Raynaud Phenomenon
22
AT-A-GLANCE
■ Raynaud phenomenon is a vascular disorder characterized by recurrent episodic attacks of digital ischemia provoked by exposure to cold or emotional stress.
■ Affects up to 10% of the population, 4:1 female-tomale ratio.
■ Classified as primary (idiopathic) and secondary (underlying disease or cause present) forms; severity ranges from mild/benign to severe with loss of tissue and risk of amputation.
■ Connective tissue diseases, particularly systemic sclerosis, are among the most common underlying causes of secondary Raynaud phenomenon.
■ Behavioral modification, pharmacologic therapies, and surgical interventions are effective at reducing the frequency and severity of attacks.
Raynaud phenomenon (RP) is a common disorder characterized by recurrent attacks of arterial vasoconstriction resulting in hypoperfusion of the digits and acral tissues. Episodes of RP are triggered by exposure to cold or, less commonly, emotional stress. Classically, RP exhibits a triphasic sequence of color changes of the digits of the hands and/or feet: well-demarcated pallor (corresponding to vasoconstriction and ischemia), followed by cyanosis (venous stasis), and, finally, erythema (compensatory reperfusion) upon rewarming.1
However, not all patients demonstrate this classic triad of color changes. Depending on the presence or absence of an underlying disorder, 2 forms of RP are recognized and usually display divergent disease courses. Primary (idiopathic) RP represents an exaggerated physiologic response to cold or emotional stimuli caused by functional changes in blood vessels and their innervation.2 By definition, primary RP does not result in tissue injury. Secondary RP, which occurs as a result of a systemic disorder or drug exposure, is distinguished by a more aggressive course that can lead to profound tissue ischemia and eventuate in cutaneous ulceration, scarring, or digital gangrene. Management of RP centers on behavioral changes to avoid attacks and on pharmacologic and nonpharmacologic therapies to allay symptoms and reduce morbidity. When present, treatment of the underlying cause remains a critical component of managing secondary disease.
EPIDEMIOLOGY
Precise epidemiologic data on RP are lacking. True estimates are biased by underreporting because many patients with RP never seek medical attention and by the greater attention that has been given to secondary forms of the disease. RP likely affects up to 10% of the general population and 90% of patients with systemic sclerosis (SSc).3-5 Despite study biases, cases of primary RP far outnumber those of secondary disease and comprise up to 90% of all cases.6,7 Symptoms of RP often develop during the second decade of life, and there is a strong female predominance, with an estimated 4:1 female-to-male prevalence ratio. Increases in the frequency and severity of attacks during menstrual cycles suggest that female hormones play a role in the pathogenesis of RP.8 Differences in seasonal skin temperatures, alcohol use, age, smoking status, and marital status between women and men also explain the sex differences observed.9,10 Familial aggregation has been noted in some series, substantiating a role for genetic predisposition.11 Other associations reported in epidemiologic studies include living in a cold climate, certain occupations, cardiovascular disease, low body mass index, and use of vibratory tools.
CLINICAL FEATURES
HISTORY
HISTORY
A clear description of vasospastic attacks is fundamental to the diagnosis of RP. Patients with RP report episodic attacks of white or blue digits induced by cold exposure and, less commonly, by emotional stimuli. Often, only a portion of the digit is affected, and the thumbs are typically spared. Patients rarely volunteer the classic tri-sequence color change, and most only recognize the pallor phase. During attacks, affected digits are numb and, upon rewarming, become bright red and may be accompanied by throbbing pain. If pain is prominent during the ischemic (pallor) phase, a secondary cause is more likely. Other features suggestive of secondary disease are cutaneous ulceration or thumb involvement, as these are rarely seen in primary RP.2 Episodes of RP usually last for 30 minutes, but can persist for hours. Although the fingers and toes are classically affected, attacks may involve the nose, earlobes, or nipples. A careful review of systems is needed to screen for symptoms that point to an underlying disorder as a cause for secondary RP. Arthralgias, dysphagia,
22
muscle weakness, photosensitivity, gastroesophageal reflux, shortness of breath, or sicca symptoms suggest a connective tissue disorder. Claudication indicates atherosclerotic arterial disease. A careful review of medications allows for identification of a potential drug cause. Use of vibratory tools or perpetual hand trauma helps to establish an occupational exposure or hobby as the cause for RP.
CUTANEOUS FINDINGS
CUTANEOUS FINDINGS
Well-demarcated pallor or cyanosis extending from the tip to the more proximal segments of the digits of the fingers or toes typifies the skin changes seen in RP (Fig. 145-1). The skin distal to the line of ischemia is cold and pale, while the proximal skin is often pink and warm. As digits rewarm, blanched skin becomes cyanotic, secondary to low blood flow and deoxygenation, and then transitions to bright red, due to reactive hyperemia. Persistent ischemic discoloration in spite of rewarming suggests secondary disease. Trophic changes of the digits are signs of prolonged attacks of RP and also point to secondary disease. Other skin changes may include atrophy, dystrophic nail changes, and alopecia on the dorsal surfaces of the digits. If present, true sclerodactyly warrants a high degree of suspicion for SSc. In the setting of longstanding RP with repeated bouts of ischemia, digital tapering may occur, which can be challenging to distinguish from sclerodactyly for many clinicians. Ulcerations, which can be extremely painful and punctuated at night, favor the pulp of the finger and the nail unit. Ulcers heal slowly, leaving characteristic small, pitted scars (Fig. 145-2). Ulcers may become infected and can even result in digital osteomyelitis. Although rare, gangrene and autoamputation of distal portions of the digits can occur. Careful inspection of the proximal nailfold, giving attention to the capillaries with the aid of microscopy (or handheld dermoscopy), is a critical part of evaluating the patient with RP. In a large, single institution
2614
study prospectively following 586 patients with RP, the presence of an abnormal nailfold capillary pattern (capillary enlargement and/or capillary loss) at baseline predicted the development of SSc in 151 (25.8%) of patients during a 15-year followup period.12 When accompanied by an SSc-specific autoantibody, abnormal capillaries portended a 60-fold increased risk for progression to SSc among subjects in their cohort. The authors concluded that microvascular damage, which can be assessed by evaluating the proximal nailfold capillaries, is an independent predictor for progression to SSc, highlighting the importance of this examination finding. The presence of hand edema (puffy hands), sclerodactyly, mat telangiectasias, or calcinosis in a patient with RP points to a potential diagnosis of SSc. Other cutaneous findings may imply a specific secondary disorder, for example, purpura, indicating a blood dyscrasia, or jaundice, suggesting viral hepatitis.
OTHER FINDINGS
OTHER FINDINGS
In addition to a careful skin examination, peripheral pulses should be evaluated and blood pressure obtained in both arms. An Allen test also should be performed to assess arterial and capillary function of the hands. In this test, the examiner simultaneously compresses the radial and ulnar arteries, while the patient opens and closes the fist to induce blanching of the palm. Selective arterial filling is judged by the rate of color return as pressure is sequentially released from the radial and ulnar arteries. Abnormal filling implies structural disease of the microcirculation, raising the suspicion for a secondary form of RP or the presence of a thrombus. A positive Allen test should be confirmed with a more definitive diagnostic evaluation such as a Doppler study or angiogram. Vascular obstruction from the thoracic outlet syndrome can be assessed by the Adson maneuver, which tests for diminution of the radial pulse with exaggerated movement of the neck and shoulder. A careful neurologic
examination looking for signs of sympathetic nervous system hyperactivity, abnormal reflexes, or muscular weakness or atrophy can help identify an underlying neurologic disorder.
ASSOCIATIONS
By definition, primary RP develops without an identifiable systemic or drug cause. Several studies have examined the long-term outcome of patients with primary RP.6,12-14 Progression to a secondary form, most commonly a connective tissue disease such as SSc or systemic lupus erythematosus, is as high as 15% during the first decade of onset. Features predictive of progression include nailfold capillary abnormalities, hand edema (puffy hands), positive Allen’s test, and antinuclear antibodies.12,14
22
■β-Adrenergic blockers
■β-Adrenergic blockers
■Ergotamines
■Ergotamines
■Oral contraceptives
■Oral contraceptives
■Methysergide
■Methysergide
■Bleomycin
■Bleomycin
■Vinblastine
■Vinblastine
■Clonidine
■Clonidine
■Bromocriptine
■Bromocriptine
■Cyclosporine
■Cyclosporine
■Amphetamines
■Amphetamines
■Interferon-α and interferon-β
■Interferon-α and interferon-β
■Imatinib
■Imatinib
Secondary RP develops in the context of various disorders and/or drug and toxin exposures (Tables 145-1 and 145-2). CONNECTIVE TISSUE DISEASES
Connective Tissue Disease
■Systemic sclerosis (SSc)
■Systemic lupus erythematosus
■Dermatomyositis and polymyositis
■Mixed connective tissue disease
■Systemic vasculitis
■Sjögren syndrome
Obstructive Arterial Disease
■Atherosclerosis
■Thromboangiitis obliterans (Buerger disease)
■Thromboembolism
■Thoracic outlet syndrome
Neurologic Disorders
■Carpal tunnel syndrome
■Reflex sympathetic dystrophy
■Hemiplegia
■Poliomyelitis
■Multiple sclerosis
■Syringomyelia
Occupation/Environmental Exposure
■Vibration injury (lumberjacks, pneumatic hammer operators)
■Posttraumatic injury (hypothenar hammer syndrome, crutch pressure)
■Vinyl chloride exposure
■Cold injury
Hyperviscosity Disorders
■Cryoproteins (cryoglobulins, cryofibrinogens)
■Cold agglutinins
■Macroglobulins
■Polycythemia
■Thrombocytosis
Miscellaneous
Miscellaneous
■Hypothyroidism
■Hypothyroidism
■Infections (bacterial endocarditis, Lyme disease, viral hepatitis)
■Infections (bacterial endocarditis, Lyme disease, viral hepatitis)
■Malignancy
■Malignancy
■Primary pulmonary hypertension
■Primary pulmonary hypertension
■Arteriovenous fistula
■Arteriovenous fistula
CONNECTIVE TISSUE
DISEASES
The connective tissue diseases are the most common cause of secondary RP. Among patients with SSc, 80% to 90% manifest symptoms of RP. It is the presenting sign in approximately one-third of patients with SSc and may be the only manifestation of the disease for years. Among patients with systemic lupus erythematosus, autoimmune myositis, and systemic vasculitis, RP develops in up to a third. Interestingly, although patients with rheumatoid arthritis often complain of mottled skin changes accompanying cold hands, the incidence of RP appears to be equal to that of the general population.15 Arteriograms of patients with connective tissue diseases often show digital and sometimes ulnar or radial artery obstructions.
NEUROLOGIC DISORDERS
NEUROLOGIC DISORDERS
Any neurologic condition that results in impaired use of a limb may be associated with sympathetic nervous system disturbances and RP. Although distinct from RP, thermoregulatory changes may be a prominent feature of reflex sympathetic dystrophy and can simulate RP.16 Nerve root compression may also cause RP. RP infrequently complicates carpal tunnel syndrome, but if it does develop, the pattern of involvement conforms to the innervation of the median nerve, affecting the first, index, and middle fingers.17,18 RP may also develop from neurovascular compression at the thoracic outlet by cervical ribs, scalene muscles, bony defects of the cervical vertebrae or clavicle, or shoulder compression syndromes.19,20
OCCUPATIONAL FACTORS
OCCUPATIONAL FACTORS
RP is common among individuals with certain occupations. Specifically, individuals who work with
2615
22
vibratory tools, such as air hammers, chainsaws, and rivet guns, and those who experience prolonged exposure to cold temperatures, such as butchers, ice cream workers, and fish packers, are at risk for RP. The prevalence of RP appears to correlate with the vibration level of the tool used, duration of use, and the duration of exposure to cold temperatures.21 Vinyl chloride manufacturing in the polymer industry also confers a risk for developing RP.22
MEDICATIONS AND TOXINS
MEDICATIONS AND TOXINS
A variety of medications can cause or exacerbate RP (see Table 145-2). Mechanistically, drugs may cause peripheral vasoconstriction, endothelial injury, neurotoxicity, or local enhancement of blood viscosity.23
β-Adrenergic blockers, a widely prescribed class of antihypertensives, are the most common cause of iatrogenic RP.24,25 Unopposed peripheral vasoconstriction likely accounts for the development of RP, and specific drugs within the class, for example, propranolol, exhibit a higher propensity to cause disease than do other drugs.25 Other drugs capable of causing RP by vasoconstrictive mechanisms include clonidine, ergot alkaloids (for migraine headaches), dopaminergic agonists, centrally acting stimulants such as methylphenidate and dextroamphetamine, cyclosporine, sympathomimetics (pseudoephedrine, phenylephrine), and cocaine.26-35
Chemotherapies, in particular bleomycin, cisplatin, and vinblastine, are also well-known causes of RP, likely precipitating symptoms by toxin-mediated endothelial dysfunction.36-39 Although the risk of developing RP appears to be commensurate with the cumulative dose of chemotherapy, there are reports of RP after a single injection of bleomycin for the treatment of common warts, supporting the concept that idiosyncratic reactions may also account for some cases.40
RP is a known side effect of treatment with interferon.23,41 Administration of both isotypes of interferon (α and β) can cause severe RP, and some interferon-induced cases have even required surgical amputation because of the ischemic injury sustained.42
The pathophysiology of interferon-induced RP is potentially related to several mechanisms, including a direct vasospastic effect, an increase in blood viscosity, a deposition of immune complexes, and arterial occlusion by thrombi.43-45
Sulfasalazine, propofol, amphotericin B, and, more recently, the tyrosine kinase inhibitors, also have been reported to cause RP.23
In cases of drug-induced RP, discontinuation of the offending medication usually reverses symptoms, but in some instances, the vascular changes are permanent and may require disease-specific interventions. Notably, in patients with preexisting RP, many of these medications can exacerbate disease symptoms. Careful attention to a patient’s medication regimen allows for appropriate substitutions to be made to mitigate disease activity.
2616
MISCELLANEOUS DISORDERS
MISCELLANEOUS
DISORDERS
Patients with hyperviscosity from cryoglobulins, cryofibrinogens, macroglobulins, cold agglutinins, and polycythemia can develop RP. Endocrine disorders, infections, and a variety of malignancies, may also manifest with symptoms of RP.
ETIOLOGY AND PATHOGENESIS
Although the pathogenesis of RP is incompletely understood, it appears that complex interactions between the vasculature, nervous system, and circulating cytokines are responsible for its development.2,46
VASCULAR ABNORMALITIES
VASCULAR ABNORMALITIES
Several studies have demonstrated that endothelialdependent vasodilation is reduced in both primary and SSc-related RP.47-50 Inadequate production of vasodilatory mediators, including nitric oxide and prostacyclin, appears to be critical for this impaired vasodilation.51
In addition, excessive vasoconstriction, partly caused by high circulating levels of endothelin-1 and angiotensin II, contributes to acral hypoperfusion.52,53
Inhibition of the endothelin-1 receptor with bosentan attenuates symptoms of SSc-associated RP, substantiating the pathogenic role of this vasoconstrictor in RP.54,55
These functional blood vessel abnormalities (impaired vasodilation and enhanced vasoconstriction) are present in both forms of RP. Structural derangements of the microvasculature and digital arteries also occur in secondary RP and augment impaired digital perfusion.2,56
Microangiopathy and intimal wall hyperplasia characterize these structural changes and promote ongoing vascular injury, likely accounting for the progressive nature of some cases of secondary RP.
NEURAL ABNORMALITIES
NEURAL ABNORMALITIES
Aberrant signals from the autonomic nervous system, afferent sensory nerves, and the CNS are implicated in the pathogenesis of RP.2 Blood vessels receive innervation from 3 primary sources including sympathetic, parasympathetic, and sensory neurons.46 An imbalance favoring the activation of neurally mediated vasoconstrictive pathways has been demonstrated in RP. Calcitonin gene-related peptide–immunoreactive sensory neurons are reduced in the skin of fingers in patients with SSc-associated RP and primary RP compared to healthy controls, and by altering the neurovascular axis, this deficiency contributes to defective vasodilation.57
Moreover, hyperresponsive α2-adrenoceptors that govern
vasoconstriction in response to cold stimuli have been detected in the digital arteries of individuals with RP.58,59 Central mechanisms may also contribute to RP, as attacks can be elicited by emotional stress. The inability to habituate to episode-provoking stimuli has been cited as a cause for CNS-mediated RP.60,61
INTRAVASCULAR ABNORMALITIES
INTRAVASCULAR
ABNORMALITIES
Platelet activation, increased thrombin generation, defective fibrinolysis, reduced red cell deformability, aberrant white blood cell activation, and increased viscosity collectively constitute the intravascular alterations seen in RP.2 Secondary forms of the disease display a higher likelihood of several of these abnormalities being present simultaneously.62 Oxidative stress imposed on endothelial cells through peroxidation of cell membranes and hypoxia-reperfusion injury, as a result of recurrent ischemic and hyperemic insults, also contribute to SSc-associated RP and, to a lesser extent, to primary RP.2
OTHER MECHANISMS
OTHER MECHANISMS
A variety of other factors likely play a role in the genesis of RP, but are poorly defined. Among those described, hormonal influences from estrogen and genetic predisposition have the strongest data supporting an etiologic association.62 Polymorphisms in genes encoding portions of the neuromuscular acetylcholine receptor and serotonin 1B and serotonin 1E receptors may confer genetic susceptibility to developing primary RP.63
DIAGNOSIS
Primary RP is common, and although a large subset of patients never seek medical attention, many with primary RP do so out of concern for the possibility of an underlying connective tissue disorder.2 Criteria for the diagnosis of primary RP have been developed and validated (Table 145-3).64-66 An expert consensus definition of primary RP has been proposed based on a 3-step algorithm.67 To satisfy a diagnosis of primary RP, patients must have evidence of their fingers having unusual cold sensitivity, experience at least biphasic color changes during vasospastic episodes (white and blue), and have a minimum of 3 of the following features present: attacks triggered by stimuli other than cold (eg, emotional stress); involvement of both hands, even if asymmetric; attacks accompanied by numbness or paresthesias; color changes characterized by a welldemarcated border between affected and unaffected skin; photographs that strongly support a diagnosis of RP; episodes occurring at other body sites (eg, nose, ears, feet, and nipples); and triphasic color changes (white, blue, red).
22
■Vasospastic attacks precipitated by exposure to cold or emotional stimuli
■Vasospastic attacks precipitated by exposure to cold or emotional
stimuli
■Bilateral involvement of extremities
■Bilateral involvement of extremities
■Normal vascular examination with symmetric peripheral pulses and normal nailfold capillary microscopy
■Normal vascular examination with symmetric peripheral pulses and
normal nailfold capillary microscopy
■Absence of gangrene or, if present, limited to the skin of the fingertips
■Absence of gangrene or, if present, limited to the skin of the
fingertips
■No evidence of an underlying disease, drug, or occupational exposure that could be responsible for vasospastic attacks
■No evidence of an underlying disease, drug, or occupational expo-
sure that could be responsible for vasospastic attacks
■Negative antinuclear antibody test
■Negative antinuclear antibody test
■Normal erythrocyte sedimentation rate
■Normal erythrocyte sedimentation rate
■History of symptoms for at least 2 years
■History of symptoms for at least 2 years
Combined criteria of Allen and Brown64 and Le Roy and Medsger.65
In addition to classic symptoms, the diagnosis of secondary RP requires the simultaneous identification of a systemic disorder, medication, or toxin exposure known to cause the disease. Secondary RP is more likely in the following settings: an age at onset of 30 years or older; episodes that are intense, painful, asymmetric, or associated with ischemic skin lesions; clinical signs suggestive of a connective tissue disease, such as arthritis or abnormal lung function; specific autoantibodies; and evidence of microvascular disease seen on nailfold microscopy, particularly capillary dropout and giant capillary loops.68-70
LABORATORY STUDIES
LABORATORY STUDIES
In all patients with RP, a complete blood count, erythrocyte sedimentation rate, urinalysis, and antinuclear antibody testing should be obtained.68 In patients with abnormal antinuclear antibody titers, testing for antibodies to specific nuclear antigens, for example, centromere or topoisomerase, are helpful to identify specific connective tissue diseases such as SSc. Notably, a positive antinuclear antibody without antigen specificity carries a lower risk of a concomitant connective tissue disorder, as compared to antigen-specific autoantibodies.13,71,72
Additional laboratory studies may be warranted based on findings from the history and physical examination and include a comprehensive chemistry panel; thyroid function tests; measurement of C3 and C4 complement levels; serum protein electrophoresis and immunofixation electrophoresis; testing for rheumatoid factor; and evaluation for cryoglobulins. A chest radiograph may detect a cervical rib in patients with symptoms of thoracic outlet obstruction. If proximal large vessel disease is suspected, for example in the case of unilateral RP or when peripheral pulses are difficult to palpate, arterial Doppler investigations are necessary.2 Abnormal Doppler studies require further evaluation with appropriate imaging and/or referral to a vascular specialist.
2617
22
A
C
B
D
SPECIAL TESTING
SPECIAL TESTING
Nailfold capillaroscopy is a helpful adjunctive tool to predict progression to SSc. Whereas normal nailfolds consisting of uniformly sized capillaries with regular spacing are reassuring and are present in the majority of cases of primary RP, capillary dilation (giant capillaries) with focal hemorrhage and areas of avascularity (capillary dropout) are highly specific for and can predict transition to SSc (Fig. 145-3).2,70,73
In SSc-associated RP, serial nailfold capillary microscopy examinations show progressive decreases in the total number of nailfold capillary loops, and end-stage changes, which include haphazardly arranged vessels (telangiectasia) and near total loss of capillaries, correlate with advanced sclerodactyly.74 These dynamic nailfold changes are not observed in primary RP. Thermal imaging (thermography) is a newer diagnostic technique that measures digital and acral surface temperatures and may be able to distinguish between patients with primary RP and those with SSc.75 By determining the temperature differences between distal fingertips and the dorsal hand (“distal–dorsal difference”), parameters derived from thermography appear to reliably predict whether a structural vascular defect (eg, related to SSc) is present. Thermography awaits further validation, and its usefulness is limited by its cost and availability. Other techniques that have been used to diagnose RP include laser Doppler imaging, plethysmography,
2618
and finger systolic pressure measurements.76-78 As of this writing, such tests are not routinely used in clinical practice, but may ultimately provide practical, noninvasive methods to assist in the diagnosis of RP.
DIFFERENTIAL DIAGNOSIS
The major forms of vascular disease that must be distinguished from RP are physiologic cold fingers, acrocyanosis, pernio, erythromelalgia, livedo reticularis, and reflex sympathetic dystrophy (Table 145-4). Many patients experience cold, sometimes painful digits without a color change in response to cold temperature exposure. This condition is physiologic and, although pronounced in some individuals, represents normal sympathetic nervous system activity. This type of response to cold exposure is not synonymous with RP.
■Physiologic response to cold temperature
■Physiologic response to cold temperature
■Acrocyanosis
■Acrocyanosis
■Pernio
■Pernio
■Erythromelalgia
■Erythromelalgia
■Livedo reticularis
■Livedo reticularis
■Reflex sympathetic dystrophy
■Reflex sympathetic dystrophy
Acrocyanosis is a functional vascular condition characterized by blue-violet discoloration of acral skin as a result of diminished oxyhemoglobin.79,80 Defects in central oxygenation, as seen in cardiac and pulmonary diseases, or local hypoxia are responsible for the manifestations of the disorder. Acrocyanosis is much less common than RP, and by definition, the color changes seen in acrocyanosis are persistent, irrespective of exposure to cold temperature or other stimuli. Triphasic color changes are not seen in acrocyanosis. Pernio is an acral, inflammatory dermatosis that develops in response to exposure to cold, wet conditions. Lesions of pernio appear as erythematous to violaceous macules, papules, or plaques that symmetrically involve the toes and/or fingers. Rarely, the heels, thighs, nose, and ears may be affected. Hemorrhagic lesions, bullae, loss of the nails, and ulcerations may complicate severe cases. If ulcerations develop, secondary infections may supervene. Pain, pruritus, and a burning sensation may accompany lesions of pernio. The disorder is typically benign and selflimiting, and lesions last approximately 1 to 3 weeks. Uncomplicated cases of pernio do not require treatment, but when present in patients with concomitant connective tissue disease, it may be more challenging to manage and necessitate disease-specific therapy. Erythromelalgia is a rare, functional vascular disease characterized by pain, burning, edema, and erythema, most often of the extremities. Unlike RP, affected limbs are characteristically warm. Exercise, standing, walking, limb dependency, and warm exposure trigger episodes of erythromelalgia. Attacks of erythromelalgia tend to occur in the evening and at night, and can disrupt sleep. The feet are affected in 90% of patients, whereas the hands are involved in only 25%.81 Rarely, the face and the ears may be involved. Because of the extreme warmth and burning pain experienced, patients seek various ways to cool the affected area, and often find relief with limb elevation or immersion in ice water. Immersion in ice water causes reactive vasoconstriction that may lead to skin breakdown and cold water tissue injury, eventuating in infection and, rarely, autoamputation. Erythromelalgia may be primary, or may occur as a result of a systemic disorder. Although the etiology and pathogenesis of erythromelalgia are poorly understood, it is thought to relate to abnormalities of platelet function, changes in vascular dynamics, and dysfunction of voltage-gated sodium channels.82,83 Cases of coexisting erythromelalgia and RP have been described, and some investigators view the 2 disorders as existing on a spectrum, with RP representing the excessive vasoconstrictive form and erythromelalgia representing the exaggerated vasodilatory form.82
Livedo reticularis is a very common skin change resulting from a localized physiologic response to cold exposure and appears as a mottled, well-formed reticulated (net-like) vascular pattern that blanches with pressure. Although any body site may be affected, lesions preferentially occur on the limbs, particularly the lower extremities. Livedo reticularis develops from alterations in blood flow through the cutaneous
22
microvasculature.84 It may be a primary physiologic response or, less commonly, associated with an underlying condition, especially disorders that alter blood viscosity or cause intraluminal vascular obstruction. Reflex sympathetic dystrophy is a rare, painful disorder accompanied by vasomotor instability that results from autonomic nervous system dysfunction.85
Most cases arise after injury to a limb. Consequently, changes seen in reflex sympathetic dystrophy favor the upper and lower extremities, as well as the hands. Complex alterations in nociceptive nerve terminals amplify pain signals from the CNS and are thought to cause the disorder. Reflex sympathetic dystrophy characteristically progresses through various stages that ultimately result in soft-tissue destruction.85 The second stage of disease, which is characterized by pain and vasomotor instability, develops months after nerve injury has occurred and may resemble RP. Distinguishing features include disproportionate levels of pain, hypotrichosis or hypertrichosis, nail changes, hyperhidrosis or anhidrosis, and, in advanced stages, soft-tissue atrophy.
CLINICAL COURSE AND PROGNOSIS
The clinical course of RP is largely dictated by whether the disorder is primary or secondary. The vast majority of cases of primary RP exhibit an indolent course. Simple behavioral modifications alone usually suffice to control the disease. Complications such as digital ulceration, soft-tissue atrophy, and bone loss rarely occur in primary RP. In contrast, secondary RP has a more guarded prognosis. In secondary disease, repeated bouts of prolonged digital ischemia result in skin breakdown, soft-tissue injury, ulceration, and, occasionally, autoamputation. These complications are more frequent in inadequately treated patients. Digital pulp cellulitis (felon) and osteomyelitis may also complicate secondary RP, especially after the development of cutaneous ulceration. Raynaud crisis is a rapidly progressive form of RP that is characterized by acute, potentially catastrophic tissue ischemia and is considered a medical emergency. Without intervention, Raynaud crisis results in digital infarction and may lead to digit loss. Patients with secondary RP should be alerted to the possibility of developing this rare complication, which is heralded by extreme pain and persistent white-blue color changes in a digit that will not rewarm. Susceptibility to Raynaud crisis is highest among patients with SSc with coexisting macrovascular disease and positive anti-centromere antibodies.86
RP can have a profound impact on a patient’s quality of life. When controlling for severe pulmonary and GI disease in a study examining RP activity in SSc patients, patient-reported health assessment questionnaire pain and disability scores, as well as visual analog scale severity scores were greater for RP and
2619
22
digital ulcers compared to breathing and intestinal complaints, indicating a more substantial impact on quality of life.87 High levels of depressed mood and feelings of anxiety related to attacks of RP were also found in the study’s cohort. The development of digital ulcers is a poor prognostic sign. Apart from morbidity directly related to digital ulcers, higher incidences of disability, pain, and limited hand function accompany this complication.87
A validated, reliable measure of RP activity, the Raynaud Condition Score (RCS), has been developed.87 The score represents a global composite of objective metrics (number of attacks per day, length of each attack) and a subjective, patient-reported severity score. The severity score component is administered on either a visual analog scale (0 to 100) or an 11-point Likert scale, averaged over a 1- or 2-week period. While primarily used to assess response to therapy in clinical trials, implementation of the RCS as a practice tool has gained popularity, allowing clinicians to assign a severity score to patients in order to gauge suitability for an intervention and to objectively follow their outcome. The RCS and other RP measures, including the health assessment questionnaire’s pain and disability scale and mood scales, are highly sensitive to changes in RP activity and can discriminate between subjects with and without digital ulcers.87 Recently, the minimally important difference, representing the smallest improvement in a score that patients perceive as beneficial, and the Patient Acceptable Symptom State, defined as the absolute value beyond which patients consider themselves well, have been established for the RCS.88 These estimates, a 14- to 15-point improvement (0 to 100, visual analog scale) and a score of 34 points or less for the minimally important difference and Patient Acceptable Symptom State, respectively, will assist with objectively evaluating the success of treatments for RP using meaningful end points in future clinical trials.
MANAGEMENT
The management of RP centers on attenuating the frequency, severity, and duration of attacks as well as treating ischemia-related complications. These goals can be achieved through the implementation of behavioral modification, pharmacologic therapies, and procedural interventions. In some cases, a combination approach is necessary. When causes of secondary RP are identified, treatment of the underlying disorder may result in improvement of RP. When a drug or occupational exposure is suspected, cessation of the culprit medication or removing the patient from the causal environment is necessary.
BEHAVIORAL MODIFICATION
BEHAVIORAL
MODIFICATION
2620
-
Dress warmly and layer clothing
-
Maintain higher-than-normal thermostat settings indoors
-
Limit time spent outdoors during winter
-
Use hand or foot warmers
-
Recognize and terminate attacks early
-
Smoking cessation and/or avoidance of secondhand smoke
-
Limit caffeine consumption
-
Dress warmly and layer clothing
-
Maintain higher-than-normal thermostat settings indoors
-
Limit time spent outdoors during winter
-
Use hand or foot warmers
-
Recognize and terminate attacks early
-
Smoking cessation and/or avoidance of secondhand smoke
-
Limit caffeine consumption
with layered clothing and maintaining a higher-thannormal thermostat setting while indoors are easy habits for patients to implement. Limiting time spent outdoors during the winter, wearing insulated mittens or gloves and thick socks, and using hand or foot warmers, are also helpful. Patients should be taught to recognize and terminate attacks of RP promptly by returning to a warmer environment and applying heat to affected digits if symptoms persist after acclimating. In addition, counseling to maintain a warm core temperature (including wearing hats and additional layers centrally) should be reinforced at each patient encounter. This measure prevents the reflexive, peripheral vasoconstriction that accompanies a drop in core temperature, as blood shunts centrally to rewarm the body. Smoking cessation in smokers with RP and counseling to avoid secondhand smoke in nonsmokers should be emphasized because nicotine induces cutaneous vasoconstriction and can provoke attacks of RP. Caffeine has mixed vasoactive properties, but one of its major downstream effects is to enhance vasoconstriction by blocking adenosine receptors. Consequently, limiting caffeine consumption should also be considered in caffeine-sensitive patients. Stress modification is important to minimize vasoconstriction in those with hyperactivity of the sympathetic nervous system. Counseling, training in relaxation, biofeedback techniques, and, in anxiety-provoked cases, anxiolytics may be beneficial.
PHARMACOLOGIC INTERVENTIONS
PHARMACOLOGIC
INTERVENTIONS
VASODILATORS
Calcium channel blockers (CCBs) are the preferred first-line therapy for both primary and SSc-associated RP in patients who do not respond to behavioral modification alone.89-91 The dihydropyridine class of CCBs (nifedipine, amlodipine, nicardipine, and felodipine) are the least cardioselective and appear to be the most efficacious in terms of reducing the frequency and severity of attacks of RP.46 Their beneficial effect
CLASS DRUGS DOSE & ADMINISTRATION
Vasodilators
Nifedipine 30 to 89 mg by mouth each evening
Amlodipine 5 to 20 mg by mouth every day
Diltiazem 30 to 120 mg by mouth thrice daily
Tadalafil 20 mg by mouth every day
Sildenafil 20 mg by mouth thrice daily
L-Arginine 2 to 8 g by mouth every day
Inhibitors of vasoconstriction
Losartan 25 to 100 mg by mouth every day
Enalapril 5 to 20 mg by mouth twice daily
Quinapril 20 to 80 mg by mouth every day
Fluoxetine 20 to 40 mg by mouth every day
Bosentan 62.5 mg by mouth twice daily × 2 weeks, then increase to 125 mg by mouth twice daily
Prazosin 1 to 5 mg by mouth twice daily
Other medications
Aspirin 150 to 325 mg by mouth every day
Pentoxifylline 400 to 800 mg by mouth thrice daily
Infusionsa Sodium
0.3 to 10 mcg/kg/min
Sodium nitroprusside 0.3 to 10 mcg/kg/min
Infusionsa
nitroprusside
Iloprost 0.5 to 2 ng/kg/min
Iloprost 0.5 to 2 ng/kg/min
Alprostadil 6 to 10 ng/kg/min
Alprostadil 6 to 10 ng/kg/min
aTypically reserved for Raynaud crisis.
has been confirmed in several randomized, blinded, placebo-controlled trials. Diltiazem, a nondihydropyridine CCB, also reduces vasospastic episodes in both primary and secondary RP.92 A metaanalysis of 18 trials evaluating CCBs as a primary intervention for RP demonstrated an average decrease of 2.8 to 5 attacks and a 33% reduction of symptom severity during a 1-week period.89 Adverse side effects from CCBs occur in up to 15% of users and include headache, flushing, hypotension, and lower-extremity edema.93 Side effects can be dose-dependent or idiosyncratic. In SSc patients with esophageal dysmotility, CCBs can also exacerbate gastroesophageal reflux symptoms.46,94 Commencing treatment with a low dose followed by a gradual escalation until the desired response is achieved is the most effective approach. Furthermore, selection of a once-daily, sustained-release preparation is preferable
22
to shorter-acting formulations and encourages patient compliance. In addition, when the sustained-release dose is given nightly, CCBs are better tolerated, even in patients with low baseline blood pressures. Studies implicating the pathogenic deficiency of nitric oxide in RP have led to an interest in strategies that increase tissue levels of nitric oxide as a therapeutic approach. Nitric oxide stimulates smooth muscle relaxation by increasing intracellular concentrations of cyclic guanosine monophosphate, and results in vasodilation and increased digital perfusion. Initial studies exploiting this pathway showed promise, as topical nitrates attenuated symptom severity and improved digital ulcer healing times in patients with connective tissue disease–associated RP in a randomized, placebocontrolled trial.95 Subsequent studies have validated the efficacy of other nitric oxide substitutes such as l-arginine and sodium nitroprusside.96 Although promising, difficulty associated with their administration (eg, sodium nitroprusside requires intravenous infusion) and the limited availability of some these agents has hindered their routine use in clinical practice. More recently, the phosphodiesterase (PDE) inhibitors have emerged as a promising class of medications for managing patients with CCB-refractory RP. These vasodilators exert their biologic effects by enhancing nitric oxide signaling via inhibition of cyclic guanosine monophosphate degradation, resulting in improved tissue perfusion. In a double-blind, randomized, placebocontrolled trial examining the effect of the PDE inhibitor tadalafil in individuals with CCB-refractory RP, those receiving tadalafil had significant improvements in multiple outcome measures including frequency and duration of RP attacks, RCS, digital ulcer healing time, prevention of digital ulcers, physician and patient global assessments, health assessment questionnaire disability and pain scales, and several quality-of-life domains at the end of a 6-week period.97 Similar results have been published for sildenafil, a shorter-acting PDE inhibitor, with a comparable safety and tolerability profile.98 PDE inhibitors are usually well tolerated, but occasional side effects include headache, dyspepsia, dizziness, and, rarely, visual disturbances. Interestingly, not every placebo-controlled trial evaluating the utility of PDE inhibitors for secondary RP has demonstrated benefit.99,100 The issue of reproducibility among these null trials has been ascribed to insufficient powering, as many trials used small sample sizes and each showed trends favoring PDE inhibitor over placebo. A recent metaanalysis examining the data across all studies has substantiated the efficacy of PDE inhibitors for treating secondary RP.101 In the authors’ experience, the addition of sildenafil to a CCB-based therapeutic regimen has typically resulted in disease improvement, including the amelioration of digital ulcers. Prostaglandins and their analogs possess potent vasodilatory properties and have been used successfully to treat both primary and SSc-associated RP. As of this writing, iloprost, a chemically stable synthetic prostacyclin analog that dilates the peripheral vasculature and inhibits platelet adhesion and aggregation, has been the most rigorously studied. Intravenous administration of
2621
22
iloprost attenuates the severity and number of attacks of RP and leads to more rapid digital ulcer healing time in patients with SSc-associated RP.102,103 In some trials, the effects of iloprost were sustained and led to a decreased requirement for ongoing therapies. In fact, in a 12-month prospective, parallel-group trial assessing the outcomes of subjects with SSc-associated RP assigned to receive either iloprost infusions at 6-week intervals or conventional vasodilator therapy, individuals in the iloprost intervention arm had significant reductions in RP severity scores and required fewer ancillary therapies.104 Additional end points of significance favoring the iloprost treatment group, while controlling for immunomodulatory therapy, included improvement in modified Rodnan skin scores and diffusion capacity for carbon monoxide, reflecting reduced cutaneous sclerosis and enhanced pulmonary function, respectively. As a result of their findings, the authors concluded that iloprost might act as a disease-modifying agent in SSc-associated RP. Owing to the expense and occasional hypersensitivity associated with intravenous administration, an oral formulation of iloprost has been developed. A single randomized, placebo-controlled trial confirmed the efficacy of oral iloprost for RP,105 but this finding was not replicated in a larger, multicenter study.106 Consequently, intravenous, but not oral, iloprost is recommended for the management of refractory RP in the setting of SSc.107
INHIBITORS OF VASOCONSTRICTION
Angiotensin-converting enzyme inhibitors and angiotensin II receptor antagonists have been investigated for treating RP. Both act on the renin–angiotensin system and impede vasoconstriction by reducing the downstream activity of angiotensin. Despite mixed results with enalapril108,109 and quinapril,110 a greater treatment response using once-daily losartan was observed when compared to nifedipine in a parallel-group trial over a 12-week period in participants with both primary and secondary RP.111 This data supports the use of direct angiotensin receptor inhibitors over indirect inhibitors (angiotensin-converting enzyme inhibitors) for managing RP, although both are effective. In select circumstances, for example, scleroderma renal crisis, angiotensin-converting enzyme inhibitors may be the preferred option. Several studies have implicated serotonin as an important mediator in the development of RP.112,113
An in vivo human experiment infusing serotonin into the brachial artery reproduced the characteristic color changes seen in RP, confirming that serotonin is a potent vasoconstrictor in the peripheral circulation under physiologic circumstances.114 In the periphery, selective serotonin reuptake inhibitors (SSRIs) block serotonin uptake by platelets, which decreases arterial vasoconstriction. Centrally, serotonin acts as a vasodilator, and by increasing the availability of serotonin in the CNS, SSRIs facilitate centrally mediated peripheral vasodilation. The results of 1 randomized, controlled trial demonstrated that the SSRI fluoxetine was more
2622
efficacious than nifedipine in terminating attacks and decreasing the severity of RP over a 6-week period.115
SSRIs may, therefore, represent a rational choice in patients who have not adequately responded to CCBs. Given their anxiolytic properties, SSRIs may be especially desirable in patients with anxiety and RP triggered by emotional stimuli. As previously mentioned, endothelin-1 contributes to the pathogenesis of RP by inducing vasoconstriction. Bosentan, an oral endothelin receptor antagonist, has demonstrated efficacy for treating SSc-associated RP.55 Apart from improving symptoms of RP, bosentan decreased ulcer healing time and prevented the formation of new ulcers in 2 similar cohorts of patients with SSc-associated digital ulcers.116,117 Dose-dependent elevation of hepatic transaminases is seen during treatment with bosentan in up to 10% of individuals, and rare occurrences of cirrhosis and fulminant liver failure have been reported with its use. Although prescribers should exercise caution prior to choosing this agent, in carefully selected circumstances, bosentan may prove to be an indispensable option, particularly in the setting of refractory digital ulcers. α-Adrenergic blockers, in particular the α1- adrenoceptor inhibitor prazosin, can also effectively treat RP. In a Cochrane database review, investigators found high-quality evidence from 2 randomized, controlled trials that demonstrated a beneficial effect of prazosin over placebo in patients with SSc-associated RP.118 Side effects, including postural hypotension, drowsiness, and fatigue, were common among treatment participants, but were mild overall and could be avoided by nighttime administration.119 A recent Phase II, randomized, placebo-controlled trial investigating the effect of a novel, high-potency α2-adrenoceptor antagonist in subjects with SSc-associated RP showed no benefit over placebo in terms of recovery from a cold challenge test.120 For unclear reasons, it appears that selective blockade of α1-adrenergic but not α2-adrenergic receptors is an effective treatment strategy for RP. Recent advancements in our understanding of coldinduced vasoconstriction have identified the Rho family of kinases as putative targets for RP. Cold exposure initiates a cascade of events involving the activation of the sympathetic nervous system and release of norepinephrine, ultimately resulting in cutaneous vasoconstriction. Norepinephrine stimulates vascular smooth muscle cells to contract, and this latter process is controlled in part by activation of the Rho kinase pathway.121 Rho kinases play a central role in regulating actin-dependent and myosin-dependent vasoconstriction,122 which created interest in exploiting this pathway as a mechanismbased approach to treating RP. Unfortunately, results from a randomized, placebo-controlled trial using the Rho kinase inhibitor fasudil failed to show benefit in terms of skin temperature recovery time and digital blood flow following a cold challenge in individuals with SSc-associated RP.123 The trial’s investigators attributed the study design and selection of participants with advanced disease as possible explanations for its failure. Future studies will seek to address whether Rho kinase inhibition is relevant for treating RP.
OTHER MEDICATIONS
Aspirin and other antiplatelet therapies are routinely used in RP, despite a paucity of data to support their use. These agents likely exert benefit by reducing local thrombosis and platelet-mediated vasoconstriction, the latter of which results from the release of vasoactive mediators by platelets. Occasionally, aspirin therapy can worsen RP. This phenomenon may be explained by its effect on reducing the production of vasodilatory prostaglandins.46
Agents that alter blood viscosity and the hemorrheologic dynamics of red cells, such as pentoxifylline, also have been used to treat RP.124,125 These are preferable in select settings, such as in cases of cryoprecipitable disorders or Waldenström macroglobulinemia in which vascular sludging contributes to the development of RP, or in individuals with a baseline low blood pressure who are intolerant of CCBs. Pentoxifylline also can be added to an existing drug regimen to enhance therapeutic efficacy. Anticoagulants and thrombolytic agents are most useful when treating RP secondary to an embolus or vasoocclusive event. In Raynaud crisis, heparin may be indicated during the acute phase of ischemia to prevent irreversible tissue injury. A pilot study showed benefit from adding low-molecular-weight heparin to a conventional RP treatment protocol in a cohort of patients with primary and secondary RP, the effect of which was maximal by 20 weeks of daily use.126 When considering heparin for RP, the risk of serious bleeding must be balanced against any potential benefit it may confer. Anticoagulation with warfarin is not routinely recommended to treat RP. Notable exceptions include cases in which a thrombotic diathesis exists, or in cases of SSc in which warfarin is specifically selected to treat associated calcinosis cutis.127
As oxidative stress likely contributes to RP, there is ongoing interest in using antioxidants to placate the symptoms and sequelae of the disorder. Intravenous N-acetylcysteine significantly reduced the frequency and severity of RP attacks as well as the number of digital ulcers in a cohort of 20 patients with SSc.128 The therapy was well tolerated, and no substantial side effects were observed. Other studies have also supported the role of antioxidant therapy for RP.129 The benefits of antioxidants are potentially greatest when used early in the course of disease.46
Several complementary and alternative medicines have been used for RP with no demonstrable benefit as of this writing.130
PROCEDURAL INTERVENTIONS
PROCEDURAL
INTERVENTIONS
BOTULINUM NEUROTOXIN
Interest in botulinum neurotoxin (BoNT) as a treatment of RP emerged after a series of ex vivo experiments demonstrated a blunting effect on arterial
22
contraction following incubation with modest concentrations of BoNT.131 A seminal clinical report followed, in which 2 patients with severe, multidrug-resistant RP were given local injections of BoNT and subsequently experienced substantial improvements in both patient-reported disease activity and digital perfusion, as measured by laser Doppler interferometry.132
A larger, prospective study comprised of 11 patients with pharmacologically refractory RP secondary to connective tissue disease supported these findings.133
According to the study results, after digital injections with BoNT, each subject achieved clinically meaningful improvement in RP-associated pain, 9 of the 11 reported decreased severity and frequency of vasospastic episodes, and previously nonhealing ulcers spontaneously healed following therapy in 9 subjects. Benefit was observed as early as 24 hours after injection, and all subjects experienced pain relief within 48 hours. Numerous subsequent studies, including 1 placebo-controlled trial, have further validated BoNT as an effective option for RP, particularly in the setting of multiple medication failures.134,135 Complications related to BoNT injections include dysesthesia and transient hand weakness, but the rate is acceptably low. The effect of BoNT usually lasts for months, but some reports have indicated ongoing benefit for up to a year. Mechanistically, BoNT decreases muscle tone by preventing the presynaptic release of acetylcholine at the neuromuscular endplate. This results in paralysis of both striated and smooth muscle, including the musculature encasing blood vessels.136 Chemodenervation with BoNT therefore enhances digital perfusion via toxin-mediated vasodilation. In addition to its direct effect on muscle, BoNT blocks the recruitment of α2-adrenoceptors and decreases C-fiber nociceptor density, which raises the threshold of smooth muscle reactivity to cold stimuli and attenuates pain, respectively.131,137
A standardized technique for injecting BoNT has been reported and is easy to perform because it uses reliable anatomic landmarks.138 At the metacarpophalangeal flexion crease, 5 to 10 units of onabotulinumtoxinA (BoNT type A) are injected while aiming proximally toward the neurovascular plexus. Approximately 40 to 100 units of onabotulinumtoxinA are used per hand, and in most instances, injection of the thumb is unnecessary. In some highly responsive individuals, pain relief is felt almost instantaneously. Use of a topical anesthetic under occlusion prior to injections makes the procedure more tolerable. In the authors’ experience, use of BoNT as an adjunctive therapy for RP has resulted in notable improvements in patient and physician global assessments, particularly among those who have failed multiple medical interventions.
SYMPATHECTOMY
In rare instances, aggressive medical therapies are insufficient to adequately control RP. In such scenarios,
2623
22
surgical intervention may be warranted. The most commonly performed surgery is a sympathectomy, which serves to permanently sever vasoconstrictive signals from the sympathetic nervous system innervating the hands. As of this writing, 2 techniques, either a thoracocervical or a digital approach, are used and appear to be comparable in terms of benefit. Thoracocervical sympathectomy is the traditional approach for RP and can be performed in either an open fashion or using an endoscopic technique. The goal of the procedure is to transect postganglionic fibers that exit via the thoracic sympathetic chain and fuse with the cervical stellate ganglion to innervate the hand. Outcomes data are mixed. Although early reports documented poor long-term outcomes with high rates of symptom recurrence and postoperative complications,139 advances in surgical techniques have yielded better results. A review collating the most recent outcomes data indicated that shortterm improvement after thoracic sympathectomy was achieved in 92% and 89% of patients with primary and secondary RP, respectively.140 Healing of refractory digital ulcers following the procedure was also high, with 98% of patients deriving benefit, the majority of which had complete resolution. Data from the same review showed that long-term improvement (on the order of years) was higher among patients with secondary RP (89%) compared to those with primary RP (58%). While promising, complications related to thoracic sympathectomy are not uncommon and can include the development of hyperhidrosis, Horner syndrome, and persistent neuropathic pain.139 If the procedure proves unsuccessful, the recurrence of symptoms generally occurs after 6 months. Localized digital sympathectomy is an alternative procedure that appears to have comparable efficacy to the thoracocervical approach. The operation involves careful stripping of the adventitia containing the autonomic nerve plexus from the palmar arterial arch, common digital arteries, and/or proper digital arteries.141,142 As a result of the meticulous nature of the procedure, its availability is limited to specialized centers. Serious complications are very infrequent. Postoperative pain and scar formation constitute the major cause for procedurerelated morbidity. A novel 2-step incision technique for performing digital artery sympathectomy for RP has been published, with similar results in terms of symptom improvement and lower rates of scar formation, faster postoperative recovery time, and better aesthetic outcomes.143
SURGICAL DEBRIDEMENT AND AMPUTATION
Surgical debridement may be needed for chronic, nonhealing ulcers and if devitalized necrotic tissue develops. If gangrene supervenes, amputation may be required. Osteomyelitis developing in the context of a digital ulcer may also mandate partial digit amputation.
2624
VASCULAR RECONSTRUCTION
Surgical reconstruction of the digital arteries is rarely indicated for RP. It may provide relief of symptoms and improve digital perfusion if proximal artery occlusion develops, which is most often seen in the setting of severe SSc, advanced atherosclerosis, or chronic thromboembolic disease.144
SPECIAL CONSIDERATIONS
SPECIAL CONSIDERATIONS
ULCER CARE
Digital ulcers from RP can be extremely painful and often take weeks or months to heal. Pain control is important because pain may lead to vasospasm and provoke additional bouts of ischemia. In some instances, opioids are needed to control symptoms. Digits with ulcers should be soaked in a tepid antiseptic solution twice daily to soften or loosen crusts or eschars. After drying, plain petrolatum is applied to the ulcer, and the digit is covered with an occlusive dressing. Maximum tolerated pharmacologic therapies should be employed throughout treatment of an ulcer to promote wound healing by improving blood flow to the area. Importantly, local wound care alone without pharmacologic intervention to improve digital blood flow is unlikely to result in ulcer resolution. Infection is a common complication of digital ulcers and typically manifests with increasing pain, erythema, swelling, or purulent drainage. Cultures usually demonstrate Staphylococcus species, and treatment with cephalosporins, or in the case of methicillin-resistant Staphylococcus aureus, trimethoprim-sulfamethoxazole, clindamycin, or a tetracycline, are usually effective. Antimicrobial therapy should be directed by the local antibiogram when available.
CRITICAL ISCHEMIA
Raynaud crisis is typified by critical ischemia and always requires urgent intervention. The guiding principle for managing Raynaud crisis is early diagnosis and intervention to preempt irreversible tissue injury. Patients with critical ischemia require hospitalization and intravenous prostaglandin therapy.2,145
Iloprost dosed 0.5 to 2 ng/kg by continuous infusion should be given over several hours on 3 consecutive days. Intraarterial phentolamine also has been successfully used in cases of Raynaud crisis, but its administration requires monitoring in an acute care setting given the risk for hemodynamic instability. Analgesics and antibiotics are often coadministered when digital ulcers are present. Skilled nursing and podiatry care (for toe involvement) is an important element of ulcer care, and wound assessments should be performed at routine intervals. It is essential to exclude competing diagnoses when evaluating the patient with critical ischemia. Medium-vessel vasculitis, thromboembolism, and severe atherosclerotic
22
Treatment algorithm for Raynaud phenomenon
Confirmed case of Raynaud phenomenon
Behavioral modification
Layered clothing
Smoking cessation
Limiting caffeine ingestion
Titrate to lowest possible dose, consider treatment holiday during warm season
Response
No response
Nifedipine 30–90 mg extended-release, every evening
Intolerance
Discontinue nifedipine and start sildenafil 20 mg thrice daily and/or pentoxifylline 400–800 mg thrice daily and/or fluoxetine 20–40 mg daily
Inadequate response
Add sildenafil 20 mg thrice daily and/or pentoxifylline 400–800 mg thrice daily and/or fluoxetine 20–40 mg daily
Inadequate response Intolerance
Trial of losartan 25–100 mg daily or Trial of prazosin 1–5 mg daily
Response
Titrate to lowest possible medication doses
Inadequate response
Recalcitrant digital ulcers or Raynaud crisis
Botulinum neurotoxin injections 40–100 units per hand*
Inadequate response
Iloprost 0.5–2 ng/kg/min infused over 8 hours × 5 consecutive days, followed by every 6-week infusions
Trial of topical nitrate or
L–arginine 2–8 g daily
Recalcitrant digital ulcers or Raynaud crisis
In carefully selected patients, trial of bosentan 62.5 mg twice daily × 4 weeks then increase to 125 mg twice daily
disease may mimic Raynaud crisis, but their management differs substantially. Anticoagulation therapy with heparin may be considered if signs of tissue ischemia continue despite aggressive medical therapy. A digital block with lidocaine or bupivacaine can provide pain relief and serves as a chemical sympathectomy to reverse vasoconstriction. Surgical interventions may be considered as a salvage effort in unresponsive patients.
TREATMENT ALGORITHM
TREATMENT ALGORITHM
*if effective, repeat injections every 3–6 months

Figure 145-1 Triphasic color changes on the fingers of a patient with primary Raynaud phenomenon.

Figure 145-2 Pitted scarring involving fourth and fifth fingertips in a patient with Raynaud phenomenon in the setting of systemic sclerosis.
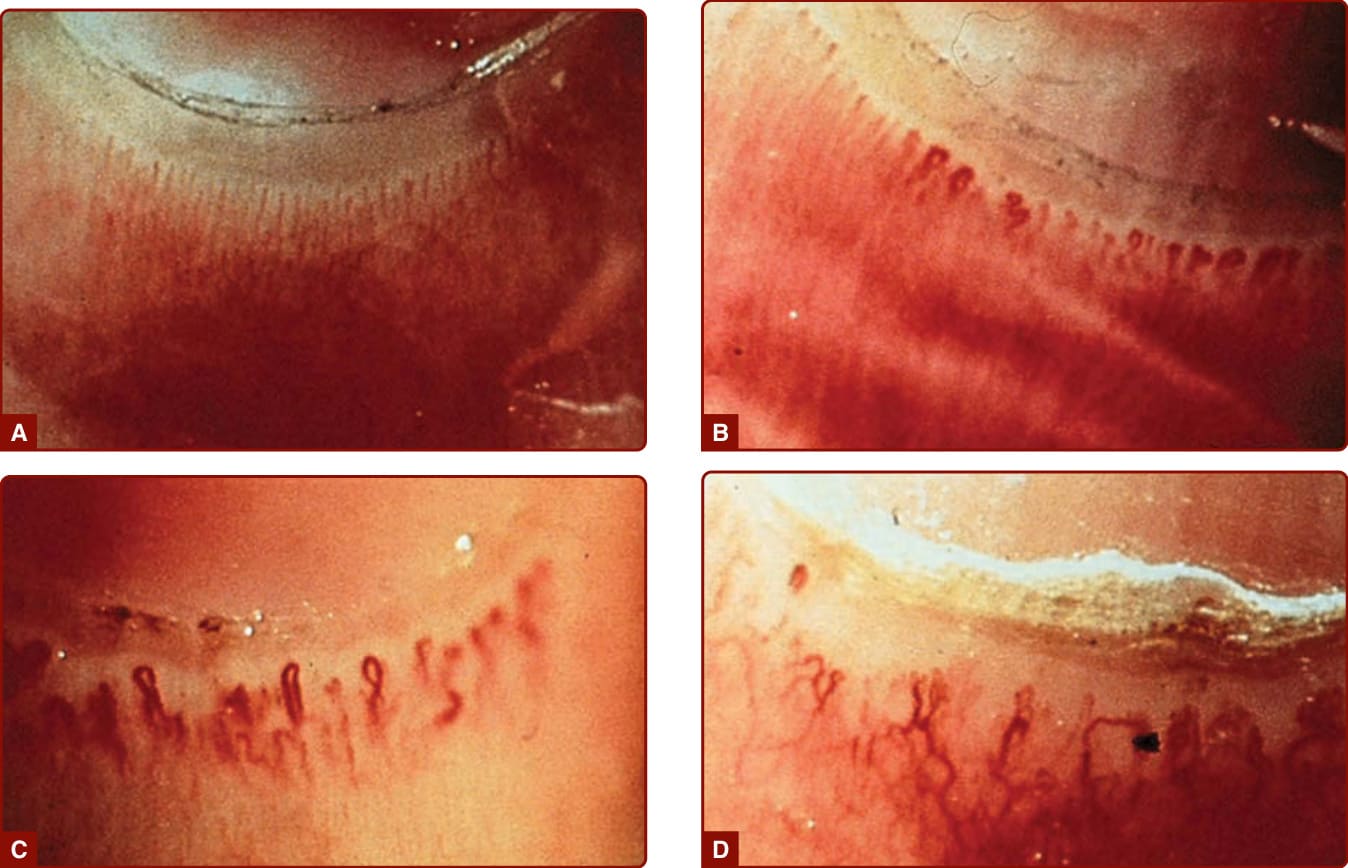
Figure 145-3 Nailfold capillary microscopy in a normal patient (A) compared to 3 patients with systemic sclerosis showing dilated capillaries (B), capillary tortuosity with dropout (C), and a telangiectatic pattern (D).
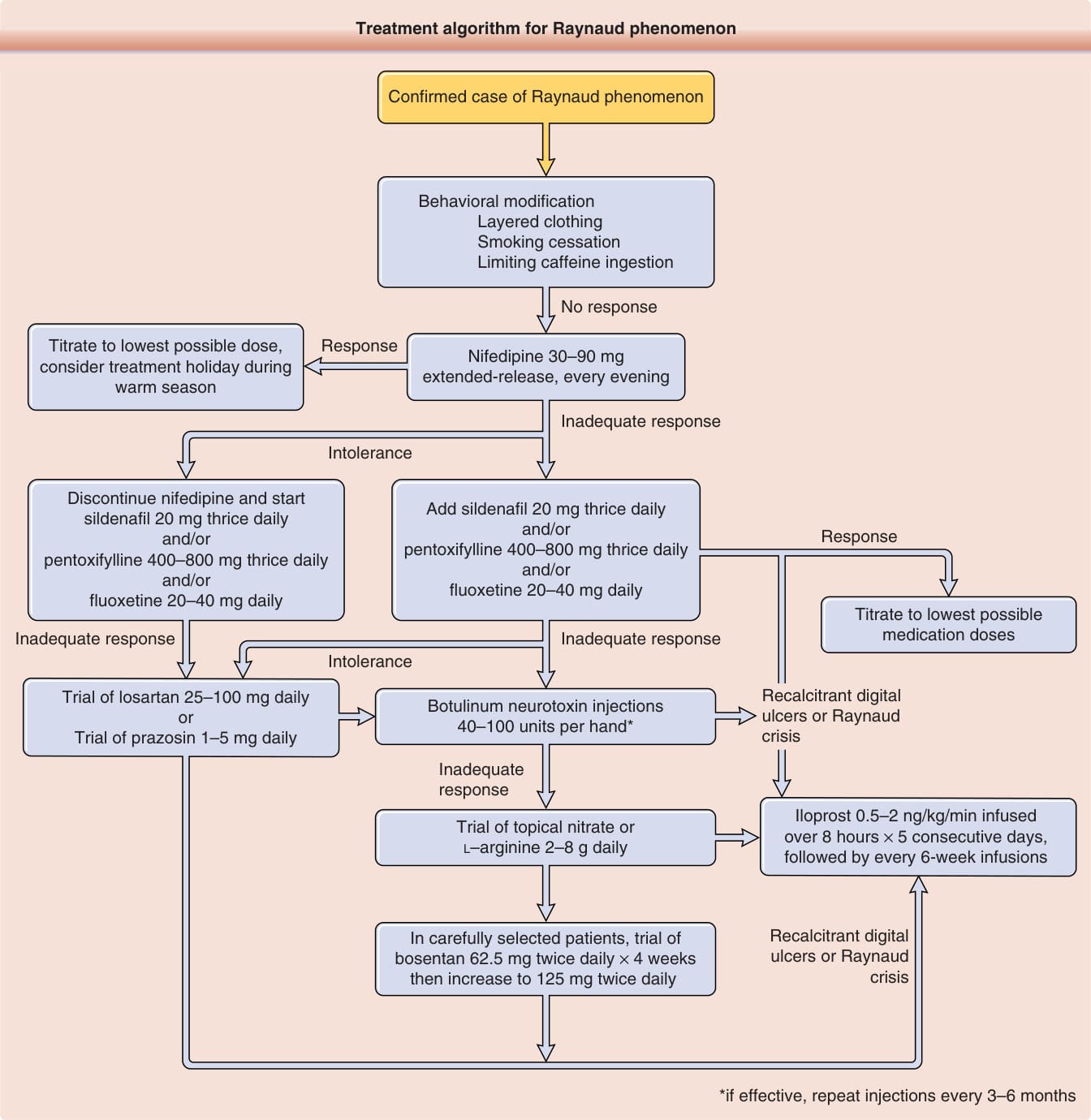
Figure 145-4 Treatment algorithm for Raynaud phenomenon.
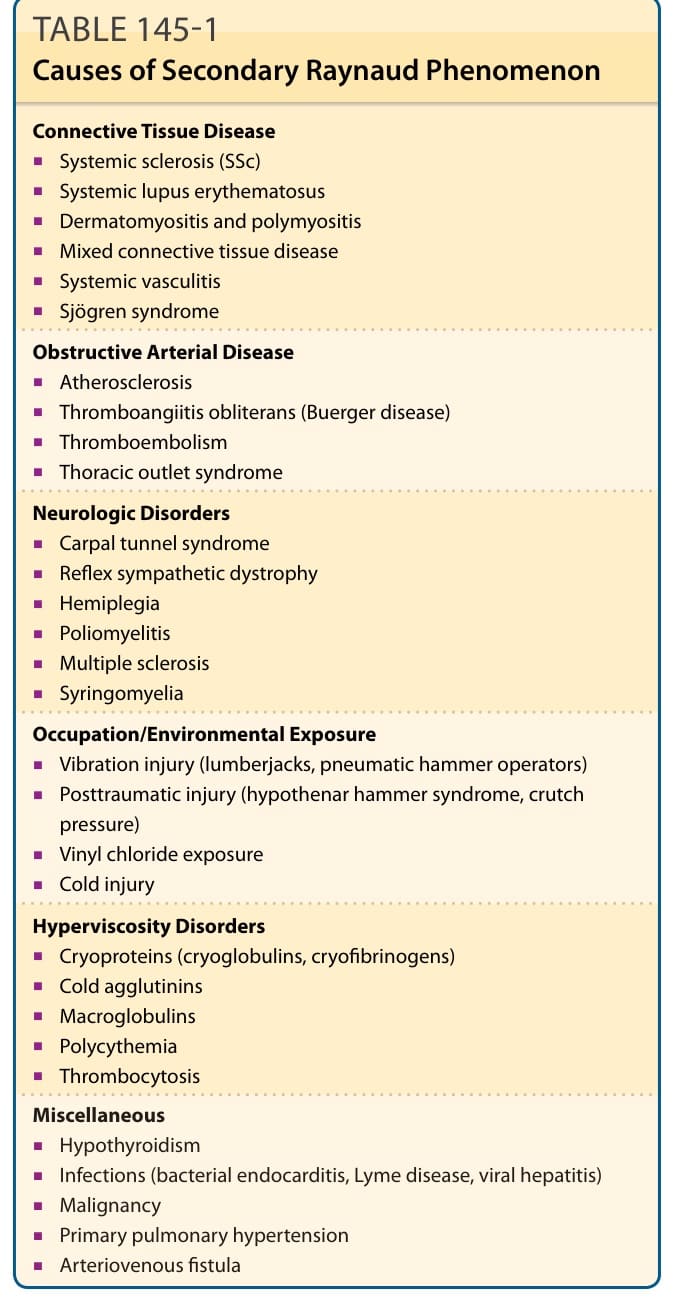
TABLE 145-1 Causes of Secondary Raynaud Phenomenon
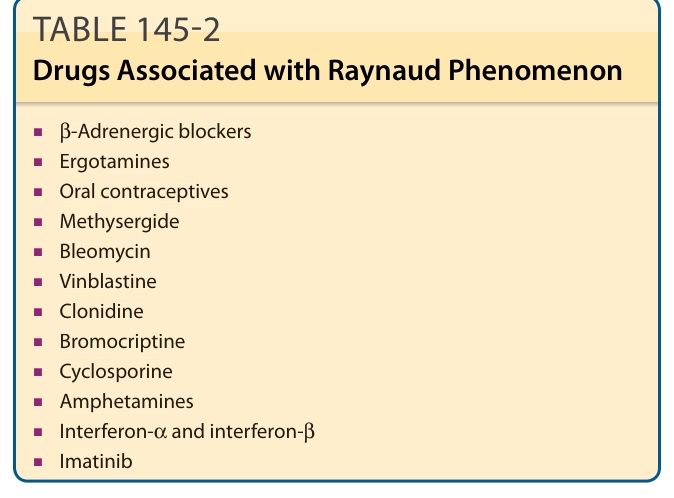
TABLE 145-2 Drugs Associated with Raynaud Phenomenon
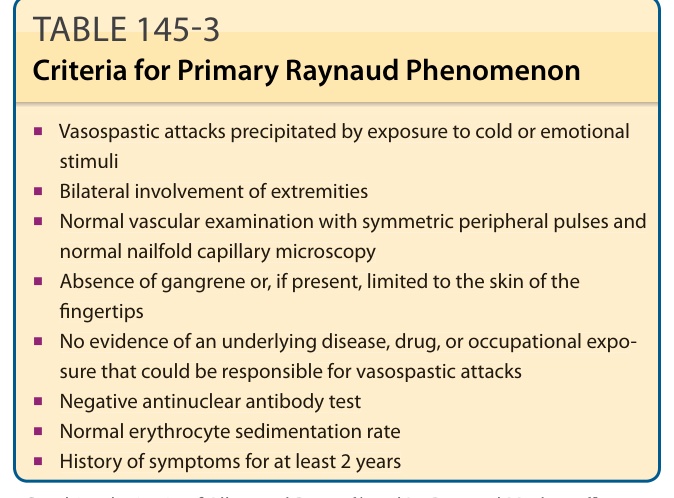
TABLE 145-3 Criteria for Primary Raynaud Phenomenon
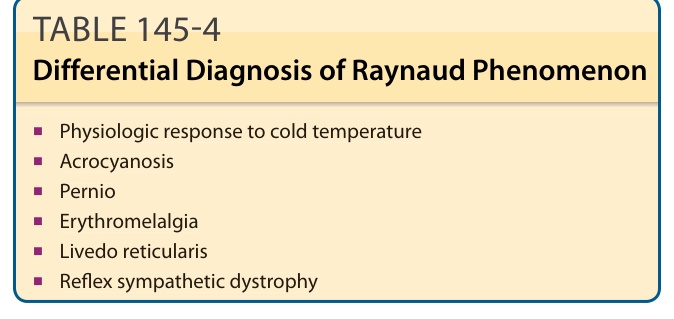
TABLE 145-4 Differential Diagnosis of Raynaud Phenomenon
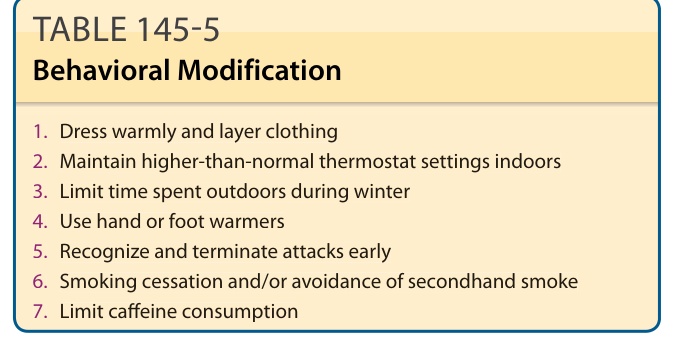
Table 145-5 outlines effective behavior modifications. Mild RP is generally amenable to lifestyle changes that minimize exposure to the cold. Dressing warmly
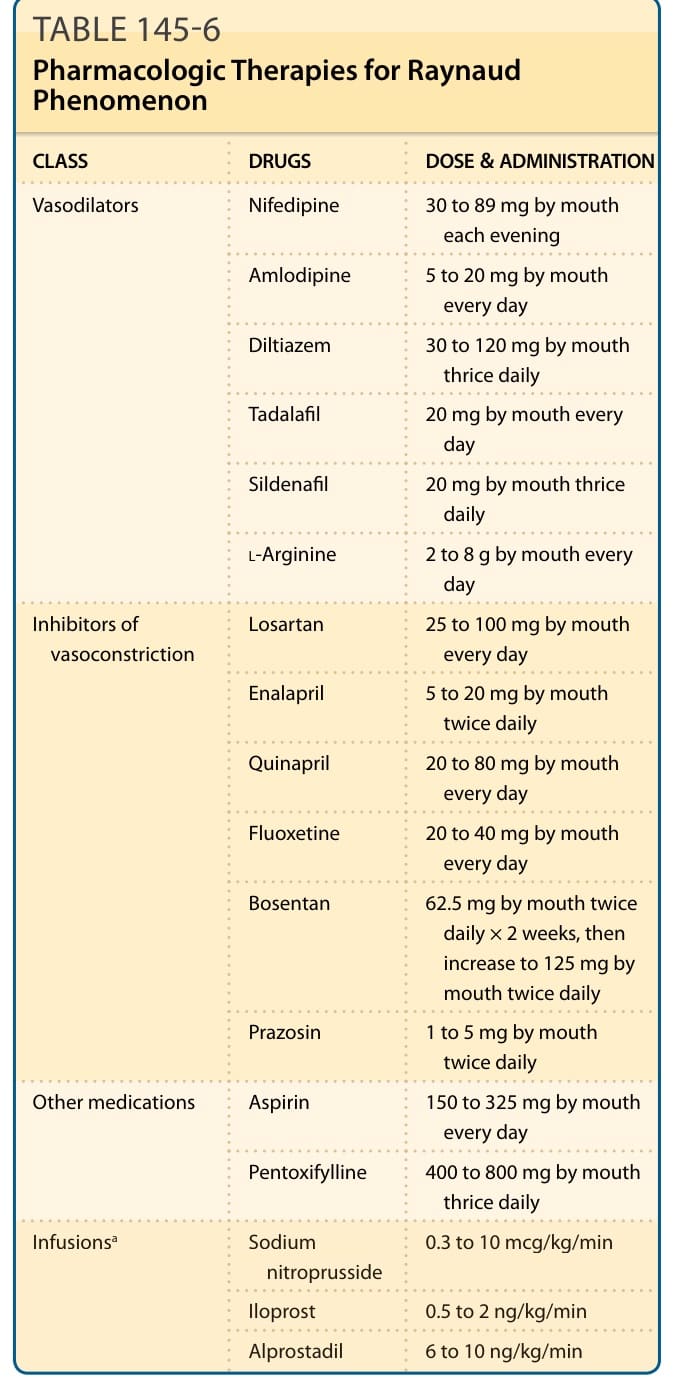
Table 145-6 outlines pharmacologic therapies for Raynaud phenomenon.