Drug Abuse
18
AT-A-GLANCE
■ Drug use is a growing problem in the United States and around the world. There are many cutaneous findings that suggest use, abuse, and addiction to drugs.
■ Specific findings in affected patients include dental caries, madarosis, presence of scarring, tattooing, and staining in the skin.
■ Levamisole causes a unique syndrome characterized by retiform purpura of the ears associated with neutropenia, perinuclear antineutrophil cytoplasmic antibody and anti- MPO3 antibodies.
■ Less-specific findings of drug use include morbilliform eruptions, vasculitis, and formation of autoantibodies.
■ Drug-use–related infections predominantly affect the skin and soft tissues. Staphylococcal species are the most common organisms, followed by streptococcal species, oral pathogens, and Candida.
■ Other sequelae of drug use include increased risk of infections including HIV, hepatitides B and C, and syphilis.
DEFINITION
The term drug is defined as a medication or other substance, other than food, that has a physiologic effect when ingested or otherwise introduced into the body. Modern society is rife with medications that affect function or structure in the body, caffeine being the most widely used psychoactive substance in the world. Drug abuse is defined as the recurrent use of illegal drugs, or the misuse of nonprescription or prescription drugs, that results in negative consequences. Drug addiction is characterized by physiologic dependence and inability to consistently abstain from the drug. Tobacco and alcohol, although not illegal in the United States and most of the western world, are also considered substances of addiction and abuse.
HISTORICAL PERSPECTIVE
Drugs have been used and abused for thousands of years and all over the world. Use in religious
ceremonies, for healing, or by the general population for recreation has occurred since ancient times. There is evidence that opium has been used since 5000 bc and alcohol since 3500 bc. References to those and other medications are found in the Bible and other religious and historical texts. Columbus and his crew introduced tobacco into Europe when they returned from the New World.
EPIDEMIOLOGY
Based on estimates released in the United Nations Office of Drugs and Crime’s (UNODC) 2015 World Drug Report, 246 million people worldwide—1 of 20 people between 15 and 64 years of age—used an illicit drug in the year 2015, which corresponds to a global prevalence of 5.2%.1 With the exception of caffeine, cannabis is the most widely used drug in the world, and its’ use is increasing. Amphetamines are the second most commonly used drugs worldwide, and their use is also increasing. The use of cocaine was in decline for several years but it too is now on the rise. Opiates, particularly prescription opioids cause the highest negative health impact. Approximately 29.5 million people suffer from drug dependancy world wide, with the highest prevalence of illicit drug use is among those 18 to 25 years of age (1 in 5 persons in this age group). Marijuana was used by 8.2% of the population, making it the most commonly used illicit drug; it is commonly referred to as the “gateway drug” because marijuana use often leads to using other drugs. Prescription pain relievers were the second most commonly used drug, followed in decreasing prevalence by sedatives, stimulants, cocaine, hallucinogens, inhalants, heroin, and sedatives. Approximately 66.9 million people were current tobacco users, a decrease over previous years. An estimated 139.7 million people were current alcohol drinkers (52.7%), including 60.9 million binge alcohol users and 16.3 million heavy alcohol users.
ETIOLOGY AND PATHOGENESIS
The biologic and environmental mechanisms by which an individual comes to abuse certain licit and illicit substances is complex and studies suggest varying levels of genetic and environmental influence. Even though the biochemical changes in the brain
18
that lead to drug abuse are intricate, dopaminergic neural pathways involved in motivation, reward, and habit formation play a central role in many neuropsychiatric conditions, including substance addiction.2
Twin studies suggest that at least some component of drug abuse and dependence is driven by genetic preponderance. Environmental risk factors include easy access to the drug, poor school bonding, and peer use. Trauma, both physical and psychological, parental use and family conflict in the home are associated with use. Several protective factors also have been illustrated, including religiosity and strong family support, as well as social involvement in community organizations.3
DIAGNOSIS
Recognition of signs and symptoms associated with drug use is crucial and potentially lifesaving. Drug testing is the gold standard for diagnosis of most legal and illegal agents. Bodily fluids, including blood, urine, saliva, and hair can be used for drug detection. Suspected infections should be cultured by swab and, when necessary, tissue specimens. Serologic evaluation for transmissible infection, such as HIV, hepatitis, and sexually transmitted diseases, should be considered in appropriate patients.
CLINICAL FEATURES OF DRUG ABUSE (TABLE 101-1)
SIGNS OF INTRAVENOUS DRUG USE
SIGNS OF INTRAVENOUS
DRUG USE
TRACK MARKS
Track marks are the result of venous thrombosis with subsequent scarring (Fig. 101-1) and pigmentation of the veins (Fig. 101-2). Damage results from repeated injections, use of blunt needles, and irritation from chemicals that are added to the injected material. Early lesions show crusting and ecchymosis along the course of a vein; linear cords form with chronic use. The most common site is the medial vein in the antecubital fossa of the nondominant arm.4 However, many people inject in less-visible places, such as the popliteal fossa, dorsal veins of the feet, and inguinal veins.5 As these veins scar, intravenous drug users (IDUs) find other access points and will inject into hemorrhoids, the dorsal vein of the penis, the ventral surface of the tongue, or the internal jugular vein.6 It is important to remember that a lack of track marks does not preclude IV drug use. Scarring is usually associated with a longer
SIGN MOST COMMON DRUG SPECIFIC FINDINGS
Track marks Skin popping Soot tattoos
Cocaine Heroin Scarring along veins and skin
Madarosis Cocaine Heroin Methamphetamine
Hand dermatitis, puffiness, or discoloration Cocaine Heroin Inhalants Cannabis Tobacco
Acne Anabolic steroids MDMA (methylenedioxymethamphetamine) Methamphetamine Cannabis
Vasculitis Cocaine Levamisole Cannabis Tobacco
Formication and/or
Methamphetamine and amphetamines Cocaine Heroin/opiates Alcohol
Formication and/or pruritus Methamphetamine and amphetamines Cocaine Heroin/opiates Alcohol
pruritus
1706
Loss of lateral eyebrows
Erythema, fissuring, edema, or staining
Pustules and nodules May be severe
Cocaine—urticarial vasculitis, midline nasal destruction Levamisole—retiform purpura of ears and elsewhere associated with p-ANCA (perinuclear antineutrophil cytoplasmic antibody) and MPO (myeloperoxidase) Cannabis—cannabis arteritis and thromboangiitis obliterans Tobacco—thromboangiitis obliterans and peripheral vascular disease
Excoriations Prurigo nodules Ulcerations
Excoriations Prurigo nodules Ulcerations
duration of drug use7 and cocaine does not normally induce track marks because it does not typically contain the sclerosing chemicals that are added to other drugs such as heroin.8
SCARS RESULTING FROM SKIN POPPING
Sometimes drug users inject intradermally or subcutaneously. This is done accidentally or when veins can no longer be found and used. Some prefer this method of delivery instead of injecting intravenously. This is called skin popping. It leaves irregular, leukodermic, atrophic, punched out scars that result from irreversible tissue injury. Hypertrophic scars or keloids can develop over these areas.9
PANNICULITIS
Inflammation of the dermis and subcutaneous fat may occur with injection into the skin itself or with extravasation of intended IV administration. Sclerosants, particularly pentazocine, and additives, such as talc, may induce subcutaneous nodules. A lobular panniculitis is often seen on histopathology and the injected material may leave spaces in the tissue after fixation or cause birefringence on tissue polarization.10
HYPERPIGMENTATION
Sooting tattoos are also stigmata of drug abuse. Sooting tattoos are caused by cooking the drugs and
18
flaming the needles with matches. Carbon and soot then deposit into the dermis. Users may cover these with commercial tattoos so they are hidden. Hyperpigmentation can also develop at tourniquet sites when placed too tightly and left on for too long, causing inflammation and subsequent hyperpigmentation.11
SKIN AND SOFT-TISSUE INFECTIONS
Skin and soft tissue infections (SSTIs) are very common among IDUs (Fig. 101-3). SSTIs are the most common disease for which users are usually admitted to the hospital.12 Sepsis, rather than overdose, is the usual acute complication seen in this population. The increased risk of SSTI in IDUs is multifactorial. Independent risk factors were found to be skin popping, the use of nonsterile needles, “speedball” (mixture of heroin and cocaine) injections, and “booting” (drawing back a small amount of blood usually into a dirty syringe prior to injection).11 Skin popping has a fivefold greater risk of infection when compared to IV injection.13 Infections associated with skin popping tend to be multilobulated, deeper, and have more extensive necrosis than those in non-IDUs.8 Females also have an increased risk of SSTIs as compared to male IDUs, which is most likely a consequence of their less-prominent veins leading to more sticks to gain access.14 Any type of immunocompromised state, such as AIDS, increases the risk of SSTIs. The local anesthetic properties of many illegal drugs can also make it difficult for users to feel the injury or realize they are developing an infection. Many different pathogens are responsible for SSTIs in IDUs. Blood cultures are often negative in SSTIs, making it harder to identify the causative organism unless a culture can be performed of an abscess
1707
18
or ulceration. One pathogen is cultured in 50% of the cases, and more than 1 is found in 33% to 45% of cases. The etiologic organism(s) in most SSTIs appear to be from the skin or oral cavity of the user rather than from the drug or paraphernalia used.15 This correlates with other studies demonstrating Staphylococcus species (particularly Staphylococcus aureus) as the most frequently cultured organism, followed by group A β-hemolytic Streptococcus and other streptococcal species and then oral or skin pathogens.16,17 Oral pathogens, including Eikenella corrodens, are also a cause of infection, as IDUs sometimes “clean” their needle or skin prior to injection with their saliva. Drug dealers have also hidden drug containers in their mouths, which was the source of an outbreak of a clonal strain of Streptococcus pyogenes.18 Gram-negative bacteria and anaerobes also may be a cause of infection and the classic signs of anaerobic infections, such as free air bubbles on radiograph or foul smell, may not be present. There have been numerous reports of SSTIs caused by uncommon pathogens. Quinine, which is usually added to heroin, increases the risk of tetanus.19 Clostridium botulinum and Clostridium tetani are unusual organisms except in IDUs who skin pop. Wound botulism most commonly occurs from injection of black tar heroin, which is cut with dirt and is ideal for the growth of botulism because of its high water content. Heating the drug prior to injection actually stimulates the spores to germinate. Wound botulism in IDUs can present with symptoms of blurred
1708
vision, diplopia, and ptosis without any mental status changes. The patient may or may not have a visible cellulitis and may only present with pain, swelling, and tenderness. Approximately 85% of the cases of wound botulism at the time of presentation had wounds that were grossly infected and 65% had C. botulinum isolated from the wound. The diagnostic test of choice is detecting the toxin by standard mouse bioassay of the serum. Treatment includes the antitoxin and high-dose penicillin along with surgical debridement.20 Other Clostridium species, including Clostridium novyi, Clostridium perfringens, Clostridium sordellii, and Clostridium histolyticum, have been reported to be the cause of serious illness or deaths among IDUs. Necrotizing fasciitis (Fig. 101-4) is also common among IDUs. Chen et al reported 55% cases were in IDUs. IDUs with necrotizing fasciitis most commonly present with severe pain disproportionate to the examination (94%) or an abnormal temperature (88%).21,22
They may show the classic findings of hemorrhagic bullae, systemic toxicity, or palpable crepitans. The pain complaints may be mistaken as a “drug-seeking” behavior, which could be deadly. Surgical exploration needs to be done in IDUs with cellulitis and unexplained severe pain.23
Fungal infections, including dermatophytes, are commonly seen in IDUs. Disseminated candidiasis has been reported among IV heroin users who used lemon juice to dissolve the heroin. The lemon juice was contaminated with Candida albicans and the patients developed high fevers, myalgias, and
headaches with negative blood cultures. Painful nodules later developed on the scalp which resolved with alopecia. They also had ocular disease (Candida endophthalmitis), pleuritis, and costochondritis. It has been suggested that physicians should specifically ask IDUs who present with cutaneous, ophthalmologic and osteoarticular disease about a history of using lemon juice. Aspergillosis and zygomycosis also have been reported among IDUs. In addition to SSTIs, IDUs may present with pseudoaneurysms, which may be mistaken for a cutaneous abscess, especially when they present as a nonpulsatile inflammatory mass. These usually manifest as a pulsatile mass located in the area of major arteries. They can develop if an IDU injects accidentally or purposefully into an artery. Gangrene can also develop after intraarterial injection and present as swelling cyanosis, and extreme pain.
CUTANEOUS SIGNS OF ENDOCARDITIS
A link between endocarditis and IDU has long been established. Cutaneous signs include Janeway lesions and Osler nodes. Chapter 155 provides a more detailed discussion of the link between endocarditis and IDU.
SIGNS OF INHALANT ABUSE
SIGNS OF INHALANT ABUSE
Euphoria and delirium can be achieved through the use of inhalants; adolescents are the most common population to abuse them. Inhalants represent a diverse group of readily vaporized chemical compounds with variable properties and have a wide range of potential clinical consequences. Common inhalants of abuse can be subdivided into 3 groups defined as: volatile solvents, fuels, and anesthetics; nitrous oxide; and volatile alkyl nitrites. These compounds can be found in readily available household products such as paint thinner, glues, lighter fluid, spray paint, and nail polish remover.24 Inhaling these products from their original container through the nose (“sniffing”), a soaked rag (“huffing”), or a bag (“bagging”) can lead to myriad clinical presentations resulting from mucous membrane irritation: rhinorrhea, epistaxis, sneezing, coughing, excess salivation, conjunctival injection, dyspnea, and wheezing, as well as dermatitic eruptions in the perioral and/ or perinasal distribution. One specific condition that has been described includes “huffer’s rash,” which is perioral or perinasal dermatitis with pyoderma. Frostbite on the face or oral/nasal cavity can be seen following inhalation of refrigerants or coolants (eg, chlorofluorohydrocarbon propellants in computer duster spray).25 A helpful clinical clue to inhalantinduced hand and/or face dermatitis is the appearance of a yellow crust when it is caused by nitrites.
18
SPECIFIC ILLEGAL DRUGS AND ADDITIVES
SPECIFIC ILLEGAL DRUGS
AND ADDITIVES
COCAINE (ALSO KNOWN AS “COKE,” “C,” “SNOW,” “FLAKE,” OR “BLOW”)
Cocaine is a sympathomimetic that creates feelings of euphoria and causes tachycardia, altered mental status, hypertension, and mydriasis. It is extracted and refined from the Erythroxylum coca plant leaves in the form of a coca paste. The paste is then treated with numerous chemicals to purify it into a water-soluble cocaine hydrochloride powder that is close to 100% pure. By the time the user buys it, the street dealer has generally diluted it with inert or active substances. Cocaine sold on the streets is a fine, bitter, white, crystalline powder that can be injected, inhaled as a powder, or ingested orally, but cannot be smoked. The free base form, also called crack, is processed with ammonia or sodium bicarbonate (baking soda) and water, and then heated to produce a smokable substance. The feelings of euphoria are more intense when inhaled and thus crack is more addictive. Smoking crack stimulates the user in seconds as opposed to snorting cocaine, which takes approximately 15 minutes. There are many cutaneous signs of cocaine abuse, including halitosis, frequent lip smacking, cuts and burns on the lips from broken or chipped crack pipes, madarosis (lateral loss of the eyebrow) from the hot steam rising from the crack pipe,26 palmar and digital hyperkeratosis from holding the hot crack pipe,27 and midline destructive lesions of the nasal septum which result from snorting the cocaine.8 “Snorter’s warts” are nasal verrucae that can develop in cocaine abusers. They are caused by the human papillomavirus transmitted on items such as dollar bills that are used to snort the cocaine. The dollars bills are passed from person to person transmitting the human papillomavirus infection.28
Many types of vasculitis have been described in cocaine abusers, including urticarial vasculitis,29 Churg-Strauss vasculitis,30 necrotizing granulomatous vasculitis,31 palpable purpura, and Buerger disease.32-34 Cocaine-induced midline destructive lesions may cause aggressive nasal deformity that can sometimes be misdiagnosed as Wegener granulomatosis.35 The cause is thought to be vascular ischemia and inflammation. Anti–human neutrophil elastase antibodies are also found in most patients with cocaine-induced midline-destructive lesions.36
Drug eruptions also have been documented, including acute generalized exanthematous pustulosis and Stevens-Johnson syndrome.37,38 Cocaine also has been reported to unmask or cause scleroderma39,40 and has been implicated in the development of Raynaud phenomenon. Cocaine abuse can cause formication, a tactile hallucination of insects crawling underneath the skin, which leads to delusions of parasitosis and/or neurotic excoriations. Cocaine abuse should be suspected
1709
18
in a patient who develops these symptoms, especially if the patient has a vague medical history, labile affect, and delusional behavior.9,41
Levamisole: Levamisole has been discovered as a common adulterant added to cocaine. Unlike other cutting agents, levamisole is added at the onset of manufacturing in the countries of origin and is readily available and inexpensive. Levamisole adds bulk and weight to the cocaine and goes unnoticed by cocaine users because it has a similar appearance, taste, and melting point as pure cocaine. It also has its own stimulant effects and enhances the euphoric effects of cocaine. Levamisole was used in humans as treatment of colon cancer, nephritic syndrome, and rheumatoid arthritis because of its immunomodulating effects, but it was withdrawn from the market in 2000 because of neutropenia, agranulocytosis, and vasculitis. Currently, it can only be used in veterinary medicine as an antihelminthic medication. Side effects of levamisole-adulterated cocaine are widely reported. Most specific is levamisole-induced necrosis syndrome (LINES), which should be considered in patients who present with a distinctive retiform purpura on the ears (Fig. 101-5) with or without lesions elsewhere (particularly on the nose, cheeks, and extremities); the retiform purpura may also present
1710
with hemorrhagic bullae or ulceration. This is usually associated with leukopenia (especially neutropenia) and high titers of perinuclear antineutrophil antibodies and anti-myeloperoxidase antibodies, which are present in more than 70% of cases. Other testing that suggests LINES includes presence of cytoplasmic antineutrophil antibodies and anti–proteinase-3 antibodies, which are present in approximately 50% of cases. Other serologic studies may be positive for antinuclear antibodies, antiphospholipid antibodies, and the lupus anticoagulant. Biopsy specimens show leukocytoclastic vasculitis, thrombotic vasculopathy, vascular occlusion, or a combination of these. Vascular deposits of immunoglobulin M, immunoglobulin A, immunoglobulin G, and complement C3 on immunofluorescence studies point toward a vasculitis caused by levamisole-adulterated cocaine. There also have been reports of pyoderma gangrenosum in patients using levamisole-adulterated cocaine. The lesions are consistent with classic pyoderma gangrenosum, but patients have serologic profiles that are similar to those seen in LINES.42
Unfortunately, levamisole is difficult to detect because of its short half-life (5 to 6 hours) and requires specific testing that is not readily available. Treatment consists of removing levamisole exposure, and mild organ involvement usually is managed with corticosteroids.43
HEROIN (ALSO KNOWN AS “SMACK,” “H”, “SKA”, OR “JUNK”)
Heroin is an opiate that causes euphoria, addiction, respiratory depression, and miosis. It is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. It is typically sold as a white or brownish powder or as a black sticky substance called black tar heroin. Heroin base (common in Europe) can only dissolve in water when mixed with an acid; the most commonly used are citric acid powder and lemon juice. Hydrochloride salt, mainly found in the United States, requires only water to dissolve. Most of the time, heroin is heated, drawn into a syringe or eyedropper through cotton, and then injected. A heroin abuser may inject up to 4 times a day. Because of decreasing prices and the increases in purity, heroin may now be snorted or smoked by inhaling its vapors, either with tobacco in a rolled cigarette or by heating the drug on aluminum foil. There are many cutaneous signs of heroin abuse. Because it is often injected, the signs listed above for IDUs are the most common cutaneous evidence of use. Four percent of addicts develop urticaria, which can last for days. They can develop a “high pruritus,” which is intense itching, especially on their genitals and on their face. “Puffy hand syndrome” (Fig. 101-6) is the condition where edema develops in the dorsal hands but not the fingers. This is mainly caused by lymphatic damage resulting from quinine, which is an adulterant that is added to heroin.12 There have been
a few cases of penile ulcers and necrotizing cellulitis of the scrotum when heroin was injected into the dorsal vein of the penis.44 Pemphigus vegetans,45 fixed drug eruptions, toxic epidermal necrolysis, necrolytic migratory erythema not associated with glucagonoma, and acanthosis nigracans11 have all been described with heroin abuse.8 Sometimes users resort to other drugs when heroin is not available. One of the commonly used alternatives to heroin is tripelennamine with pentazocine (called Ts and blues). Injection causes severe ulceration with hyperkeratosis that follows a linear pattern.
“CLUB DRUGS”
Methylenedioxymethamphetamine (MDMA, Ecstasy): The main active ingredient in the popular club drug ecstasy is 3,4-methylenedioxymethamphetamine (MDMA), which is used for its ability to induce a sense of euphoria and enhance sensory perception via effects on multiple neurochemical pathways.46 MDMA is typically ingested as a tablet. When prepared in its pure powder form it is referred to as “molly” and can be snorted or orally ingested. MDMA is often combined with a wide variety of other drugs, such as amphetamine derivatives, caffeine, and aspirin, when manufactured in tablet form for ingestion. Few cutaneous manifestations following use/abuse have been reported as its deleterious adverse effects on the kidney, liver, and neuropsychiatric systems are more commonly encountered and studied. An acneiform eruption aptly labeled “ecstasy pimples” has been described,47 as has a widespread guttate psoriasiform eruption.
γ-Hydroxybutyrate (also known as “Liquid Ecstasy,” “Liquid X,” or “Fantasy”): γ-Hydroxybutyrate (GHB) is a popular “party drug” based on its euphoric and aphrodisiac properties. It is also used as a “rape drug” in the nightclub scene based on its ability to induce a reversible coma as well as short term memory loss. Specific cutaneous features following its use are not well described. However,
18
GHB use can cause an overdose syndrome in which pale skin is prominent and should prompt immediate medical attention if use is suspected.48
Methamphetmine (also known as “Speed,” “Meth,” “Chalk,” “Ice,” “Crystal,” “Crank,” or “Glass”): Methamphetamine is made by the reduction of ephedrine or pseudoephedrine in “meth labs.” It can be made in a single 2-L bottle using batteries and fertilizer, which makes meth labs more mobile and the drug more accessible. The process of making methamphetamine is very toxic and flammable. It causes euphoria, increased energy, anxiety, aggression, hallucinations, and severe withdrawal. It may be injected, smoked, or snorted.8 Signs of methamphetamine abuse are intense pruritus, body odor, weight loss, premature aging, and hyperhidrosis. “Meth mouth”, which consists of numerous dental caries and enamel erosions starting at the gum line, develops in users.49 It is caused by a combination of xerostomia, bruxism (clenching and grinding of the teeth), and poor dental hygiene. Formication may also develop, especially on the face. Acne excoriee and lichenoid drug eruptions have been reported from methamphetamine use.50
Other Amphetamines and Methylphenidate—Uppers, Speed, Eye Openers, Pick Me Ups: The CNS stimulants amphetamine and methylphenidate are used for narcolepsy to improve alertness and appear to decrease abnormalities in brain structure and function found in attention deficit hyperactivity disorder.51 Formication and obsessive skin-picking, as well as urticaria and acne, have been reported.
Hallucinogens—Lysergic Acid Diethylamide, Mushrooms: Lysergic acid diethylamide (LSD, acid) is found in ergot, a fungus cultivated from rye and other grains, which is often ingested in liquid form for its ability to alter one’s sense of time and sensory perception. Psilocybin and its active metabolite psilocin (4-hydroxy-N,N- dimethyltryptamine) are the psychoactive compounds of various forms of hallucinogenic mushrooms ingested for their mind altering properties.52 Dry mouth appears to be the main cutaneous effect.
Sedatives: Cutaneous reactions to sedatives are rare. The sedative class of drugs includes cannabis, benzodiazepines, and hydroxybutyrate. Drug reactions are rarely associated with benzodiazepines, including morbilliform hypersensitivity eruptions, erythema multiforme to clonazepam, and acute generalized exanthematous pustulosis.
CANNABIS (ALSO KNOWN AS “MARIJUANA,” “POT,” “WEED,” OR “MARY JANE”)
Cannabis is a mixture of dried shredded leaves and flowers of the Cannabis sativa plant. The psychoactive
1711
18
chemical compound is ∆9-tetrahydrocannabinol (THC). The potency of marijuana has increased over the years and is now 5 times stronger than the marijuana used in the 1970s. Since its legalization in some states of the United States, marijuana use has increased in those states by approximately 20% according to early data. Although recreational use tends to be for its ability to produce euphoria, medicinal use is gaining acceptance. Treatment of pain, glaucoma, muscle spasm, nausea, seizures, poor appetite, and inflammation are only a few of the disorders for which cannabinoids are being used and investigated. There are topical formulations that profess to improve the appearance of aging skin. There are 4 ways to consume marijuana: inhalation, oral, sublingual or topical application. Inhalation causes an effect within minutes, peaks at approximately 1 hour, and wanes in approximately 2 hours. Inhalation occurs via smoking or vaporization (vaping). Marijuana can be smoked in joints (hand-rolled cigarettes), bongs (pipes), or blunts (marijuana cigars). Other drugs, such as cocaine, may be mixed with it. Vaping (see below) is also gaining popularity. Oral ingestion is becoming more common as cannabis is used for medical purposes and is legal in several states. Onset of action for oral consumption is slower than for inhalation, with initial effects taking 30 minutes or longer and peaking at approximately 2 hours; total duration of effects can be as long as 6 hours. The effects from oral consumption have been described as more “intense” than those from inhalation. Dosage of marijuana taken orally can be difficult to titrate; irregular effects and overdose are more common with this form. Cannabis edibles include the classic brownies and cookies, as well as other formulations, including lollipops, fudge, “cannabutter,” oils and tinctures, and baked in breads and pizza. Sublingual use includes product in dissolvable strips, lozenges, and sublingual sprays. Onset of action may be earlier than in oral consumption. Finally, cannabis can be delivered topically via transdermal patches, oils, salves, lotions, and bath salts. Transdermal patches may deliver enough active ingredient to cause a “high” but usually only produce local effects. There are few cutaneous signs of cannabis use. Acne, ranging from mild to severe, has been described. Allergic reactions, including contact dermatitis, also have been reported. Cannabis arteritis is a serious vascular complication that can occur with chronic use. Cannabis arteritis is rare, with approximately 50 cases reported in the literature despite more than 5 million daily users worldwide. It presents as peripheral ischemia and necrosis, most often of the lower limbs. Cannabis arteritis is one of the most frequent causes of peripheral arterial disease in adults younger than age 50 years and is a subtype of thromboangiitis obliterans.53 It may present with Raynaud phenomenon and digital necrosis. Cannabis arteritis is thought to be caused by the combined vasoconstrictive effects of THC and arsenic, arsenic being a common contaminant in marijuana.54
1712
Claudication may present before the development of
ulcers or gangrene.55 Duplex ultrasound can be used to differentiate between cannabis arteritis and atherosclerosis. Cannabis arteritis shows occlusion of peripheral arteries below the knee, whereas atherosclerosis has calcified plaques in the iliofemoral arteries. Treatment is for the patient to stop cannabis use and to take lowdose (81 mg) aspirin. For severe cases, iloprost (0.5 to 2 ng/kg/min), which is a prostaglandin analog, can be given.56
CUTTING AGENTS
Drugs of abuse often contain additional ingredients besides the active compound the user desires to consume. These ingredients can be added intentionally to increase the volume of the product for additional profit, or, it may be unintentionally included in the final product as a result of the chemical manufacturing process. So-called cutting agents can be divided into diluents and adulterants. Diluents, such as dirt, baking soda, talc, and mannitol, are added to expand the volume of the drug for increased distribution.57
Adulterants, such as caffeine, hydroxyzine, diltiazem, levamisole, and phenacetin, are added to enhance the effect of the main active ingredient or facilitate administration of the drug. Several cutting agents deserve special mention because of their potential to induce cutaneous manifestations following exposure. Most notable among these is levamisole in cocaine and arsenic in cannabis. Diluents such as talc and starch are reported to cause foreign-body granulomas after parenteral use with various drugs (Fig. 101-7).58
Another example of an emerging adulterant leading to adverse outcomes with heroin use is clenbuterol. Although unremarkable for its skin manifestations, several case series have described dangerous cardiac events.59
BETEL
Betel is a common drug of abuse in the Asian and Southeast Asian cultures. Betel quid is a combination of areca nut, betel leaf, slaked lime, and other ingredients. Psychoactive alkaloids appear to be the main stimulant. It is usually ingested by mucosal absorption similar to chewing tobacco. Chewing of the betel mixture causes maceration, erosions, and fissures of the oral commissures, which can be mistaken for other disorders such as angular cheilitis, candidiasis, or vitamin deficiencies. Chewer’s mucosa is a brownish-red discoloration of the buccal mucosa associated with irregular desquamation. Lichenoid lesions may also appear. Oral submucous fibrosis is characterized by a prodrome of oral dysesthesia followed by palpable vertical fibrous bands that may require surgical interventions for opening of the mouth. Oral carcinoma can occur, usually on the buccal areas of the tongue and labial mucosa.60
KROKODIL
Desomorphine, a synthetic opioid derivative, manufactured using chemically altered codeine with several household ingredients, goes by the street name “Krokodil” and is reportedly ten times more potent than heroin. The drug acquired its name from the thick, scaly, green-black skin changes seen in its users.61
The injectable drug is highly addictive and known for inducing widespread necrotizing skin lesions. It gained its popularity as a drug of abuse in Russia and cases of its adverse effects have been documented recently throughout Europe and only rarely in the United States. Besides skin color and texture change, cutaneous manifestations include swelling and pain at sites where the drug is subcutaneously injected followed by extremely aggressive necrotic ulcerations, which commonly involve muscle and cartilaginous tissue. Destructive infections often ensue and lead to extremely morbid sequelae. Alarmingly, these reactions are typically reported after short periods of use and the analgesic effects of the medicine can cause delay in the user seeking medical attention.
LEGAL DRUGS OF ABUSE
LEGAL DRUGS OF ABUSE
ALCOHOL
Cutaneous manifestations of alcohol consumption comprise a wide spectrum of clinical presentations. Vascular lesions are some of the most easily recognizable skin findings seen in patients who abuse alcohol; they occur secondary to alcohol’s effects on the vasodilatory properties of blood vessels as well as hormonal changes induced by alterations in liver metabolism.62
Spider angiomata, palmar erythema, and telangiectasia are examples of common cutaneous signs in alcohol abuse. More subtle findings include corkscrew scleral
18
vessels. Other signs of liver insufficiency include dilated periumbilical veins on the abdominal wall (caput medusae) and unilateral nevoid telangiectasia, a vascular proliferative syndrome. Nevoid telangiectasias have been proposed as latent congenital nevi that present in the setting of alcohol-induced hyperestrogenism. They appear on the upper body in the C3–C4 dermatomal distribution as thread-like collections of fine telangiectasias. Systemic jaundice is typically seen after serum bilirubin levels reach greater than 2.5 mg/dL.63 Generalized pruritus is another end-stage sequelae of liver dysfunction and may present clinically as nonspecific excoriations or as prurigo nodules if areas are chronically scratched. Several nail abnormalities to both the nail plate and nail bed have been described in the setting of alcohol abuse and concomitant liver dysfunction. The classic nail change seen in these patients are “Terry’s nails” in which the proximal nail is nontranslucent white while the distal nail remains pink. One study reported that 80% of patients with cirrhosis will manifest this finding. Furthermore, nail findings previously described in the literature include transverse white bands and red lunulae in the setting of cirrhosis with congestive heart failure. There are many chronic skin conditions that can be induced or exacerbated by alcohol abuse. One hallmark cutaneous condition associated with alcohol abuse is porphyria cutanea tarda, which is discussed in Chap. 125. Other notable alcohol-associated conditions include Dupuytren contracture, as well as Madelung disease, psoriasis, rosacea, nummular eczema, and seborrheic dermatitis, although the exact connection with these conditions is unclear.
TOBACCO (CIGARETTES, CHEWING TOBACCO, ORAL TOBACCO, SPIT OR SPITTING TOBACCO, DIP, CHEW, SNUFF, OR SNOOZE)
Tobacco is made from the leaves of plants of the genus Nicotiana. Tobacco is usually smoked, but can be chewed (ie, absorbed via the oral mucosa when placed between the buccal and gingival mucosa) or sniffed. “Vaping” is a relatively new phenomenon where the tobacco is inhaled through a vaporizer that infuses water into the smoke. Nicotine in tobacco in particular is known to be addictive because of its mood-boosting effects; it is also known to suppress appetite. There are many signs and symptoms of tobacco use. Yellow-brown staining of the teeth, fingers and fingernails from nicotine is clearly visible in many smokers. One of the most-well-established effects of tobacco smoking on the skin is premature aging. Although this association has been appreciated for decades, studies in the late 20th century confirmed the link between wrinkles on tobacco and further identified that the association is proportional to the tobacco load of the patient.64 Some of the mechanisms by which this occurs have been described. One such mechanism is the increase in elastic fiber content of the reticular
1713
18
dermis along with upregulation of enzymes crucial to skin remodeling and repair essentially creating the effect of solar elastosis. Tobacco’s effects on fibroblasts and the microvasculature impair wound healing. There are more than 7000 chemicals found in cigarette smoke, more than 70 of which are known to be carcinogenic.65 Although many studies have sought to identify a potential relationship between tobacco use and skin cancers, they have failed to identify a definitive causal relationship. One study did show an increased prevalence of keratoacanthomas in smokers compared to nonsmokers. Tobacco use also has been linked to hand dermatitis.66
Use of tobacco incites or worsens chronic skin conditions, including psoriasis (particularly the palmoplantar pustular variant), hidradenitis suppurativa, and subacute and chronic cutaneous lupus erythematosus. Smoking tobacco impairs the efficacy of antimalarial therapy in patients with lupus, making treatment of these patients more difficult.67 Also, smokers should not use beta-carotene supplements because of the higher risk of lung cancer. Chemical effects include peripheral vasoconstriction, platelet aggregation, and decrease in prostacyclin formation, which increase the risk of cardiovascular disease. Thromboangiitis obliterans (Buerger disease) is an inflammatory arteritis of the medium and small vessels of the upper and lower extremities. It typically presents with pain and necrosis of the digits in young male tobacco smokers. Carbon monoxide also increases risk of cardiovascular problems, as well as peripheral ischemia, in end organs such as the skin and digits.68
Both cigarette smoking and chewing are associated with several conditions of the oral mucosa. This includes leukokeratosis nicotinica palati (nicotine stomatitis, smoker’s palate) which is characterized by uniform keratosis of the hard palate with multiple umbilicated erythematous papules that are the inflamed orifices of minor salivary glands. Leukokeratosis nicotinica glossae is a homogeneous white plaque that affects the anterior two-thirds of the dorsal tongue. Oral verrucous carcinoma, oral warty dyskeratoma, and oral melanosis (brown-black pigmentation of the oral mucosa) are also associated with tobacco use.69
PRESCRIPTION OPIATES
Hydrocodone, oxycodone, morphine, and codeine are legally prescribed analgesics that can produce euphoria. CNS depression is the most common side effect. Because they are taken orally, these medications do not produce the signs listed above for heroin. Urticaria and pruritus are the most common cutaneous effects.
ANABOLIC STEROIDS
Anabolic steroids are synthetic hormones similar to testosterone. They can be ingested or injected and have many legal indications. Illicit use is usually
1714
to build muscle and augment athletic performance. Cutaneous side effects are common and should be suspected in any patient who presents with acne vulgaris, hair growth on the body and loss on the scalp, and striae. Increased body hair, increased oil in the skin and hair, and premature androgenetic alopecia are also common.70 Steroid acne is most commonly distributed on the face, chest, back, and shoulders. Women may demonstrate androgen-mediated effects, including androgenetic alopecia, deepening of the voice, clitoral enlargement, and menstrual irregularity. Men may experience gynecomastia, testicular atrophy, and infertility. Teenage use can induce precocious puberty and growth stunting. Side effects may not reverse upon discontinuation of the drug.71
Striae may develop from muscle hypertrophy. Acne fulminans, psoriasis, familial angiolipomas and exacerbation of coproporphyria also have been reported. Systemic side effects also may be present, including hepatic enzyme elevations, jaundice, hypertension, and lipid abnormalities.
NONCUTANEOUS ISSUES
Noncutaneous complications and sequelae of drug use are extensive. In particular, bloodborne or sexually transmitted diseases, such as HIV and hepatitides B and C virus, are well-established comorbidities of IV drug use. There is data to suggest that illicit drug use is associated with premature mortality in young adults both from trauma and suicide.72
MANAGEMENT
The key to managing drug use, abuse and addiction is as early intervention as possible. The dermatologist may be able to help with recognition of the problem. Relatively recently, drug addiction has been recognized as a multifactorial disease and therapies ranging from medications, psychiatric treatment, and alternative treatments, including acupuncture and meditation, are being implemented.

Figure 101-1 Track marks. Examples of track marks from intravenous drug use on the upper extremity.

Figure 101-2 Hyperpigmentation. Intravenous drug use– induced hyperpigmentation on the dorsal forearm and hand.

Figure 101-3 Infection. Sequelae following soft-tissue infection as a result of intravenous drug abuse.

Figure 101-4 Necrotizing fasciitis. Photographic depiction of necrotizing fasciitis following intravenous drug use.
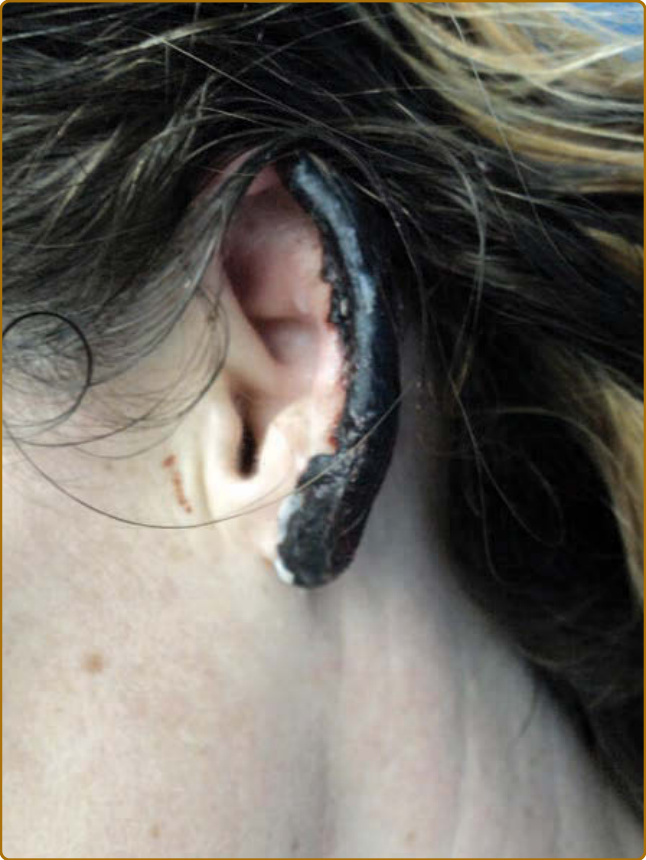
Figure 101-5 Levamisole. Characteristic purpuric eruption on the ear following levamisole toxicity. (Reproduced with permission from Hennings C, Miller J. Illicit drugs: what dermatologists need to know. J Am Acad Dermatol. 2013;69:135-142.)

Figure 101-6 Puffy hand syndrome. Example of dorsal hand edema following intravenous drug use.

Figure 101-7 Talc granulomas. Multiple granulomas on the bilateral legs from intravenous use of drugs containing talc as a cutting agent.
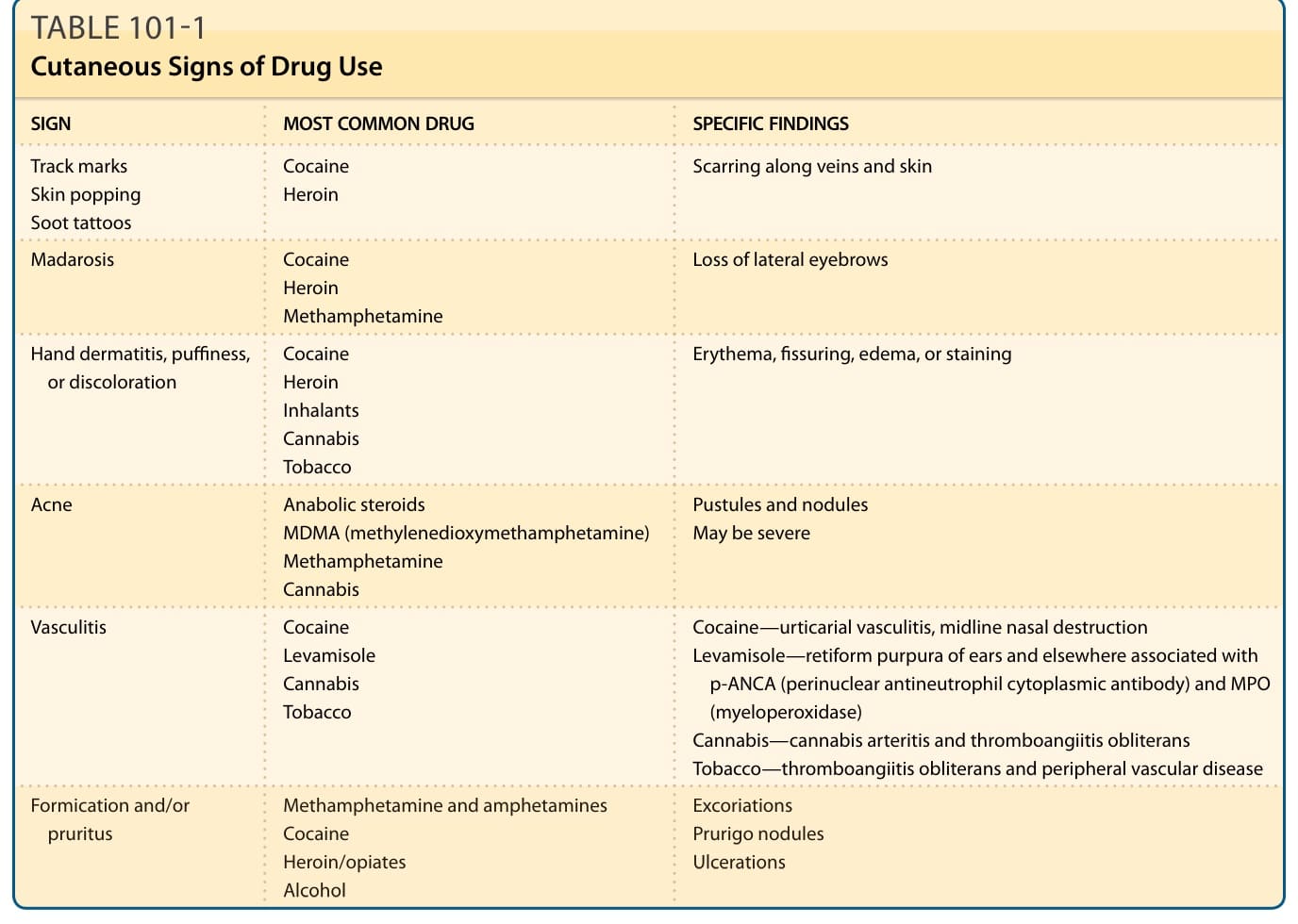
TABLE 101-1 Cutaneous Signs of Drug Use