Noninvasive Body Contouring
3
31
AT-A-GLANCE
■ Noninvasive body contouring includes skin tightening, fat reduction, and cellulite treatment.
■ Noninvasive body-contouring treatments are associated with minimal intraoperative risk, postoperative discomfort, and recovery time, but overall effectiveness may be less than for more invasive procedures.
■ Improvement in body contouring may be maximized when noninvasive modalities are repeated or used in combination.
BACKGROUND
WHAT IS NONINVASIVE BODY CONTOURING?
WHAT IS NONINVASIVE
BODY CONTOURING?
In dermatology, body contouring is defined in contradistinction to more superficial skin remodeling. Change in the fine skin texture is thus not considered amenable to treatment by body-contouring methods. On the other hand, body contouring can correct change in skin elevation, shape, and drape associated with full-thickness dermal aging or injury, as well as such change secondary to alteration in the morphology or size of the subcutaneous layer. Whether a method of body contouring is classified as noninvasive or invasive is predicated on the degree of manual or device-based macroscopic injury to the skin that use of this method entails. This can be a subtle determination. Noninvasive body contouring may be defined by exclusion as typically not requiring scalpel incision or excision, manual dissection of the skin tissue planes, or insertion of devices (eg, suction cannulas, drains, sutures) that are of sufficient size and bore to elicit scarring upon healing. In general, noninvasive procedures are associated with less postoperative discomfort and briefer recovery, requiring minimal time away from work and social activities.
MAJOR TYPES OF NONINVASIVE BODY CONTOURING
MAJOR TYPES OF
NONINVASIVE BODY
CONTOURING
Noninvasive body contouring is a rapidly evolving field. As such, the nosology of clinical conditions requiring body contouring remains fluid and subject
to change. Currently, the 3 widely recognized therapeutic subtypes of noninvasive body contouring are skin tightening, fat reduction, and cellulite treatment. As is obvious, these treatments are designed to address excess or sagging skin (skin tightening), pockets of unwanted fat (fat reduction), and dimpling of the thighs and buttocks (cellulite treatment). There may be overlap. That is, noninvasive body-contouring modalities used to target a particular condition may favorably impact other skin contour problems at the same anatomic site, albeit to a lesser extent.
PHYSICIAN AND PATIENT PREFERENCE FOR NONINVASIVE BODY CONTOURING
PHYSICIAN AND PATIENT
PREFERENCE FOR
NONINVASIVE BODY
CONTOURING
Physicians and patients both have reasons for preferring noninvasive body contouring to invasive contouring procedures. Patients may perceive noninvasive interventions as less “frightening,” or safer, and also less drastic or vain than surgery. Those who wish to avoid even the smallest visible scars, or to minimize postoperative downtime, also may be attracted to noninvasive options. From a physician’s standpoint, noninvasive body contouring offers the promise of fewer complications to manage. It is also less time intensive from a provider standpoint, as in some cases much of the work is accomplished by devices that are positioned or injected over the treatment area rather than by direct physician manipulation. Finally, more patients are good candidates for noninvasive body-contouring approaches, which are routinely used to correct minor conditions for which an invasive procedure may be excessive or not indicated.
TYPES OF BODY CONTOURING
SKIN TIGHTENING1-14
SKIN TIGHTENING
1-14
INDICATIONS AND PATIENT SELECTION
Noninvasive skin tightening is most appropriate for patients with mild to moderate skin laxity without severe sagging. In patients with Fitzpatrick skin types I to III, this usually correlates to ages in the
31
25 to 55 years range. Focal facial anatomic areas that are responsive to noninvasive tightening include the forehead and brows, the midface, and the neck and jowls. Off the head and neck, skin can be tightened on the upper arms, décolletage area, abdomen, knees, and other areas. Patients appropriate for this procedure expect the possibility of modest improvement, but clearly understand that complete resolution, a socalled home-run, is unlikely except in selected cases of mild skin laxity. Some types of cosmetic complaints will not resolve with skin tightening. Crepe-like skin with fine superficial textural change will generally not respond. Pigmentary abnormalities must be addressed by vascular or pigment devices, not skin-tightening devices. Extremely saggy skin, with underlying loss of substructure and fat-pad integrity, will not return to its youthful contour after noninvasive tightening. Patients with severe photodamage or severe sagging who would like the gold standard treatment are typically dissuaded from receiving skin tightening. For such concerns, nonablative or ablative resurfacing procedures with or without excisional lifting approaches, such as rhytidectomy, brow lift, or blepharoplasty, may be more successful.
TYPES OF DEVICES AND TECHNOLOGIES
Several distinct technologies have been adapted for skin tightening. These include light-based devices, notably infrared lasers and light sources. Additionally, radiofrequency devices, including monopolar and bipolar devices, as well as more exotic configurations, are in widespread use. Recently, there has been a proliferation of insertional needle and injectable radiofrequency skin tightening devices that skirt the boundary between noninvasive and minimally invasive. Highfrequency ultrasound is also commonly used for skin tightening. Devices that have other primary indications, but secondarily induce skin tightening, include ablative resurfacing devices, particularly carbon dioxide laser, as well as insertional infrared laser-tipped devices used in laser lipolysis.
MODES OF ACTION
Fully noninvasive skin tightening spares the epidermis and superficial dermis, and directs energy into the deep dermis and subcutis. This energy, which can be infrared light, radiofrequency, or ultrasound, heats the skin. Precisely directed heat injury results in numerous small volumetric zones of thermal necrosis. The immediate mechanisms of shrinkage include collagen contraction resulting from collagen denaturation, and shrinkage of the fibrous septae of the fat lobules, which compresses the subcutis (Fig. 211-1). It has been suggested that heat-induced shrinkage may also effect superficial muscular aponeurotic system shrinkage, in a manner akin to surgical plication in a facelift, but this is highly speculative and unproven. Longer-term, over
3858
a period of 30 to 90 days, neocollagenesis may result in additional skin tightening. Based on experience with the index device for noninvasive skin tightening, a monopolar radiofrequency1,2,9-12 device introduced in 2002, several treatment paradigms have been adopted across devices. First, to avoid the risk of skin burns or localized fat atrophy manifesting as configurated skin depressions, several to many lower-energy passes rather than 1 to 2 high-energy passes are typically performed. Second, to maximize effectiveness, zones of thermal necrosis are placed close together, very densely. As many focal necrosis zones as feasible are created in each plane of the dermis, with 2 to 3 such planes not being uncommon. The objective is to maximize the cumulative volumetric injury because this is believed to coincide with the degree of tissue tightening. Of course, some skin must be spared between zones of thermal injury so as to allow prompt, reliable, and scarless wound healing. Ultrasound3,4,6,14 is useful for skin tightening because it is a form of energy that can be configured to penetrate arbitrarily deeply into the skin without causing injury to overlying structures. As such, ultrasound for skin tightening can be readily configured to create zones of thermal necrosis at several different levels in the dermis (Fig. 211-2). Insertional radiofrequency needles5 penetrate into the skin, with an array of fine microneedles delivering heat to an adjustable depth of less than 1 mm to several millimeters. In this manner, insertional hot needles can achieve many of the same benefits of microfocused ultrasound. Insulated needles may be used to propagate heat just from the needle tips; noninsulated needles leak heat along their whole length, thus potentially causing more tightening at the cost of more of a visible epidermal and superficial dermal injury. Carbon dioxide (10,600 nm) laser7,13 ablates the epidermis and partial thickness dermis. Immediate tissue tightening is seen as a result of collagen denaturation. Laser lipolysis operates under the skin surface, as a fine laser fiber encased in a protective metal sleeve is introduced via a skin puncture into the subcutis. The hot laser tip, traditionally an Nd:YAG (neodymium:yttrium aluminum garnet) laser, protrudes from the sheath and is moved back and forth under the dermis to induce heat-related contraction. A handheld temperature gun can be held over the skin by an assistant to ensure that the peak temperature adjacent to the laser tip does not exceed the 40°C to 42°C (100°F to 107.6°F) at which full-thickness injury or burn can occur. In this manner, laser lipolysis can augment liposuction, which reduces fat but does not tighten skin. Similar radiofrequency wands can be used for skin tightening at multiple sites on the body.
AVOIDING AND MANAGING COMPLICATIONS
Noninvasive skin tightening is generally very safe, with anticipated mild sequelae. Expected posttreatment tissue effects are erythema and edema, lasting
3
31
Immediate collagen denaturation and contraction
A
Thermally mediated shrinkage of the fibrous septae of the subcutaneous fat
B
from several hours to 1 to 2 days. Intraoperative discomfort can be managed with topical anesthesia or, in some cases, with oral benzodiazepines and analgesics. Because treatment paradigms have moved away from very-high-energy passes, burns and fat atrophy have become rare. Repeated treatment of the same size can very rarely result in heat stacking culminating in white, wheal-like skin plaques, which resolve with time and topical steroids. Scars and pigmentary change are exceedingly rare.
Radiofrequency needling may result in punctate marks on the skin, which resolve over 1 to 2 days. Pinpoint bleeding may also occur with some devices. Rare indented scarring has been reported. Carbon dioxide laser is routinely associated with more protracted downtime: 1 week for fractional resurfacing and 2 to 3 weeks for traditional full-face resurfacing. Persistent erythema, edema, crust, and serous drainage is common, particularly after full-face resurfacing. Overtreatment and heat stacking with
3859
31
Facial surface depicting 3D zones of thermal necrosis
A
Dermal cross-section depicting 3D zones of thermal necrosis
3 mm 1 mm
B
4.5 mm
1.5 mm
carbon dioxide laser can result in significant adverse events, notably hypopigmentation that does not resolve and scarring. Laser lipolysis is usually uncomplicated, requiring only healing of the entry sites, which may also have been used for liposuction. Burns, including those associated with full-thickness tears in the skin, can occur if the laser tip is held subdermally at one anatomic location for too long. Overtreatment can also result in seromas, which must be drained promptly. Radiofrequency wands comparable in effect to lipolysis lasers have been optimized for skin tightening, with built-in temperature monitoring that can help prevent burns.
3860
ADAPTING TREATMENTS FOR ANATOMIC AREAS, SKIN TYPES, AND DEGREE OF RESPONSE15
A certain minimum density of zones of thermal necrosis is required to elicit the best result. As such, patients with larger faces or bodies may require more total treatment spots or lines. Pain response is subjective and also varies across individuals. Even though noninvasive skin-tightening procedures are always performed with the patient awake, some patients may require anxiolytics or analgesics. There is a very low treatment-associated risk of pigmentary abnormality in
patients with darker-pigmented skin; consequently, treatment regimens are not usually adjusted for skin type. Greater care is taken when treating off the head and neck. On truncal and extremity sites, posttreatment healing is slower, and handpieces are adapted to be larger and to deliver energy deeper, as the dermis is thicker. Depending on treatment response, repeat treatments may be indicated. If a patient is among the minority who experience no or very minimal response, additional treatments may be deferred as they may be similarly futile. Should the patient be willing to try again and incur further costs, then despite the heightened risk of failure, it is reasonable to proceed. More commonly, an observable benefit is obtained after the first treatment. In this case, a patient may receive additional treatments to improve upon this outcome. The average number of treatments per course varies by device and technology, from as few as 1 or 2, to as many as 4 to 6 or more. In some cases, it may be prudent to wait for 2 or 3 months before retreating to allow new collagen to form, as these newly laid-down fibers may be relatively more amenable to subsequent energy-mediated contraction. Carbon dioxide laser, laser lipolysis, and radiofrequency wand tightening are often single procedures, as their longer-associated postoperative downtime is counterbalanced by greater effectiveness. Carbon
A
3
31
dioxide procedures, and to a lesser extent insertional radiofrequency needles, should be used with some caution in patients with darker-pigmented skin so as to minimize the risk of hyperpigmentation. Indeed, the risk of such pigmentation in darker skin types is almost 100% with carbon dioxide laser. Laser lipolysis and subdermal radiofrequency wand tightening are less concerning in darker skin types because they deliver energy under the skin and do not directly injure the epidermis and papillary dermis.
EXPECTED OUTCOMES
After treatment of the forehead and upper face, 1 to 2 mm of brow elevation is commonly seen at 60 to 90 days (Fig. 211-3). Treatments on the lower face may result in modestly more defined jawline or neck contour with slightly reduced skin excess. Midface treatments may result in more subtle skin tightening. Off the face, outcomes are even more variable. Successful skin tightening on the abdomen, upper and lower knees, décolletage area, and upper arms has been reported. Treatment parameters are modified for these indications. The degree of tightening or wrinkle reduction is generally modest. Patients with significant skin excess may be better served by a surgical tightening or skin-reduction
B
3861
31
procedure, or by a minimally-invasive form of skin tightening like carbon dioxide laser, laser lipolysis, or subdermal wand radiofrequency. Alternatively, such patients should be prepared to undergo numerically more treatments of energy-based noninvasive skin tightening for an incrementally greater degree of improvement.
NONINVASIVE AND MINIMALLY INVASIVE FAT REDUCTION16-31
NONINVASIVE AND
MINIMALLY INVASIVE FAT
REDUCTION
16-31
INDICATIONS AND PATIENT SELECTION
Noninvasive fat reduction is most appropriate for treatment of small pockets of excess fat resistant to diet and exercise. Treatments with energy-based modalities may result in permanent reduction of such pockets. Early data with cryolipolysis showed that socalled love handles, or protrusions of abdominal fat on either side of the flanks, were particularly responsive to treatment (Fig. 211-4). More recent experience has confirmed that even large subcutaneous collections of abdominal and truncal fat will remit with noninvasive fat reduction, although many serial treatments may be needed.
Noninvasive fat reduction does not reduce excess skin, and may worsen the appearance of skin folds if a substantial quantity of fat is removed because normal skin elasticity is insufficient to retract the skin adequately. For example, after fat-reduction treatment, patients seeking correction of sagging upper arms may observe even more hanging skin. When faced with the risk of exacerbating excess skin, physicians consulting with patients requesting fat reduction should explain the risks. Ideally, susceptible patients should be prepared to undergo, if necessary, a subsequent skinreduction procedure, such as an elliptical excision to resect upper arm skin. Thermal fat-reduction methods may be slightly more effective in shrinking skin, but the aforementioned constraints still apply. Fat-reduction treatments do not smooth the appearance of cellulite. Cellulite, or dimpling of the thighs and buttocks, is discussed further in the next section.
TYPES OF DEVICES AND TECHNOLOGIES
Fat reduction can be accomplished with physical modalities, including radiofrequency energy, therapeutic ultrasound, and cryolipolysis. In the United States, cryolipolysis was the first widely used noninvasive treatment for fat, and is the most used and best described approach for this indication. Minimally-invasive approaches include injection
3862
chemical adipocytolysis and laser lipolysis. Tumescent liposuction, which accesses fat through tiny apertures that reepithelialize without sutures into barely visible punctate scars also may be considered a form of minimally-invasive fat reduction, but it is incorrectly often considered more invasive than it is. Liposuction is discussed in depth elsewhere in this text.
MODES OF ACTION
The different technologies for noninvasive and minimally-invasive fat reduction span a range of modes of action. As a group, the energy-based modalities16-21
are more similar than different. Radiofrequency and ultrasound energy targeting fat are configured to direct energy deeper and more diffusely than necessary for tightening skin. Ultrasound fat reduction devices can be further subdivided into thermal and mechanical types. Thermal ultrasound heats adipocytes, as does radiofrequency used for fat destruction, and mechanical ultrasound breaks fat cells apart by propagating an acoustic shock wave. Cryolipolysis22-25 is predicated on the mechanism of popsicle panniculitis (Fig. 211-5). Fat is destroyed by freezing while the overlying dermis and epidermis are spared (Fig. 211-6B). Chemical adipocytolysis26-29 employs deoxycholate, a detergent, to emulsify fat cells. It is currently only U.S. Food and Drug Administration (FDA) approved for submental fat reduction (Fig. 211-6A). Laser lipolysis,30,31 discussed in depth in the previous section on skin tightening, can also melt fat by direct heat injury. In all cases of noninvasive and minimally invasive fat reduction, fat cells are lysed, with the constituent fatty acids then resorbed into the systemic circulation. For modalities that have proceeded through the FDA premarket approval process, the FDA has requested data regarding blood lipid levels following treatments. Such analyses have shown the absence of a cotemporaneous sharp elevation in lipid levels. This may be attributable to the small quantity of fat cells lysed per treatment, the high intrinsic biologic clearance capacity for fatty acids, or the slow rate at which the products of adipocytolysis are mobilized over many hours to days.
AVOIDING AND MANAGING COMPLICATIONS
Like nonsurgical skin tightening, noninvasive and minimally-invasive fat reduction are safe procedures. Intraoperative tenderness can be managed with oral anxiolytics and analgesics. Tenderness requiring medication is less common with cryolipolysis, as the associated cold sensation inherent to the procedure results in intraoperative pain relief after a few minutes. With heat and shockwave–based modalities, treatment over bony prominences, surgical scars, or hernias is avoided to prevent injury to these structures. After each treatment of cryolipolysis, local paresthesia and numbness are expected to persist for several
3
31
weeks before gradually resolving completely. There are extremely rare reports of cryolipolysis actually stimulating fat growth, which then can be corrected by liposuction; these episodes are idiosyncratic and cannot be planned for, predicted, or actively circumvented. Fat-reduction treatments can result in asymmetry. Similarly, they can result in too much fat being removed, which can lead to a skeletonized, unattractive appearance. The risk of both these outcomes is minimized by carefully mapping the distribution of pretreatment fat. Pinching the fat to be treated can provide the operator with information regarding the quantity and relative distribution of fat. Treatment intensity, duration, and frequency can then be adjusted to meet specific patient needs, and to correct preexisting asymmetries. It is preferred that patients be at or above their normal weight before a fat reduction treatment regimen. If they diet to a level below their baseline weight prior to treatment, they will likely eventually regain weight after treatment. This new gain may manifest in unexpected areas, as treated pockets of fat will be depleted of adipocytes and less able to accommodate future weight gain. Chemical injection adipocytolysis routinely results in extreme posttreatment edema. Patients receiving such treatment to the submental area may have a “bull frog”–like double-chin and underneck swelling for several days. This can be tender and warm. Injections are best avoided over the course of the marginal mandibular nerve. In a small proportion of cases, chemical injection adipocytolysis results in temporary marginal mandibular nerve dysfunction and palsy, but this resolves completely over several weeks. Laser lipolysis can result in burns and seromas. These are discussed further in the section on skin tightening.
ADAPTING TREATMENTS FOR ANATOMIC AREAS AND SKIN TYPES
Noninvasive and minimally invasive fat reduction modalities can be safely and effectively applied at a wide range of anatomic sites. Common treatment areas include the neck and submental area, upper arms, upper and lower abdomen, flanks and love handles, thighs, and knees. The feasibility of treatments at a particular site can be limited by the size and shape of available handpieces. For instance, in recent years, specialized cryolipolysis handpieces have been developed to conform to the submental area, thighs, and other areas. One to several noninvasive or minimally-invasive fat reduction treatments may be needed to reach the desired outcome. Multiple treatments are the norm. Fat reduction without surgery is appropriate for patients of all Fitzpatrick skin types. Pigmentary abnormality typically does not occur at a higher rate in darker-skinned patients.
EXPECTED OUTCOMES
Fat-reduction treatments can result in partial or complete permanent resolution of small pockets of excess
3863
31
A
a b
c d
e f
C
B
3864
Nonsurgical treatment by injection application in grid-like pattern
A
3
31
Nonsurgical treatment by injection in overlapping applications of a cryolipolysis device
B
subcutaneous fat that is diet and exercise resistant. Visceral fat, which can be associated with health risks, is not reduced. Patients should be aware that fatreduction treatments will not tighten skin or erase cellulite, and may even worsen loose skin in older patients. Repeated treatments with noninvasive modalities can eliminate larger reservoirs of fat for patients willing to tolerate many consecutive treatments as well as the attendant financial cost. Given the intervals between treatments, treatments of large accumulations of fat may require many months or even years to complete. A more efficient one-time procedure like liposuction may be a reasonable alternative. Needless to say, and as discussed before, regardless of the modality used, successful fat removal does not preclude future weight gain, including fat accumulation at untreated anatomic sites.
CELLULITE REMOVAL32-40
CELLULITE REMOVAL
32-40
INDICATIONS AND PATIENT SELECTION
Cellulite was historically a popular rather than a technical term, but is now also in common usage in clinical
and research medicine, and serves both functions. Simply, cellulite is skin dimpling of the buttocks and upper thighs (Fig. 211-7). It is more common in women, and may worsen with aging. There is no strong association between overall body weight and cellulite, which is seen frequently in non-overweight individuals. Cellulite removal technologies are best suited for patients with localized dimpling of the affected areas. Widespread skin rippling, deep creases, and severe excess fat of the upper thighs and buttocks are not corrected with current therapies for cellulite. Younger people tend to respond better, as they often do not suffer from the concurrent issues of skin excess and skin sagging. It is unclear why cellulite is more common in women than in men (Fig. 211-8). One hypothesis, borne of anatomic studies, is that men have fascial bands in the affected area comprised of crisscrossed rather than parallel fibers. Presumably, these bands are more impermeable to fat herniation, and hence dimpling, than the parallel bands in most women. Whatever the cause, cellulite is markedly more common in women, who also tend to be more bothered by it, and more likely to seek treatment. Patients seeking cellulite treatment should understand that this will not prevent the formation of new
3865
31
Cellulite elicited by manual compression or full-blown, occurring even at rest
A B
cellulite dimples in the future. Some dimples may not respond at all, and cellulite treatment will not result in fat reduction or a buttock or thigh lift. Multiple treatments may be necessary. A physical exercise regimen also may be recommended as adjunctive therapy. The ideal patient is a 20- to 50-year-old woman of normal weight with a few localized areas of cellulite, mostly on the buttock.
Anatomic variation of cellulite in females
A
TYPES OF DEVICES AND TECHNOLOGIES
There are several specific therapies for cellulite. Many of these are predicated on the concept of subcision, pioneered for treatment of acne scars by the late Norman Orentreich, a pioneering New York dermatologist who also discovered the scientific basis for
Anatomic variation of cellulite in males
B
3866
hair transplantation. Hypodermic needles, lasers, and mechanical devices have been used to correct cellulite. Temporary improvement in the appearance of cellulite can be obtained by noninvasive light and massage devices. Nondevice interventions include physical exercise, but weight loss is less helpful.
MODES OF ACTION
Subcision entails inserting a metal implement with a sharp end through the skin, and then moving it back and forth subdermally in a fanning motion to sever fascial bands and release fibrous attachments around pockets of subcutaneous fat depression or herniation (Fig. 211-9A). This results in elevation of the depressed area by mechanical release. Trauma associated with the procedure can secondarily induce collagen remodeling as well as capillary leaks that culminate in fibrotic plugs that further elevate the depressed area. Subcision with a hypodermic needle similar to that used for acne scar subcision was shown to be effective for cellulite by Doris Hexsel, a Brazilian dermatologist. Limiting factors were routine bleeding and bruising, and risk of hematoma. To make subcision32-36 for cellulite better tolerated, specific devices have been developed. These aim to minimize disfiguring bleeding and bruising, and to reduce the sensitivity of the procedure to minor differences in operator technique. An insertional Nd:YAG
3
31
laser device with a hot tip has been used to separate fascial bands and melt fat, while cauterizing small vessels to reduce bleeding. More recently, a device has been developed to mechanically elevate and hold the dermal–subcutaneous junction in place, after which standardized cold needles separate the fascia using a fanning motion. Remaining in the same plane mitigates the risk of injuring peripheral vessels. Device-based subcision for cellulite uses injection of dilute local anesthesia, so-called tumescent anesthesia, to protect skin structures by inflating the skin layers and inducing preoperative vasoconstriction. Noninvasive laser and light devices, often with multiple heads, have been used to treat cellulite. The FDA guidance for these devices notes that they37-40 may temporarily improve the appearance of cellulite. The primary mode of action appears to be the induction of edema, which camouflages cellulite dimples. There also may be some degree of mechanical disruption of the cellulite, but this is speculative and has not been definitely shown. Weight loss does not improve cellulite, which is a condition of the superficial subcutis and not of the deeper fat. Liposuction, by reducing superficial fat, can exacerbate cellulite, although in most cases liposuction is performed to avoid superficial suctioning and therefore has no net effect on cellulite. Physical exercise can improve cellulite by increasing muscle mass. Muscle growth increases the size of the compartment under the fat, pressing the fascia against the subcutis and dermis, and thus flattening cellulite.
Subcision for cellulite by sharp implement and bruising
A B
3867
31
AVOIDING AND MANAGING COMPLICATIONS
Bruising is the common, annoying but not serious complication of subcision-based techniques for cellulite reduction. Apart from being tender and impeding social activities in which the affected skin is exposed, bruising can be troublesome, if it resolves with persistent hyperpigmentation. This is more common in patients with darker-pigmented skin, who also may be left with dark marks caused at the point of needle or device insertions. Bruising in cellulite treatment can be minimized. Sharp injury to small vessels that results in bleeding and bruising can be reduced by employing devices that either cauterize or stabilize the skin tissue during the procedure (Fig. 211-9B). Allowing tumescent anesthesia to set for approximately 30 minutes or longer before the procedure ensures adequate vasoconstriction. Hematomas and seromas have been reported infrequently and appear to be relatively more likely after application of hot-tipped laser treatments that may induce copious focal trauma. If such fluid accumulation occurs, it needs to be decompressed by syringe extraction or surgical drainage. A preventive strategy is limiting the number of dimples treated at one time in a given contiguous anatomic area. Like bleeding and bruising, discomfort during the procedure can be managed by application of tumescent anesthesia. Such anesthesia also inflates the skin mechanically, reducing the risk of inadvertent injury to deeper structures and vessels.
ADAPTING TREATMENTS FOR ANATOMIC AREAS AND SKIN TYPES
In general, subcision-based treatments for cellulite are safe for all skin types. Patients with Fitzpatrick skin Type IV and higher may develop hyperpigmentation at the site of ecchymoses or entry sites. Buttock dimpling appears more amenable to treatment than cellulite of the thighs.
EXPECTED OUTCOMES
Treatment of cellulite can result in improvement of small skin dimples of the buttocks and thighs. Several treatments are typically required, and not all dimples will resolve. Better demarcated round dimples will improve more than larger, irregular ones, and buttock dimples may respond better than thigh dimples. Postoperative bruising and pinpricks at the site of insertion sites may be visible and tender for several days to 2 weeks. Hyperpigmentation in localized patches is possible, but uncommon, and is a greater risk in darker-skinned patients. Current treatments do not reduce the future risk of developing more cellulite. Physical exercise and stable, normal weight levels may improve cellulite, or at least slow its exacerbation.
3868
MEANS OF OPTIMIZATION
REPEAT THERAPIES
REPEAT THERAPIES
Treatments for skin tightening, fat reduction, and cellulite removal are often performed repeatedly for best effect. The likely number of treatments is dependent on the degree of the problem to be corrected, a discussion with the patient regarding their preference, and practical constraints, like the time required, patient tolerance of discomfort,41 and aggregate cost. There is increasing evidence that performing many treatments for skin tightening or fat reduction can result in marked and continuous improvement. Treatments are frequently spaced 1 to 3 months apart to allow for wound healing and collagen remodeling prior to retreatment.
COMBINATION THERAPIES
COMBINATION THERAPIES
In some cases, improvement may be maximized by using different modalities in combination for the same indication. For instance, several different technologies may be used for fat reduction for optimal effect. Different molecular mechanisms associated with these treatments may augment the cumulative improvement. Again, this requires planning, discussion with the patient, and communication of reasonable expectations.
SUMMARY
Noninvasive body-contouring methods, including skin tightening, fat reduction, and cellulite removal, are emerging technologies. Adverse events are minimal and posttreatment recovery time is brief. Younger to middle-aged adult patients with limited overall skin laxity and sagging are the best candidates. Effectiveness continues to improve and is further enhanced by repeat and combination treatments. Even though some single-intervention invasive surgical procedures for similar indications may be as, or even more, effective, patients are increasingly averse to the risk, scarring, and sense of invasiveness associated with these.
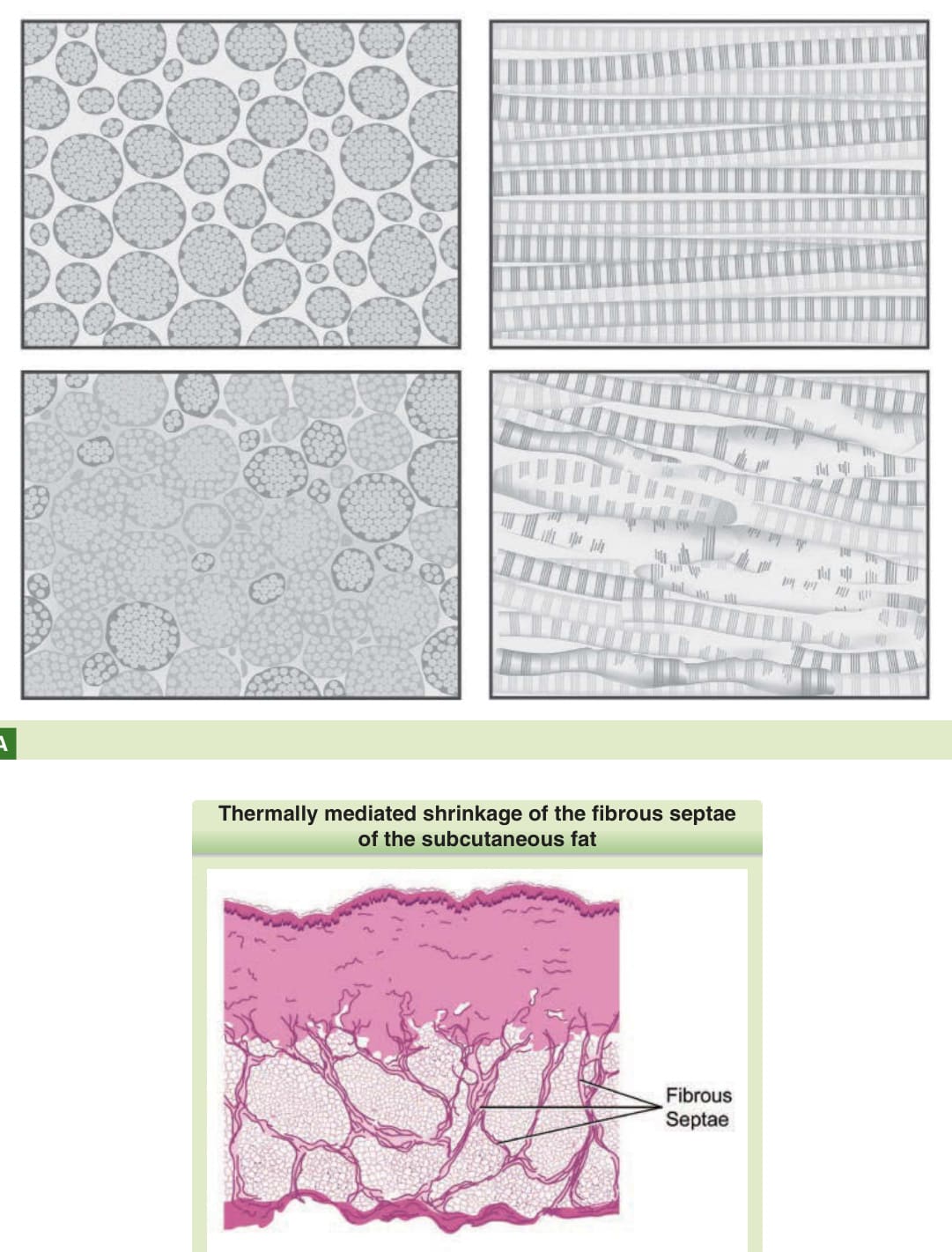
Figure 211-1 Immediate collagen denaturation and contraction (A), as well as thermally-mediated shrinkage of the fibrous septae of the subcutaneous fat (B), are among the mechanisms of noninvasive skin tightening.
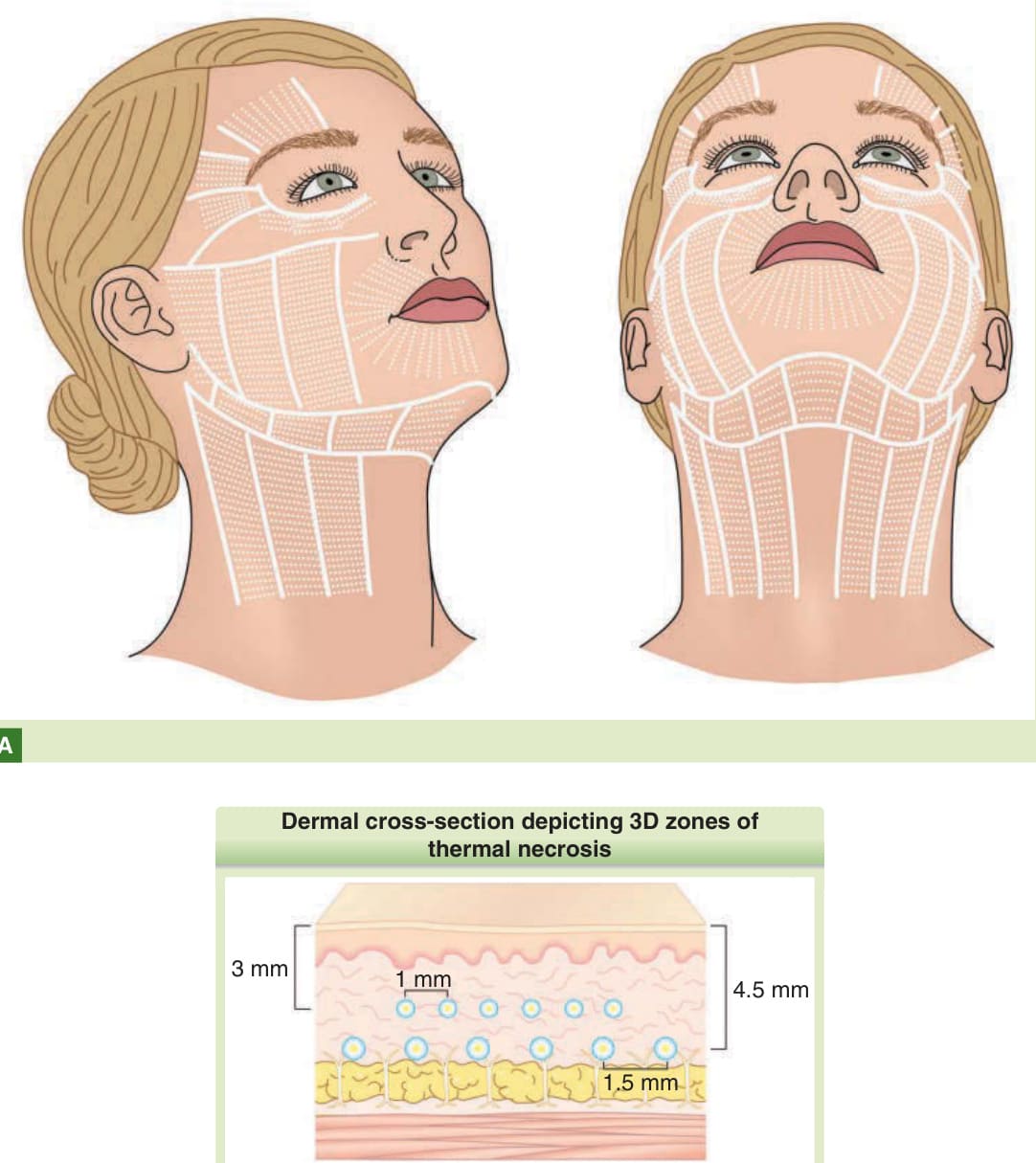
Figure 211-2 Noninvasive skin tightening proceeds by creating minute 3-dimensional zones of thermal necrosis in the dermis, with skin tightening the sum of immediate contraction and collagen remodeling over the ensuing months. Over time, these zones of thermal necrosis are placed ever more densely across the face (A) and in multiple planes in the skin (B), as demonstrated in these schematics of the facial surface and dermal cross section, respectively.

Figure 211-3 Noninvasive skin tightening was first quantitatively demonstrated for brow elevation, which is relatively easier to measure given the availability of anatomic landmarks. More recently, skin tightening has been used on the lower face, neck, and other parts of the body. (From Alam M, White LE, Martin N, et al. Ultrasound tightening of facial and neck skin: a rater-blinded prospective cohort study. J Am Acad Dermatol. 2010;62(2):262-69, Fig. 5, with permission.)
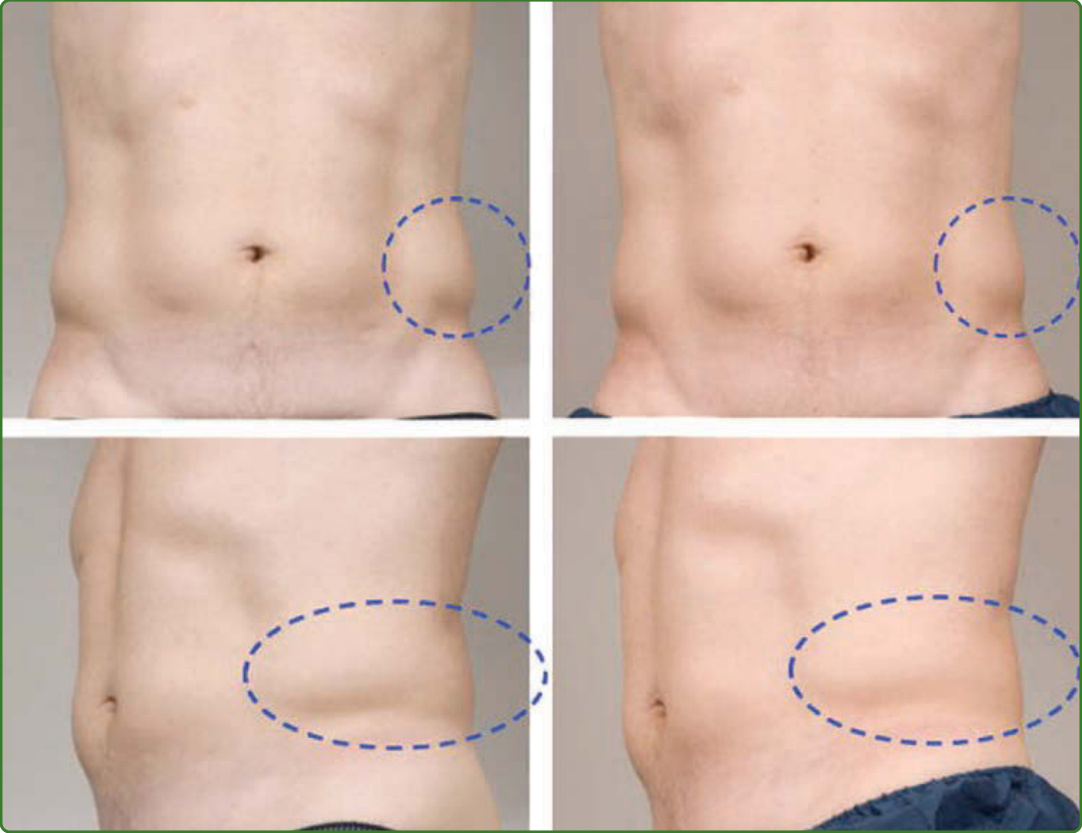
Figure 211-4 Fat reduction by cryolipolysis was first demonstrated to reduce the small fat pockets in the “love handles,” as shown in this figure. Noninvasive fat-reduction methods have since been also used to treat larger areas of subcutaneous fat and fat accumulations in the submental area on the neck, using modified handpieces and repeated treatments. (Reprinted by permission from Springer: Coleman SR, Sachdeva K, Egbert BM, et al. Clinical efficacy of noninvasive cryolipolysis and its effects on peripheral nerves. Aesth Plast Surg. 2009;33(4):482-488, Fig. 1. Copyright © 2009.)
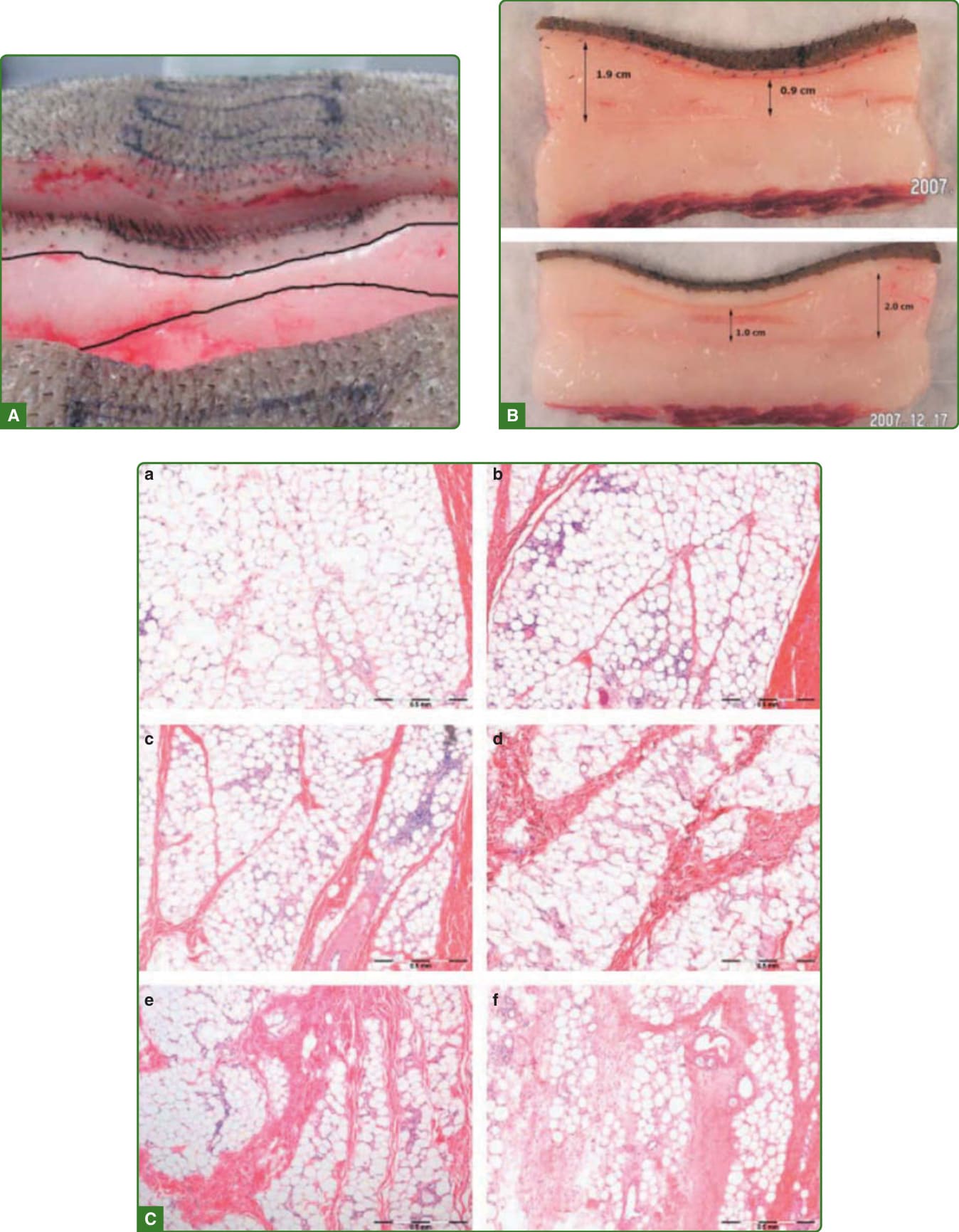
Figure 211-5 Fat shrinkage secondary to cryolipolysis creates a band of cold-mediated injury in the deep subcutis, with this causing shrinkage of the fat layer, in vivo (A) and ex vivo (B), as shown in this porcine model. Concurrently, there is an inflammatory reaction (C) that is easily seen from day 3 (top left) to day 90 (bottom right). (From Zelickson B, Egbert BM, Preciado J, et al. Cryolipolysis for noninvasive fat cell destruction: initial results from a pig model. Dermatol Surg. 2009;35(10):1462-70, Figs. 4, 6, and 8, with permission. © 2009 by the American Society for Dermatologic Surgery, Inc. Published by Wiley Periodicals, Inc.)
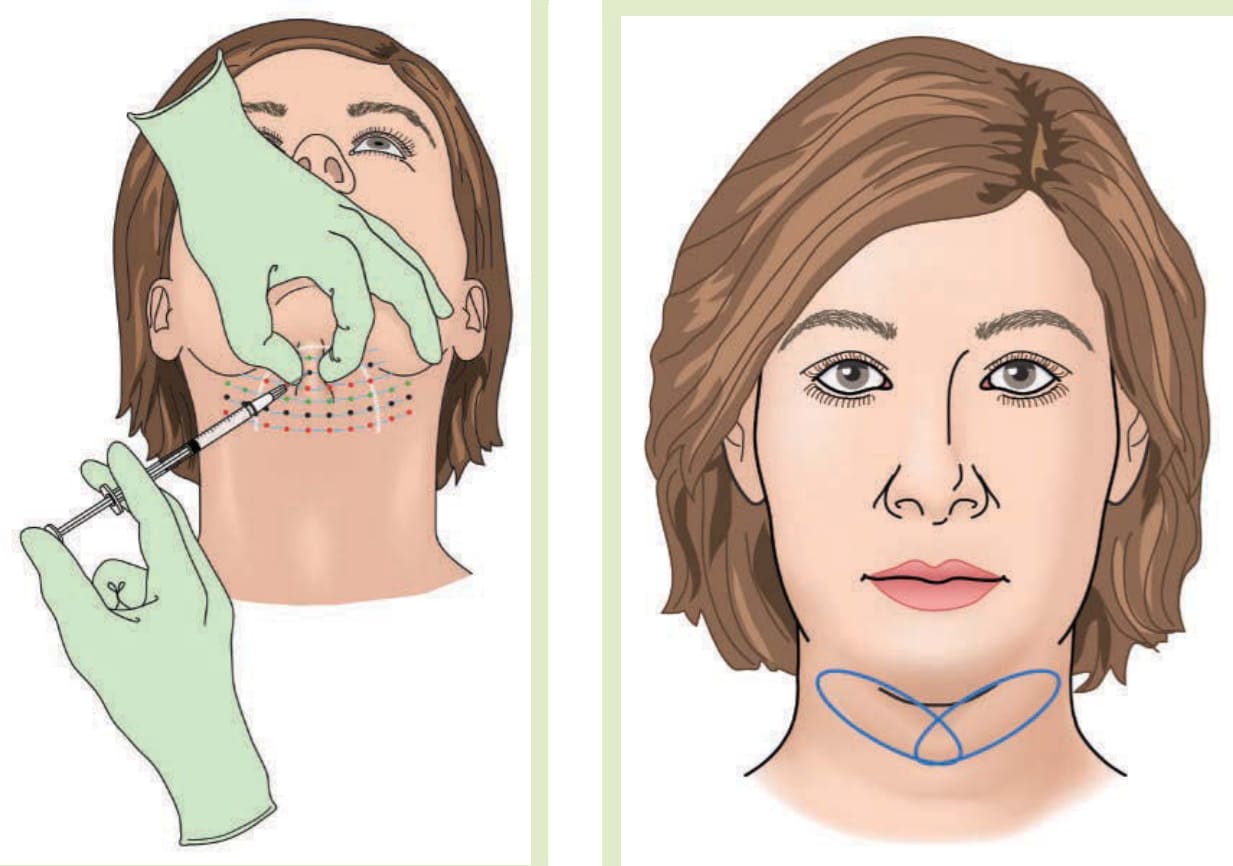
Figure 211-6 Nonsurgical treatment of submental fat can be accomplished by injection of deoxycholate in a grid-like pattern (A), or by 2 overlapping applications of a cryolipolysis device (B). The marginal mandibular nerve is avoided in both cases.
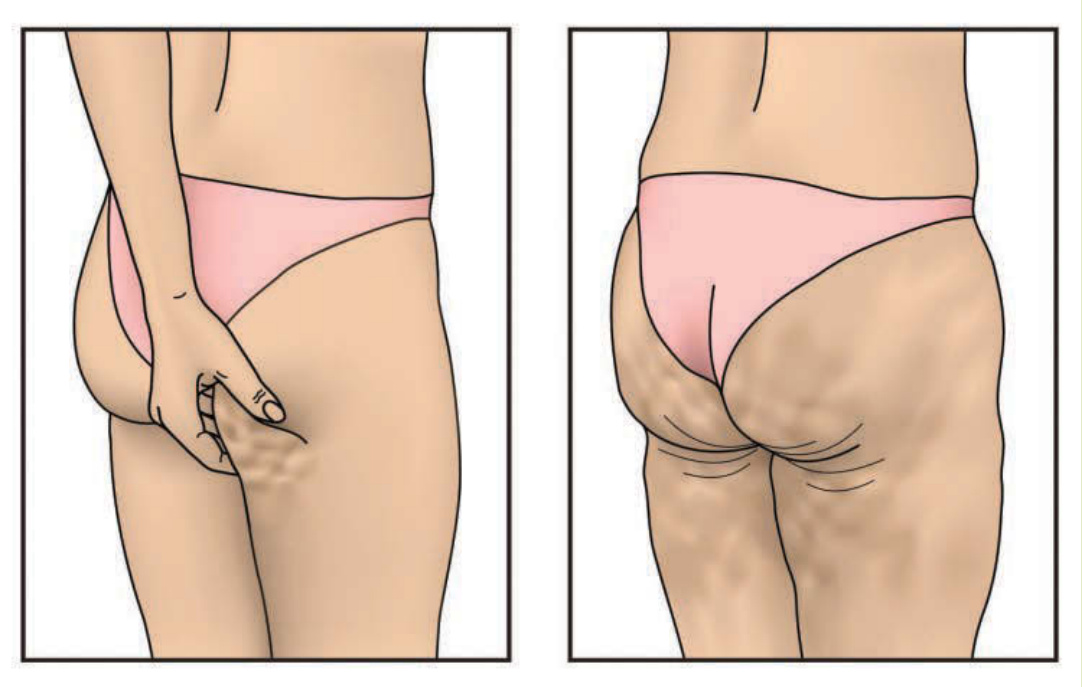
Figure 211-7 Cellulite is the dimpling of the skin on the thighs and buttocks, and can be incipient, elicited by manual compression (A) or full-blown, occurring even at rest (B).

Figure 211-8 Cellulite is believed to be potentiated by anatomic variation, particularly by the parallel fascial bands more characteristic in women (A). The fascial bands more typical in men, which are believed to be a more crisscross pattern (B), may be more resistant to subcutaneous fat herniation.
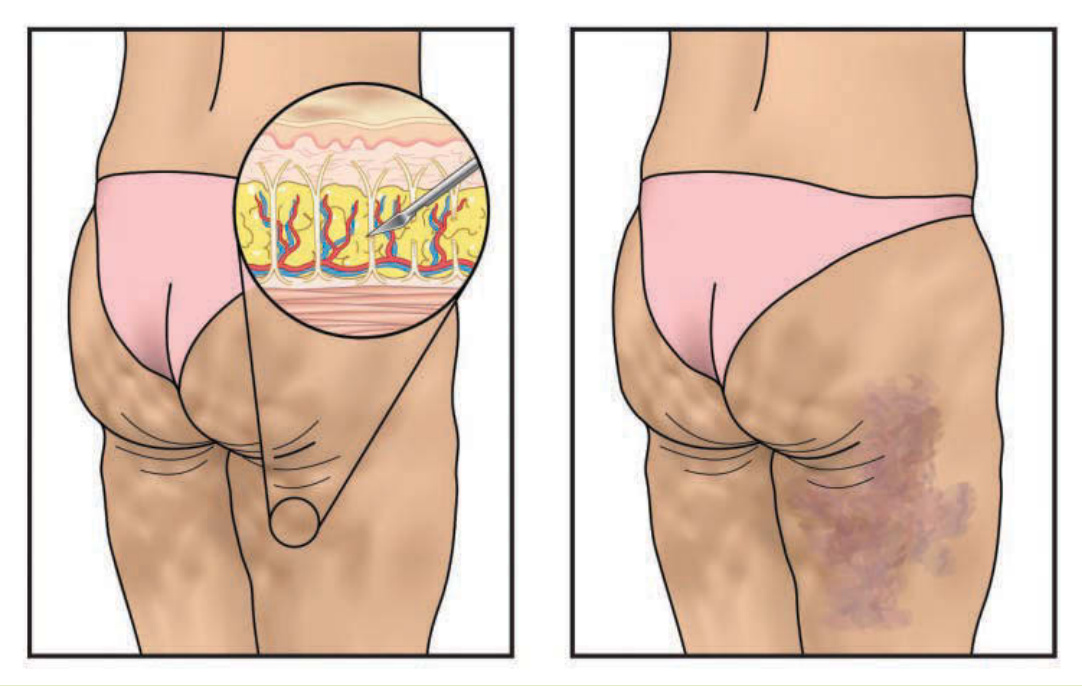
Figure 211-9 Subcision for cellulite entails release of skin dimpling by using a sharp implement in a rasping, fanning motion under the dermis to sever restrictive subcutaneous fibrous septae and fascial bands (A). Preoperative infiltration of tumescent anesthesia can mitigate bruising (B). More modern device-based variants of this technique are less operatordependent and less likely to cause pain or bruising.