Physical Abuse
18
AT-A-GLANCE
■ Child abuse, elder abuse, and domestic violence are common and affect patients of all socioeconomic classes and races.
■ Identifying specific cutaneous findings concerning for physical abuse allows for early intervention to impact outcomes.
■ Bruising on soft padded areas of the body and patterned bruising that are multiple and in different stages of healing are suspicious of abuse.
■ Burns that are bilateral and uniform are suspicious of abuse.
■ Law mandates the reporting of all suspected cases of child abuse and, in some states, elder abuse.
INTRODUCTION
Abuse is a world-wide medical issue that is notoriously difficult to diagnose in those who are either not able to provide reliable histories (especially seen in pediatric, geriatric, or cognitively impaired patients) or those who fear the ramifications of reporting abuse (pertinent to any victim of abuse). The main diagnostic challenge lies in the various manifestations of physical abuse due to great diversity of patients and range of means used to inflict trauma. Injuries can result from primary trauma (abrasions, hematomas, choke marks) or secondary effects of an initial trauma (such as in thermal injuries). Superficial cutaneous signs can also indicate the presence and extent of internal injury. Both severe penetrating and blunt trauma can cause bone fractures, torn ligaments, and joint instability. Internal organ hemorrhage can produce fatal consequences and are especially of concern in (though not exclusive to) head and abdominal injuries. Identifying specific cutaneous findings concerning for physical abuse may allow for early intervention to impact outcomes.
EPIDEMIOLOGY
Types of abuse and their respective incidence rates are listed in Table 102-1. More than 1 type of abuse can occur simultaneously.9,10
CHILD ABUSE
CHILD ABUSE
Despite potentially severe morbid and even fatal consequences, child abuse remains under-identified
and thus under-reported.1,2 In the United States, child abuse/neglect annual incidence is 700,000 to 1.25 million children, with approximately 18% of cases involving physical abuse.3-5 Among the United States and developed countries of Europe, the prevalence of physical abuse anytime throughout childhood ranges from 5% to 16%, with only 5% of all episodes estimated to be reported to child protective services.6,7 It is estimated that more than 300,000 children suffer from sexual abuse each year in the United States. The lifetime risk of sexual abuse is approximately 25% to 40% for girls and approximately 10% for males.
ELDER ABUSE
ELDER ABUSE
Elder abuse is one of the fastest-growing forms of abuse. Although statistics vary, the National Center on Elder Abuse in Washington, DC, estimates that 1 to 2 million Americans 65 years of age or older are victims of various forms of abuse each year. Abuse may affect a range of 2% to 10% of the elderly population. Those older than age 80 years are 2 to 3 times more likely to suffer abuse, and the American population in this age range continues to increase each year. True prevalence is difficult to determine as diagnoses can be often missed, with one study claiming that for every case of reported elder abuse, at least another 5 cases go undetected.8 All segments of society are affected.
DOMESTIC ABUSE
DOMESTIC ABUSE
Conservative estimates say that in the United States approximately 1 million people suffer domestic violence each year, but the actual number likely approaches 4 million. Women comprise approximately 90% to 95% of all victims, and men account for 95% of all perpetrators. Forty percent to 60% of men who abuse their partner or spouse are also abusing their children. In the United States, approximately 1 in 3 women suffers at least 1 physical assault during her life, and 1500 women are murdered by their husbands or boyfriends each year.11,12
CLINICAL FEATURES— CUTANEOUS FINDINGS
Because many forms of physical abuse have external manifestations, the skin examination may serve as important evidence that abuse is taking place. Implausible history can provide the first warning sign,
18
■Neglect: 55%
■Neglect: 55%
■Physical abuse: 15%
■Physical abuse: 15%
■Financial and material abuse: 12%
■Financial and material abuse: 12%
■Emotional or psychological abuse: 8%
■Emotional or psychological abuse: 8%
■Sexual abuse: 1%
■Sexual abuse: 1%
■Unspecified forms of abuse: 9%
■Unspecified forms of abuse: 9%
particularly when the clinical examination and extent of injury does not match up with the proposed mechanism of trauma. Explanations for injury should be both comprehensible and coherent; providers should seek to identify congruence between history provided and physical examination findings.13 Because of the significant heterogeneity of cutaneous clinical findings, morphology as well as traditional diagnostic criteria (localization, patterned injuries, repeated injuries, clustered injuries) helps to identify concerning lesions suspicious for abuse. In particular, morphology and localization are key features in forensic classification of abuse.13
MORPHOLOGY
MORPHOLOGY
Just as in all other facets of dermatology, morphology is key to accurate diagnosis. Examination of secondary lesions to determine concern for abuse requires inspection of size, shape (discussed in the section “Patterned Injuries”), color, and location (discussed in the section “Localization”), but also palpation to determine texture and degree of pain. These clinical features can vary based on the anatomic site, the degree of force used, the firmness of the object delivering the force, and the underlying health of the injured individual. Although penetrating wounds develop from trauma due to sharp objects, bruises result from blunt injury. Multiple bruises of differing colors may indicate repeated trauma rather than one isolated incident. Determining time of injury based on bruise characteristics is challenging as bruise color depends on the intensity, depth, and location of the injury. However, evidence suggests that a bruise with a yellow hue is likely older than 18 hours, but a bruise may be red, blue, or purple/black throughout its life span, from onset to resolution. Bruises of identical age and cause on the same person may not appear as the same color and may not change at the same rate.14 Faint bruising can be better appreciated with use of a Wood lamp.
CHILD ABUSE
Confounding early identification and diagnosis of abuse in this population, active children (especially toddlers) are prone to multiple accidental bruises. Although there are no absolute features to differentiate accidental bruising from intentionally inflicted
1718
bruising, location can be the most helpful for identifying abuse (see below).
ELDERLY ABUSE
Cutaneous morphologies that are more unique and specific to elderly abuse include bed sores and strangely patterned alopecia.
LOCATION
LOCATION
Injury distribution can vary. Although the head is a common target of physical abuse in children, centrally located injuries are more common in domestic abuse. Perpetrators in any cases of abuse may choose to injure hidden areas, such as the breast or genitals, to deter detection. Black eyes are often seen in accidental injuries but are more suspicious if they are bilateral or are unaccompanied by evidence of trauma to the nose or superior orbital ridge. Accidental bruising or other injuries to the oral mucous membranes are unusual and should be considered as suspect.
CHILD ABUSE
Because young children tend to explore in a forward direction, accidental bruises more frequently occur on the distal arms and legs, knees, elbows, and forehead. Soft, padded, posterior, and protected areas of the body are far less likely to be accidentally injured. Bruises on the trunk, buttocks (Fig. 102-1), neck folds, palms/soles, thighs, genitalia, ear lobes, neck, and cheeks are uncommon, so marks in these areas should raise concern. Trauma to the oral cavity including mucosal surfaces, posterior pharynx, teeth, and lingual/labial frenula are concerning findings that warrant abuse consideration.
Face: Subconjunctival hemorrhages can be seen in 0.5% to 13.0% of typical newborns, but a large subconjunctival hemorrhage beyond 1 and 2 weeks of life is
suspicious of abuse. Petechiae in the periorbital region have been seen in children with abuse-related retinal hemorrhages.
Genitalia: Per the American Academy of Pediatrics, sexual abuse is the engaging of a child in sexual activities that the child cannot comprehend, for which the child is developmentally unprepared, and cannot give informed consent and that violate the social taboos of society.15 Thus, as sexual abuse is not limited to physical abuse of genitalia, most victims of sexual abuse have no physical findings.16,17 Although genital maltreatment (including touching, fondling, and penetration) can affect victims of all ages, the focus of sexual abuse in this chapter will be on its cutaneous manifestations in pediatric patients. Acute genital or anal injuries without plausible explanation and marked hymeneal opening enlargement with associated hymeneal disruption are very definitive signs of sexual abuse, yet these are not commonly present. The American Academy of Pediatrics Committee on Child Abuse and Neglect recommends that certain findings are consistent with, but not diagnostic of, abuse. These include chafing, abrasions, or bruising of the inner thighs and genitalia, scarring, tears or distortion of the hymen, a decreased amount or absent hymeneal tissue, scarring of the fossa navicularis, injury to or scarring of the posterior fourchette, scarring or tears of the labia minora, and enlargement of the hymeneal opening, even without disruption of the hymen.15
Genital warts pose a particularly difficult problem for practitioners. They certainly can be sexually transmitted to children, and the possibility of sexual abuse needs to be discussed with parents. However, there is much evidence that genital warts can be acquired perinatally from an infected mother, through autoinoculation from warts on other parts of the body, or through nonsexual contact with caretakers.18 Children younger than 3 years of age at the onset of warts are least likely to have acquired their warts from sexual contact, whereas children with onset after 5 years of age have a much greater risk of having suffered sexual abuse. The ages in between represent a gray zone. Of note, human papillomavirus typing is not helpful.
DOMESTIC ABUSE
Unlike infants or debilitated adults, blows to a young adult may be to areas suggesting a defensive posture and might include purpura, sprains, dislocations, and fractures to the wrist or forearms, palms, and soles.
DISTRIBUTION
DISTRIBUTION
Injuries in particular distributions, namely those that are repeated, clustered, and/or patterned injuries are more concerning for intentional abuse. Repeated injuries pertain not only to multiple injuries in various stages of healing but also history of recurrent injuries of similar distribution. Regarding clustered injuries,
18
while the rule of 3 or more individual injuries in the same body region is a classic guideline for raising concern for abuse, one study further identified concerning clustered injuries by age. Pre-mobile children should rarely have more than one isolated bruise, whereas infants who crawl/cruise infrequently have more than 2 bruises especially in the same body region, as compared with children who walk and have commonly greater than 5 or more bruises that may or may not be clustered based on location and activity.22
Certain patterned injury findings can reveal method of abuse and can provide a more specific clinical indicator of abuse. Inflicted bruises often leave patterned imprints of a hand, whip, or hard object. Linear purpura, with a small triangle at the base (Fig. 102-2) representing the interdigital and finger web spaces, occurs after a slap injury. Grab or pinch marks can be recognized by their location on soft padded areas and their unusual patterning. Circumferential purpura or hemosiderin pigmentation (Fig. 102-3) suggests a ligature injury,
1719
18
which would be difficult to explain as accidental. Tramline bruising, distinguished as 2 parallel linear bruises with appearance of preserved “normal skin” within the lines, results from trauma usually with a rectangular or round object (though an ovoid instrument can produce a variant finding). Tramline bruising results after a “high velocity” impact causes rupture of blood vasculature along the edges of the object with shunting of blood throughout the surface of contact with the skin. Withdrawal of the object allows blood from the periphery to return to the site of contact with preservation of vasculature of the center of the contact surface. Blood then extravasates from the damaged vasculature of the edges of impacted skin producing the parallel/symmetrical bruising pattern with often normal appearance of central impacted skin. Bite marks (Fig. 102-4) are always inflicted, although they are sometimes from children or pets. The shape and size of the marks can identify an adult mouth versus a bite from a child. Inflicted burns can result from hot objects (such as iron, cigarette, spatula) applied to skin to cause shaped injuries. The most common agent involved in childhood burns (both accidental and inflicted) is hot liquid. Accidents such as inadvertently stepping into a hot tub or pulling a hot liquid off a table counter or stove leave irregular or geographic burn patterns that lack symmetry. By contrast, inflicted scalds tend to be symmetric, with sharply demarcated edges and an absence or paucity of splash marks characterized by tapered edges. In one study, all the children whose bathtub burns were inflicted had associated features of abuse, including bruises, fractures, or evidence of neglect.19 Stocking and glove burns result when the feet or hands are forcibly held under hot water. The uniformity of the burn indicates that the child was not able to reflexively withdraw from the scalding water as would happen with accidental immersion. A common pattern of inflicted immersion burn involves the buttocks, low back, and thighs. The child is flexed at the waist and dipped into the hot water, frequently as a punishment for a toilet training accident. The resultant pattern may give “zebra stripes” on the abdomen due to sparing of
1720
the flexural skin that is protected from the scald when bent forward. A “donut hole” pattern of sparing might be seen on the buttock if the child is pushed forcibly to the bottom of the tub that is cooler than the scalding water.20 Inflicted splash burns are much more difficult to differentiate from accidents. An inflicted contact burn can be recognized by the pattern that duplicates the object creating the injury. Accidental contact burns tend to be smaller, less severe, less patterned, and of irregular depth. When a patient is held against a hot object, the depth is more uniform, the pattern is more clearly defined, and the burn is more severe. Irons, curling irons, hot plates, and cigarettes are objects commonly used to inflict burns.21 Some burns may, in fact, be accidental but represent inadequate supervision and neglect. This situation is also harmful and needs to be reported to the appropriate agencies.
ETIOLOGY AND PATHOGENESIS/RISK FACTORS
CHILD ABUSE
CHILD ABUSE
Victims and perpetrators span all racial, religious, and socioeconomic spectrums; however, identified factors placing children at higher risk for being victims of abuse are classified into characteristics of the patient, the provider, and the environment (society and community).23 Typical children who suffer abuse have emotional, behavioral (including ADHD), or learning disabilities; have chronic illnesses (including failure to thrive and congenital anomalies) with special medical needs; may be premature at birth with low birth weight; have several siblings; resulted from unwanted pregnancy and/or deemed an unwanted child; live in single-parent households; or live at or below the poverty level. Girls are more likely than boys to suffer sexual abuse and the risk rises in preadolescence (Fig. 102-5). Perpetrators tend to have
emotional or psychological problems, have frequently been victims of abuse themselves, abuse drugs or alcohol, are perpetrators of spousal abuse or have a history of marital discord, have marginal parental skills or knowledge, absentee mothers (extensively out of the home), and have poor self-esteem. Parents are the perpetrator 80% of the time24; only 10% child abuse is estimated as inflicted by strangers. Most common environmental factors seen in the setting of child abuse include poverty, social isolation, unrelated adult male in household, single-parent families, and significant family stressors. Although these profiles are helpful, it is important to remember that any child may be the victim of abuse.
ELDERLY ABUSE
ELDERLY ABUSE
Risk factors for abuse are listed in Table 102-2. Note that the risk factors have far more to do with the caretaker than the abused patient. In particular, the level of debility or health status of the patient does not predict abuse. Abuse most often occurs at the hands of caregivers or family members who have frequent close contact with patients and often may live with them. Historically, adult children of the abused patient have been the most common perpetrators, but most recent data show that spouses now account for the majority of abuse cases. Men are more likely to abuse than women. The abuser is often financially dependent on the victim, and they are usually in a shared living situation. However, financial abuse is more common among those who live alone.
DOMESTIC ABUSE
DOMESTIC ABUSE
Women ages 19-29 years are the most common victims, with other risk factors being low income, mental health issues, alcohol or substance abuse by the victim or the perpetrator, pregnancy, large age difference between partners, separated or divorced status, and a family history or personal past history of abuse and violence. Women with educational or occupational levels above
■Older age
■Older age
■Lack of access to resources
■Lack of access to resources
■Low income
■Low income
■Social isolation
■Social isolation
■Minority status
■Minority status
■Low level of education
■Low level of education
■Functional impairment
■Functional impairment
■Substance abuse by elder or caregiver
■Substance abuse by elder or caregiver
■Previous history of family violence
■Previous history of family violence
■History of psychological problems
■History of psychological problems
■Caregiver stress
■Caregiver stress
■Cognitive impairment
■Cognitive impairment
18
that of their partners may be at higher risk. Abusers are typically underachievers with occupational status below their educational level.11,12
DIAGNOSIS
CHILD ABUSE
CHILD ABUSE
A careful history is needed to detect inconsistencies between the proposed injury and the physical examination. Identified red flags to trigger suspicion for abuse include unexplained delay in presentation, caregiver’s history provided that is inconsistent or conflicting, denial of trauma despite concerning injury, trauma secondary to in-home resuscitation attempts, and severe injury for which blame is placed on pets or young children. As fall height and ground surface have been found to be predictors of severity of injury, short fall history in a child presenting with significant injuries should trigger suspicion for abuse.25 The history should include as much detail as possible and inconsistencies in the parent’s story clearly documented in the medical record.26
All historical information must be very well documented and preserved with the same care as any piece of forensic evidence. It is immensely important to enlist the help of an experienced abuse team in obtaining the history and completing an appropriately thorough physical examination. It is essential to perform a total body, skin, and mucous membrane examination. It is also important to note the child’s behavior and parent-child interactions. The color of all bruises should be noted and clearly documented. This may aid in determining the age of a bruise and may point out inconsistencies in the caretaker’s history. It is helpful to include a ruled measuring scale in any photographs to help forensic identification at a later date. Most importantly, the child’s spoken word is a valuable piece of evidence in establishing sexual abuse.
ELDERLY ABUSE
ELDERLY ABUSE
The US National Academy of Sciences has defined elder abuse as:
(a) intentional actions that cause harm or create a serious risk of harm (whether or not harm is intended) to a vulnerable elder by a caregiver or other person who stands in a trust relationship to the elder, or (b) failure by a caregiver to satisfy the elder’s basic needs or to protect the elder from harm.
Acts of commission and omission are thus included in the definition. Unexplained repetitive injuries or explanations by caretakers that do not match the pattern of injury are concerning. Caretakers who act withdrawn, infantilize the patient, or insist on providing the medical history should alert the clinician.
1721
18
It is important to interview by directing questions to the patient rather than the caregiver, and it is prudent to try to arrange a time to confer with and examine the patient alone. Repetitive followup visits help develop a rapport with the patient and allow serial observation of past and ongoing injuries. The assurance of confidentiality facilitates garnering sensitive information.
DOMESTIC ABUSE
DOMESTIC ABUSE
Domestic violence is a pattern of coercive behaviors that may include repeated battering, psychological abuse, sexual abuse, social isolation, deprivation, and intimidation perpetrated by someone who is or was involved in an intimate relationship with the victim. Whenever possible, the patient should be interviewed alone in the absence of her or his partner. A thorough examination should be done with a nurse chaperone, but not the partner, in the room. Repeat visits may be used to document new or progressing skin findings and to build trust with the patient. For various reasons, a victim may not want to reveal abuse. Implausible explanations for an injury or a delay in seeking medical attention may be clues of abuse. Signs of depression, excessive use of sedatives, chronic pain disorders, or vague stress-related symptoms may be subtle signs of abuse.11
SUPPORTIVE STUDIES— LABORATORY TESTING
The advised laboratory workup is patient presentationdependent. Although there is an argument for obtaining basic bleeding studies (to include complete blood count with differential, platelet count, prothrombin and partial thromboplastin times) in all cases of suspected child abuse, the recommendation for other laboratory studies varies based on patient presentation. Coagulation studies are helpful in identification of coagulopathy following trauma and can help to differentiate this from an underlying preceding coagulopathy. The above basic bleeding studies can be supplemented with additional coagulation studies, though hematology should be involved in opting for this more aggressive workup approach.23,27
For intraabdominal trauma, transaminase (alanine aminotransferase [ALT], aspartate aminotransferase [AST]) levels are elevated in those with hepatic damage whereas serum amylase and lipase are elevated in those with pancreatic injury.28 Even in the absence of cutaneous findings to suggest intraabdominal trauma, transaminases can be elevated (greater than 80 U/L) correlating with hepatic injury in an abused child.23 An observational study reported 17 of 54 children with no clinical findings to have intraabdominal injury, with 14 of the 17 injured to have elevated transaminases. Thus, not all patients with abdominal trauma have cutaneous manifestations nor is serologic testing perfectly
1722
sensitive to detect intraabdominal injury following abuse. Followup study performed noted transaminase elevation to be 83% specific and 84% sensitive for detection of such occult injury.29
Other serologies are ordered if suspecting specific injuries including serum electrolytes and osmolality for abusive head trauma; water intoxication or dehydration; as well as serum phosphate, calcium, and alkaline phosphatase in the setting of fractures to rule out bone disease as an underlying etiology. Workup for bone fragility is controversial, with no clear guidelines for screening; thus, it is proposed to consult with a bone metabolism expert should a child present with only fractures in the absence of cutaneous findings to suggest abuse.23,30
Urinalysis should be considered in patients with convincing history or examination suspicious for dehydration, abdominal trauma, or concerning urinary symptoms, such as hematuria (common finding following genitourinary or abdominal injury). If heme is found in the urine in the absence of red blood cells, further workup for rhabdomyolysis would then be warranted. Toxicology testing can be performed but should be ordered based on patient presentation and clinical suspicion for the inappropriate administration of medications and street drugs. Regional poison control centers throughout the United States are always available for consultation and should be involved in unclear clinical cases and in critically ill patients.
SUPPORTIVE STUDIES—IMAGING
Imaging studies are case-dependent and should be tailored to the patient based on age, history, and examination.31 Radiographic studies can aid in determining the extent of injury in intentional cases, but such studies can also help to provide an alternative etiology to injuries, especially fractures.31-33
FRACTURES
FRACTURES
Fractures concerning for intentional trauma include: bilateral long bone acute fractures, metaphyseal corner fractures, long bone fracture in a non-ambulatory child, epiphyseal separations, rib/sternal/spinous process/scapular fractures, fractures of variable healing stages, digital fractures in children younger than 36 months, and vertebral subluxations/fractures without high force trauma, and severe skull fractures in children younger than 18 months. Despite being widely regarded as the superior study for detection of fractures in abused children,23,3134-36 skeletal surveys were found to rarely provide information supplemental to history and physical examination in newly diagnosed isolated skull fracture in infants, to help with determination of report to child protective services.37
HEAD INJURY
HEAD INJURY
Neuroimaging has been proposed as indicated in all patients with suspected nonaccidental head trauma as well as all children younger than 6 months with any suspected injury.23,34,38,39 Unenhanced CT of the head is the recommended imaging for initial workup and evaluation. Among cases of child abuse, in the absence of neurologic symptoms, patient age less than 1 year is the only key factor found to predict more thorough diagnostic evaluation. Considering history and examination to be poorly sensitive when compared with neuroimaging detected abnormalities, providers should have low threshold for neuroimaging in the setting of suspected child abuse,40 as there are no specific physical findings to identify abusive head trauma. Although any physician can perform an eye examination, ophthalmology referral is recommended in the setting of concern for abusive head trauma, given the subjective nature of funduscopy and rendering a diagnosis of retinal hemorrhage.
VISCERAL TRAUMA
VISCERAL TRAUMA
Esophageal, cardiac, pulmonary, or intraabdominal injury can be caused by many different methods of abuse with variable presenting signs and symptoms. Low threshold is warranted to perform such imaging, especially considering the need for early diagnosis of such organ injury with prompt intervention.
DIFFERENTIAL DIAGNOSIS
A broad knowledge of skin diseases provides a unique insight into those diagnoses that may mimic various forms of abuse, namely, child abuse (Tables 102-3 and 102-4) and sexual abuse (Table 102-5).
ELDERLY ABUSE
ELDERLY ABUSE
Diagnosis of abuse can be especially challenging in the elderly population because of bruising being so common in this population. Not only does the normal process of aging entail increased skin fragility, but this patient population is more likely to be on medications causing ease of bleeding, particularly blood thinners.
CLINICAL COURSE AND PROGNOSIS
Early recognition and prompt diagnosis allows for expeditious intervention to allow for appropriate medical treatment. Additionally, taking steps to provide protection from perpetrators helps to prevent recurrence and optimizes prognosis.
18
■True petechiae and purpura
■True petechiae and purpura
■Disorders of coagulation
■Disorders of coagulation
■Ehlers-Danlos syndrome
■Ehlers-Danlos syndrome
■Infections
■Infections
■Rocky Mountain spotted fever
■Rocky Mountain spotted fever
■Meningococcal infections
■Meningococcal infections
■Group A streptococcal infections
■Group A streptococcal infections
■Palpable purpura of vasculitis
■Palpable purpura of vasculitis
■Valsalva petechiae
■Valsalva petechiae
■Lichen sclerosus
■Lichen sclerosus
■Folk remedies
■Folk remedies
■Cao gio: rubbing vigorously with a hard object such as a coin
■Cao gio: rubbing vigorously with a hard object such as a coin
■Cupping: suction mark left by the cooling of a warm metal cup
■Cupping: suction mark left by the cooling of a warm metal cup
■Nodular lesions mimicking deep bruises
■Nodular lesions mimicking deep bruises
■Neuroblastoma
■Neuroblastoma
■Vascular malformations
■Vascular malformations
■Dermatomyositis-associated nodules
■Dermatomyositis-associated nodules
■Erythema nodosum
■Erythema nodosum
■Discolorations that look like bruises
■Discolorations that look like bruises
■Phytophotodermatitis
■Phytophotodermatitis
■Maculae caeruleae from lice infestation
■Maculae caeruleae from lice infestation
■Mongolian spots
■Mongolian spots
■Dye from blue jeans
■Dye from blue jeans
■Inflammatory conditions that mimic bruising
■Inflammatory conditions that mimic bruising
■Urticaria/angioedema/urticarial vasculitis
■Urticaria/angioedema/urticarial vasculitis
■Pernio
■Pernio
■Conditions that mimic whip marks
■Conditions that mimic whip marks
■Incontinentia pigmenti
■Incontinentia pigmenti
■Striae
■Striae
■Phytophotodermatitis
■Phytophotodermatitis
CHILD ABUSE
CHILD ABUSE
Pediatric patients who suffer from abuse that was not initially promptly diagnosed with the first offense have up to 50% risk of a second event.41-44 One retrospective study identified children in ED thought to have accidental traumatic injuries, reporting 13% of these patients to present for second physical abuse injury
■Phytophotodermatitis
■Phytophotodermatitis
■Folk remedies (Maquas, or moxibustion): burns delivered near diseased organs or therapeutic sites as in acupuncture
■Folk remedies (Maquas, or moxibustion): burns delivered near dis-
eased organs or therapeutic sites as in acupuncture
■Impetigo/ecthyma
■Impetigo/ecthyma
■Epidermolysis bullosa
■Epidermolysis bullosa
■Immunobullous diseases
■Immunobullous diseases
■Sunburn/xeroderma pigmentosum
■Sunburn/xeroderma pigmentosum
■Burns from objects heated by sun
■Burns from objects heated by sun
■Electric burn from an enuresis blanket
■Electric burn from an enuresis blanket
■Chemical burn from use of undiluted acetic acid
■Chemical burn from use of undiluted acetic acid
■Chemical burn from Icy Hot balm
■Chemical burn from Icy Hot balm
■Chemical burn from calcium chloride
■Chemical burn from calcium chloride
■Diaper dermatitis
■Diaper dermatitis
■Pernio
■Pernio
1723
■Fixed drug eruption
■Fixed drug eruption
18
■Lichen sclerosus
■Lichen sclerosus
■Crohn disease
■Crohn disease
■Localized vulvar pemphigoid
■Localized vulvar pemphigoid
■Langerhans cell histiocytosis
■Langerhans cell histiocytosis
■Perianal streptococcal dermatitis
■Perianal streptococcal dermatitis
■Hemangiomas
■Hemangiomas
■Urethral prolapse
■Urethral prolapse
■Entities that look like condylomata acuminata
■Entities that look like condylomata acuminata
■Focal epithelial hyperplasia
■Focal epithelial hyperplasia
■Darier disease
■Darier disease
■Lymphangioma circumscriptum
■Lymphangioma circumscriptum
■Pigmented vulvar hamartomas
■Pigmented vulvar hamartomas
■Pseudoverrucous papules
■Pseudoverrucous papules
■Epidermal nevus and inflammatory linear verrucous epidermal nevus
■Epidermal nevus and inflammatory linear verrucous epidermal
nevus
■Entities that look like herpes simplex
■Entities that look like herpes simplex
■Localized varicella/zoster
■Localized varicella/zoster
■Allergic contact dermatitis
■Allergic contact dermatitis
within 5 years of first event.45 In the United States, deaths related to child abuse/neglect incidence is estimated to reach up to 2500 deaths annually (predominantly of infants less than 1 year of age).6 The World Health Organization (WHO) proposed that 13% of the 1.2 million deaths worldwide of children younger than 15 years to be due to child abuse/neglect.6
MANAGEMENT
True abuse must be reported and a thorough evaluation conducted. It is essential that practitioners develop a relationship with the institution or individual in their area who is best able to manage these difficult cases. Ideally, there should be an abuse team consisting of a dermatologist, pediatrician, social worker, medical photographer, and, when needed, pediatric subspecialists such as orthopedists, hematologists, psychologists, and gynecologists. The need for specialization in this field is highlighted by the institution in the United States of pediatric subspecialty board certification in child abuse, beginning in 2010. It is most helpful if one’s relationship is forged with the abuse team before an abuse incident and a set protocol for dealing with alleged or suspected abuse is established in the practitioner’s office. Hospitalization is indicated not only for medical stabilization to workup and manage acute injuries, but also in select patients to ensure safety from his or her perpetrator. Many countries including the United States require reporting any cases of suspected abuse to appropriate government authorities. Documentation is essential and should include a recount of the (preferably quoted) spoken word (by patient and by any other involved individuals, including providers and family members) as well as detailed physical examination findings with reliance on facts. Photographs are ideal for documentation of injuries.
1724
CHILD ABUSE
CHILD ABUSE
Local emergency phone numbers for reporting abuse can be obtained from the Child Welfare Information Gateway or Childhelp National Headquarters.
ELDERLY ABUSE
ELDERLY ABUSE
Information on a particular state’s laws can be obtained from the National Center on Elder Abuse. The nearest medical center’s social service department is well equipped to offer guidance, but the agencies listed in Table 102-6 are also helpful resources.
DOMESTIC ABUSE
DOMESTIC ABUSE
The social service department at the local medical center is a good resource for information and help on domestic violence. The National Domestic Violence hotline (800-799-7233) is a 24-hour resource for women who need to find a local shelter. Other helpful organizations can be contacted (Table 102-6).
■Child Welfare Information Gateway, 1250 Maryland Avenue, SW, Eighth Floor, Washington, DC 20024, Ph: (800) 394-3366, email: info@childwelfare.gov, http://www.childwelfare.gov/
■Child Welfare Information Gateway, 1250 Maryland Avenue, SW,
Eighth Floor, Washington, DC 20024, Ph: (800) 394-3366, email: info@childwelfare.gov, http://www.childwelfare.gov/
■Childhelp National Headquarters, 15757 N. 78th Street, Suite B, Scottsdale, AZ 85260, Ph: (480) 922-8212, http://www .childhelpusa.org
■Childhelp National Headquarters, 15757 N. 78th Street, Suite B,
Scottsdale, AZ 85260, Ph: (480) 922-8212, http://www .childhelpusa.org
■Domestic Violence International Resources, http://www.vachss. com/help_text/domestic_violence_intl.html
■Domestic Violence International Resources, http://www.vachss.
com/help_text/domestic_violence_intl.html
■International Network for the Prevention of Elder Abuse, http://www.inpea.net, e-mail contactus@inpea.net
■International Network for the Prevention of Elder Abuse,
http://www.inpea.net, e-mail contactus@inpea.net
■International Society for Prevention of Child Abuse and Neglect, 13123 E. 16th Ave, B390, Aurora, CO 80045, Ph: (303) 864-5220, Fax: (303) 864-5222, email: ispcan@ispcan.org, http://www.ispcan.org
■International Society for Prevention of Child Abuse and Neglect,
13123 E. 16th Ave, B390, Aurora, CO 80045, Ph: (303) 864-5220, Fax: (303) 864-5222, email: ispcan@ispcan.org, http://www.ispcan.org
■National Adult Protective Services Association, 920 S. Spring Street, Suite 1200, Springfield, IL 62704, Ph: (217) 523-4431, Fax: (217) 522-6650, http://www.apsnetwork.org
■National Adult Protective Services Association, 920 S. Spring Street,
Suite 1200, Springfield, IL 62704, Ph: (217) 523-4431, Fax: (217) 522-6650, http://www.apsnetwork.org
■National Center on Elder Abuse, c/o Center for Community Research and Services, University of Delaware, 297 Graham Hall, Newark, DE 19716, Ph: (302) 831-3525, Fax: (302) 831-42525, e-mail ncea-info@aoa.hhs.gov, http://www.elderabusecenter.org
■National Center on Elder Abuse, c/o Center for Community
Research and Services, University of Delaware, 297 Graham Hall, Newark, DE 19716, Ph: (302) 831-3525, Fax: (302) 831-42525, e-mail ncea-info@aoa.hhs.gov, http://www.elderabusecenter.org
■National Committee for the Prevention of Elder Abuse, 1612 K Street, NW, Suite 400, Washington, DC 20006, Ph: (202) 682-4140, Fax: (202) 223-2099, email: ncpea@verizon.net, http://www .preventelderabuse.org
■National Committee for the Prevention of Elder Abuse, 1612 K
Street, NW, Suite 400, Washington, DC 20006, Ph: (202) 682-4140, Fax: (202) 223-2099, email: ncpea@verizon.net, http://www .preventelderabuse.org
■National Coalition Against Domestic Violence, 1120 Lincoln Street, Suite 1603, Denver, CO 80203, Ph: (303) 839-1852, Fax: (303) 831-9251, email mainoffice@ncadv.org, http://www.ncadv.org
■National Coalition Against Domestic Violence, 1120 Lincoln Street,
Suite 1603, Denver, CO 80203, Ph: (303) 839-1852, Fax: (303) 831-9251, email mainoffice@ncadv.org, http://www.ncadv.org
■National Resource Center on Domestic Violence, 6400 Flank Drive, Suite 1300, Harrisburg, PA 17112, Ph: (800) 537-2238 ext. 5, Fax (717) 545-9456, http://www.nrcdv.org
■National Resource Center on Domestic Violence, 6400 Flank
Drive, Suite 1300, Harrisburg, PA 17112, Ph: (800) 537-2238 ext. 5, Fax (717) 545-9456, http://www.nrcdv.org

Figure 102-1 Purpura and erosions on the soft, padded areas of the buttock and thighs, representing very obvious abuse. (Used with permission from Paul Bellino, MD.)

Figure 102-2 Linear purpura representing the interdigital spaces from a hand slap. Note the inferior triangular shape that corresponds to the finger web space. (Used with permission from Paul Bellino, MD.)

Figure 102-3 Linear, circumferential hyperpigmentation at the site of previous ligature. (Used with permission from Paul Bellino, MD.)

Figure 102-4 Human bite marks. (Used with permission from Paul Bellino, MD.)

Figure 102-5 Sexual abuse. Perianal wound in a 3-year-old girl after anal penetration. (Used with permission from Dr. Francesca Navratil, Zurich, Switzerland.)
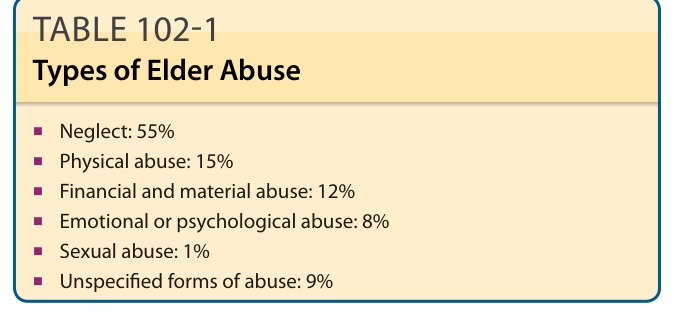
TABLE 102-1 Types of Elder Abuse
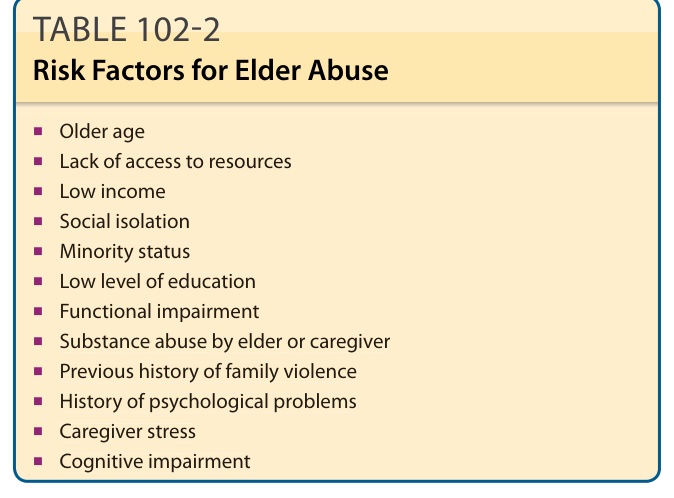
TABLE 102-2 Risk Factors for Elder Abuse
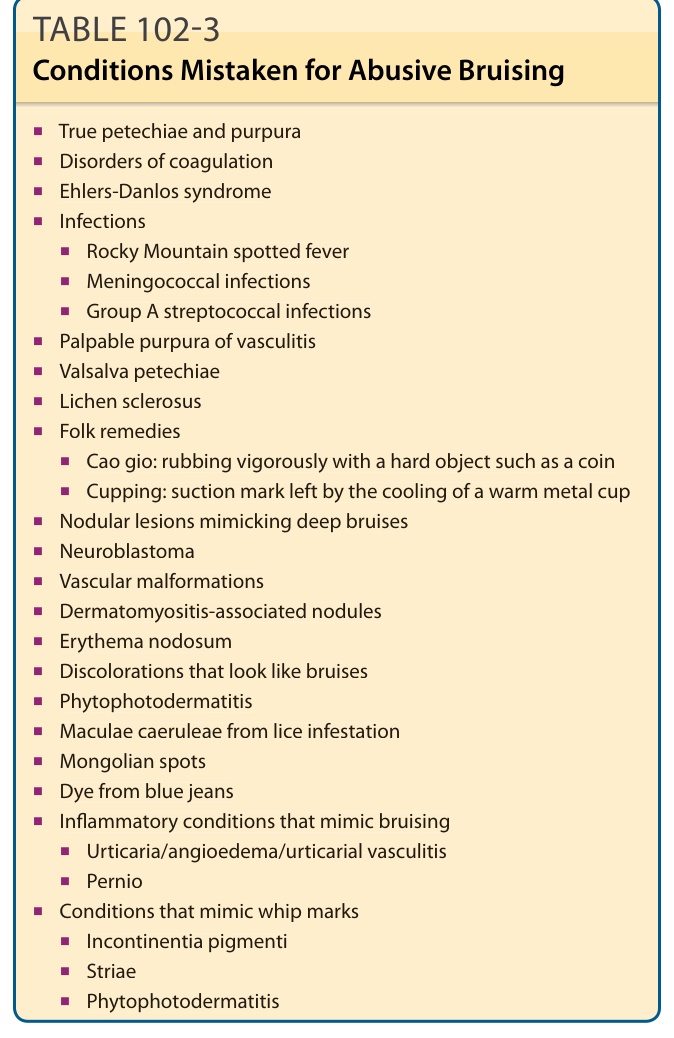
TABLE 102-3 Conditions Mistaken for Abusive Bruising
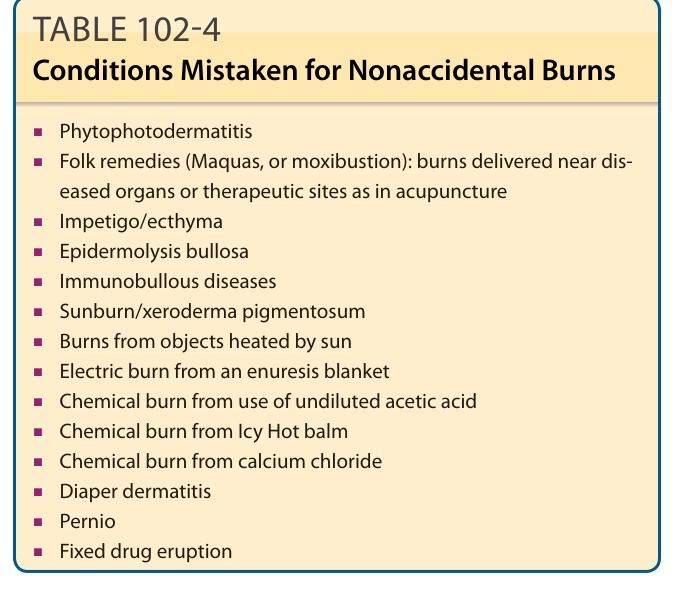
TABLE 102-4 Conditions Mistaken for Nonaccidental Burns
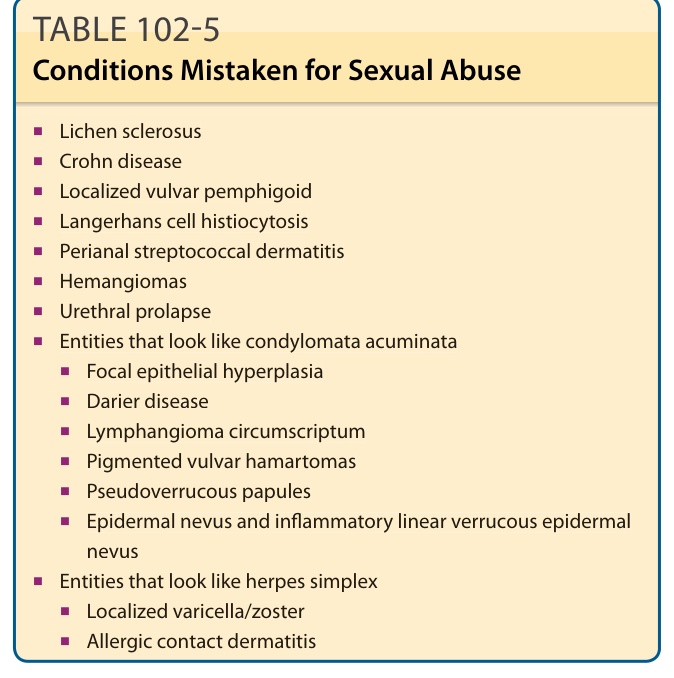
TABLE 102-5 Conditions Mistaken for Sexual Abuse
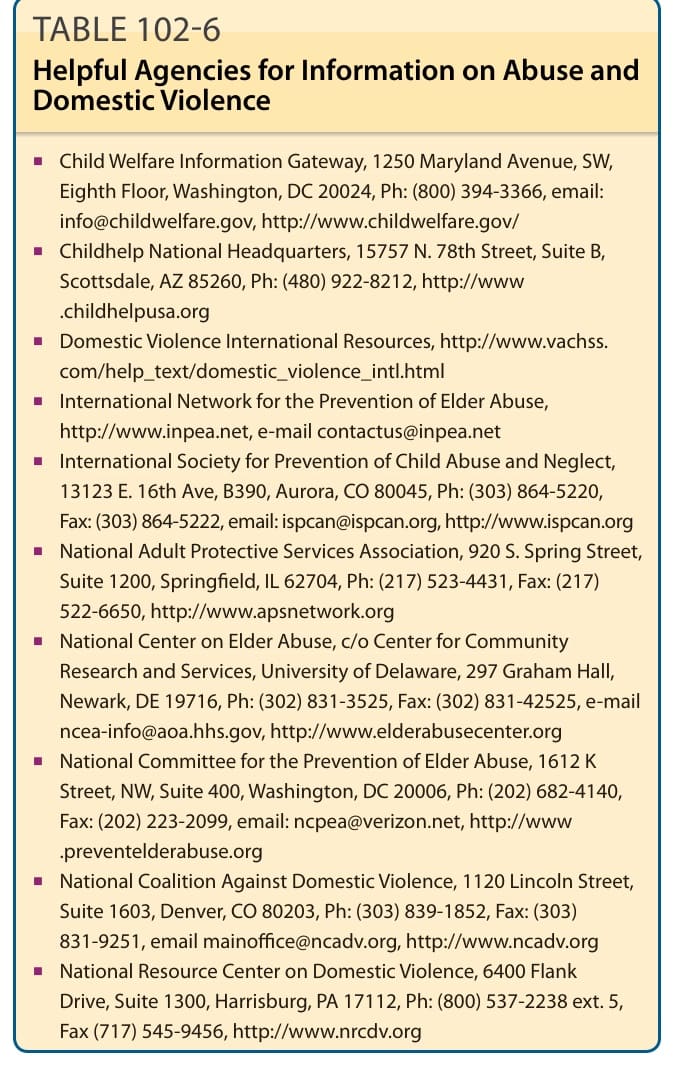
TABLE 102-6 Helpful Agencies for Information on Abuse and Domestic Violence