Photoprotection
28
AT-A-GLANCE
■ Photoprotection measures include seeking shade during the peak ultraviolet (UV) B hours of 10:00 am to 2:00 pm and the use of high sun protection factor (SPF) broad spectrum sunscreen, clothing, widebrimmed hat, and sunglasses.
■ UV induces skin aging and skin cancer, but using sunscreen may slow down skin aging and reduce the risk of developing skin cancer.
■ Photoprotection in children is essential and its importance should be taught from childhood.
■ Although oral photoprotection cannot substitute for topical sunscreen, it may serve as a secondary measure to prevent skin damage from solar radiation.
■ UV protection factor is a UV protection rating for fabrics. Several chemical treatments can increase a fabric’s natural UV protection factor.
■ Many types of glass have very good UVA2 and UVA1 protection (up to 380 nm).
■ Sunglass standards, mandatory in Australia and voluntary in the United States, specify a maximum percentage of light allowed to be transmitted and a minimum vertical dimension of sunglasses.
The earth is constantly exposed to radiation from the sun, which is indispensable for life. Radiation includes ultraviolet, visible, and infrared rays. Ultraviolet (UV) light B, which accounts for 5% to approximately 10% of the UV light that reaches the surface of the earth, is high in energy and induces erythema. UVA is composed of UVA2 (320 nm to approximately 340 nm) and UVA1 (340 nm to approximately 400 nm). UVA1 is low energy and accounts for 95% of the UV that reaches the surface of the earth because it can penetrate through clouds and glass windows, and is not obstructed by the ozone layer For this reason, UVA1 is present all the time, regardless of cloud cover or other obstruction. Although UVA1 may not cause erythema, it is more likely to cause pigmentation than any other wavelength. In addition, it induces reactive oxygen species (ROS), which cause damage to blood vessels, collagen fibers, and elastic fibers located deep under the skin, and are involved in skin aging. Infrared rays also affect skin and trigger skin aging by increasing skin temperature.1
With increased attention to physical fitness and outdoor recreational activities, daily exposure to sunlight is common. In addition, longer life expectancy has increased the amount of lifetime exposure to sunlight. Although sun exposure may have beneficial effects, such as mood elevation and vitamin D3 photosynthesis, unwanted effects are well known. Acute
effects of sun exposure include sunburn and delayed tanning. Acute responses to sunlight result from the direct influence on biologic chromophores like DNA. These responses release proinflammatory cytokines, enzymes, and immunosuppressive factors. These effects are mediated by ROS, which are generated by UVB, UVA and visible light as well as and infrared rays. Chronic responses to sunlight are a result of accumulation of damage and decreased ability to repair. Chronic sun exposure is strongly associated with photoaging, actinic keratoses, and skin cancers. Complete avoidance of sun exposure is neither necessary, practical, nor would it be generally acceptable to the general public. As such, behavioral modifications such as seeking shade during peak UVB hours of 10:00 am and 2:00 pm, the use of photoprotective measures, such as sunscreen, clothing, wide-brimmed hat, and sunglasses, and, when appropriate, intake of vitamin D supplements, have become the public health message to deliver. This chapter discusses the currently available (as of this writing), commonly used photoprotective measures, as well as oral photoprotection, which is gaining increasing attention.
AVOIDANCE OF SUN EXPOSURE
An ideal photoprotection method is to avoid sunlight. Therefore, it is recommended to stay indoors when the UV rays are strong. The amount of UV that reaches human skin is influenced by the changes in environment. Sunlight is absorbed when entering the atmosphere. The ozone (O3) layer, the stratosphere layer at 10 to 50 km above the surface of the earth, absorbs all of the UVC, most of the UVB and barely any UVA. When the sun is at its highest above the horizon, the distance UV penetrates the atmosphere is relatively shorter, and thus less is absorbed in the atmosphere and more reaches the surface of the earth. Therefore, between 10:00 am and 2:00 pm, when UV is strongest, the sun is best avoided. Also, UV decreases by 3% as the latitude increases by 1°. Because atmosphere becomes thinner as altitude increases, UV increases by 4% every 300 meters from the horizon. Snow, sand, and metal can reflect up to 90% of UV. UV is reduced by 50% to approximately 95% under the shade; hence, one should stay in the shade if possible.
SUNSCREEN
Sunscreen is used to prevent the detrimental effects of UV, and should not be used to prevent sunburn simply to stay longer outside under the sun. People generally
28
apply sunscreen less than the recommended amount, and do not reapply it every 2 hours. Furthermore, the amount of UV required for DNA damage is far less than the amount of UV needed to induce erythema. Therefore, application of sunscreen does not preclude sun damage, and one should continuously take all measures to prevent UV irradiation.
HISTORY
HISTORY
The first UVB filter, PABA (para-aminobenzoic acid), was patented in 1943, and the first UVA filter, a benzophenone, was introduced in 1962. In 1972, the U.S. Food and Drug Administration (FDA) reclassified sunscreens from cosmetics to nonprescription drugs, resulting in more stringent regulation. In 1979, long UVA filters, dibenzoylmethane derivatives, became available. In the 1990s, the need for protection against UVA, as well as against UVB, was recognized, which led to further development of UVA filters. In 2001, the FDA defined 16 active sunscreen ingredients with maximum concentrations, and in 2011, established labeling and effectiveness testing for broad-spectrum protection and water resistance.2
SUN PROTECTION FACTOR
SUN PROTECTION FACTOR
The sun protection factor (SPF) was first developed by an Austrian, Franz Greiter, in 1962, and was adopted by the FDA in 1978.3 Current FDA guidelines specifically require that products be tested using a solar simulator with emission spectrum covering the wavelength range of 290 nm to 400 nm, and that the sunscreen product be applied at a concentration of 2 mg/cm2. By definition, SPF is the ratio of the minimal erythema dose (MED) of a subject’s sunscreen-protected skin over the MED of the unprotected skin:
SPF MED of sunscreen-protected skin MED of unprotected skin =
Because the end point is erythema, SPF is a reflection of sun protection against the biologic effect of UVB (290 nm to 320 nm), and, to a lesser extent, UVA2 (320 nm to 340 nm). In other words, SPF15 does not mean that the exposure time to solar radiation is extended by 15 times, but that the amount of radiation required to cause erythema is increased by 15 times after the use of sunscreen. Figure 197-1 shows the effect of sunscreens with different SPFs on the transmission of erythemogenic rays.4 If an individual develops slight erythema after 10 minutes of sun exposure, 30 minutes of unprotected sun exposure will result in a 3 MED sunburn. In contrast, when wearing an SPF15 or SPF30 sunscreen, the same 30-minute exposure would result in only 20% or 10%, respectively, of an MED. With chronic exposure, the added protection from an SPF30 sunscreen halves the cumulative UV damage
3624
Effect of sun protection factor on an individual
SPF15
40
SPF30
% Sunburning dose
30
20
10
0
0 10 20 30 40
Sun exposure (minutes)
compared to the SPF15 sunscreen, even though both products prevent sunburn. The concentration of sunscreen specified for SPF testing (2 mg/cm2) is the equivalent of 1 oz (30 mL) of sunscreen to cover the entire body surface. Studies of the actual sunscreen usage by individuals have consistently demonstrated that the amount of sunscreen applied is closer to 0.5 to 0.8 mg/cm2, so that the actual in-use SPF is significantly lower than the label SPF.5
The relationship is not linear, and an SPF30 product (at 2 mg/cm2) has an SPF of only 3 if applied at 0.5 mg/cm2 (Fig. 197-2).6
Relationship between the dose of sunscreen applied and the in-use SPF
40
35
SPF15 SPF30
30
Predicted in-use SPF
25
20
15
10
5
0
0 .5 1 1.5 2 2.5 3
Dose (mg/cm2)
SPF2 products absorb 50% of the UVB when applied at 2 mg/cm2 and the other 50% is absorbed into skin. SPF15 blocks 93.3% of UVB and 6.7% is absorbed into skin. SPF30 blocks 96.7% of UVB and 3.3% is absorbed into skin. It may appear that this difference is not significant as SPF15 blocks 93.3% and SPF30 blocks 96.7% of UVB; however, this is not true. In fact, the important factor in photoprotection is not how much is blocked by sunscreen, but how much is prevented from being absorbed into skin. For SPF15, 6.7% is absorbed into skin, whereas for SPF30, 3.3% is absorbed, which is only half the amount. Also, the amount of UVB needed to cause DNA damage that results in skin cancer is less than the amount needed to cause erythema. Moreover, the amount of sunscreen people use is always less than 2 mg/cm2. Therefore, it is more helpful to choose sunscreen with the highest SPF available.
ASSESSMENT OF ULTRAVIOLET A PROTECTION
ASSESSMENT OF
ULTRAVIOLET A
PROTECTION
SPF is accepted as the worldwide standard for the assessment of protection against the erythemogenic effects of UVB and UVA2. Among the several methods to evaluate protection against UVA, the persistent pigment darkening (PPD) method has become the most widely used in the past years.6,7 In the PPD method, the dose of UVA required to induce PPD observed 2 to 24 hours after exposure of sunscreen-protected skin is compared to that of sunscreen-unprotected skin; the ratio is then expressed as the UVA protection factor. In many countries, including Japan and Korea, the UVA protection of sunscreen products is then classified as PA+, PA++, or PA+++ (where PA indicates protection for UVA). The European Union requires UVA protection factor to be at least one-third of the labeled SPF, with the PPD method as the assessment of the UVA protection. For example, a SPF30 sunscreen must have a UVA protection factor of at least 10.8
In June 2011, the FDA decided to use an in vitro critical wavelength test (broad-spectrum test) to assess UVA protection of sunscreens sold in the United States.9 The broad-spectrum test measures a sunscreen product’s absorbance of UV radiation across both the UVA and UVB regions of the spectrum. To label a sunscreen product as “broad spectrum,” it should have a critical wavelength of at least 370 nm. The critical wavelength is the wavelength at which the area-under-the-absorbance-curve represents 90% of the total area-under-the-curve in the UV region. For SPF15 or higher sunscreen products that are broad spectrum, use of the following statement is optional: “if used as directed with other sun protection measures, decreases the risk of skin cancer and early skin aging caused by the sun.” In addition, in vivo PPD testing is no longer required in the United States according to this rule.
28
IMMUNE PROTECTION FACTOR
IMMUNE PROTECTION
FACTOR
SPF for a sunscreen product correlates poorly with its ability to protect against immunosuppression. This has resulted in the development of the concept of immune protection factor to quantify the ability of sunscreen products to prevent immunosuppression.10 Several different methods have been used, including contact sensitization and intradermal injection, all of which are quite laborious and time consuming to perform. Until a simple and reliable method that can be easily performed in a large number of test persons is developed, it is unlikely that immune protection factor will be used to rate commercial products.
ULTRAVIOLET FILTERS
ULTRAVIOLET FILTERS
There are 3 different nomenclatures used by the sunscreen industry and regulatory agencies around the world: (a) International Nomenclature of Cosmetic Ingredients (INCI), (b) United States Adopted Name (USAN), and (c) trade name. USAN is the nomenclature used in the FDA Sunscreen Monograph. For example, for a widely used UVA1 filter, the INCI name is butyl methoxydibenzoylmethane, the USAN is avobenzone, and a trade name is Parsol 1789. In this chapter, when available, the USAN nomenclature is used. The term sunblock is commonly used to refer to sunscreens and their active ingredients, but it is a misnomer, and the FDA Sunscreen Monograph does not sanction the term. All sunscreen active ingredients are filters that absorb part of the incident UV radiation, but a portion of the radiation is always transmitted. Microfine inorganic filters additionally reflect and scatter UV radiation. In the United States, all active sunscreen ingredients are regulated by the FDA as nonprescription drugs.9
Only UV filters listed in the Sunscreen Monograph issued by the FDA may be marketed in the United States (16 active ingredients; Table 197-1). In addition, filters approved by the FDA as active ingredients of final products through the New Drug Application (NDA) process also can be marketed in the United States, as was done for the latest UVA filter available in the U.S. market, ecamsule (Mexoryl SX). In 2002, the FDA instituted the Time and Extend Application process as an alternate to filing the NDA.11 With the Time and Extend Application process, data generated outside the United States can, for the first time, be used for the application, provided that the sunscreen product has been marketed for nonprescription purchase for a minimum of 5 years in the country where testing was performed. In the European Union, South America, many Asian countries, and Africa, sunscreens are regulated as cosmetics, resulting in a simpler and more expeditious approval process compared to the United States, usually resulting in approval within 1 to 2 years
3625
28
U.S. ADOPTED NAMEa INTERNATIONAL NOMENCLATURE OF COSMETIC INGREDIENTS kmax (nm); OR ABSORPTION RANGE COMMENT
Organic Filters: UVB
■PABA derivatives
■PABA PABA 283 Stains clothing; not widely used
■Padimate O Ethylhexyl dimethyl PABA 311 Most commonly used PABA derivative; photounstable
■Cinnamates
■Octinoxate Ethylhexyl methoxycinnamate 311 Most widely used UVB filter; photounstable
■Cinoxate Cinoxate 289 —
■Salicylates
■Octisalate Ethylhexyl salicylate 307 Weak UVB absorbers; improves photostability of other filters
■Homosalate Homosalate 306
■Trolamine salicylate Triethanolamine salicylate 260 to 355 Weak UVB absorbers; good substantivity—used in waterresistant sunscreens and hair-care products
■Others
■Octocrylene Octocrylene 303 Photostable; improves photostability of photolabile filters
■Ensulizole Phenylbenzimidazole sulfonic acid 310 Water soluble; enhances sun protection factor of the final product
Organic Filters: UVA
■Benzophenones
■Oxybenzone Benzophenone-3 288, 325 Most commonly used UVA filter; most common cause of photoallergic contact dermatitis to UV filters
■Sulisobenzone Benzophenone-4 366 —
■Dioxybenzone Benzophenone-8 352 —
■Others
■Avobenzone Butyl methoxydibenzoylmethane 360 Photounstable; enhances the photodegradation of octinoxate
■Meradimate Menthyl anthranilate 340 A weak UVA filter; no sensitization reaction reported
Inorganic Filters
■Titanium dioxide
■Titanium dioxide
■Zinc oxide Titanium dioxide Zinc oxide See belowb
See belowb No report of sensitization reaction; photostable; used to enhance photostability of the final product; micronized zinc oxide has better UVA1 protection compared to microfine titanium dioxide; micronized zinc oxide has lower refractive index compared to microfine titanium dioxide and thus appears less white; commonly coated with dimethicone or silica to maintain effectiveness as sunscreen
Titanium dioxide Zinc oxide
See belowb
■Zinc oxide
See belowb
aThis is the name used by the U.S. Food and Drug Administration in the listing.
No report of sensitization reaction; photostable; used to
enhance photostability of the final product; micronized zinc oxide has better UVA1 protection compared to microfine titanium dioxide; micronized zinc oxide has lower refractive index compared to microfine titanium dioxide and thus appears less white; commonly coated with dimethicone or silica to maintain effectiveness as sunscreen
bλmax ranges from visible to UVA to UVB range, depending on the particle size. As titanium dioxide is micronized (10 nm to 50 nm in diameter), λmax shifts toward UVB; microfine zinc oxide maintains a flat absorption profile spanning from UVB to UVA. PABA, para-aminobenzoic acid. Data from Kullavanijaya P, Lim HW. Photoprotection. J Am Acad Dermatol. 2005;52:937; and Department of Health and Human Services, Food and Drug Administration. Sunscreen drug products for nonprescription human use; final monograph. Fed Regist. 1999;64:27666.
of filing. Currently, there are at least 34 approved active ingredients in Australia and 26 in the European Union. UV filters can be divided into 2 categories: organic and inorganic. These terms are recommended by the FDA to replace the terms chemical and physical filters, respectively. Organic filters can be subdivided further into UVB filters and UVA filters. The most widely used UVB filter worldwide is octinoxate (ethylhexyl
3626
methoxycinnamate), whereas the most widely used UVA filter is oxybenzone (benzophenone-3). Titanium dioxide (TiO2) and zinc oxide (ZnO) are inorganic filters that are snowy white in color and insoluble in water. They are photostable and do not react with organic filters. When their size is larger than 200 nm, inorganic filters can protect skin from all the wavelengths of UV. Also, visible rays and infrared rays may be reflected
and scattered. Depending on the size, the properties of reflection or absorption change. Inorganic filters are not allergenic and do not react with skin, and are thus recommended for children and adults with allergies. However, inorganic filters are not preferred and are restricted in use because they leave a white coating behind. If applied too often, they may be comedogenic. On the other hand, micronized titanium dioxide is 10 nm to 100 nm in size. Because titanium dioxide scatters less visible light, it does not leave a white coating behind. However, its ability to block UV radiation decreases, leading to declined effect of photoprotection. Also, titanium dioxide may have negative effects on health if absorbed into skin. Therefore, more studies are required to elucidate whether inorganic filters actually penetrate into the skin, especially if they are used on inflamed skin or infants. Sunscreen products combine ingredients in a variety of combinations to produce a product that confers stability and optimal UV protection. Currently, unless products are approved as new drugs through the NDA process, the FDA guidelines do not allow avobenzone to be combined with PABA, padimate O, or inorganic filters (titanium dioxide, zinc oxide).
ULTRAVIOLET FILTERS AND PHOTOSTABILITY
Avobenzone (butyl methoxydibenzoylmethane; Parsol
1789) is an excellent UVA1 filter but is photounstable and degrades during UV exposure. There are several other UV filters with this characteristic, including UVB filters padimate O (ethylhexyl dimethyl PABA) and octinoxate (ethylhexyl methoxycinnamate).12 It is possible to incorporate other agents to increase the photostability of the final product (Fig. 197-3). Most of these agents are photostable UV filters (eg, octocrylene, salicylates, oxybenzone) that absorb photons to minimize the effect on the photounstable UV filter; they also serve as receptor molecules for energy transfer from excited state photounstable filter, hence minimizing the photodegradation of the latter (Fig. 197-3).5,13
In vitro, sunscreens containing photostabilized avobenzone have been shown to retain up to 90% of the active filter following 25 MED (50 J/cm2) of solarsimulated radiation, the equivalent of approximately 5 hours of sun exposure.13 Under ideal circumstance this would allow the user to apply sunscreen only once daily. However, it should be noted that sunscreens do migrate on the skin surface toward follicular orifices, resulting in an uneven distribution of UV filters; furthermore, sunscreens do get removed by rubbing and from water or sweat exposure. This is the reason that the FDA, in the final rule, advises that sunscreen should be reapplied every 2 hours.9
ULTRAVIOLET FILTERS AND PHOTOALLERGY
Octocrylene, oxybenzone (benzophenonone-3), and avobenzone (butyl methoxydibenzoylmethane) are
28
Photostabilization of photounstable filter
Excited state
Photostable UV filter ground state
Energy transfer
UV Excited state
Photodegradation
Photounstable filter ground state
the most common causes of UV filter photoallergy.14 It should be noted that although UV filters are the most common cause of photoallergy in many studies in the United States and the United Kingdom, considering the number of individuals using sunscreens, the prevalence of photoallergy to UV filters is very low (much less than 1%). No photoallergy has been reported with inorganic UV filters (titanium dioxide and zinc oxide).
SUNSCREEN USE IN CHILDREN
SUNSCREEN USE IN
CHILDREN
Because of the concern about percutaneous absorption of sunscreens, the 1999 FDA Sunscreen Monograph recommends that the physician should be consulted on the use of sunscreens in children younger than age 6 months.9 For this group of patients, it is prudent to use other means of photoprotection, such as clothing.15
Children younger than 2 years old should use inorganic sunscreen rather than organic sunscreen.
SUNSCREEN USE IN PREGNANCY
SUNSCREEN USE IN
PREGNANCY
During pregnancy, sunscreen is also recommended to prevent skin damage from UV radiation, such as pigmentary disorders, especially melasma. Sunscreen has been proven safe by toxicology tests, including
3627
28
teratogenic tests; however, studies regarding safety of nanoparticulate inorganic ingredients during pregnancy are not available.16
CONTROVERSIES
CONTROVERSIES
POTENTIAL SYSTEMIC ABSORPTION Organic Ultraviolet Filters: Systemic absorption of some organic UV filters following topical application to the skin has been reported.17 In humans, up to 2% of an applied dose of benzophenone-3 and its metabolites were excreted in the urine following topical application of a commercially available product. The chemical characteristics of organic UV filters, such as molecular weight and solubility in fluids, as well as vehicle and viscosity of the sunscreen products, influence skin penetration.
Inorganic Nanoparticles: Metal oxide inorganic UV filters (titanium dioxide and zinc oxide) have been widely used in the form of nanoparticles. This is to minimize the reflection of visible light, thereby enhancing the aesthetic appearance of the final product. Nanoparticles are defined as particles less than 100 nm. In vitro, these particles can induce free radical formation in the presence of UV radiation, resulting in cell damage. Multiple studies have shown that neither nanostructured titanium dioxide nor zinc oxide penetrates beyond the stratum corneum of skin.18 The risk for humans from using sunscreens that contain nanostructured titanium dioxide or zinc oxide is considered negligible.
NONMELANOMA SKIN CANCER AND MELANOMA
Although there have been questions in the past, the protective role of sunscreens in the prevention of skin cancer development has now been established. In a 4.5-year study with an 8-year followup of more than 1600 individuals in Australia, it was shown that the group that was assigned to use SPF16 broad-spectrum sunscreen had a decreased incidence of squamous cell carcinoma and basal cell carcinoma by 38% and 25%, respectively.19 In a 10-year followup, 11 melanomas developed in the sunscreen group, compared to 22 in the control group.20
VITAMIN D
Another area of controversy is the concern that photoprotection may compromise health by decreasing a person’s serum vitamin D level, specifically the level of the highly variable “storage form” (25-OHvitamin D) that is the precursor to the tightly regulated active form [1,25-(OH)2-vitamin D]. There are only 3 sources of vitamin D. Exposure to the UVB spectrum of sunlight converts 7-dehydrocholesterol in
3628
the skin to previtamin D by photoisomerization. Also, previtamin D converts to vitamin D by heat isomerization. Subsequently, vitamin D is hydroxylated in the liver and kidneys to its active form. The peak action spectrum for previtamin D synthesis is 300 ± 5 nm. However, previtamin D3 and vitamin D3 are sensitive to UV radiation. If they are constantly exposed to sunlight in the skin, they will be photodegraded and become inactive. Therefore, continuous exposure to sunlight does not produce vitamin D proportionally. It is the reason why vitamin D intoxication does not occur with excessive sun exposure. The amount of UVB required to produce daily needed vitamin D in humans is not so much; exposure of 0.33 or 0.5 MED 2 or 3 times a week to arms, hands, and face is sufficient. In other words, a person with skin type II who lives in Boston needs only 5 minutes at noon in July.21 According to another study, arms and legs can create 3000 IU by being exposed to 0.5 MED of UVB. Therefore, lightskinned people can produce sufficient vitamin D by staying under midday sunlight for 5 to approximately 30 minutes, twice a week.22
Another source is dietary intake, although only a few naturally-occurring foods contain a significant amount of vitamin D (eg, oily salt water fish [herring, salmon, and sardines], cod liver oil, and egg yolk). In the United States, milk, orange juice, margarine, butter, cereals, and chocolate mixes are fortified with vitamin D. Lastly, vitamin D supplements are readily available as vitamin D3 (cholecalciferol, the form produced in skin) or vitamin D2 (ergocalciferol); as of this writing, vitamin D3 is more commonly used than vitamin D2 because vitamin D3 is considered to be more stable.22
The effect of application of sunscreens on vitamin D levels has been evaluated. A relatively recent review of all the published evidence concluded that normal usage of sunscreens does not generally result in vitamin D insufficiency.23 This is primarily a result of the inadequate application of sunscreens—applying an insufficient amount of sunscreen or not reapplying sunscreen every 2 hours—and sunscreen users may expose themselves to more sun than nonusers. Hence, in these cases, even when sunscreen is applied, daily required UVB for vitamin D production is achieved. However, among patients who practiced diligent photoprotection (eg, those with lupus erythematosus or erythropoietic protoporphyria), a large percentage were found to have inadequate serum vitamin D levels.24,25 A comprehensive review by the U.S. Institute of Medicine, released in November 2010, concluded that the strongest evidence for the beneficial effect of vitamin D on health is for bone health; in contrast, for extraskeletal outcomes, the Institute of Medicine review indicated that the current evidence is inconsistent and inconclusive and as such is insufficient to make public health recommendation.26 Because the action spectrum for cutaneous vitamin D synthesis (ie, UVB) is the same as for DNA damage and photocarcinogenesis, it is not advisable to use sun exposure as a means of obtaining vitamin D. For those individuals who are concerned or are at risk for vitamin D insufficiency, a balanced diet and a daily 600 IU vitamin D3 supplement, along with 1 g of calcium,
is recommended.26 This recommendation applies especially to elderly individuals who are homebound darkskinned individuals with modest sun exposure, and those who practice rigorous photoprotection.
ORAL PHOTOPROTECTION
Oral photoprotection refers to consumption of one or more active ingredients to minimize skin damage caused by solar radiation. However, by definition an oral substance cannot replace topical sunscreen, because consumption of the substance is incapable of physically blocking UVR penetration into skin. Instead, it can be used as a complement to prevent or reduce skin damage caused by solar radiation absorption. Oral photoprotection is convenient and useful, assuming that it is effective. It is not influenced by external environments, such as swimming and sweating, and it is not affected by the need to penetrate through the horny layer of skin. However, systemic adverse effects may be present. The action mechanisms by which active ingredients for oral photoprotection prevent skin damage from UV radiation are diverse. The substances react with various targets in UV-induced signaling pathways, exerting antioxidant, antiinflammatory, and immunomodulating actions. The most common substance used for oral photoprotection is an antioxidant, which should be stable and highly capable of eliminating ROS. Its end products after reaction as an antioxidant should not be converted into free radicals. Oral photoprotection alone, without topical sunscreen, is insufficient to adequately protect skin from solar radiation. Nevertheless, its effectiveness is evident. Vitamins, such as vitamin C and vitamin E, as well as extracts or purified substances from certain plants (phytochemicals) can prevent skin damage from solar radiation. Hence, they may be used topically or as oral supplements to maintain healthy skin. Such active phytochemicals include polyphenols, which are either flavonoids or nonflavonoids, and nonpolyphenols, such as carotenoids and caffeine (Table 197-2).
VITAMINS
VITAMINS
L-ASCORBIC ACID (VITAMIN C)
Because of its water soluble properties l-ascorbic acid is the most important antioxidant in the hydrophilic phase. As it is not naturally synthesized in humans, daily intake is best be achieved through food. Studies have not yet proven that oral supplementation of vitamin C alone can protect human skin from sunlight exposure. However, some studies have demonstrated that combined use of vitamin C and vitamin E has positive effects.27
TOCOPHEROL (VITAMIN E)
Along with vitamin C, tocopherol is a natural antioxidant, but is lipid soluble. Having affinity mainly with
28
Vitamins
■ L-Ascorbic acid (vitamin C)
■Tocopherol (vitamin E)
■Nicotinamide
Polyphenol
■Flavonoids
■Catechins
■Isoflavones (genistein, silymarin)
■Proanthocyanidins
■Nonflavonoids
■Phenolic acid (benzoic, gallic, and cinnamic [caffeic, ferulic, and p-coumaric] acids)
■Resveratrol
Nonpolyphenols
Nonpolyphenols
■Carotenoids
■Carotenoids
■Beta-carotene
■Beta-carotene
■Lycopene
■Lycopene
■Astaxanthin
■Astaxanthin
■Caffeine
■Caffeine
cell membrane lipids and intercellular cement lipids, tocopherol plays an important role in protection from oxidative damage by eliminating ROS. α-Tocopherol is oxidized to tocoferoxyl radical by ROS and, in turn, regenerated by vitamin C. Along with vitamin C, glutathione and coenzyme Q10 can recycle tocopherol. Although controversial, high dose oral vitamin E appears effective at reducing UVB-induced damage in human skin.28
NICOTINAMIDE
Nicotinamide (or niacinamide) is an amide form of vitamin B3, which is an essential water-soluble vitamin. Oral nicotinamide is photoprotective. Nicotinamide prevents adenosine triphosphate depletion induced by UV radiation, thereby boosting cellular energy and enhancing DNA repair. Oral nicotinamide is safe and effective in reducing the rates of new nonmelanoma skin cancers and actinic keratoses in high-risk patients.29
POLYPHENOL
POLYPHENOL
Polyphenols are mainly found in fruits, vegetables, coffee, tea, red wine, nuts, cereal, and chocolate. Polyphenols are chemicals that have more than one phenolic ring per molecule. A phenolic ring has a hydroxyl group bound to an aromatic ring. The intrinsic antioxidant activity of polyphenols resides in this hydroxyl (−OH) group that acts as a hydrogen or electron donor to a free radical or other reactive species. The typical classification of these molecules depends on the number and type of phenolic rings, which determine their biologic properties. Polyphenols are classified
3629
28
as flavonoids or nonflavonoids and are being proven effective for cutaneous inflammation, oxidative stress, UV-induced DNA damage, and carcinogenesis in vivo.30
FLAVONOIDS
The flavonoids include catechins, isoflavones, and proanthocyanidins.
Catechins: The catechins are mainly present in tea leaves and are made up of catechin, epicatechin, galactocatechin, epicatechingallate, and epigallocatechin-3-gallate. A double-blind, placebo-controlled study revealed that consuming green tea polyphenols decreased UV-induced erythema in women.31
Isoflavones: The most well-known isoflavones are genistein, derived from soybean, and silymarin, derived from the milk thistle (Silybum marianum). Genistein exerts a photoprotective effect in animal models.32 The major active component of silymarin is silibinin, which has been shown to protect against photocarcinogenesis in animals.33
Proanthocyanidins: The proanthocyanidins are also known as condensed tannins; this is a group of substances widely present in grape seeds. Oral administration of an extract of grape seeds is effective in preventing the UV-induced pigmentation of guinea pig skin34 and inhibiting tumor induction in response to UV radiation in mice.35
NONFLAVONOIDS
The nonflavonoids include the phenolic acids and resveratrol.
Phenoic Acid: The phenolic acids include benzoic, gallic, and cinnamic (caffeic, ferulic, and p-coumaric) acids. They appear mostly in red wine and tea. They exhibit antioxidant properties. Caffeic acid has been shown to protect against UVA-induced photodamage by ROS in mice.36
Resveratrol: Resveratrol, a stilbene found in grapes, red wine, and nuts, is also a potential polyphenolic antioxidant. Resveratrol suppresses UV-induced malignant tumor progression in mice.37
NONPOLYPHENOLS
NONPOLYPHENOLS
The nonpolyphenolic phytochemicals include carotenoids and caffeine.
CAROTENOIDS
Carotenoids, which are vitamin A derivatives, include beta-carotene, lycopene, and astaxanthin. They are effective antioxidants for photoprotection.
3630
Lycopene and beta-carotene are relatively abundant in the human skin.38
Beta-Carotene: Fruits and vegetables (eg. carrot, pumpkin, sweet potato, mango) are rich in beta-carotene. As an endogenous photoprotector, it prevents erythema formation resulting from UV radiation.39 The effect of photoprotection is dependent on treatment dosages and duration.
Lycopene: Lycopene, a bright red carotenoid pigment, exists in tomatoes and red vegetables or fruits, such as red carrots, watermelons, and papayas, and is a very efficient singlet oxygen quencher. Research has proven its effectiveness in reduction of erythema resulting from UV radiation.40
Astaxanthin: Microalgae, salmon, trout, shrimp, and crayfish contain astaxanthin. Astaxanthin has proven photoprotective activity against UVA.41
GARMENTS
CLOTHING AS A PHOTOPROTECTIVE MEASURE
CLOTHING AS A
PHOTOPROTECTIVE
MEASURE
Clothing, including hats, is an integral part of photoprotection. Compared to sunscreens, clothing is easy to put on, durable, and a social necessity. However, in most cultures, there are body sites that are infrequently covered by clothing, such as the face, the V area of the neck, and the dorsal hands. During hot (and sunny) weather, garments tend to cover even less skin. When performing outdoor activities, it is crucial that one wear clothing that provides protection against the sun, especially children. Parents should educate their children about proper clothing before going outdoors. A wide-brimmed hat is highly recommended as it can protect wider areas, including the forehead, eyes, and nose.
ULTRAVIOLET PROTECTION FACTOR
ULTRAVIOLET PROTECTION
FACTOR
UV protection factor (UPF) is the in-vitro measurement used in many countries, including the United States, Australia, and the European Union, to quantify the ability of fabrics to protect against UV. The amount to which 290 to 400-nm wavelengths penetrate through clothing is measured by spectrophotometric technique. The higher UPF, the less UV penetrates through fabrics. Because erythema is the factor considered, similar to the SPF, UPF is a better reflection of UVB than UVA protection.42 In the United States, garments are classified as having good protection (UPF15 to UPF24), very good protection (UPF25 to UPF39), or excellent protection (UPF40 to UPF50+).
Several factors affect the UV protectiveness of garments.5,42 Polyester fibers are the best UV absorber, whereas cotton and rayon are the poorest. Laundering garments made from cotton or rayon increases the UPF because of shrinkage, causing a decrease in the porosity of the fabrics. Wetness decreases the UV protection of a light-colored (especially white) garment. This is because the protective effect of white cotton fabric is mainly from light-scattering at the fiber–air interface: when wet, the fabric no longer scatters light and the garment becomes more transparent to both UV and visible light. In contrast, dark-colored garments absorb light and thus do not become see-through or provide less UV protection when wet. Chemical treatments include the incorporation of UV absorbers in fabrics during the manufacturing (mill finishing) process; the addition of UV absorber as laundry additives, and the addition of optical whitening agents, which are widely incorporated in many laundry detergents in the United States and Europe. These optical whitening agents absorb UV radiation at 360 nm and convert it to a visible light wavelength of 430 nm, thereby decreasing UV transmission through the fabric. The emission of visible light from the fabric makes the fabric look “brighter.” It is a common misperception that color of the fabric linearly correlates with the UPF. In experiments with cotton fabric with a UPF of 4.1, red fabric with the same dye concentration had UPF of 41, 31, and 20, depending on the type of red dye used. A yellow fabric had UPF of 25, whereas a violet one had UPF of 24.42
This is because color is a reflection of the visible light that the eye would see and the brain would perceive; it does not necessarily correlate with the transmission of UV rays through the fabric.
GLASS
GLASS USED IN BUILDINGS AND CARS
GLASS USED IN BUILDINGS
AND CARS
Transmission of UV radiation through windows depends on glass type, thickness, and color. It is well known that UVB is effectively filtered by glass. Many types of glass now also have very good UVA2 and UVA1 protection (up to 380 nm). It should be noted that car windshields are made of laminated glass, which allows less than 1% of UV (300 nm to 380 nm) to pass through, whereas side and rear windows are usually made from nonlaminated glass that allows a higher level of UVA transmission. This explains why common sites of involvement for patients with a photodermatosis are the side of the face and forearm closest to the side window of the car.43
SUNGLASSES
SUNGLASSES
Sunglasses protect eyes and skin near eyes from the sunlight, as UV radiation damages cornea, conjunctiva,
28
lens, and retina. Acute UV damage includes photokeratitis, mainly caused by UVB, and solar retinitis, caused by visible light. Chronic damage include cataract, pterygium, and macular degeneration. Mainly UVB is absorbed by the cornea to damage it; in addition, UVA, the longer UV wavelengths, damages the lens and further provokes cataracts. Visible and infrared rays impair the retina. Consequently to protect the retina, yellow-colored or red-colored sunglasses, which can block blue or purple light, are preferred.44 Sunglasses are especially important for children because their clear ocular lenses transmit more visible light when compared to adult lenses.45 Lenses with darker colors may induce greater exposure to UV as a consequence of pupil dilation, unless the lenses offer good UV protection. Also, the shape of the lenses should such that they block light entering from the side. Sunglasses are also recommended during morning and afternoon hours when sunlight is parallel with eye levels. The time of maximum UV exposure to the eye is not from 10:00 am to 2:00 pm as in the case of the skin, but is between 8:00 and 10:00 am and 2:00 and 4:00 pm, when solar radiation is parallel to the eye.46
Australia has led the world in sunglass standards, developing the world’s first national mandatory standard for sunglasses for general use in 1971; it was last revised in 2003 (AS/NZ 1067:2003). The amount of visible light transmitted through the lens is called luminous transmittance; a lens with 20% luminous transmittance would allow 20% of the visible light to pass through. Lenses are grouped into 5 categories (0 to 4), ranging from fashion sunglasses (lens category 0) to specialpurpose sunglasses for very high sun-glare reduction (lens category 4); category 4 lenses are not to be worn during driving. Category 0 lenses are allowed to have luminous transmission of 80% to 100%, whereas category 4 transmission is limited to 3% to 8%. The standard requires that the UVB transmittance be 5% of the luminous transmittance. Specifically, if the luminous transmittance is 20%, then the allowed UVB transmittance is 5% of 20%, which is 1%. The UVA transmittance for lens categories 0 to 2 must be no more than the luminous transmittance, while for lens categories 3 and 4, it must be no more than 50% of the luminous transmittance. The standard also mandates that the minimum vertical diameter for adult sunglasses is 28 mm, and for children, 24 mm. The 2003 Australian Standard is similar to the European Standard EN 1836:2005. The 2 standards differ in the maximum amount of UVB transmission allowed and the definition of UVA.47
The U.S. sunglass standard was first published in 1972 by the American National Standards Institute (ANSI) and last revised in 2010 (ANSI Z80.3). However, unlike the Australian standard, compliance with the U.S. standard is voluntary and is not followed by all manufacturers. The U.S. standard classified sunglasses as Normal Use (eg, from home to the car to the office) or High or Prolonged Exposure (eg, at the beach, fishing, skiing). Lenses are classified by intended function as cosmetic purpose, general purpose, special purpose very dark, and special purpose strongly colored.47 For example, for general purpose sunglasses, ANSI Z80.3
3631
28
requires less than 1% of the wavelengths below 310 nm to be transmitted. No minimum vertical dimension of the sunglasses is stated in the U.S. standard.
PHOTOPROTECTIVE CARE FOR PHOTOSENSITIVE SKIN DISEASES
Photosensitivity is generally defined as an abnormal reaction of the skin to sunlight and other sources of UV light. In patients with photosensitive skin diseases, it is important to provide them with specific instructions and guidelines regarding how to incorporate photoprotection in daily life (Table 197-3). Individuals with limited sun exposure because of rigorous practice of photoprotection and patients with photosensitive skin diseases are known to be at risk for vitamin D insufficiency. In a newer study with cutaneous lupus erythematosus patients, 25-hydroxyvitamin D levels were found to be significantly lower among sun avoiders and daily sunscreen users than among individuals who did not avoid the sun.24 Dietary supplementation with at least 400 IU/day of vitamin D3 (cholecalciferol) is thus recommended for all patients with photosensitive disorders who avoid sun and use sunscreens. Vitamin D3 (cholecalciferol, the natural form produced endogenously) is superior to vitamin D2 (ergocalciferol).
LUPUS ERYTHEMATOSUS
LUPUS ERYTHEMATOSUS
As UV-induced skin lesions in patients with cutaneous lupus erythematosus could develop up to several weeks after UV exposure, a relationship between sun exposure and exacerbation of cutaneous lupus erythematosus does not seem obvious to the patient. Consequently, patients must be informed about the relationship of UV exposure to their disease. The use of a broad-spectrum sunscreen with high UVB and UVA protection factors prevents skin lesions in all patients with photosensitive cutaneous lupus erythematosus.48
■Strict avoidance of sunlight exposure and other sources of ultraviolet
■Strict avoidance of sunlight exposure and other sources of
ultraviolet
■Physical protection including clothing, hat, umbrella, and sunglasses
■Physical protection including clothing, hat, umbrella, and
sunglasses
■Broad-spectrum sunscreens (sun protection factor ≥50)
■Broad-spectrum sunscreens (sun protection factor ≥50)
■Oral antioxidants
■Oral antioxidants
■Removal of photosensitizing drugs
■Removal of photosensitizing drugs
3632
■Vitamin D supplementation
■Vitamin D supplementation
XERODERMA PIGMENTOSUM
XERODERMA
PIGMENTOSUM
Xeroderma pigmentosum is a rare autosomal recessive disease of DNA repair, characterized by severe UV sensitivity with greatly increased risk for skin cancer. The goal of UV protection is to significantly lessen the amount of UV radiation reaching the skin and eyes of xeroderma pigmentosum patients. Special UV-blocking clothing treated with UV absorbers and blockers is recommended. Xeroderma pigmentosum patients should wear large-brimmed sun hats (made with UV blocking material), and may use a UV-blocking plastic shield attached to the hat that covers the whole face. Xeroderma pigmentosum patients should wear UVA-blocking and UVB-blocking sunglasses that provide full eye coverage, as well as a highly effective sunscreen on a daily basis. During the day, sunscreen should be reapplied every 2 to 3 hours.
ERYTHROPOIETIC PROTOPORPHYRIA
ERYTHROPOIETIC
PROTOPORPHYRIA
Erythropoietic protoporphyria is a rare, autosomal recessive inborn error of metabolism that is associated with severe painful photosensitivity. When the skin is exposed to sunlight, the accumulated phototoxic protoporphyrin is activated by blue light, resulting in singlet oxygen free radical reactions that lead to severe neuropathic pain, often followed by swelling and redness. Although several treatments (including betacarotene, N-acetyl-l-cysteine, and vitamin C) have been described in the literature, a systematic review of more than 20 studies showed little to no benefit.49 Afamelanotide (analog of human α-melanocyte–stimulating hormone) provided safe and effective photoprotection through eumelanin synthesis in patients with erythropoietic protoporphyria.50
ACKNOWLEDGMENTS
This chapter has been revised from its previous version written by Dr. Henry W. Lim.
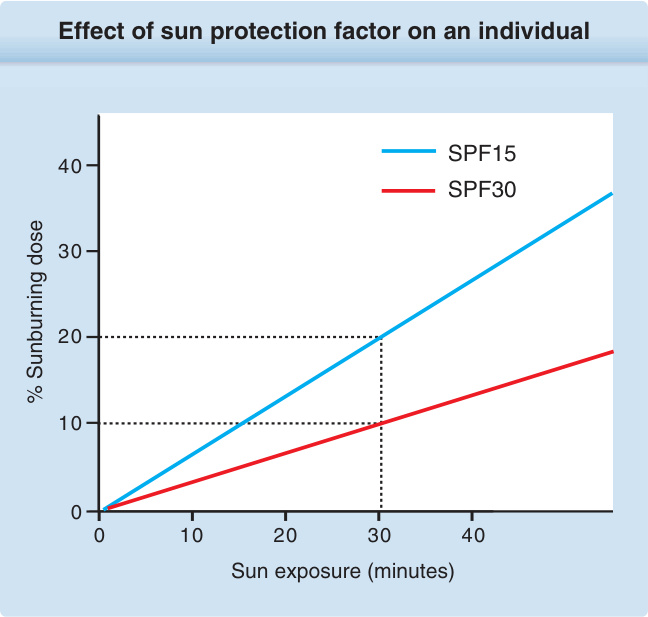
Figure 197-1 Effect of sun protection factor (SPF) 15 and SPF-30 sunscreens on an individual who would develop minimal erythema after 10 minutes of unprotected sun exposure. After a 30-minute sun exposure, 20% of a sunburning dose is achieved after the application of SPF15 sunscreen; after the application of SPF30 sunscreen, only 10% of a sunburning dose reaches the skin.
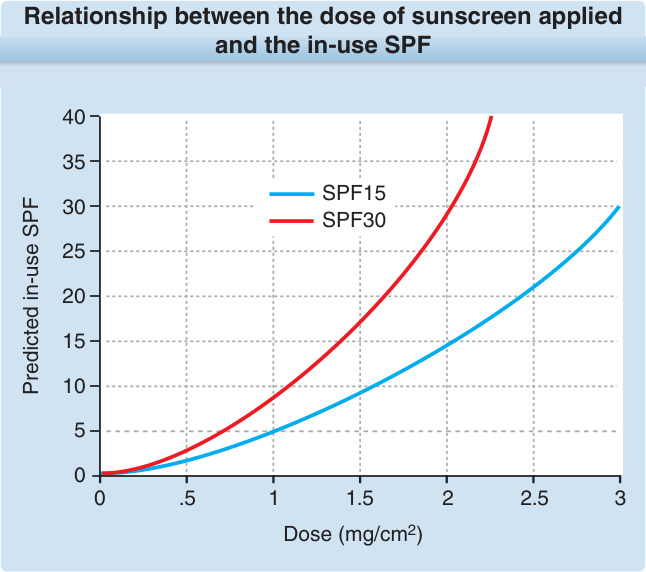
Figure 197-2 Relationship between the dose of sunscreen applied and the in-use sun protection factor (SPF). (Used with permission from JF Nash, Procter & Gamble, Cincinnati, OH.)
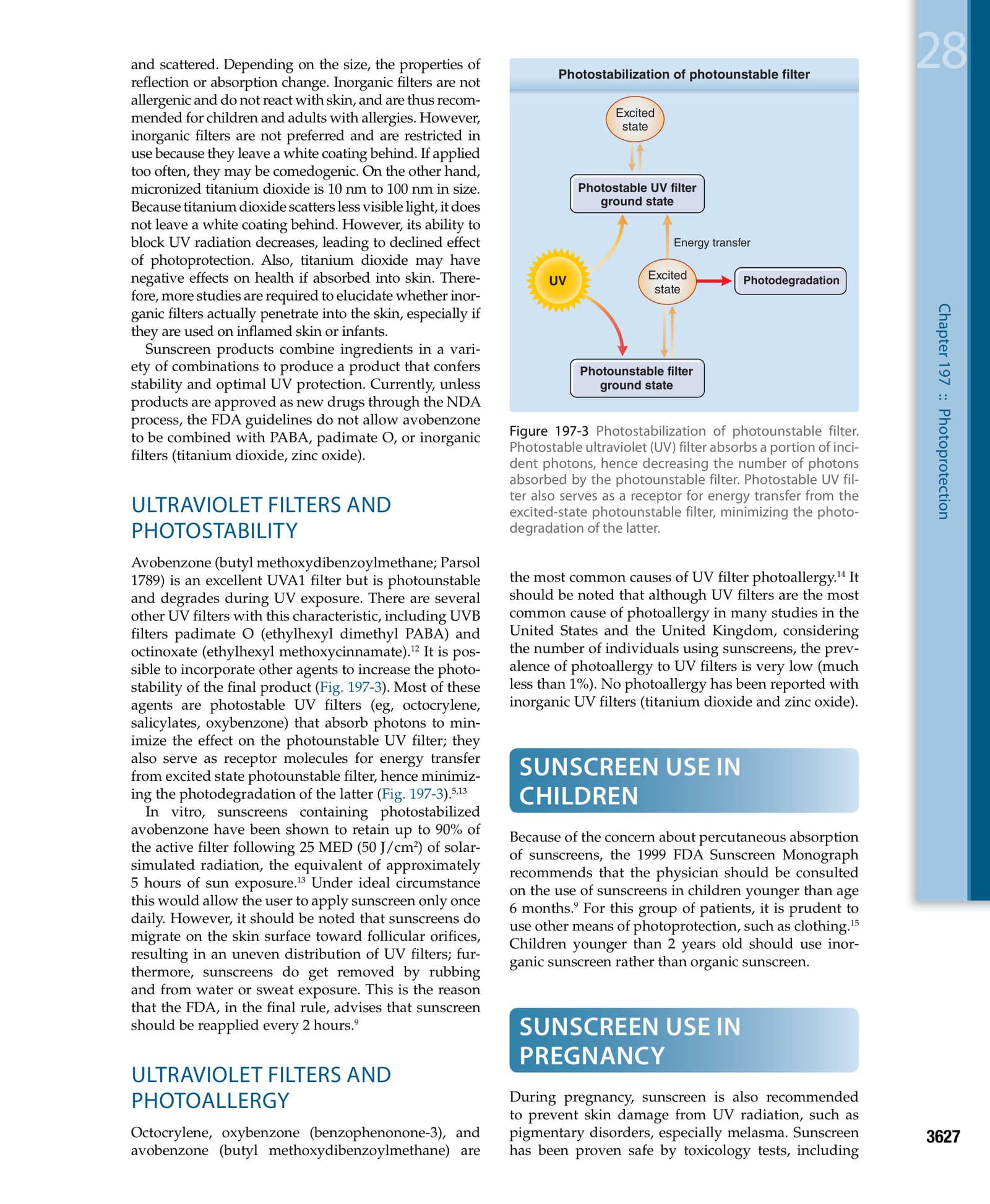
Figure 197-3 Photostabilization of photounstable filter. Photostable ultraviolet (UV) filter absorbs a portion of incident photons, hence decreasing the number of photons absorbed by the photounstable filter. Photostable UV filter also serves as a receptor for energy transfer from the excited-state photounstable filter, minimizing the photodegradation of the latter.
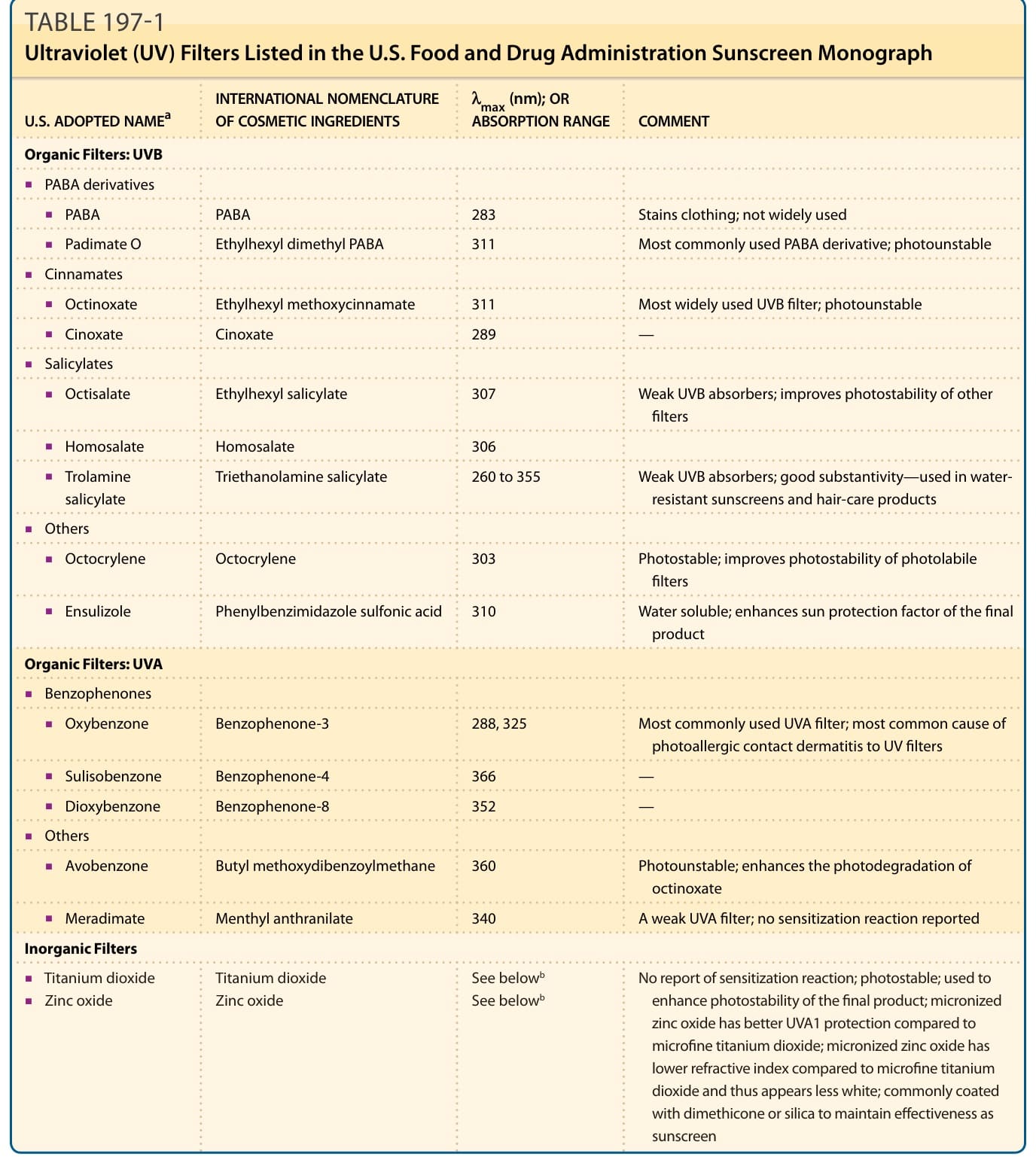
TABLE 197-1 Ultraviolet (UV) Filters Listed in the U.S. Food and Drug Administration Sunscreen Monograph
TABLE 197-2 Active Ingredients for Oral Photoprotection