Retinoids
28
AT-A-GLANCE
■ A retinoid is any molecule that by itself or through metabolic conversion binds to and activates retinoic acid receptors.
■ Retinoid receptors are ligand-dependent transcription factors.
■ The predominant retinoid receptors in human skin are retinoic acid receptor α (RAR-α), RAR-γ, retinoid X receptor α (RXR-α), and RXR-β. RAR-γ/RXR-α heterodimers bind to retinoic acid–responsive elements and are responsible for retinoid signaling.
■ Clinical use of topical retinoids:
■ Approved indications: acne, psoriasis, cutaneous T-cell lymphoma, Kaposi sarcoma, melasma, photoaged skin
■ Unapproved indications with clinical studies supporting benefit: postinflammatory hyperpigmentation, and early stretch marks
■ Clinical use of oral retinoids:
■ Approved indications: acne, chronic hand eczema, psoriasis, and cutaneous T-cell lymphoma
■ Unapproved indications with clinical studies supporting benefit: pityriasis rubra pilaris, premalignancies, photoaging, ichthyosis, and Darier White disease
■ Teratogenicity is the most concerning side effect. Mucocutaneous (cheilitis, xerosis, skin peeling, conjunctivitis) involvements are common, as are reversible abnormal results on laboratory tests (hyperlipidemia, increased liver enzyme levels, and hypothyroidism [bexarotene/alitretinoin]). Musculoskeletal and central nervous system side effects are rare.
INTRODUCTION AND BACKGROUND
Retinoids are widely used as prescription drugs as well as cosmeceuticals. They are able to elicit skin responses by mediating their effects through their intranuclear retinoid receptors, acting as transcription factors. Indeed, the discovery of retinoic acid receptors (RARs) and retinoid
X receptors (RXRs) have been pivotal to our understanding of the retinoid action mechanism.1,2 In 1976, Michael Sporn and his colleagues originally defined retinoids as both the naturally occurring compounds with vitamin A activity and the synthetic analogs of retinol. This concept is no longer adequate. Now, retinoid is defined as any molecule that, by itself or through metabolic conversion, binds to and activates the RARs, thereby eliciting transcriptional activation of retinoic acid–responsive genes, resulting in specific biologic responses. Our understanding of retinoid mechanism, as highlighted in this chapter, is primarily based on action of topical natural retinoids in vivo. Mechanism for oral retinoids is less clear, and further elucidation is needed.
PHARMACOLOGY AND MECHANISM OF ACTION
STRUCTURE
STRUCTURE
NOMENCLATURE
All-trans-retinoic acid (tretinoin), which binds to and activates RARs, is derived from sequential oxidation of all-trans-retinol (or vitamin A) and all-transretinaldehyde. It is a 20-carbon molecule that consists of a cyclohexenyl ring, a side chain with four double bonds (all arranged in trans-configuration), and a carboxylic-acid end group (Fig. 185-1). The numbering of the carbon atoms is as shown in Fig. 185-1. The terms 9-cis- (alitretinoin) and 13-cis-retinoic acid (isotretinoin) refer to stereoisomers of all-trans-retinoic acid in which the double bond that begins with the 9th and 13th carbon atoms, respectively, is in the cis- rather than transconfiguration. The fourth carbon atom is located in the cyclohexenyl ring of retinoic acid and is involved in a hydroxylation reaction to generate 4-hydroxy-retinoic acid (see Fig. 185-1). The addition of a hydroxyl group to the cyclohexenyl ring renders the molecule more polar, making it more amenable to excretion/elimination.3,4
A group of compounds referred to as retinyl esters functions as the molecular storage form of retinol. The compounds are formed by esterification of retinol with fatty acids (see Fig. 185-1), which specify the ester. Hydrolysis of retinyl esters regenerates retinol (see Fig. 185-1). Retinoids are also classified into first, second, and third generations. First-generation retinoids include all-trans-retinoic acid (tretinoin), 13-cis-retinoic acid (isotretinoin), and 9-cis-retinoic acid (alitretinoin).
28
Nomenclature of natural retinoids
Sequential oxidation of retinol
CH2OH
All-trans-retinol
CHO COOH
All-trans-retinaldehyde All-trans-retinoic acid
All-trans-retinoic acid and its stereoisomers
16 17 19 20
COOH
15 7 13 11 9
1 2 3 4
6 5
8 10 12 14
18
13 9
COOH
COOH
All-trans-retinoic acid 9-Cis-retinoic acid 13-Cis-retinoic acid
Hydroxylation of all-trans-retinoic acid and subsequent oxidation
COOH COOH COOH
OH O
All-trans-retinoic acid
4-Hydroxy all-trans-retinoic acid 4-Oxo-all-trans-retinoic acid
Esterification of retinol
O
CH2OH
C R
HO
H2O
All-trans-retinol
H2O
O
O R
Retinyl esters
Structural relationship of β-carotene and 14-hydroxy 4, 14-retro-retinol to retinol
CH2OH
All-trans-retinol
3396
β-Carotene
Through replacement of the β-ionone ring in all-transretinoic acid with an aromatic structure, newer retinoids, also known as second-generation of retinoids, were synthesized in the 1970s. These include etretinate, which is an ethyl ester, and its free acid metabolite, acitretin. With the discovery of retinoic acid receptors, receptor-specific, third-generation retinoids adapalene, tazarotene, and bexarotene were developed (Fig. 185-2). In fact, the second- and third-generation retinoids are also known as synthetic retinoids. They bear no structural similarities to all-trans-retinol or retinoic acid yet are still considered retinoids by virtue of
Chemical structures of the synthetic retinoids
O
O
Etretinate O
CH3
CH3 CH3 COOH
H3C
CH3
CH3O
Acitretin
COOH
H3CO
CH2
C H
2 C H2
Adapalene
O
OCH2CH3
N
S
Tazarotene
CH2
H3C
CH3
CH3 CH3 COOH
H3C
Bexarotene
28
their ability to activate the receptor(s), therefore mediating the retinoid effect.
RETINOID RECEPTORS
The discovery and characterization of RARs as having molecular features that are similar to steroid and thyroid hormone receptors were landmark findings.1,2 A characteristic common to these receptors is that they bind to regulatory regions in DNA called hormone response elements, or target sequences, and activate gene transcription in a ligand-dependent manner. These receptors bind to specific DNA sequences as dimers. The critical partner for heterodimerization and functioning of RAR is the RXR,5 whose physiologic ligand is 9-cis-retinoic acid.3 There are three different members of RAR (α, β, and γ) and RXR (α, β, and γ), each encoded by different genes. When the heterodimer binds to the hormone response element, specifically the retinoic acid–responsive element (RARE) in the gene promoter, the basal transcriptional machinery is stimulated. In skin, cellular retinoic acid binding protein (CRABP) II, cellular retinol binding protein (CRBP), retinoic acid 4-hydroxylase (CYP26), and keratin 6—all of which contain RAREs—are regulated by all-trans-retinoic acid.6-9 These protein products, in turn, activate other non–RARE-containing genes in a cascading reaction to produce the clinical features of retinoid action in skin (Fig. 185-3). Please see Table 185-1 for additional genes regulated by topical retinoids.
METABOLISM
METABOLISM
ESTERIFICATION AND OXIDATION OF RETINOL
Treatment of human skin with all-trans-retinol or retinaldehyde increases retinyl ester levels in the epidermal layer by more than 10-fold.6 This reaction is catalyzed by two enzymes: (1) lecithin/retinol acyltransferase and (2) acyl-coenzyme A/retinol acyltransferase. In human keratinocytes, lecithin/retinol acyltransferase has the predominant retinol-esterifying activity.10
Sequential oxidation of all-trans-retinol forms alltrans-retinoic acid, with all-trans-retinaldehyde as the intermediate metabolite. The first step (oxidation of all-trans-retinol to all-trans-retinaldehyde) is rate limiting for all-trans-retinoic acid formation. Application of all-trans-retinol or retinaldehyde to human skin results in histologic and molecular alterations that mimic those after all-trans-retinoic acid treatment.6 These include epidermal hyperplasia; epidermal spongiosis; compaction of the stratum corneum; and induction of CRBP, CRABP-II, and CYP26.10,11
HYDROXYLATION OF ALL-TRANS- RETINOIC ACID
In human skin, all-trans-retinoic acid is catabolized primarily to the more polar 4-hydroxy-all-trans-retinoic
3397
28
Cellular metabolism of natural retinoids and molecular mechanism of retinoid-specific gene activation
Cytoplasm
4-OH t-RA
t-RA– CRABP II
CYP26
t-RA
ROL
CRBP-I
L R A T
R E H
ROL
9c RA 13c RA
5′ Nucleus
9c RA
RXR-α
AGGTCA
AGGTCA 5n
t-RA t-RA RAR-γ
mRNA
3′
GENEa ROLE
Cellular retinol binding protein (CRBP) Intracellular transport protein for retinol
Cellular retinoic acid binding protein (CRABP) II
Intracellular transport protein for retinoic acid
Retinoic acid 4-hydroxylase (CYP26)
Cytochrome P450 enzyme that inactivates all-trans-retinoic acid by hydroxylation at the fourth carbon molecule; this CYP26 is inducible by retinoic acid
Keratin 6 An intermediate filament; pairs with keratin 16 or 17
Heparin-binding (HB)-EGF Induced by retinoic acid; stimulates basal cell growth via EGF receptor activation; neither HB-EGF nor AR possesses RARE; thus, RAR/RXR is likely regulating other transcription factor(s) that would, in turn, regulate AR and HB-EGF gene expression
Amphiregulin (AR)
Amphiregulin (AR)
aGenes known to be regulated by topical retinoids. (HB)-EGF, heparin binding-epidermal growth factor; RARE, retinoic acid– responsive element; RXR, retinoid X receptor.
3398
acid, which is further metabolized to 4-oxo-retinoic acid. In untreated normal human skin, CYP26 activity is minimally detectable. Administration of alltrans-retinoic acid, all-trans-retinol or retinaldehyde to human skin, however, increases its activity several fold.11,12 The CYP26 activity can be effectively inhibited by ketoconazole and a related azole, liarozole.12,13 By blocking this major inactivation pathway of all-transretinoic acid, topical liarozole can serve as a retinoic acid mimetic amplifying human skin responses to alltrans-retinol and all-trans-retinoic acid.13 This approach of targeting CYP26 has given rise to a novel class of new chemical entities referred to as retinoic acid metabolism blocking agents (RAMBAs). The drug development progress for RAMBA, however, has been slow.
ORAL RETINOIDS
Metabolism and pharmacokinetics for oral retinoids share similarities as topical retinoids but also exhibit differences. Because of their lipophilicity, the oral bioavailability of all retinoids is markedly enhanced when they are administrated with food, especially with fatty meals. Retinoids are metabolized mainly by oxidation and chain shortening to biologically inactive and
hydrophilic metabolites, which facilitate biliary or renal elimination (or both).
Isotretinoin and Other First-Generation Retinoids: Isotretinoin and alitretinoin are partially interconvertible isomers that differ in their elimination half-lives. Isotretinoin undergoes first-pass metabolism in the liver and subsequent enterohepatic recycling. The major metabolite is 4-oxoisotretinoin, which has reduced bioactivity; both compounds are excreted in urine and feces. After the end of treatment, endogenous concentrations of isotretinoin and its major metabolite are reached within 2 weeks. Therefore, a 1-month posttherapy period of contraception provides an adequate safety margin.14
Acitretin and Etretinate: Etretinate is a prodrug of acitretin that undergoes extensive hydrolysis in the body to yield the corresponding acid metabolite. Acitretin has a great pharmacokinetic advantage because it is eliminated more rapidly than etretinate.15
Whereas etretinate is approximately 50 times more lipophilic than acitretin and binds strongly to plasma lipoproteins, acitretin binds to albumin. Thus, after etretinate is taken, it is stored in adipose tissue from which it is released slowly; it has a half-life of up to 120 days. In contrast, acitretin has a half-life of only 2 days.15 However, small amounts of etretinate can be formed in patients receiving acitretin if it is taken simultaneously with alcohol.16 This has prompted the manufacturer to extend the time of compulsory contraception in patients taking acitretin to 2 years (3 years in the United States).17 Acitretin still has a pharmacokinetic advantage over etretinate; however, all women must strictly avoid alcohol consumption during treatment and for 2 months thereafter.16 Acitretin metabolism primarily involves isomerization instead of oxidation. The major metabolite of acitretin is its 13-cis-isomer, which is inactive.
Bexarotene: Bexarotene is approximately 100- fold more potent in activating retinoid X receptors than RARs. The half-life for this drug is between 7 and 9 hours.18 Bexarotene is metabolized by CYP 3A4 and generates its own inactive oxidative metabolites via hepatic CYP 3A4 induction. Neither bexarotene nor its metabolites are excreted in urine; thus, elimination is believed to occur primarily via the hepatobiliary system.19
INDICATIONS AND CONTRAINDICATIONS
TOPICAL RETINOIDS
TOPICAL RETINOIDS
Until recently, clinical use of topical retinoids has been limited to all-trans-retinoic acid, which is approved in the United States for the treatment of acne, photoaged skin, and melasma. Topical adapalene and tazarotene have also received approval for acne; tazarotene has received approval for psoriasis and photoaging.
28
Bexarotene is approved for management of cutaneous T-cell lymphoma, and alitretinoin is approved for patients with Kaposi sarcoma (KS). It is widely accepted that topical retinoids are extremely effective for acne therapy, especially for comedonal lesions. Of the different antiacne medications, retinoids are thought to be the best, if not the only, agents to normalize the abnormal follicular epithelial differentiation and desquamation that occur in acne. Therefore, the use of retinoids can also provide protection against the development of new lesions. This prophylactic property is the basis for including topical retinoid in almost all antiacne regimens. Moreover, in an era in which antibiotic stewardship has come to the forefront, retinoid is playing an even more important role in acne treatment in place of antibiotics. Fine wrinkles and dyspigmentation are two features of photoaged skin that are improved by topical tretinoin or tazarotene. Several weeks of treatment are required before clinical improvement is appreciated.20-22 For the effacement of fine wrinkles by topical tretinoin, partial restoration of markedly reduced levels of collagen in sun-exposed skin toward those seen in sun-protected skin appears to be responsible.21,23
Primary cutaneous T-cell lymphoma (CTCL) is characterized by clonal proliferation of skin-homing malignant T lymphocytes. As an RXR-selective retinoid, topical bexarotene inhibits tumor cell growth, encourages terminal differentiation, and induces apoptosis.24
It may also play a role in chemoprophylaxis.25,26
Alitretinoin gel was approved in 1999 for the management of cutaneous KS, which is caused by human herpes virus 8 (HHV-8). Alitretinoin’s mechanism of action in KS is not entirely clear, but it presumably relates to inhibition of cellular proliferation as well as induction of apoptosis seen with other retinoids. Furthermore, alitretinoin and tretinoin have been reported to inhibit herpes simplex virus replication; thus, alitretinoin may have an antiviral role against HHV-8.27 In clinical trials, most patients saw improvement after 4 to 8 weeks of treatment with the most significant response occurring after 14 weeks of therapy.28
Besides the approved indications, topical retinoids have been demonstrated to be effective in the treatment of several other conditions. These include, but are not limited to, postinflammatory hyperpigmentation in blacks,29 actinic dyspigmentation in Chinese and Japanese individuals,30 and early stretch marks.31 The controlled studies show more than therapeutic efficacies. They also provide valuable information to dispel some of the myths about retinoid use in humans. For example, African Americans and Asians tolerate topical tretinoin as well as, if not better than,29,30,32 whites.21,33 Furthermore, the often observed retinoid dermatitis does not usually lead to postinflammatory hyperpigmentation in those with greater constitutive pigmentation. Many other skin disorders have been reported to be improved by topical retinoids, but most of them have not been rigorously studied; thus, their therapeutic claims should be interpreted with caution. Molluscum contagiosum, warts, and various forms of ichthyosis
3399
28
may be improved by topical retinoids to a variable degree. In psoriasis, especially, irritation of treated skin has limited the use. Topical tazarotene, which is approved for psoriasis, does not appear to have fully overcome the irritation problem34; thus, it is typically used in combination with topical steroids. With such a wide variety of skin conditions treatable by topical retinoids, their use has included all age groups, perhaps with the exception of neonates. The use of topical retinoids in pregnancy is an emotional issue. As discussed later, teratogenicity is not caused by topical retinoids. However, because none of the dermatologic conditions seen in pregnancy that may respond to topical retinoids (ie, acne, melasma, stretch marks) is life threatening to the mother or the fetus, it seems prudent to delay the treatment until after delivery.
ORAL RETINOIDS
ORAL RETINOIDS
Isotretinoin is remarkably effective in treating acne, possibly because it affects majority of etiologic factors implicated in the pathogenesis of acne: sebum production (caused by atrophy of sebaceous glands not achievable by topical retinoids or other systemic retinoids), comedogenesis, and colonization with Propionibacterium acnes.35 In the early 1980s, isotretinoin treatment was restricted to patients with severe nodulocystic acne. Its use now has extended to patients with less severe disease who respond unsatisfactorily to conventional therapies or who have extensive scarring.36,37 Lastly, in the age of antibiotic stewardship, isotretinoin has also been explored for the treatment of rosacea in an off-label manner.38,39
In addition to acne, oral retinoid is also used to manage psoriasis and the retinoid of choice is acitretin. The best results have been obtained in pustular psoriasis of the palmoplantar or generalized (von Zumbusch) type.40-42 Rebound does not usually occur after cessation of treatment, and reintroduction of the drug produces a beneficial response.43 Although complete clearing of plaque-type psoriasis is achieved in only approximately 30% of treated patients, significant improvement is obtained in a further 50%.44-46 The decrease in the psoriasis area and severity index is approximately 60% to 70%, depending on the dosage.44,47 Combination of acitretin with other antipsoriatic agents may be required. Oral retinoid can also be used to manage chronic hand eczema. Alitretinoin is approved in Europe and Canada for treatment-resistant chronic hand eczema. Between 3 and 6 months of therapy is usually required to fully appreciate the effect.48 This medication is not yet available in the United States. In 1999, the U.S. Food and Drug Administration (FDA) approved bexarotene as oral therapy for the treatment of CTCL that is refractory to at least one systemic therapy. In early (IA–IIA) and advanced (IIB– IVB) stages of CTCL, oral bexarotene monotherapy produced approximately 60% and 50% response rates,
3400
respectively, at a dosage of 300 mg/m2 or more per day within the first 2 months in most patients.49,50
Multiple other skin disorders respond to oral retinoids but for only a few of them is the effect established in controlled studies.51 In pityriasis rubra pilaris, early treatment with acitretin appears to offer the best chance for clearing of this eruption. In extensive cases, concomitant use of methotrexate may be advantageous, but this combination carries an increased risk for toxicity.52
Acitretin is effective in the treatment of premalignancies, including human papillomavirus–induced tumors and actinic keratoses. In basal cell nevus syndrome and xeroderma pigmentosum, these drugs dramatically reduce the incidence of malignant degeneration of the precancers. A double-blind study demonstrated that acitretin at a dosage of 30 mg/day for 6 months prevented the development of premalignant and malignant skin lesions in renal transplant recipients.53
More recently, there is an increase in usage of lowdose oral retinoids for photoaging, especially outside of the United States. However, data regarding this indication are mixed. In one study, isotretinoin significantly improved the clinical features of photoaging and increased collagen as well as elastic fiber density.54 In contrast, other studies found no significant differences in clinical and histologic improvement of photoaging when comparing isotretinoin to topical retinoic acid 0.05%. No significant differences were also seen when comparing isotretinoin to daily sunscreen use.55,56 More rigorous studies are needed to further elucidate these effects. Furthermore, one must also consider the potential adverse effects of oral retinoids when choosing this treatment modality for skin aging. Oral retinoid therapy has also been used in various forms of ichthyosis. The best results are obtained with acitretin for autosomal recessive congenital ichthyoses such as lamellar ichthyosis. Moderate to severe forms of Darier-White disease have also been shown to respond to retinoid therapy. Care should be taken to initiate therapy with a low dosage, such as 10 mg/day of acitretin, to prevent initial exacerbation of the disease; usually 20 mg/day is sufficient for significant improvement. Long-term treatment is usually needed to prevent relapse.
DOSING REGIMEN
TOPICAL RETINOIDS
TOPICAL RETINOIDS
For decades, tretinoin was the only topical retinoid available for clinical use sold under the trade name Retin-A. Now, tretinoin is also available in other formulations (Table 185-2). Adapalene is also available in varying formulations, and more recently, combination medications have been introduced (see Table 185-2). For acne and psoriasis, topical tazarotene is available and for photoaging treatment, tretinoin and tazarotene are
TOPICAL RETINOID DOSAGE SCHEDULES AND EXAMPLE FORMS
Tretinoin Avita (0.025% cream and gel) Atralin (0.05% gel) Refissa (0.05% cream) Renova (0.02% cream) Retin-A (0.025%, 0.05%, 0.1% cream; 0.01%, 0.025% gel) Retin-A Micro (0.04% and 0.1% microsphere gel) Tretin-X (0.025%, 0.05%, 0.1% cream; 0.01%, 0.025% gel) TriLuma (tretinoin 0.05%/hydroquinone 4%–fluocinolone 0.1% cream) Ziana (tretinoin 0.025%/clindamycin 1.2% gel)
Adapalene Differin 0.1% cream; 0.1%, 0.3% gel) Epiduo (adapalene 0.1%/benzoyl peroxide 2.5% gel)a
Tazarotene Tazorac 0.05%, 0.1% gel and cream Avage (0.1% cream)
Bexarotene Targretin gel
Alitretinoin Panretin gel
Alitretinoin Panretin gel
aThe chemical structure of adapalene renders it more resistant to oxidation (thus permitting its combination with benzoyl peroxide) and ultraviolet degradation frequently seen with retinoids.
approved for use. Tretinoin 0.05%/hydroquinone 4%– fluocinolone 0.1% is a topical combination approved for the treatment of melasma. Different formulations allow some flexibility in terms of tailoring the therapy to an individual’s skin dryness or oiliness. Finally, more recently approved topical retinoids, including bexarotene and alitretinoin, are sold in gel formulations. The most important element in topical retinoid therapy is patient education. It must be explained to each patient that local skin irritation, characterized by redness and peeling, can be expected. The concept that clinical improvement correlates with the degree of irritation has been erased through a large, controlled clinical study in which 0.025% and 0.1% tretinoin were shown to be equally efficacious, but the former was
28
significantly less irritating than the latter.22 Therefore, unlike most medications for which the dosing schedule may be set as once or twice daily, administration of a topical retinoid should be individualized and titrated depending on the skin reaction. Under the nonprescription category, there are countless “natural retinoid” preparations with various claims (mostly antiaging). Most of these contain retinyl esters, which are less active than retinol and retinaldehyde. Whether any of these products can deliver retinoid activity to human skin should be established in every case and formulation. Current experts’ views are that, with appropriate dosing and formulation, some preparations do induce biological effects that may reverse and partially prevent skin aging.
ORAL RETINOIDS
ORAL RETINOIDS
The consensus is that optimal benefit in acne would be achieved with a daily dose of isotretinoin, approximately 0.5 to 1 mg/kg of body weight per day (Table 185-3).35 Posttherapy relapse is minimized by administering a cumulative dose of at least 120 mg/kg.57 This implies 6 to 8 months of therapy. A lag period of 1 to 3 months may occur before the onset of the therapeutic effect, and a flare-up of disease during the first few weeks may be observed. Continued healing of acne after the discontinuation of therapy regularly occurs. Approximately one third of patients with acne require a second course of therapy for either persistent disease or relapse. The recommended alitretinoin dose in treatment of chronic hand eczema is 10 to 30 mg/day. Treatment periods of up to 6 months are often needed before a full evaluation of the therapeutic effects can be made. In psoriasis, patients are typically given an initial low dose of 10 to 25 mg/day of acitretin followed by progressively increasing doses.58 Total clearing of the lesions may require a combination of treatments, such as retinoids plus topical glucocorticoids, topical vitamin D derivatives, dithranol (anthralin), ultraviolet B irradiation, or photochemotherapy (psoralen and ultraviolet A light [PUVA] treatment).59-63
DRUG INDICATION INITIALLY (mg/kg/day) SUSTAINED (mg/kg/day) LENGTH OF THERAPY (months)
Isotretinoin Acne 0.3–0.5 0.5–1.0 4–6
Acitretin Psoriasis 0.2–0.5 0.3–0.8 >3
DOKa 0.3–0.6 0.5–1.0 >3
Alitretinoin Hand eczema 10–30b 10–30b >6
Bexarotene CTCL 4–8 2–4 (8) >2
Bexarotene CTCL 4–8 2–4 (8) >2
aLower dosing is recommended for Darier-White disease and epidermolytic ichthyosis.
3401
bDaily dose in milligrams. CTCL, cutaneous T-cell lymphoma; DOK, disorders of keratinization (genetic).
28
The recommended initial dosage of bexarotene is 300 mg/m2/day, administered as a single oral dose with meals. Based on the severity of adverse effects, the dosage may be adjusted down to 100 or 200 mg/m2/day, or administration may be suspended temporarily. If CTCL does not respond after 8 weeks of therapy, the dosage may be increased to 400 mg/m2/day with careful monitoring.49,50
SIDE EFFECTS AND PRECAUTIONS
ADVERSE EFFECTS
ADVERSE EFFECTS
TOPICAL RETINOIDS
The most common adverse effect associated with topical retinoid use is local skin irritation. This predictable skin response is temporary, but troubling, for many patients. It tends to peak within the first month of treatment and diminishes thereafter. It responds to a temporary reduction in the frequency or amount of retinoid application and to liberal use of emollients. For bexarotene and alitretinoin, local irritation is also the most common side effect. With alitretinoin, the local erythema can increase to edema and vesiculation with continued use. However, most reactions are mild to moderate with only 7% of patients requiring treatment withdrawal in clinical trials.28 Finally, the central hypothyroidism seen with systemic bexarotene is not observed when used in the gel formulation.64,65
Systemic retinoid exposure, as discussed later, has been well established as a cause of embryonic death and congenital malformation, and understandably, there is concern about potential teratogenicity from long-term topical retinoid use. Systemic absorption of retinoids from topical application is negligible, and the levels of endogenous retinoic acid in the blood are not increased by twice-daily application of 0.025% tretinoin to more than 40% of body area over 1 month. Furthermore, controlled topical administration of tretinoin at
doses used for acne therapy (2 g of 0.025% gel applied daily to the face, neck, and upper part of the chest for 14 days) has less influence on plasma levels of endogenous retinoids than diurnal and nutritional factors.66
Indeed, a large, population-based study demonstrated no excess risk of birth defects in offspring born to mothers who were exposed to topical tretinoin during pregnancy.67 Therefore, no evidence exists for teratogenicity of topical tretinoin in humans.
ORAL RETINOIDS
See Table 185-4. Teratogenesis as alluded to earlier is the most serious adverse effect of oral retinoids. Retinoid-induced birth defects include auditory, cardiovascular, craniofacial, ocular, axial and acral skeletal, central nervous system (hydrocephalus, microcephaly), and thymus gland abnormalities.68 In men, retinoid therapy does not appear to produce abnormalities in spermatogenesis, sperm morphology, or sperm motility.69 However, it is usually recommended that men who are actively trying to father children avoid systemic retinoid therapy. Most patients receiving oral retinoids will also develop dryness of the lips, skin, and mucous membranes. More severe cases can lead to significant retinoid dermatitis, which can be misdiagnosed as an allergic reaction to the drug with resulting inappropriate discontinuation of the retinoid medication. Bexarotene appears to induce fewer mucocutaneous and ocular side effects than other classes of retinoids; localized or extensive exfoliative dermatitis is the most common cutaneous side effect with bexarotene.18
Staphylococcus aureus colonization tends to correlate with isotretinoin-induced reduction in sebum production and may lead to overt cutaneous infections.70 Various ill-defined skin eruptions, called retinoid dermatitis, are also observed frequently. Blepharoconjunctivitis occurs with varying severity in about one third of patients treated with isotretinoin, likely related to its effects on meibomian glands. If artificial tears fail to alleviate the conjunctivitis, ophthalmologic consultation should be sought. Alterations in
ISOTRETINOIN ALITRETINOIN ACITRETIN BEXAROTENE
Teratogenicity + + + +
Mucocutaneous + + + +
Ocular ++ + + +
Alopecia (+) + + +
Headache + ++ + +
Musculoskeletal ++ + + +
Hepatotoxicity (+) (+) + +
Neutropenia − − − +
Hyperlipidemia ++ + + ++
3402
Hypothyroidism − + − +
Hypothyroidism − + − +
visual function, mainly poor night vision, excessive glare sensitivity, and changes in color perception, also have been reported.71
Diffuse or localized hair loss (telogen effluvium), which is more severe during treatment with acitretin than with isotretinoin, is a common complaint, although objective alopecia tends to occur only at higher dosage levels and after several months of therapy. Nail thinning and paronychia-like changes with periungual granulation tissue may occur. Bone pain without objective evidence of any abnormalities and without sequelae is frequent in retinoidtreated patients. Several reports with conflicting results have implicated synthetic retinoids in the formation of diffuse idiopathic skeletal hyperostosis (DISH) syndrome–like bone changes and calcification of tendons and ligaments.72-74 Prospective studies have shown that the hyperostotic effects of retinoids are mostly asymptomatic and likely involve worsening of preexisting skeletal overgrowth rather than de novo changes.75,76 No baseline radiographs are required, although monitoring patients at high risk who receive prolonged high-dose retinoid treatment may be useful. Muscle pain and cramps rarely occur in patients taking etretinate or acitretin; however, these muscle effects are frequent with isotretinoin, particularly in individuals involved in vigorous physical activity. Increased muscle tone, axial muscle rigidity, and myopathy were reported to be related to etretinate and acitretin therapy.77
Central nervous system side effects are rare. Although signs of increased intracranial pressure are observed occasionally, the complete syndrome with papilledema (pseudotumor cerebri) and impaired vision is exceptional.78 Concomitant use of isotretinoin and tetracyclines, which rarely produce increased intracranial hypertension, is the major risk factor for development of pseudotumor cerebri. Anecdotal reports suggest a causal association between isotretinoin therapy and severe depression with suicide attempts.79 However, large-scale epidemiologic studies provide no evidence that isotretinoin exposure is associated with any greater risk of psychiatric disorders than is antibiotic use in patients with acne.80
Clinical and biochemical central hypothyroidism occurred in 40% of patients in the trials of bexarotene therapy for CTCL. It was rapidly and completely reversible with cessation of therapy without any clinical sequelae.49,81 The same adverse effect has been noted with alitretinoin, which is expected because both drugs bind to RXR that dimerizes with the nuclear thyroid receptor. In very rare cases, isotretinoin has been linked to exacerbation of inflammatory bowel disease. A 5-year prospective study did not demonstrate an increased risk of inflammatory bowel disease or of cancer, diabetes, or cardiovascular disease in association with longterm etretinate use for psoriasis82; similar safety of long-term acitretin, bexarotene, or alitretinoin therapy has not been established. Serum lipid changes are the most frequent abnormalities in laboratory test results seen with retinoid therapy. Interestingly, retinoid-induced hyperlipidemia
28
is not associated with accelerated atherosclerosis or increased risk of cardiovascular disease with prolonged therapy. Depending on the type and dosage of retinoid, triglyceride levels are elevated in 50% to 80% and cholesterol levels in 30% to 50% of treated patients.49,73,83 Disturbance of blood lipid levels is generally higher with isotretinoin and bexarotene than with acitretin. In cases of severe retinoid-induced hypertriglyceridemia, eruptive xanthomas and acute pancreatitis may occur. Discontinuation of therapy is required if the triglyceride level reaches 800 mg/dL. A less severe increase may be treated by dosage reduction or lifestyle changes. In some instances, use of lipidlowering agents may be indicated.84 Coadministration of atorvastatin with bexarotene is recommended.18
Transient abnormal elevations in serum transaminase levels have been reported in approximately 20% of patients treated with etretinate or acitretin and occur much less frequently with other retinoids. Increases in serum alkaline phosphatase levels have been reported infrequently with isotretinoin and are clinically insignificant. Transaminase elevations of more than three times the upper normal range should lead to discontinuation of retinoid therapy. It is believed that in patients with hepatic insufficiency, there is impaired retinoid drug elimination.85
A high incidence (28%) of dose-related neutropenia has been reported with the use of bexarotene therapy for CTCL, occurring as early as 2 to 4 weeks after initiation of treatment.49 Hematologic abnormalities are much less common with other retinoids. Bleeding complications caused by isotretinoin-induced fibrinolysis has been reported.86
MONITORING OF THERAPY
Most adverse effects associated with retinoids are preventable and manageable with proper patient selection, dosage adjustments, discontinuation of treatment, and routine monitoring for potential toxicity. With isotretinoin, women with childbearing potential must have two negative results on a pregnancy test spaced 30 days apart and must practice effective contraception during treatment and for 1 month (2 months in some countries) after the completion of therapy.87 The iPLEDGE program (http://www.ipledgeprogram.com) has been put into effect by the FDA and the manufacturer to minimize the risk of isotretinoin teratogenicity. Similar but less strict programs exist in Europe and elsewhere. Ensuring that the patient avoids pregnancy during therapy is as imperative when prescribing acitretin and etretinate as when prescribing isotretinoin. However, because of the frequent prospect of long-term treatment of more chronic diseases (eg, psoriasis and ichthyosis) and the slow elimination of aromatic retinoids from the body after interruption of therapy, acitretin (or etretinate) therapy is usually not recommended for female patients with childbearing potential. Additional precautions before oral retinoid therapy include measurement of baseline serum lipid, complete blood count, thyroid function (bexarotene, alitretinoin), and liver enzyme levels. Laboratory studies are also
3403
28
performed during therapy. Providers should also assess for any history of skeletal abnormalities.
DRUG INTERACTIONS
DRUG INTERACTIONS
The major avenue of tretinoin inactivation is through CYP26. Ketoconazole and liarozole are effective inhibitors of CYP26 and thus concurrent use of these azoles and topical tretinoin can prolong the half-life of tretinoin locally in the skin, thereby aggravating local side effect. Other than retinoids, no other compounds have been shown to induce CYP26. The concurrent use of oral retinoids with other therapies having similar side effects may increase the risk of these adverse events. Tetracyclines (increased intracranial pressure, phototoxicity), alcohol (increased conversion of acitretin to etretinate, hepatoxicity), methotrexate (hepatoxicity), and vitamin A supplements (hypervitaminosis A) should be avoided. The concomitant administration of bexarotene and gemfibrozil may result in increased plasma concentrations of bexarotene.
ACKNOWLEDGMENTS
We would like to acknowledge the contributions of Laura Vangoor, BFA, for the graphic illustrations.
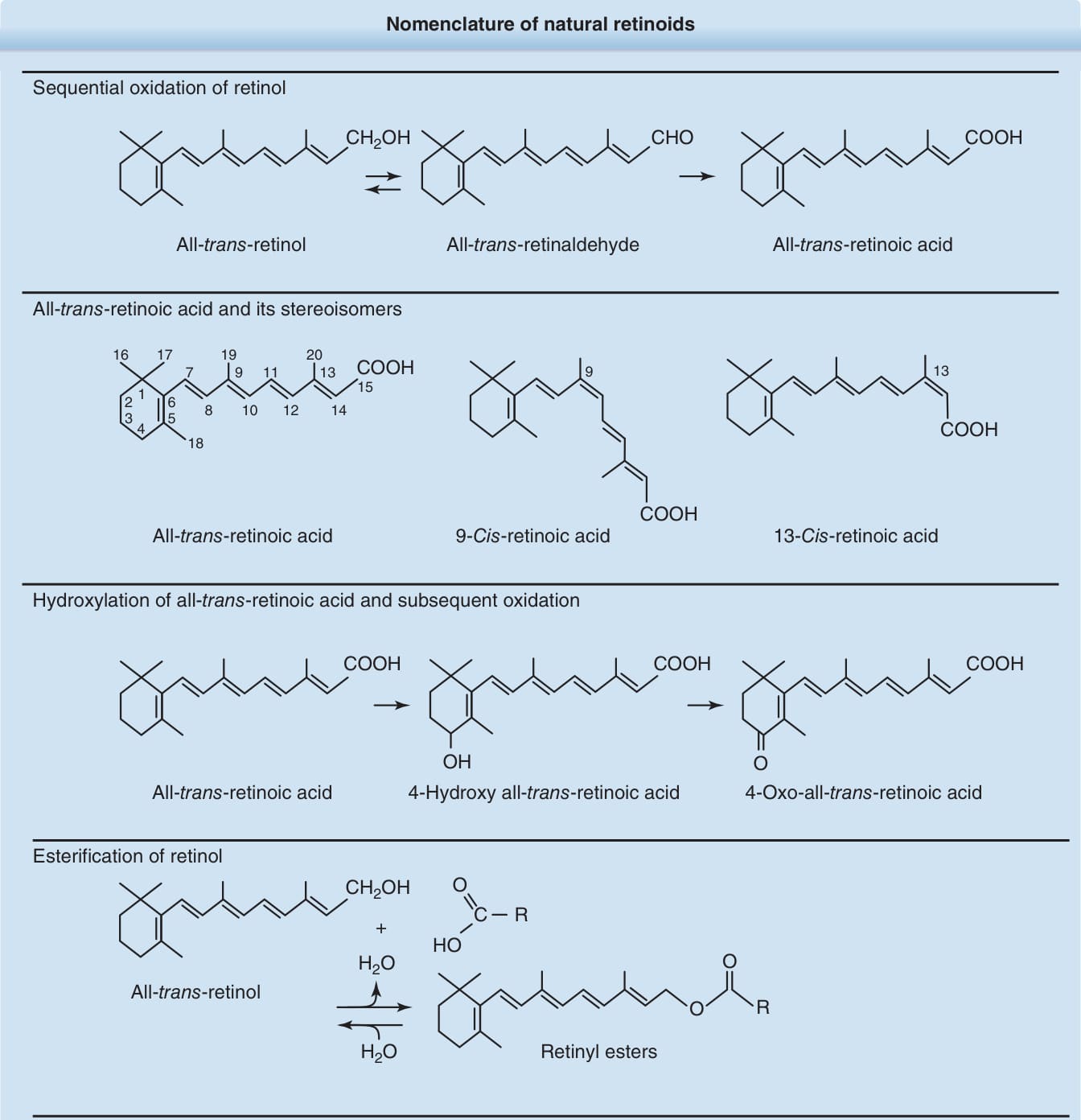
Figure 185-1 Nomenclature of natural retinoids.
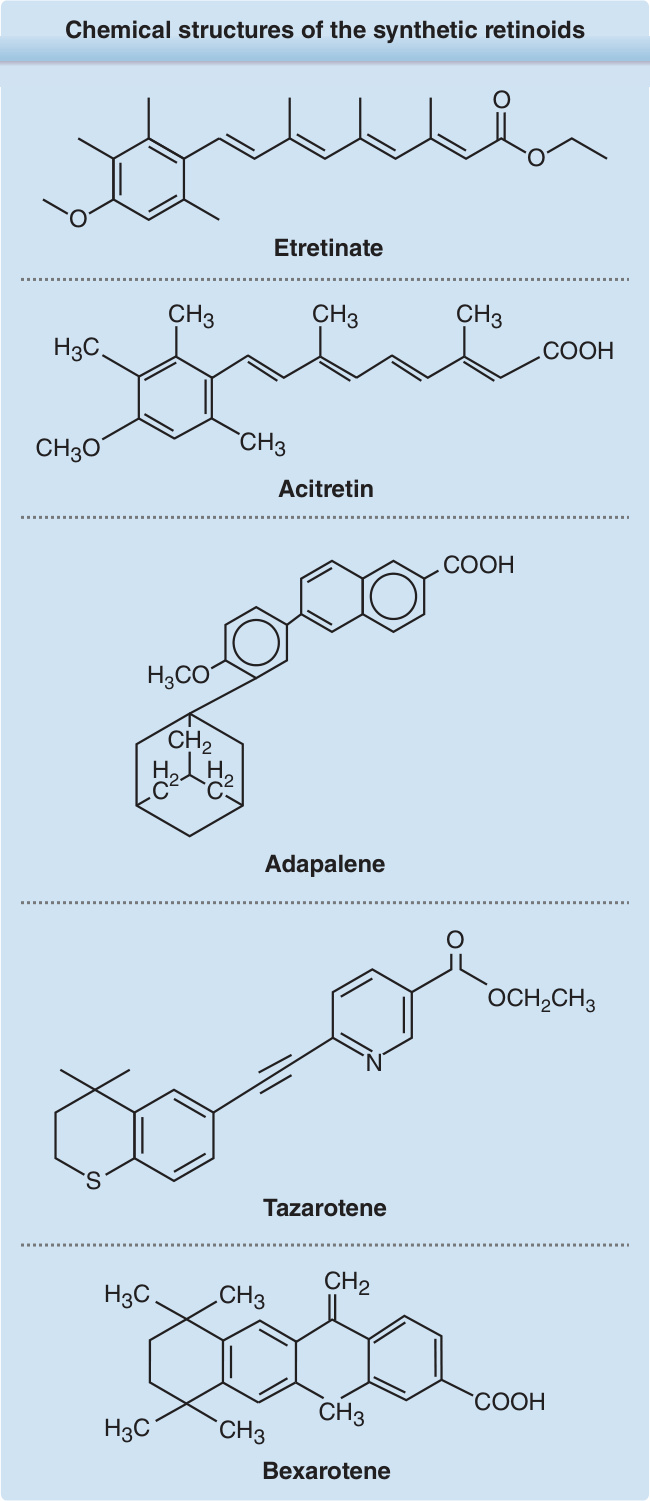
Figure 185-2 Chemical structures of the synthetic retinoids etretinate, acitretin, adapalene, tazarotene, and bexarotene.
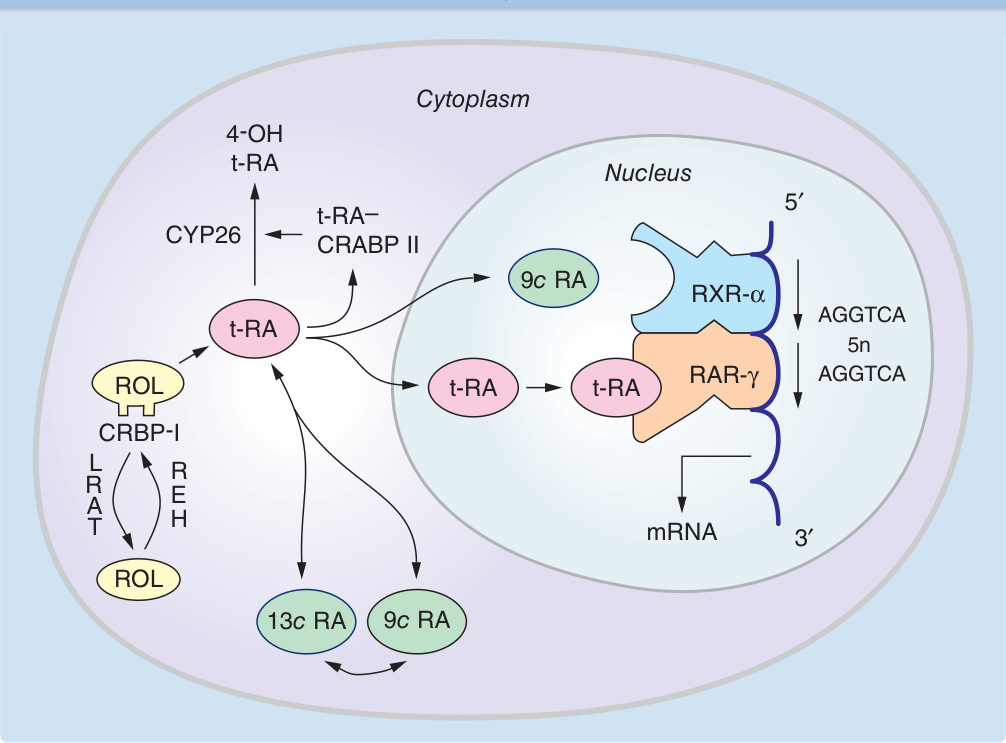
Figure 185-3 Cellular metabolism of natural retinoids and molecular mechanism of retinoid-specific gene activation. Retinol (ROL) delivered to a cell is bound to cellular retinol binding protein-I (CRBP-I). ROL can be esterified, via lecithin:retinol acyltransferase (LRAT), and stored as ROL esters. Hydrolysis of ROL ester by its hydrolase (REH) yields free ROL. Sequential oxidation of ROL generates retinoic acid (RA), which is bound to cellular retinoic acid binding protein (CRABP). All-trans-RA (t-RA) can be isomerized to 9-cis-RA (9c RA). Hydroxylation of t RA by cytochrome-P450 enzyme CYP26 generates 4-OH RA, which is relatively inactive. Retinoic acid receptors (RARs) and retinoid X receptors (RXRs) are intranuclear receptors for retinoids. In human skin, RAR-γ and RXR-α heterodimers bound to RAresponse elements (such as AGGTCA direct repeats) transduce retinoid effects in the presence of RAR ligands. mRNA, messenger RNA.
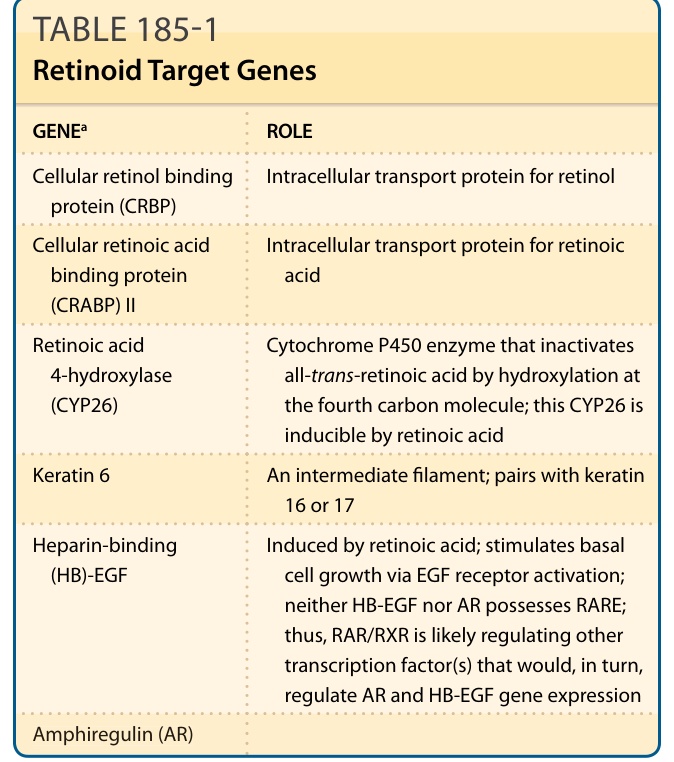
TABLE 185-1 Retinoid Target Genes
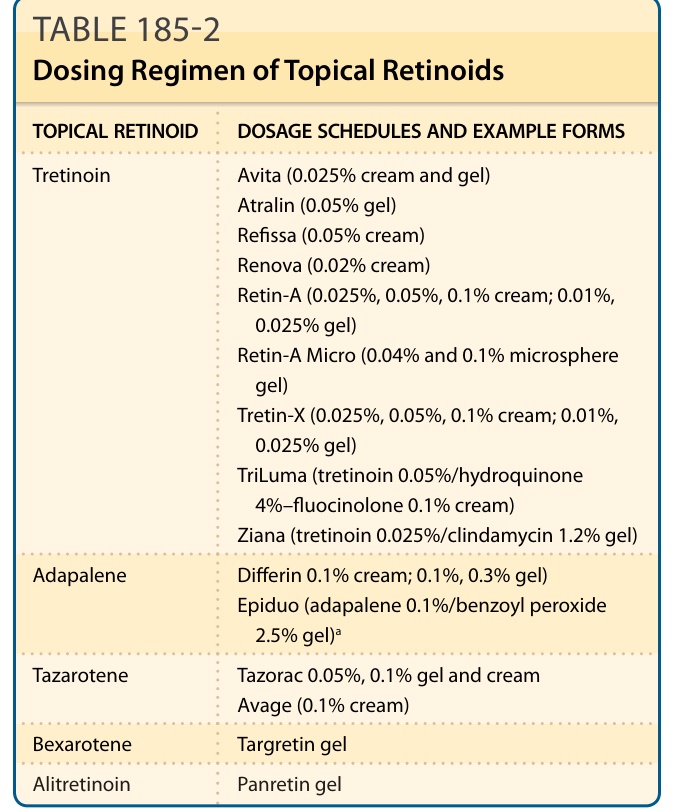
TABLE 185-2 Dosing Regimen of Topical Retinoids
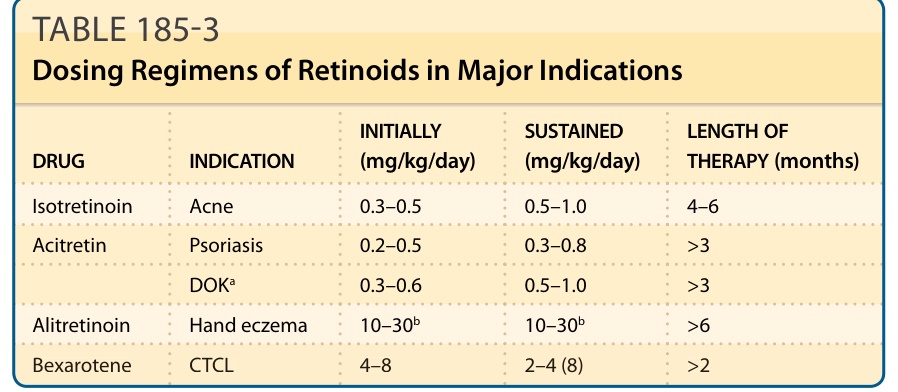
TABLE 185-3 Dosing Regimens of Retinoids in Major Indications
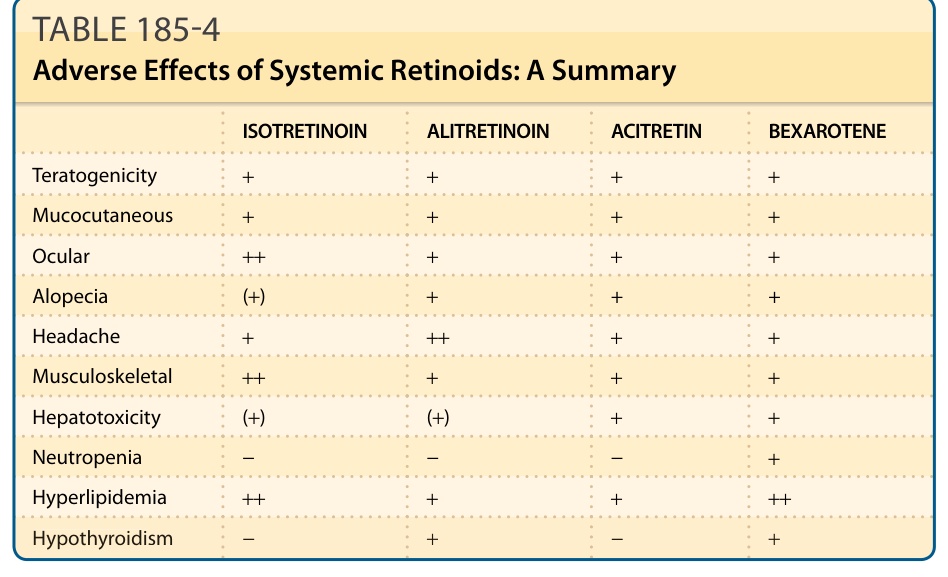
TABLE 185-4 Adverse Effects of Systemic Retinoids: A Summary