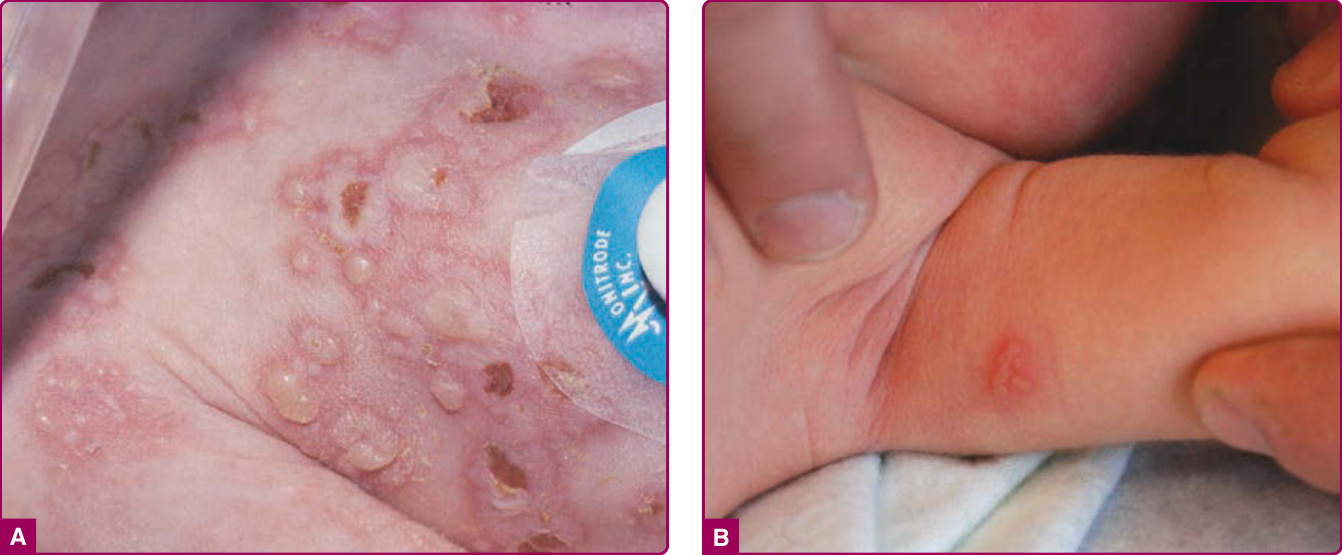
Figure 103-12 A and B, Herpes simplex infection in 2 infants. Grouped vesicles on an erythematous base. Pustules and erosions are also present. (A used with permission from Alvin H. Jacobs, MD.)

Figure 103-13 Pseudoverrucous papules and nodules in a newborn.
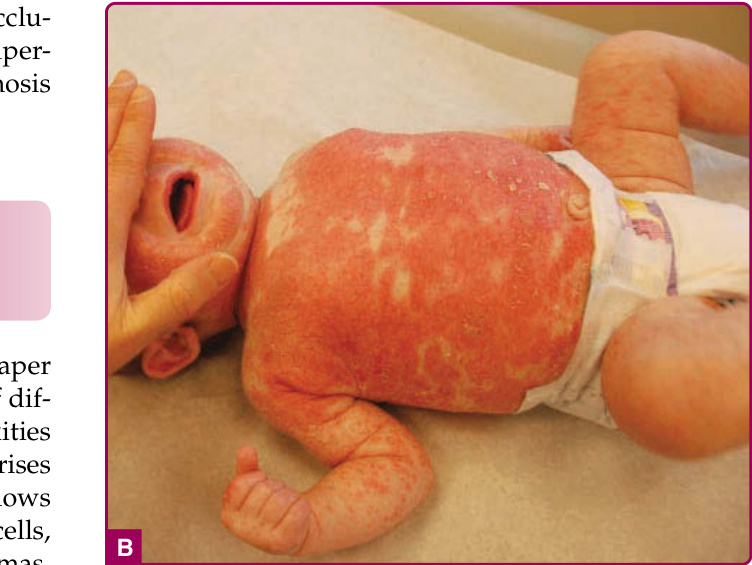
Figure 103-14 A, Infantile psoriasis with involvement in the diaper region. B, Infantile psoriasis. This generalized eruption responded well to topical steroids initially and topical tacrolimus later.

Figure 103-15 A and B, Langerhans cell histiocytosis with petechiae and erosions of the skin. This patient also had hepatosplenomegaly.

Figure 103-16 Subcutaneous fat necrosis of the newborn. This infant developed an erythematous firm mass on the back by 2 weeks of age and later developed hypercalcemia.

Figure 103-17 Cutis marmorata telangiectatica congenita. Note the atrophic, dusky, stellate patches with overlying telangiectasias.
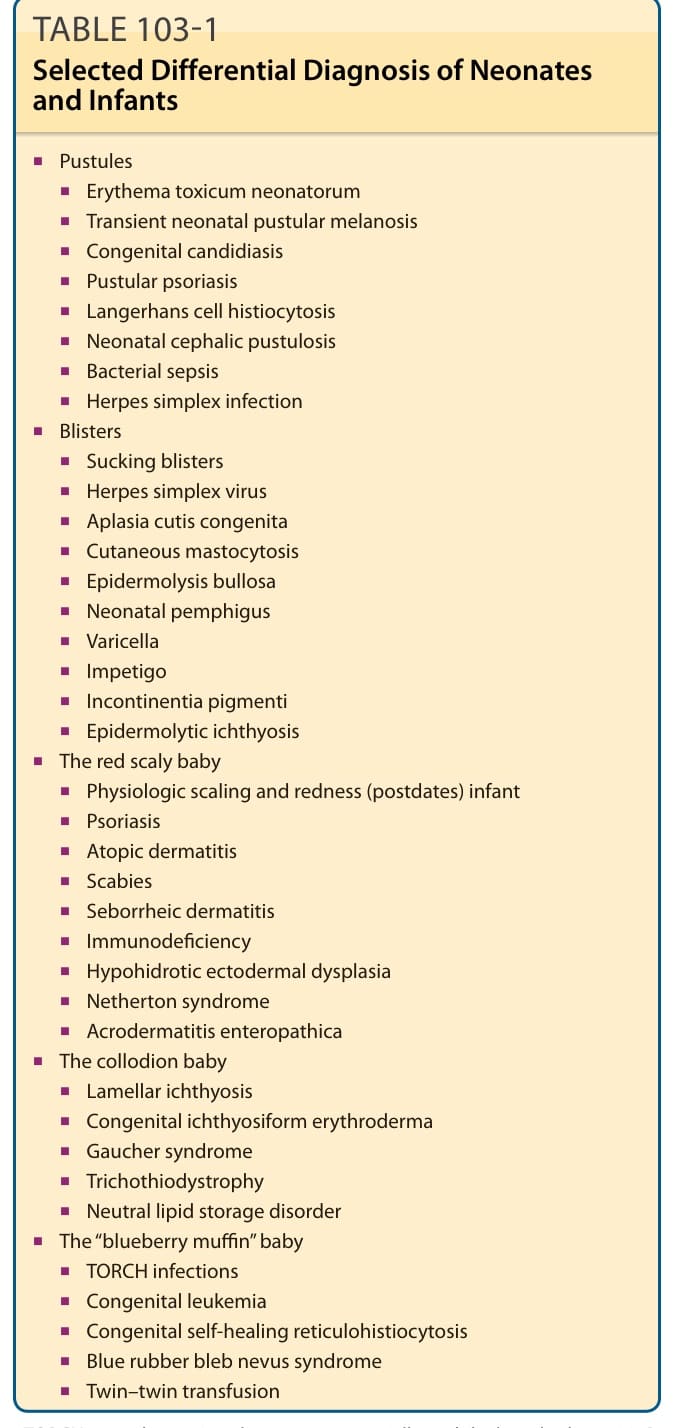
TABLE 103-1 Selected Differential Diagnosis of Neonates and Infants
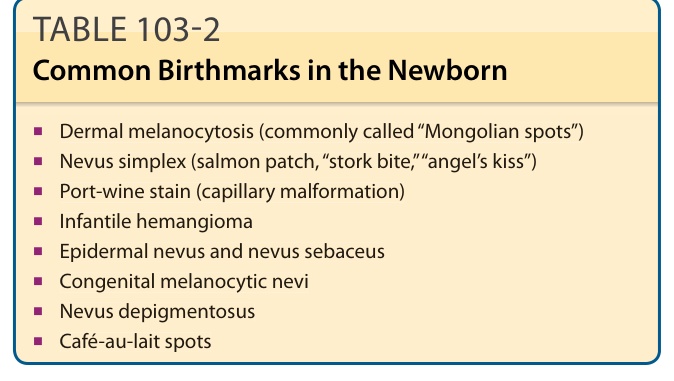
TABLE 103-2 Common Birthmarks in the Newborn
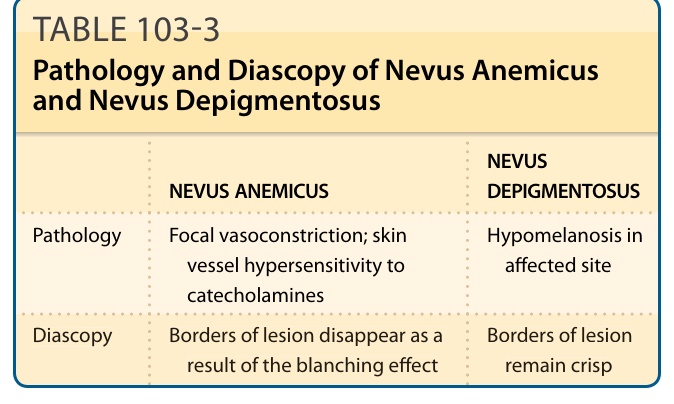
TABLE 103-3 Pathology and Diascopy of Nevus Anemicus and Nevus Depigmentosus
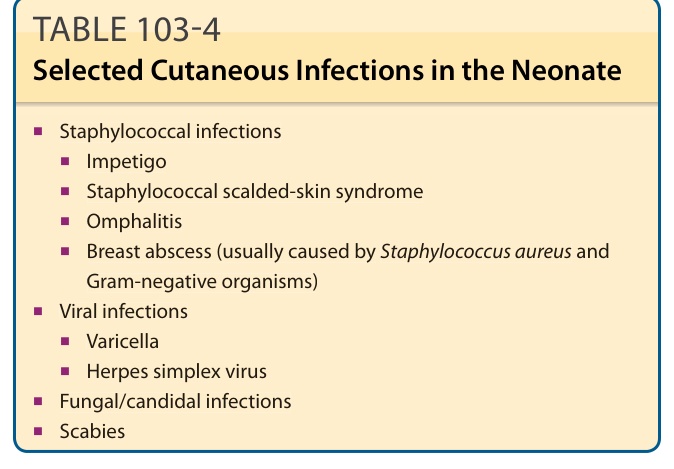
TABLE 103-4 Selected Cutaneous Infections in the Neonate
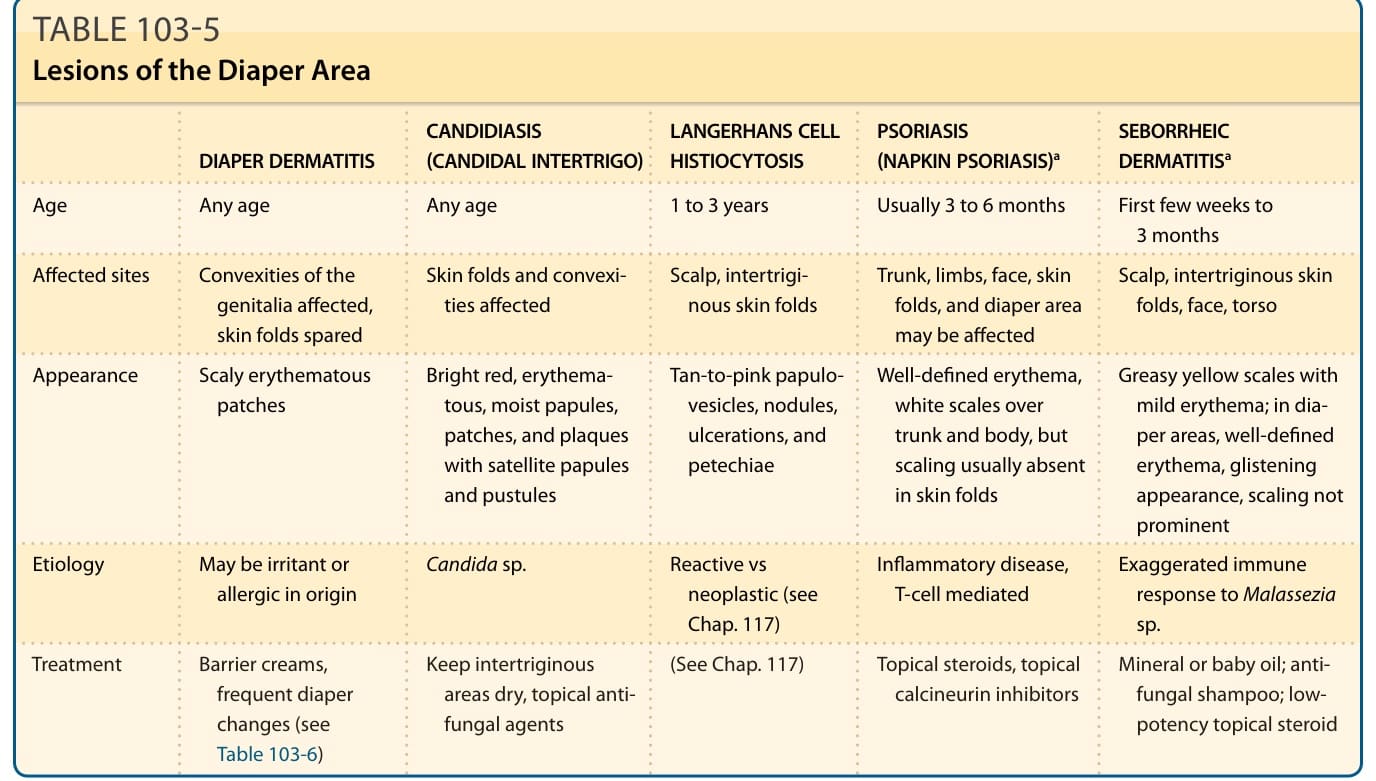
TABLE 103-5 Lesions of the Diaper Area
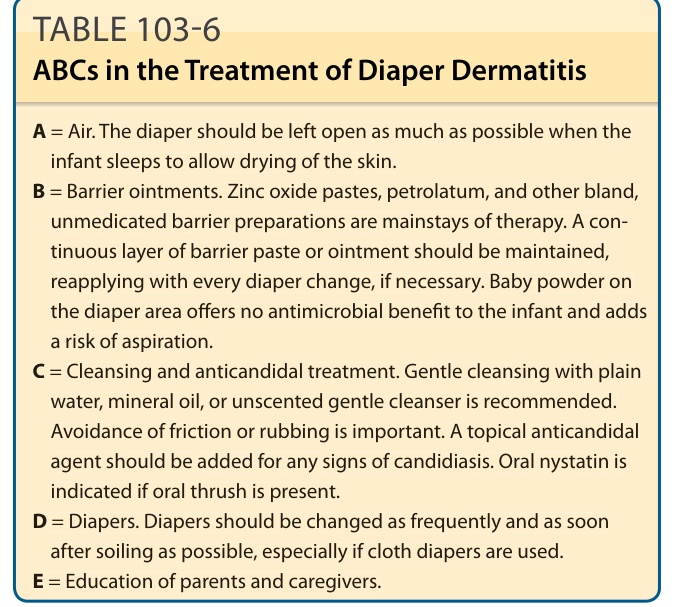
Table 103-6 outlines the treatment of diaper dermatitis.111